Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
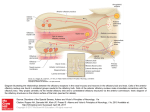
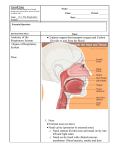
Visualization and Quantification of Nasal and Olfactory Deposition in a Sectional Adult Nasal Airway Cast Jinxiang Xi, Jiayao Eddie Yuan, Yu Zhang, Dannielle Nevorski, Zhaoxuan Wang & Yue Zhou Pharmaceutical Research An Official Journal of the American Association of Pharmaceutical Scientists ISSN 0724-8741 Volume 33 Number 6 Pharm Res (2016) 33:1527-1541 DOI 10.1007/s11095-016-1896-2 1 23 Your article is protected by copyright and all rights are held exclusively by Springer Science +Business Media New York. This e-offprint is for personal use only and shall not be selfarchived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy Pharm Res (2016) 33:1527–1541 DOI 10.1007/s11095-016-1896-2 RESEARCH PAPER Visualization and Quantif ication of Nasal and Olfactory Deposition in a Sectional Adult Nasal Airway Cast Jinxiang Xi 1 & Jiayao Eddie Yuan 2 & Yu Zhang 1 & Dannielle Nevorski 1 & Zhaoxuan Wang 1 & Yue Zhou 3 Received: 12 December 2015 / Accepted: 1 March 2016 / Published online: 4 March 2016 # Springer Science+Business Media New York 2016 ABSTRACT Purpose To compare drug deposition in the nose and olfactory region with different nasal devices and administration techniques. A Sar-Gel based colorimetry method will be developed to quantify local deposition rates. Methods A sectional nasal airway cast was developed based on an MRI-based nasal airway model to visualize deposition patterns and measure regional dosages. Four nasal spray pumps and four nebulizers were tested with both standard and point-release administration techniques. Delivered dosages were measured using a high-precision scale. The colorimetry correlation for deposited mass was developed via image processing in Matlab and its performance was evaluated through comparison to experimental measurements. Results Results show that the majority of nasal spray droplets deposited in the anterior nose while only a small fraction (less than 4.6%) reached the olfactory region. For all nebulizers considered, more droplets went beyond the nasal valve, leading to distinct deposition patterns as a function of both the nebulizer type (droplet size and initial speed) and inhalation flow rate. With the point-release administration, up to 9.0% (±1.9%) of administered drugs were delivered to the olfactory region and 15.7 (±2.4%) to the upper nose using Pari Sinus. Conclusions Standard nasal devices are inadequate to deliver clinically significant olfactory dosages without excess drug losses in other nasal epitheliums. The Sar-Gel based * Jinxiang Xi [email protected] 1 School of Engineering and Technology, Central Michigan University, 1200 South Franklin Street, Mount Pleasant, MI 48858, USA 2 Department of Mechanical Engineering, Columbia University, New York, New York, USA 3 Aerosol and Respiratory Dosimetry Program, Lovelace Respiratory Research Institute, Albuquerque, New York, USA colorimetry method appears to provide a simple and practical approach to visualize and quantify regional deposition. KEY WORDS colorimetry . intranasal delivery . nose-to-brain delivery . olfactory . point-release INTRODUCTION Neurological medications delivered to the olfactory mucosa can enter the brain via olfactory pathways and bypass the Blood–brain-Barrier (1). However, clinical applications of the direct nose-to-brain delivery are rare because of the extremely low olfactory doses using conventional nasal devices. Many challenges exist that prevent effective olfactory drug delivery. Because the olfactory nerves are located at the uppermost portion of the nose, aerosolized particles need to penetrate high and deep enough within the nose to deposit in this secluded area (Fig. 1a). Due to the complex structure of the human nasal cavity, most nasally administered drugs are filtered by the nasal valve and cannot reach the upper nose and the olfactory region. A fundamental function of the nose is the filtration of the inhaled particles as the first line of defense to airborne pollutants; however, this function also precludes effective delivery of drug particles to the superior meatus and the olfactory region. Particle deposition in the human nose has been well studied in human subjects, in vitro nasal replicas, and computational models. Despite high variabilities between subjects, these studies have consistently revealed that nasal deposition can be affected by many factors, such as the nasal devices, drug formulations, administration techniques, and patient breathing. Compared to the extensive reports of total deposition fractions (DFs) in literature, reports of deposition pattern or regional dosages were scarce. This is still the case in spite of the wellaccepted fact that local or regional deposition is more Author's personal copy 1528 Xi et al. Fig. 1 Olfactory region and nasal airway cast. (a) The olfactory (OL) mucosa is located at the uppermost of the nasal cavity and is connected directly to the brain. A