Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
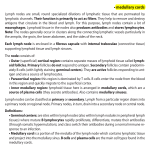
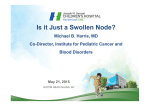
Surgical Oncology 23 (2014) 140e146 Contents lists available at ScienceDirect Surgical Oncology journal homepage: www.elsevier.com/locate/suronc Review Status and prognosis of lymph node metastasis in patients with cardia cancer e A systematic review Cecilie Okholm*, Lars Bo Svendsen, Michael P. Achiam Department of Surgical Gastroenterology, Rigshospitalet, University of Copenhagen, Blegdamsvej 9, 2100 København Ø, Denmark a r t i c l e i n f o a b s t r a c t Article history: Accepted 1 June 2014 Background: Adenocarcinoma of the gastroesophageal junction (GEJ) has a poor prognosis and survival rates significantly decreases if lymph node metastasis is present. An extensive lymphadenectomy may increase chances of cure, but may also lead to further postoperative morbidity and mortality. Therefore, the optimal treatment of cardia cancer remains controversial. A systematic review of English publications dealing with adenocarcinoma of the cardia was conducted to elucidate patterns of nodal spread and prognostic implications. Methods: A systematic literature search based on PRISMA guidelines identifying relevant studies describing lymph node metastasis and the associated prognosis. Lymph node stations were classified according to the Japanese Gastric Cancer Association guidelines. Results: The highest incidence of metastasis is seen in the nearest regional lymph nodes, station no. 1e3 and additionally in no. 7, 9 and 11. Correspondingly the best survival is seen when metastasis remain in the most locoregional nodes and survival equally tends to decrease as the metastasis become more distant. Furthermore, the presence of lymph node metastasis significantly correlates to the TNM-stage. Incidences of metastasis in mediastinal lymph nodes are associated with poor survival. Conclusion: The best survival rates is seen when lymph node metastasis remains locoregional and survival rates decreases when distant lymph node metastasis is present. The dissection of locoregional lymph nodes offers significantly therapeutic benefit, but larger and prospective studies are needed to evaluate the effect of dissecting distant and mediastinal lymph nodes. © 2014 Elsevier Ltd. All rights reserved. Keywords: Adenocarcinoma Cardia cancer Gastroesophageal junction Lymphadenectomy Lymph node metastasis Prognosis Contents Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141 Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141 Search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141 Eligibility criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141 Classifications of cardia cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141 Siewert's classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141 Classifications of lymph node stations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142 The Japanese Gastric Cancer Association . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142 Pattern of nodal spread in cardia cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 142 Five-year survival related to each lymph node station . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143 Additional findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144 Morbidity and mortality related to D1/D2 dissection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144 Number of lymph nodes removed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144 * Corresponding author. Tel.: þ45 25114720. E-mail address: [email protected] (C. Okholm). http://dx.doi.org/10.1016/j.suronc.2014.06.001 0960-7404/© 2014 Elsevier Ltd. All rights reserved. C. Okholm et al. / Surgical Oncology 23 (2014) 140e146 141 Future perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Sentinel node for gastric cardia cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Authorship statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 145 Introduction Adenocarcinoma of the gastroesophageal junction (GEJ) is an important clinical entity due to the increasing incidence in the West [1,2]. Arising from the gastric cardia, the cancer has a poor prognosis with five-year survival rates of 24e36% after curative resection [3,4]. Located in the borderline between the stomach and esophagus it shares many similarities with both regions, although the optimal characterization and treatment of cardia cancer remains controversial. Studies have shown, that lymph node involvement is a strong prognostic predictor of survival [5], and five-year survival rates significantly decreases from 53% to 11% when lymph node metastasis is present [6]. Lymphadenectomy is considered essential in addition to the surgical treatment, since lymph node involvement is a major determinant of locoregional recurrence [7,8]. The standard treatment in Asia for gastric cancer is surgical resection combined