nasal airway cast with a constant wall thickness was developed from an MRI-based nasal airway model. The cast was separated into different sections for measurement of regional depositions. Grooves were designed at the connections for easy assembly and good sealing. (b) The cast was also cut open to visualize and measure the location depositions inside the nose. The olfactory region was also separated and fabricated with 3D printing to measure the olfactory delivery efficiencies. clinically relevant than total deposition to predict therapeutic outcomes or assess adverse health effects. There exist established methods to measure total deposition fractions in hollow replica casts. In contrast, validated methods to visualize and quantify regional or local deposition fractions are rare. Computational models can predict deposition patterns; however, their use in clinical practices has largely been hampered due to the lack of model validation and direct correlation with medical outcomes. Moreover, because particle deposition is affected by so many factors (i.e., device-, drug-, patient-, administration-related), no single factor is commonly accepted as predictive of the deposition pattern in the nose, rendering experimental testing a necessity in validating targeted drug deliveries. Dye-based methods such as using methylene blue have been used to evaluate the regional bioequivalence of administered drugs by visually inspecting the stain intensity (2). Disadvantages of such methods include the inability of dosage quantification, solution dripping, and solution diffusion. Other studies have used gamma scintigraphy with technetium-99 m (99m Tc) labeled particles to visualize the deposition distributions in human noses (3–5) or in vitro nasal airway casts (6–8). Deposition images of the radioactive aerosols were acquired using a gamma camera and were subsequently processed to translate the color intensity into dosages. This method is known to be complicated by the attenuation of gamma rays on their way out of the body, with up to half of the photons being scattered or stopped by the body tissue (9). Photon scattering could also distort the scintigraphy image and gave a biased dosage. Typically, 30% of photons that reached by the gamma camera were scattered and caused measurement deviations. Other compounding factors include pre-study color-dosage, quality control of aerosol radiolabeling, and radioactivity recovery (10). In addition, the scintigraphy image is 2D and hence cannot differentiate depositions in multilayers. Dalby and associates developed an inexpensive and effective method to visualize and quantify droplet deposition patterns, and demonstrated the utility of this approach. Sar-Gel, a water-indicating paste (Sartomer Arkema Group, Exton, PA), changes its color from white to purple upon contact with water. Even though not very responsive to moisture in the ambient air, Kundoor and Dalby (11,12) demonstrated that Sar-Gel was highly sensitive to applied water mass and could detect water volume as low as 0.5 μL, the smallest water droplet from nasal sprays. Furthermore, color spreading by diffusion was not observed until the single drop volume exceeded 25 μL. Considering other attributes such as ease of use, fast reaction time, and easy clean up, Sar-Gel appears to be an ideal candidate to visualize droplet deposition patterns in this study. Noticing that the color change of Sar-Gel is gradual and depends on the amount of water mass, it is hypothesized that a colorimetry-water mass correlation can be established to quantify inversely the applied water mass from an image of Sar-Gel color. Various inhalation devices and administration techniques have been investigated to improve drug delivery to the olfactory region. Key factors influencing the deposition site from nasal sprays or nebulizers are droplet size, exiting velocity, administration angle, and spray plume angle. Cheng et al. (13) studied nasal spray pumps and their deposition patterns in a sectional nasal airway cast and reported that larger droplets and a wider spray angle increased the deposition in the front nose. Narrow plume angles and small droplet sizes provide larger deposition Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast beyond the nasal valve. Kundoor and Dalby (12) tested the administration angle starting from 0° all the way up to 90° in 15° increments. It was found that an angle of 60° or 75° created the most favorable trajectories in regards to depositing in the olfactory region of the nasal cavity. Wang et al. (14) developed a olfactory targeting technique by intubating a nasal spray nozzle into the nasal passage and releasing drugs underneath the olfactory region. However, this technique hasn’t gained popularity because of its invasive nature; it’s hard to insert the nozzle close to the olfactory mucosa without damaging the wall tissues. A less invasive approach was proposed by Gizurarson (15) that used a nasal pump with a narrow plume angle to transport drugs to the superior meatus and olfactory region. This method relied on a relative high pressure for drug particles to penetrate into the confined olfactory region and the enhancements of olfactory delivery were limited. A similar design termed as the Pressurized Olfactory Delivery (POD) device was put forward by Hoekman and Ho (16), which implemented swirling flows to facilitate drug particles to penetrate into the upper nose. Enhanced aerosol deposition in the olfactory region has been demonstrated in rats using this device (17). However, considering the interspecies variability in the nasal anatomy, direct extrapolation of the rat results to humans is questionable (18). One apparent anatomical disparity is the ratio of olfactorynasal area, which is about 50% in rats and is only 5.2% in humans (19). Noticing that particles deposited in the upper nose were from a certain area in the nostril, Si et al. (20) suggested a point-release technique by releasing drugs from a selected point instead of the entire area of the nostril. Significantly improved olfactory delivery efficiency has been demonstrated using this technique; however, still a substantial amount of drug particles was lost in the nasal passage, which would evoke adverse side effects. Furthermore, the delivered dosage to the disease site must be high enough to elicit therapeutic effects. Any device with an olfactory delivery efficiency less than 20%, for instance, will lose 80% medications in either the nose or the lung, and will not be able to induce noticeable outcomes in the brain without serious drug wastes in other regions. It is noted that all aforementioned devices depend solely on aerodynamic forces to transport particles, and there is no active control over the motion of particles within the nasal cavity. As a result, most particles will be filtered out in the complex nasal passages, leaving few particles that could possibly deposit in the olfactory region. This study aims to improve the olfactory delivery by testing four commercially available nasal spray pumps and four different types of nebulizers in an MRI-based nasal airway model. The deposition pattern inside the nose, as well as the total and subregional deposition fractions, will be visualized and quantified. There are four specific aims in this study: (1) to develop a sectional nasal airway cast for the visualization and quantification of local deposition, (2) to compare nasal and 1529 olfactory deposition with nasal sprays and nebulizers under normal administration conditions (entire-nostril release), (3) to test the point-release technique in nasal and olfactory deposition with four types of nebulizers, and (4) to develop a colorimetry-deposition correlation that can quantify local doses and verify its performance using experimental measurements. METHODS AND MATERIALS Nasal Airway Cast To reliably test inhalation drug delivery, anatomically accurate airway models are necessary. A nasal airway model that had been reconstructed from MRI scans of a 53-year-old male (21) was used to prepare in vitro nose replicas (Fig. 1a). This MRI dataset was initially reported in 1989 (22) and had been used since then in multiple particle deposition simulations and experiments (23–28). Magics (Materialise, Ann Arbor, MI) was used to generate the wall with a finite thickness. The nasal airway cast had a uniform wall thickness of 4 mm and a detailsize of 0.1 mm, which is the level of geometrical detail retained in the hollow cast. An in-house 3D printer (Stratasys Objet30 Pro, Northville, MI) was used to build the nose replicas. The material is polypropylene (Veroclear, Northville, MI), which is transparent and rigid, and the printing layer thickness is 16 μm (0.0006 in), leading to a smooth surface of the replicas. In order to measure regional deposition fractions, the nasal airway cast was divided into several parts that corresponded to different nose regions, such as nasal vestibule and valve, turbinate, nasopharynx, etc. (Fig. 1a). Only aerosols deposited in the vestibule-turbinate region were measured in this study. A step groove was designed at the end of each cast part for easy assembly and good sealing (Fig. 1a). The groove has a height of 2.5 mm, a width of 2.0 mm (half the wall thickness), and a clearance of 0.2 mm so that the cast parts can easily slide into each other. To visualize the deposition patterns inside the nose, the vestibule-turbinate was further divided into two parts along the top ridge of the right nasal septum to show the internal structures of the right nasal passage. From Fig. 1a, the inferior, middle, and superior turbinates can be clearly seen in the cut replica. The advantage of a cut model is that particle deposition patterns can be directly visualized. To quantitatively measure the drug dosages in the olfactory region, a region that approximates the olfactory region was cut out from the turbinate region, as shown in Fig. 1b. Nasal Spray Pumps and Nebulizers Four nasal spray products that are commonly prescribed for rhinosinusitis patients were tested in this