with the extensive D2 lymph node dissection, whereas most of the European countries perform a less extensive D1þ dissection [5]. The extended lymph node dissection has been associated with an increased chance for cure in some studies, but may also lead to a higher incidence of postoperative morbidity and mortality [9e11]. Given the different clinicopathological characteristics in patients with cardia cancer, the need and extent of lymphadenectomy remain controversial in the West. We conducted a systematic review of English publications dealing with adenocarcinoma of the cardia to elucidate patterns of nodal spread and prognostic implications. Materials and methods Search strategy The databases PubMed and EMBASE were searched strategically for terms according to the PRISMA guidelines on the 15th of April 2014 [12]. The search was limited to English language. The identified titles and abstracts were scanned for relevant topics, and the full texts of the potentially relevant articles were obtained. In addition, review articles were scanned for missed articles. Potentially relevant studies were identified through hand searching of the reference lists of the acquired studies. There were no restrictions on the year of publication. The search string used was: ((Gastric cardia cancer OR gastric cardia carcinoma OR gastric cardia adenocarcinoma OR esophagogastric junction cancer OR esophageal cancer OR siewert type II OR siewert type 2 OR siewerts type II OR siewerts type 2)) AND (lymphatic metastasis OR nodal spread). Siewert's classification will be presented below. The results from the search are presented in Fig. 1. Eligibility criteria Relevant papers were included in the review based on the following eligibility criteria. There were no restrictions on study design, since no RCT's has been made to date to our knowledge. Participants: Patients with cardia cancer undergoing surgery primarily focused on Siewert's type II or junctional adenocarcinomas. If the article was based on several gastric or esophageal cancers, the results for cardia cancer patients had to be presented separately. Interventions: Patients undergoing lymphadenectomy with retrieval of involved lymph nodes and estimation of lymph node status. Additionally, records of the incidences of node metastasis to each Japanese Gastric Cancer Association (JGCA) lymph node station for node positive patients. Of particular interest were articles estimating the associated five-year survival (5-Y-S) to each lymph node station. Outcome: Incidence of lymph node metastasis to JGCA lymph node stations. In cases where studies presented data from all three Siewert's types combined, we still included the studies since no difference between the three types has been observed. Data extraction: Lymph node metastasis in percent associated to each lymph node station and median and range of the correlated 5-Y-S to each station if presented. Additionally, the prognosis and correlation to the TNM-stage was extracted. Only available lymph node stations relevant to the different classifications for D1, D2 and D3 dissections were analyzed. Thus, distant lymph node stations and some upper thoracic and cervical stations were not included in this review. Exclusion: Exclusion criteria were articles with non-cardia cancer, esophagus cancer, subcardia or gastric cancer, and articles with results not distinguished from esophagus or gastric cancer. Additionally gastric carcinosarcoma, stromal tumors and squamous cell tumors were excluded. Furthermore, articles focusing on biological markers for lymph node retrieval, patients receiving neoadjuvant chemotherapy and studies without linkage to lymph node stations were considered irrelevant. If the results were combined for squamous cell and adenocarcinoma they were excluded in addition. Classifications of cardia cancer Siewert's classification In 1998 Siewert et al. [13] introduced a classification for adenocarcinomas of the GEJ, defining them as tumors having their epicenter within five cm proximal or distal of the anatomical cardia. Three distinct tumors were differentiated: Type I: Adenocarcinoma of the distal esophagus which usually arises from an area with specialized intestinal metaplasia of the esophagus and which may infiltrate the gastroesophageal junction from above. Type II: True carcinoma of the cardia, arising from the cardia epithelium or short segments with intestinal metaplasia at the gastroesophageal junction. Type III: Subcardial gastric carcinoma, which infiltrates the gastroesophageal junction and distal esophagus from below. 142 C. Okholm et al. / Surgical Oncology 23 (2014) 140e146 lymphatic flow and observed survival associated with metastasis in each station (Fig. 1). The third English edition from JGCA (2011) [16] defined lymph node stations 1e12 and 19, 20, 110 and 111 for tumors with esophageal invasion as regional lymph node metastasis; others were classified as distant metastasis. Moreover, an edition with special focus on treatment guidelines was published, in which the extent of lymphadenectomy was defined according to the type of gastrectomy [17]. In principle, a D1 or a D1þ lymphadenectomy was indicated for node negative tumors, and D2 was indicated for node positive or T2eT4 tumors. Since the pre- and perioperative diagnosis of lymph node metastases remains unreliable, it was recommended that a D2 lymphadenectomy should be performed whenever nodal involvement was suspected. Although it is not prerequisite, the examination of 16 or more regional lymph nodes was recommended for Nstatus determination [17]. Since most of the included studies describe lymph node stations and dissections according to the JGCA 1998 edition [15], the results in this review will be presented according to this edition. Results Based on the search methods described, a total of 17 articles were identified describing the pattern of lymph node spread and six articles were identified describing the associated five-year survival (5-Y-S). The six articles comprised of retrospective cohorts with a number of included patients ranging from 62 to 225 (Table 1). Pattern of nodal spread in cardia cancer Figure 1. Station numbers of regional lymph nodes. Reprinted with permission from the Japan Esophageal Society, from the article “Japanese Classification of Esophageal Cancer, tenth edition: printed in part I”, printed in Esophagus (2009) 6: 1e25. Cardia cancer was defined as adenocarcinoma of the GEJ. The search was specified to Siewert's type II, since this was considered the true cardia carcinoma [13]. Siewert type I is mainly treated like esophagus cancer, since most tumors arise from areas of intestinal metaplasia in Barrett's epithelium as a consequence of reflux. In contrast, type III tumors represent proximal gastric cancer and should be approached in accordance with gastric cancer guidelines [14]. The characterization and optimal treatment for Siewert's type II cardia cancer remains debatable, and is therefore the primary focus of this review. Classifications of lymph node stations The Japanese Gastric Cancer Association Classification guidelines published by JGCA for gastric cancer including definitions of the lymph node stations, aimed at providing a common language for the clinical and pathological description of gastric cancer. In 1998, the second English edition from JGCA classified lymph nodes into three groups depending on the location of the primary tumor [15]. These three groups were subdivided into 33 stations based on the results of studies of In Fig. 2, the incidence of lymph node metastases is presented according to the JGCA lymph node stations divided into D1eD3 dissections [3,18e33]. The highest incidence of lymph node metastasis is seen in regional lymph nodes, especially station no. 1e3, with a range from 13.7 to 72.7%. The incidence in station no.4 is lower, ranging from 0 to 31.8%. In the D2 stations the highest incidence of metastasis is observed in no. 7, 9 and 11, ranging from 0 to 45.5%. The incidences in D3 stations are remarkably lower with fewer than 20% of nodes involved. Incidences and survival rates associated with mediastinal lymph node involvement is poorly reported and few are classified Table 1 Included studies. Yamashita et al. [30] Hoskokawa et al. [20] Mine et al. [25] Fujitani et al. [19] Saito et al. [3] Wang et al. [28] Fang et al. [18] Matsumoto et al. [23] Nakamura et al. [26] Ichikura et al. [21] Feith et al. [14] Mattioli et al. [24] Yamamoto et al. [29] Kakeji et al. [22] Pedrazzani et al. [36] Gertler et al. [32] Meier et al. [31] Yuasa et al. [33] n Siewert n of LN stations 5-Y-S 225 179 150 86 110 42 51 58 30 31 485 116 67 129 62 224 167 40 II I,II,III II II II II II I,II,III II II II II II I,II,III I,II,III I,II,III II,III II 19 17 15 13 16 17 16 16 11 10 6 8 4 15 14 7 9 8 x x x x x x C. Okholm et al. / Surgical Oncology 23 (2014) 140e146 143 Figure 2. Lymph node metastasis according to JGCA stations in % with median and range. according to stations (data is not presented) [3,20,21,24e26,29]. Node metastasis in the lower mediastinal stations ranged from 7.5 to 23.8%, whereas patients with upper mediastinal node involvement were below 4%. Patients with lymph node involvement extending to the proximal field of the chest (no. 106, 107) tended to have a higher ratio of involved to total lymph nodes [34]. One study found positive nodes in the chest in 24% of the patients [35]. Five-year survival related to each lymph node station In Fig. 3 the 5-Y-S is shown in percent with median and range according to each lymph node station [3,19,20,25,30,36]. Stations in D1 has the best 5-Y-S rates overall, ranging from 0 to 50%. Involvement of no. 4sb reduced the survival rate, although the incidence of metastasis was correspondingly low. In D2 stations the 5-Y-S ranges from 0 to 53%. The best survival rate