study: Apotex, Astelin, Miaoling, and Nasonex. The spray plume angle was Author's personal copy 1530 Xi et al. measured from snapshots of the spray video-recording. Each nasal pump will be tested five times. The exit speeds were not measured in this study due to the lack of required equipment (particle image velocimetry). The output per press was quantified by measuring the weight difference of the device before and after the drug administration using an electronic balance. The dose output measurement was repeated five times for each device for later statistical analysis. The output per press was also quantified by releasing drugs into a container and measuring the container’s weight difference before and after the drug administration. Compared to quantification of spray pump output by measuring its weight loss per press, this method takes evaporation into account, which could otherwise lead to an overestimation of the device output. Four nebulizers that represent four different types of aerosol generation techniques were tested in this study: Drive Voyager Pro, Respironics Ultrasonic, Pari Sinus, and Philips Respironics 1100312 InnoSpire Essence. Drive Voyager Pro is a vibrating mesh nebulizer and will be referred to as the “mesh” nebulizer in the rest of the text. Similarly, the Respironics Ultrasonic nebulizer will be simply referred to as “ultrasonic”. Even though both techniques use ultrasonic frequencies, their aerosol generation mechanisms are different. The mesh nebulizers use ultrasonic waves to vibrate the mesh, which generates monodisperse micrometer droplets as the solution passes through it. By contrast, ultrasonic nebulizers produce aerosols by applying ultrasonic waves at the liquid surface. Philips Respironics Essence is a typical jet nebulizer with a high droplet velocity, and will be referred as “Philips” or “Jet nebulizer”. Pari Sinus is also based on the jet-flow technique, but gives a much slower output velocity. In addition, Paris Sinus has a secondary pulsating flow of 45 Hz frequency with an amplitude of 24 mbar, and was designed specifically to deliver drugs to paranasal sinuses. The operating parameters, such as aerosol size, flow output, and nebulization rate, were summarized from the device manuals and listed in Table I. The dose output of each nebulizer was measured by operating the nebulizer for a prescribed period of time and measuring the weight difference of the nebulizer before and after the operation. Each measurement was repeated five times for statistical analysis. Table I Operating Parameters of the Four Nebulizers Techniques Referred as MMDa (μm) Flow output (LPM) Nebulizing (ml/min) Intranasal Deposition Test The Schematic diagram of the intranasal deposition test is shown in Fig. 2. There are three steps: drug delivery testing, deposition rate and deposition pattern analysis, and cast cleaning dehumidification. A vacuum (Robinair 3 CFM, Warren, MI) was connected to the nasopharynx to simulate inhalations. The volumetric flow rate was monitored by an inline flow meter (Omega, FL-510, Stamford, CT). Before testing, Sar-Gel was applied to the inner surface of the nasal airway cast with a gloved finger tip in an attempt to provide an even coating. When spreading the Sar-Gel, it was important to ensure that there was a thin layer of the coating across the model and that excess Sar-Gel was wiped away. It is possible that the application method of the Sar-Gel could result in minor variations of coating thickness on the cast surface, which might lead to slightly different shades of color when applied the same water mass. However, based on our observations, such color variation was insignificant.. Photos were taken in an evenly lighted area before the nasal casts were put together and fastened with a clamp. The weight of the nasal cast (W0) was then measured using an electronic scale (Sartorious, 0.01 mg precision, Elk Grove, IL). Drug aerosols were administered into the right nostril for a specified period of time at an orientation 60° from the horizontal direction (12). The new weight of the cast was measured immediately after the drug administration (W1). The difference (ΔW = W1W2) gave the weight of deposited aerosols, and deposition rate was calculated as the ratio of ΔW to the spray/nebulizer output. The nasal airway cast was subsequently disassembled, and photos of the Sar-Gel color on the cast surfaces were taken. These images were later processed to quantify aerosol deposition rates. After each test, the Sar-Gel coating on the inner surface of the cast was washed away using a power washer (Karcher, 1600 psi, West Allis, WI). A compressed gas dryer (Craftsman 150 psi) was used to blow the residual water and moisture inside the nasal passages. The air-dried cast was then put into an oven (Thermolyne Furnatrol 18200, Dubuque, IA) set at 55°C for 60 min to remove all remaining moistures. The cast was then removed from the oven and left for another one hour to let the temperature and relative Drive voyage pro Respironics ultrasonic Pari sinus Philips respironics Innospire essence Vibrating mesh Mesh 1.0–5.0 Ultrasonic waves Ultrasonic 3.0–4.0 2.0 0.5 Jet + pulsating flow Pari Sinus 3.2, (71% < 5 μm) NA 0.22 High-velocity jet Philips or Jet 5.0 7 (max: 9.4) 0.2 MMD mass median diameter a A pulsating flow of 45 Hz with an amplitude of 20 mbar is added as a supplemental flow in Pari Sinus Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast 1531 Fig. 2 Schematic diagram of intranasal deposition test. There are three steps: (a) drug delivery testing, (b) deposition rate and deposition pattern analysis, and (c) cast cleaning dehumidification. humidity of the cast become fully equivalent to the environment. The above procedures were found to be essential to avoid the complication of water evaporation (wet surface) or hygroscopic effect (dry surface) in the deposition measurement. Large fluctuations of the electronic scale reading had been observed otherwise. Colorimetry To develop the deposition-colorimetry correlation, eight circular plates of 4 cm diameter were manufactured with the 3D printer from the same material as the nose cast. A layer of Sar-Gel was uniformly coated on the plate surface and a water mass was applied to the surface to quantify the relationship between the color depth and applied water mass for different periods of time. The resulting images were subsequently processed in Adobe Photoshop (San Jose, CA) to remove the background and analyzed in Matlab to quantify the color intensity. The test was repeated three times for each plate. A correlation was developed that can be used for deposition quantification on a regional or local basis. Statistical Analysis Minitab 17 analysis software (State College, PA) was used to analyze deposition results to determine the importance of different factors. One-Way Analysis of Variance (ANOVA) and Tukey’s method with stacked data were used to evaluate the sample variability. Results were presented as mean ± standard deviation. A difference was considered statistically significant if the pvalue was smaller than 0.05. RESULTS Deposition Using Four Nasal Spray Pumps The Sar-Gel visualization of the deposition patterns in the nasal airway cast is shown in Fig. 3 for the four nasal spray products (Miaoling, Astelin, Apotex, and Nasonex). The spray plume angles were measured as 19° ± 0.6°, 35° ± 0.8°, 33° ± 0.8°, 20° ± 0.5° for Miaoling, Astelin, Apotex, and Nasonex, respectively. Most sprays deposited in the nasal valve region. As expected, the surface deposition patterns are closely associated with the spray properties. The first product (Miaoling) has a narrow spray angle, a high exit speed, and large droplet sizes. These properties resulted in a significant portion of particles depositing in the nasal valve region. Some of the droplets that escaped the nasal valve filtration penetrated into the superior meatus and deposited in the olfactory region. For the other three spray products (Astelin, Apotex, and Nasonex), nearly all droplets were deposited in the nasal valve region, leaving no droplets to deposit in the superior meatus. The predominant nasal valve deposition of the nasal sprays was mainly due to the large droplet sizes (70–90 μm) and high droplet speeds. Dripping was observed in Miaoling and Nasonex, both of which had a narrow plume, while dripping was absent in the other two (Astelin, Apotex), which had a much wider spray plume (Figs. 3a, d vs. b, c). Particle deposition for Apotex appeared to be more dispersed than the other three sprays pumps; the “pink hue” observed in Fig. 3c for Apotex was due to particle deposition on the convex surface of the inferior and middle conchae. The unit output (per stroke) is shown in Fig. 3e. Nearly all nasal sprays discharged into the nostril were filtered out by the nasal cavity (Fig. 3f). The dosage delivered to olfactory region, as well as the ratio of the olfactory-to-nasal deposition, is shown in Author's personal copy 1532 Xi et al. Fig. 3 Deposition pattern and quantification in the nose with four nasal spray products: (a) Miaoling, (b) Astelin, (c) Apotex, and (d) Nasonex. The drug output and the deposition fraction of each press are shown in (d) and (e), respectively. Table II. The maximum deposition rate to the olfactory region was 4.6% among the four nasal spray pumps considered. Deposition Using Four Types of Nebulizers Four nebulizers that represent four different types of aerosol generation techniques were tested in this study. Slowmoving soft mists were observed in all nebulizers except the Philips, which exhibits a high-speed jet plume (Fig. 4a). For the ultrasonic nebulizer, a downward motion of droplets was observed after releasing, possibly driven by both gravity and large concentrations of the droplets. The dose outputs were qualified and compared in Fig. 4b. Linear relations and small deviations of the time-output profiles were observed for each nebulizer, indicating consistent performances. However, significant differences in the dose output were measured among the four nebulizers. For