is seen in station no. 7, the station with the highest lymph node involvement in this group. The lowest survival rate is seen in station no. 9, with survival rates below 14.7%. Metastasis to the lymph node stations in D3 shows overall very poor survival. Data is not presented due to insufficiency of reported data. No patients with involvement of station no. 5, 12 and 111 survived after five years. Only one study found patients alive after five years with involvement of station 6 [19]. Few studies reported survival in station 16 and 110, ranging from 0 to 23.8% [3,20,25,30,36]. Additional findings The presence of lymph node metastasis seems to be significantly correlated to the depth of tumor invasion [28,36e38]. Ielpo et al. found an increasing rate of distal nodal involvement as the T-stage increases [35]. Furthermore, lymph node metastases were significantly correlated to the size of the tumor, where large tumors (>4 cm) had significantly greater risk of lymph node involvement [37]. Some studies have investigated the influence of lymph node metastasis on prognosis. The majority concluded that the presence of lymph node metastasis (Nþ) was an independent prognostic factor, and was associated with poor survival [3,25,27,37,39,40]. Only one study found no significantly difference between Nþ/N [29]. A limited number of studies investigated survival rates when the frequency of lymph node involvement was divided into N-stage (Table 2). There was an observable correlation between higher Nstage and poorer survival, with 5-Y-S rates from 2 to 17.4% in N3 tumors compared to 5-Y-S in N0 up to 82.7% [5,19,30]. Figure 3. 5-Y-S according to JGCA lymph node stations in % with median and range. 144 C. Okholm et al. / Surgical Oncology 23 (2014) 140e146 Table 2 Prognosis to N-stage in %. Yamashita et al. [30] 5-Y-S Fujitani et al. [19] 5-Y-S Zhang et al. [5] 5-Y-S N0 N1 N2 N3 82.7 65.1 35.9 17.4 p < 0.0001 N0 N1 N2 N3 64.7 54.4 31.6 10.7 p < 0.0001 N0 N1 N2 N3 47.4 29.4 5.5 2.0 p < 0.001 Discussion The highest incidences of lymph node metastasis in patients with cardia cancer are located in the locoregional nodes; especially station no. 1e3 and no. 7, 9 and 11. Aikou et al. reported in 1989 [41] that lymph node metastasis from cardia cancer preferentially make their way to the upper gastric lymph nodes located at the right and left cardia and along the lesser curvature of the stomach, and in addition various involvement of the coeliac axis, the splenic hilum and the para-aortic lymph nodes [41]. A more recent review confirms the spread to the paracardial and lesser curvature regions [42]. This is in line with our results, although the incidence of paraaortic lymph involvement was below 19%. The best prognosis is correspondingly seen when metastasis remain in the nearest regional lymph nodes, which indicate that dissection here offers significantly therapeutic benefits. Station 1e3 are included in D1 dissection in both gastric classifications [15,16]. In D2 dissection the best survival is seen in patients with metastasis in station no. 7, which in the most recent classification (JGCA 2011) now is a part of D1 dissection. Station no. 10 with lymph node metastasis up to 22.7%, has 5-Y-S ranging from 0 to 50%. In both JGCA station no. 10 is a part of D2 dissection. Earlier recommendations were spleenectomy when dissecting no. 10 in order to properly dissect the nodes [43], but recently spleen- and pancreas preserving D2 dissections has been recommended in high-volume centers for western patients [44]. In general, the survival rates decrease along with an increased distal lymph node involvement, and might indicate a cancer in the advanced stage. Dissection of station no. 5 and 6 (D3 dissection) may offer marginal therapeutic benefit, and these stations might represent distant rather than locoregional metastasis [19,30]. All stations in D3 (except no 5 and 6) were in 2011 upgraded to a D1þ or D2 dissection. When interpreting the results, it is important to consider that survival associated to lymph node stations is interdependent. It is difficult to determine patient survival correlated to one isolated station, since metastasis most likely will be present in other stations as well. Also, studies have shown a decreasing survival when N-stage is increasing (Table 2). Therefore, it is difficult to conclude on survival outcome from one isolated lymph node. To our knowledge, no studies investigating survival adjusted for this factor has been made to date. The results of this review summarize survival rates correlated to lymph node stations of D1, D2 or D3 dissection. Overall, survival rates seem consistent in D1 and station no. 7 and 10. The decreasing survival rates in D2 and D3 stations may represent advanced disease. Morbidity and mortality related to D1/D2 dissection The definitions of D1 and D2 dissection have changed over the years, but the optimal treatment is still debatable. A study of 110 patients with cardia cancer found D2 morbidity and mortality rates higher than D1, although not significantly [37]. One study with 123 patients compared D4 (D3þ paraaortic station no. 15,16) and D2 dissection and concluded that in node positive patients where invasion was deeper than T2, the D4 dissection showed superior survival than D2 (p < 0.05) [40]. It has been stated that the D2 dissection allows more adequate staging and more lymph nodes examined [9,45], and Lerut et al. found that an extended three-field lymphadenectomy (D2þ posterior mediastinum) could be performed with low mortality and acceptable morbidity [46]. However, many of these studies suffered from a low number of patients and a non-randomized design. In patients with gastric cancer, large RCT's comparing the morbidity and mortality rates of D1 and D2 dissection has been performed [10,11,43]. All concluded that D2 dissection was associated with worse morbidity and mortality than D1 dissection. In contrast, patients undergoing D2 dissection experienced lower locoregional recurrence and gastric cancer related deaths [11]. The increased morbidity and mortality rates associated with the D2 dissection has been criticized to be a result of the invasive distal pancreatectomy and the removal of the spleen in order to dissect station no. 10 [11]. Degiuli et al. found no difference in morbidity and mortality rates comparing D1 and D2 dissection when performing a spleen and pancreas preserving D2 dissection in gastric cancer patients, although he did not find an increased survival [44]. According to the Danish Gastroesophageal Cancer Group (DECG), the standard approach is a D1þ dissection combined with removal of a minimum of 15 lymph nodes, always including abdominal station 7 and 9 and standard lymphadenectomy in thorax (lymph nodes no. 20,107,108,110,111) [47]. The five-year survival rate after curative resection was 32% (95% CI 28e36) in 2011 which is comparable to international studies where overall 5Y-S rates range from 21.9% to 27.2% [5,24,36,46]. The depth of tumor invasion seems to reflect the incidence and extent of lymph node metastasis, and it has been suggested that a predetermination of the T-stage may help to indicate the relevant lymph node dissection [28]. The correlation between the TNMstage and the involvement of lymph nodes indicate and confirm that TNM-staging with adequate lymphadenectomy should be the goal of the curative surgical approach. In contrast, it is difficult to predetermine the presence of mediastinal and thoracic lymph node metastasis and the removal of these stations is still controversial. Station no. 110 were in 1998 included in D3 dissection, but were in 2011 upgraded to D1þ. This indicates that the significance of mediastinal lymph node involvement may have increased. Involvement of these nodes may represent distant rather than regional metastasis and might indicate a cancer in the advanced stage [26,34,48]. The frequency of lymph node metastasis in mediastinum was low, and dissection of these nodes is suggested to have minimal or no survival benefits [26,49]. Since the number of studies is limited and the mediastinal and thoracic lymph node stations are inadequately defined, it is difficult to conclude any beneficial effect of dissection these stations. Number of lymph nodes removed Another question is whether the removal of specific lymph node stations or the amount of lymph nodes removed is the most important prognostic factor. A large international multicenter study with more than 2300 esophagus cancer patients concluded that the number of lymph nodes removed was a prognostic factor, even when adjusted for lymph node status and number of involved lymph nodes [50]. There was no relation to stage migration, but simply a correlation between the number of lymph node harvest and increased prognosis. They recommended that a minimum of 23 lymph nodes should be removed in order to achieve the best outcome. C. Okholm et al. / Surgical Oncology 23 (2014) 140e146 145 Studies investigating this approach in cardia cancer are limited, although it has been stated that adequate dissection over 15 lymph nodes is necessary to permit a sufficient staging [9,35,51]. The improved prognosis when performing an increased lymph node harvest may be due to a better diagnosis, but it could also represent better surgical techniques. Larger and prospective studies are needed to investigate this field further. lymph node metastasis remains locoregional and only involves those in the D1 dissection (JGCA 1998 edition) and no. 7 and 10. Survival rates decrease when lymph node involvement become distant but the beneficial effect of dissecting these is debatable. Larger and prospective studies are needed to validate the optimal lymphadenectomy and further investigate the significance of predetermination of T-stage and the concept of sentinel node. Future perspectives Conflict of interest statement Sentinel node for gastric cardia cancer Limited publications are available concerning sentinel node techniques for cardia cancer. In a small study of 20 patients with adenocarcinoma of the gastroesophageal junction; sentinel node were able to correctly predict lymph node status in overall 85% of the early stage carcinomas [52]. In gastric cancer, sentinel node is a promising concept and has shown high sensitivities in early stage cancers [53,54]. The presence of skip metastasis in gastric cancer, which has been observed in 10% of the cases [55] may be an obstacle [53]. In cardia cancer incidences of skip nodes is more rarely observed, one study found no cases, and another study had one incidence of skip metastasis in 22 patients [28,56]. Since the frequency of skip metastases in cardia cancer seems lower, sentinel node might have increased clinical significance due to the borderline location and varying lymphatic drainage of cardia cancer [57]. Especially in the context of the need to perform a limited lymphadenectomy including only involved stations, it is attractive to consider the use of a sentinel node technique in order to determine the extent of lymphadenectomy [58]. Limitations This review summarizes the existing literature of lymph node metastasis and prognosis in cardia cancer patients. However, studies are limited and suffer from retrospective designs. Furthermore, the studies are not exclusively comparable in relation to lymph node stations, since they describe metastasis in different numbers of lymph node stations. In addition, some authors combine stations, e.g. 8a, 8b and 8p as station 8, or do not define it in detail. Because of this, there may be some bias when investigating the exact lymph node spread. Moreover, in the results presenting lymph node spread some stations are described by all included studies and some are only described by few of the included studies. As mentioned before, some studies present results combined for all Siewert's types, and bias may exist when concluding lymphatic pathways from Siewert's type II. Also, the number of patients in the included studies is low. Furthermore, studies comparing D1 and D2 dissection regimes may be prone to selection bias, since some studies may have chosen D2 lymphadenectomy to patients that are younger and healthier. Despite an extensive reviewing of the search results, it is possible that valuable articles have been missed. Furthermore, due to language restrictions, some potential relevant articles published in Chinese or Japanese are not included in this review. The retrospective design of the studies is a major limitation, which must be adjusted for when interpreting the results. This indicates that this field needs further investigation. Conclusion This review confirms that the spread of cardia cancer preferentially involves the locoregional gastric lymph node stations, followed by station 7, 9 and 11. The best survival rates are seen when The authors have no conflict of interests to declare. Acknowledgments The authors have no conflict of interests to declare. Authorship statement Guarantor of the integrity of the study: Lars Bo Svendsen, Michael P. Achiam. Study concepts: Cecilie Okholm, Michael P. Achiam. Study design: Cecilie Okholm, Lars Bo Svendsen, Michael P. Achiam. Definition of intellectual content: Cecilie Okholm, Lars Bo Svendsen, Michael P. Achiam. Literature research: Cecilie Okholm. Data acquisition: Cecilie Okholm. Data analysis: Cecilie Okholm, Lars Bo Svendsen, Michael P. Achiam. Statistical analysis: Cecilie Okholm, Lars Bo Svendsen, Michael P. Achiam. Manuscript preparation: Cecilie Okholm. Manuscript editing: Cecilie Okholm, Lars Bo Svendsen, Michael P. Achiam. Manuscript review: Cecilie Okholm, Lars Bo Svendsen, Michael P. Achiam. References [1] DeMeester SR. Adenocarcinoma of the esophagus and cardia: a review of the disease and its treatment. Ann Surg Oncol 2006;13:12e30. [2] Devesa SS, Blot WJ, Fraumeni Jr JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998;83: 2049e53. [3] Saito H, Fukumoto Y, Osaki T, Fukuda K, Tatebe S, Tsujitani S, et al. Distinct recurrence pattern and outcome of adenocarcinoma of the gastric cardia in comparison with carcinoma of other regions of the stomach. World J Surg 2006;30:1864e9. O, Lebreton G, et al. Periop[4] Ychou M, Boige V, Pignon JP, Conroy T, Bouche erative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol 2011;29:1715e21. [5] Zhang M, Li Z, Ma Y, Zhu G, Zhang H, Xue Y. Prognostic predictors of patients with carcinoma of the gastric cardia. Hepatogastroenterology 2012;59:930e3. [6] Del Genio A, Rossetti G, Maffettone V, Napolitano V, Brusciano L, del Genio G, et al. Gastroesophageal junction adenocarcinoma: what are the factors influencing long-term survival? Int Surg 2006;91:174e80. [7] Lerut T, Coosemans W, Decker G, De Leyn P, Moons J, Nafteux P, et al. Extended surgery for cancer of the esophagus and gastroesophageal junction. J Surg Res 2004;117:58e63. [8] De Manzoni G, Pedrazzani C, Pasini F, Durante E, Gabbani M, Grandinetti A, et al. Pattern of recurrence after surgery in adenocarcinoma of the gastrooesophageal junction. Eur J Surg Oncol 2003;29:506e10. [9] Barbour AP, Rizk NP, Gonen M, Tang L, Bains MS, Rusch VW, et al. Lymphadenectomy for adenocarcinoma of the gastroesophageal junction (GEJ): impact of adequate staging on outcome. Ann Surg Oncol 2007;14:306e16. [10] Bonenkamp JJ, Songun I, Hermans J, Sasako M, Welvaart K, Plukker JT, et al. Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet 1995;345:745e8. [11] Songun I, Putter H, Kranenbarg EMK, Sasako M, van de Velde CJH. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010;11:439e49. 146 C. Okholm et al. / Surgical Oncology 23 (2014) 140e146 [12] Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336e41. [13] Siewert JR, Stein HJ, Sendler A, Fink U. Surgical resection for cancer of the cardia. Semin Surg Oncol 1999;17:125e31. [14] Feith M, Stein HJ, Siewert JR. Adenocarcinoma of the esophagogastric junction: surgical therapy based on 1602 consecutive resected patients. Surg Oncol Clin N Am 2006;15:751e64. [15] Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma - 2nd English edition. Gastric Cancer 1998;1:10e24. [16] Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011;14:101e12. [17] Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer 2011;14:113e23. [18] Fang WL, Wu CW, Chen JH, Lo SS, Hsieh MC, Shen KH, et al. Esophagogastric junction adenocarcinoma according to Siewert classification in Taiwan. Ann Surg Oncol 2009;16:3237e44. [19] Fujitani K, Miyashiro I, Mikata S, Tamura S, Imamura H, Hara J, et al. Pattern of abdominal nodal spread and optimal abdominal lymphadenectomy for advanced Siewert type II adenocarcinoma of the cardia: results of a multicenter study. Gastric Cancer 2013;16:301e8. [20] Hosokawa Y, Kinoshita T, Konishi M, Takahashi S, Gotohda N, Kato Y, et al. Clinicopathological features and prognostic factors of adenocarcinoma of the esophagogastric junction according to Siewert classification: experiences at a single institution in Japan. Ann Surg Oncol 2012;19:677e83. [21] Ichikura T, Ogawa T, Kawabata T, Chochi K, Sugasawa H, Mochizuki H. Is adenocarcinoma of the gastric cardia a distinct entity independent of subcardial carcinoma? World J Surg 2003;27:334e8. [22] Kakeji Y, Yamamoto M, Ito S, Sugiyama M, Egashira A, Saeki H, et al. Lymph node metastasis from cancer of the esophagogastric junction, and determination of the appropriate nodal dissection. Surg Today 2012;42:351e8. [23] Matsumoto S, Takayama T, Wakatsuki K, Enomoto K, Tanaka T, Migita K, et al. Surgical outcomes for cancer at the gastroesophageal junction. Am Surg 2012;78:1285e91. [24] Mattioli S, Di Simone MP, Ferruzzi L, D'Ovidio F, Pilotti V, Carella R, et al. Surgical therapy for adenocarcinoma of the cardia: modalities of recurrence and extension of resection. Dis Esophagus 2001;14:104e9. [25] Mine S, Sano T, Hiki N, Yamada K, Nunobe S, Yamaguchi T. Lymphadenectomy around the left renal vein in Siewert type II adenocarcinoma of the oesophagogastric junction. Br J Surg 2013;100:261e6. [26] Nakamura M, Iwahashi M, Nakamori M, Naka T, Ojima T, Iida T, et al. Lower mediastinal lymph node metastasis is an independent survival factor of Siewert type II and III adenocarcinomas in the gastroesophageal junction. Am Surg 2012;78:567e73. [27] Siewert JR, Stein HJ, Feith M. Adenocarcinoma of the esophago-gastric junction. Scand J Surg 2006;95:260e9. [28] Wang LS, Wu CW, Hsieh MJ, Fahn HJ, Huang MH, Chien KY. Lymph node metastasis in patients with adenocarcinoma of gastric cardia. Cancer 1993;71: 1948e53. [29] Yamamoto M, Baba H, Egashira A, Oki E, Ikebe M, Kakeji Y, et al. Adenocarcinoma of the esophagogastric junction in Japan. Hepatogastroenterology 2008;55:103e7. [30] Yamashita H, Katai H, Morita S, Saka M, Taniguchi H, Fukagawa T. Optimal extent of lymph node dissection for Siewert type II esophagogastric junction carcinoma. Ann Surg 2011;254:274e80. [31] Meier I, Merkel S, Papadopoulos T, Sauer R, Hohenberger W, Brunner TB. Adenocarcinoma of the esophagogastric junction: the pattern of metastatic lymph node dissemination as a rationale for elective lymphatic target volume definition. Int J Radiat Oncol Biol Phys 2008;70:1408e17. € fler H, Feith M. Prevalence and [32] Gertler R, Stein HJ, Schuster T, Rondak IC, Ho topography of lymph node metastases in early esophageal and gastric cancer. Ann Surg 2014;259:96e101. [33] Yuasa N, Miyake H, Yamada T, Ebata T, Nimura Y, Hattori T. Clinicopathologic comparison of Siewert type II and III adenocarcinomas of the gastroesophageal junction. World J Surg 2006;30:364e71. [34] Lagarde SM, Cense HA, Hulscher JBF, Tilanus HW, Ten Kate FJW, Obertop H, et al. Prospective analysis of patients with adenocarcinoma of the gastric cardia and lymph node metastasis in the proximal field of the chest. Br J Surg 2005;92:1404e8. [35] Ielpo B, Pernaute AS, Elia S, Buonomo OC, Valladares LD, Aguirre EP, et al. Impact of number and site of lymph node invasion on survival of adenocarcinoma of esophagogastric junction. Interact Cardiovasc Thorac Surg 2010;10: 704e8. [36] Pedrazzani C, de Manzoni G, Marrelli D, Giacopuzzi S, Corso G, Minicozzi AM, et al. Lymph node involvement in advanced gastroesophageal junction adenocarcinoma. J Thorac Cardiovasc Surg 2007;134:378e85. [37] Shimada H, Suzuki T, Nakajima K, Hori S, Hayashi H, Takeda A, et al. Lymph node metastasis with adenocarcinoma of the gastric cardia: clinicopathological analysis and indication for D1 dissection. Int Surg 1999;84:13e7. [38] Hsu CP, Wu CC, Chen CY, Hsu NY, -Hsia Jiun-Yi, Wang PY. Clinical experience in radical lymphadenectomy for adenocarcinoma of the gastric cardia. J Thorac Cardiovasc Surg 1997;114:544e51. [39] Kim DY, Joo JK, Ryu SY, Park YK, Kim YJ, Kim SK. Clinicopathological characteristics and prognosis of carcinoma of the gastric cardia. Dig Surg 2006;23: 313e8. [40] Kodama I, Kofuji K, Yano S, Shinozaki K, Murakami N, Hori H, et al. Lymph node metastasis and lymphadenectomy for carcinoma in the gastric cardia: clinical experience. Int Surg 1998;83:205e9. [41] Aikou T, Shimazu H. Difference in main lymphatic pathways from the lower esophagus and gastric cardia. Jpn J Surg 1989;19:290e5. [42] Cense HA, van Eijck CHJ, Tilanus HW. New insights in the lymphatic spread of oesophageal cancer and its implications for the extent of surgical resection. Best Pract Res Clin Gastroenterol 2006;20:893e906. [43] Cuschieri A, Fayers P, Fielding J, Craven J, Bancewicz J, Joypaul V, et al. Postoperative morbidity and mortality after D1 and D2 resections for gastric cancer: preliminary results of the MRC randomised controlled surgical trial. The Surgical Cooperative Group. Lancet 1996;347:995e9. [44] Degiuli M, Sasako M, Ponti A, Italian Gastric Cancer Study Group. Morbidity and mortality in the Italian Gastric Cancer Study Group randomized clinical trial of D1 versus D2 resection for gastric cancer. Br J Surg 2010;97:643e9. [45] Hulscher JB, Van Sandick JW, Offerhaus GJ, Tilanus HW, Obertop H, Van Lanschot JJ. Prospective analysis of the diagnostic yield of extended en bloc resection for adenocarcinoma of the oesophagus or gastric cardia. Br J Surg 2001;88:715e9. [46] Lerut T, Nafteux P, Moons J, Coosemans W, Decker G, De Leyn P, et al. Threefield lymphadenectomy for carcinoma of the esophagus and gastroesophageal junction in 174 R0 resections: impact on staging, disease-free survival, and outcome: a plea for adaptation of TNM classification in upper-half esophageal carcinoma. Ann Surg 2004;240:962e72. discussion 972e974. [47] Danish Esophagus, Cardia and Gastric Database. Annual report from 1st of January 2012 to 31st of December 2012 2012. [48] Tachimori Y, Kato H, Watanabe H, Sasako M, Kinoshita T, Maruyama K. Difference between carcinoma of the lower esophagus and the cardia. World J Surg 1996;20:507e10. discussion 511. [49] Cuschieri A, Weeden S, Fielding J, Bancewicz J, Craven J, Joypaul V, et al. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Surgical Co-operative Group. Br J Cancer 1999;79:1522e30. [50] Peyre CG, Hagen JA, DeMeester SR, Altorki NK, Ancona E, Griffin SM, et al. The number of lymph nodes removed predicts survival in esophageal cancer: an international study on the impact of extent of surgical resection. Ann Surg 2008;248:549e56. [51] Gee DW, Rattner DW. Management of gastroesophageal tumors. Oncologist 2007;12:175e85. €hrig J, Feith M, et al. Sentinel node [52] Burian M, Stein HJ, Sendler A, Piert M, Na detection in Barrett's and cardia cancer. Ann Surg Oncol 2004;11:255Se8S. [53] Moenig SP, Luebke T, Baldus SE, Schroeder W, Bollschweiler E, Schneider PM, et al. Feasibility of sentinel node concept in gastric carcinoma: clinicopathological analysis of gastric cancer with solitary lymph node metastases. Anticancer Res 2005;25:1349e52. [54] Hiratsuka M, Miyashiro I, Ishikawa O, Furukawa H, Motomura K, Ohigashi H, et al. Application of sentinel node biopsy to gastric cancer surgery. Surgery 2001;129:335e40. [55] Tokunaga M, Ohyama S, Hiki N, Fukunaga T, Yamada K, Sano T, et al. Investigation of the lymphatic stream of the stomach in gastric cancer with solitary lymph node metastasis. World J Surg 2009;33:1235e9. [56] Dresner SM, Lamb PJ, Bennett MK, Hayes N, Griffin SM. The pattern of metastatic lymph node dissemination from adenocarcinoma of the esophagogastric junction. Surgery 2001;129:103e9. [57] Gretschel S, Schlag PM. Current status of sentinel lymph node biopsy in adenocarcinoma of the distal esophagus, gastric cardia, and proximal stomach. Recent Results Cancer Res 2010;182:107e14. [58] Schiesser M, Schneider PM. Surgical strategies for adenocarcinoma of the esophagogastric junction. Recent Results Cancer Res 2010;182:93e106.