a given period of time, the ultrasonic nebulizer generated the largest amount of aerosol drugs, followed by the mesh nebulizer. The Philips and Pari Sinus generate similar amounts of aerosols, but both are much smaller in comparison to the ultrasonic or mesh nebulizers (Fig. 4b). There is almost no difference in Pari Sinus outputs with and without the vibration (pulsating flow). The development of dose-colorimetry correlation is shown in Fig. 5. The color on the plate deepens with the exposure duration time to the spray (Fig. 5a). The variation of the color intensity was (colorimetry) quantified using Matlab as a function of the exposure time, and was shown in both linear and logarithm plots (Fig. 5b). Fig. 5c displays the correlation Table II Deposition in the Nose and Olfactory Region Using Four Different Nasal Sprays Deposition (mg) Miaoling Astelin Apotex Nasonex Nasal cavity Olfactory (OL) OL-nose dose ratio 108.3 4.97 4.59% 127.7 2.27 1.78% 94.5 0.67 0.71% 93.1 0.71 0.76% Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast 1533 Fig. 4 Dose outputs of various nebulizers as a function of the release duration. (a) Aerosol patterns from different nebulizers, and (b) output quantification. Two adaptors (a cone-shaped adaptor and a plug) that were designed for nasal drug delivery are also shown in (a). between the color intensity and the applied aerosol mass, which can be expressed as: m ¼ 1:79−logðx Þ−0:677 Fig. 5 Quantification of Sar-Gel color variation using a standard nebulizer (Philips): (a) color map vs. exposure time, (b) color quantification (colorimetry), and (c) mass-colorimetry correlation. ð1Þ Figure 6a shows the total deposition fractions of the four nebulizers under three breathing conditions. The standard deviation (SD) was calculated from five trials for each nebulizer. Pari Sinus was tested in two modes: with vibration and Author's personal copy 1534 Xi et al. Fig. 6 Total deposition fraction (DF) for different nebulizers: (a) measured DF with the mass weighing approach at three inhalation flow rates, (b) comparison of DF obtained between the mass weighing and colorimetry methods at 10 L/min. without vibration. Compared to nasal sprays, the deposition fractions were much lower for nebulizers. The highest deposition fraction was 46% for the mesh nebulizer at an inhalation rate of 18 L/min. The lowest nasal deposition fraction was only 15% for the ultrasonic nebulizer during breath holding. In this study, the nebulized drug mass that was not deposited in the nasal cavity passed through the nasal cavity and exited via the nasopharynx. Interestingly, different trends were observed in light of how the deposition fraction varied with inhalation flow rate. For the mesh and ultrasonic nebulizers, the deposition fraction increased with the flow rate. In contrast, for Pari Sinus (without vibrartion) and Philips, both of which are jet nebulizers, the deposition fraction was observed to decrease with increasing flow rates. No apparent trend was observed for the Pari Sinus with vibration, indicating a more complex interaction between the airflow and pulsating aerosols. The DF was also quantified using the newly developed colorimetry method and was compared with those obtained using the mass-weigh method for the four nebulizers at 10 L/ min (Fig. 6b). It was noted that the colorimetry method persistently underestimated the direct mass weighing, but exhibited a similar trend of DF variation, indicating a qualitative match between the color- and mass-based approaches. The underestimation might partially be ascribed to the fact that some droplets deposited underneath the conchae and couldn’t be detected in the deposition images. The deposition patterns on the inner surface (turbinate side) of the right nasal passage are shown in Fig. 7 for various nebulizers and inhalation flow rates. Very different deposition patterns were observed among nebulizers, which range from highly diffusive (jet-type) to very focused (mesh nebulizer). What are the mechanisms underlying these differences? For the mesh nebulizer during breath holding, aerosol droplets are driven by inertia from the nebulizer and yield a relatively diffusive deposition pattern. Under 10 L/min, an airflow field is established within the nasal passage which entrains and transports the slow-moving aerosol droplets. The strip of deposition shown on the middle turbinate (blue arrow) is coincident with the main flow of the inhaled air. With a higher inhalation flow rate (18 L/min), more aerosol droplets were entrained into the main flow in the median passage (blue dashed ellipse). The main deposition mechanism is convection in this case as opposed to diffusion in the breath holding case. Similar patterns are observed for the ultrasonic nebulizer under 10 and 18 L/min. The absence of focused deposition in the ultrasonic nebulizer may be attributed to a lower exiting velocity and larger amount of aerosol droplets. Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast 1535 Fig. 7 Deposition pattern on the inner surface of the right nasal passage for varying nebulizers and inhalation flow rates. The deposition patterns between Pari Sinus with and without vibration look generally similar, where both exhibit more diffusive distributions than the mesh and ultrasonic nebulizers (Fig. 7c vs. d). Perceivable differences were also noted between Pari Sinus with and without vibration during breath holding and low inhalation rate (10 L/min), which was presumably attributed to the pulsating flow and a higher average velocity when the vibration is on. At 18 L/min, more droplets were deposited in the upper nose when the vibration mode was on (Fig. 7c vs. d, lower panel). Considering the Pari Sinus in Fig. 7c, the change of deposition pattern (from more diffusive during breath holding, to less diffusive at 10 L/min, to more diffusive at 18 L/min) was consistent with the variation of deposition fraction in Fig. 6a. The more diffusive deposition pattern with vibration during breath holding was caused by the larger aerosol dispersion, which was in turn induced by the flow vibrations. Considering the Philips jet nebulizer, diffusive deposition patterns were observed in Philips for all inhalation rates considered. A majority of aerosols were filtered out in the nasal vestibule and valve region under breath holding conditions (Fig. 7e). There was also appreciable deposition in the upper nose and the olfactory region. An increase in the inhalation rate, however, resulted in less deposition in the upper nose. This is because the main flow, which is at the median and lower nasal passages, entrains the inhaled particles that otherwise go to the upper part of nose. It is recalled that the drug release angle at the nostril is 30° from the vertical direction. The deposition rates in the three zones (front, upper, lower) were quantified using the colorimetry correlation (Fig. 8). The front zone represents the nasal vestibule and valve and has a one-side projected area (not the convoluted surface area) of 9.02 cm2 (Fig. 8a). The upper zone has a one-side projected area of 9.14 cm2 and depicts the middle and superior turbinate, which includes the olfactory region. The lower zone (10.42 cm2) denotes the inferior turbinate and nasal floor. The aim of this study was to enhance deposition to the upper region, in hope that more drugs can reach the olfactory region. Accordingly, the smaller the deposition fraction in the front and lower zones, the better the olfactory deposition will be. In this regard, the vibrating mesh gives the optimal results among the four nebulizers. The high deposition rates in the lower zone were presumably caused by the main flow field and/or gravity, which results in the major part of the inferior turbinate deposition. Point Release From our previous numerical studies (20,29,30), releasing aerosols to a selective point in the nostril, instead of the entire nostril, could significantly improve deposition to the superior meatus and olfactory region. Four points were tested in this study at the inhalation flow rate of 10 L/min, as illustrated in Fig. 9a. The surface deposition pattern and the sub-regional deposition fractions are shown in Fig. 9b and c, respectively. From Fig. 9b, releasing aerosols from different points gives rise to dramatically different deposition patterns, with the overall deposition shifting from the upper nose to the lower nose as the release point changes from Point 1 to Point 4. As expected, the front point release (point 1) provides the optimal deposition pattern among the points considered, with significantly reduced deposition in the front and lower nose. Figure 10 shows particle deposition with the front pointrelease for the other three nebulizers. Both sides of the right nasal passage (turbinate and septum) were shown here. No perceivable deposition in the upper nose and olfactory region was obtained using the ultrasonic nebulizer (Fig. 10a). This is because of the slow aerosol speed exiting the ultrasonic nebulizer adaptor (Fig. 10b). Instead, considerable deposition in the upper nose was obtained with both Pari Sinus and Philips jet nebulizers. The deposition in the lower nose was also greatly reduced. As the upper nose has a much larger area than the olfactory region, using the upper nose deposition fraction as the olfactory deposition will lead to a remarkable overestimation. The olfactory region was denoted by the red line (Fig. 10b, upper panel). The deposition in this region was Author's personal copy 1536 Xi et al. Fig. 8 Sub-regional deposition rates quantified with the colorimetry method: (a) areas of the sub-regions (front, upper, lower) of the nasal airway cast; (b) mesh, (b) ultrasonic, (c) Pari Sinus (with vibration), (d) Pari Sinus (without vibration), and (e) Philips (jet). There is negligible aerosol deposition in the olfactory region. quantified using the colorimetry measured by weighing the increased mass in the olfactory cast (Fig. 10b, middle panel). Pari Sinus (with vibration) gave about up to 9.0% (±1.7%) olfactory deposition fraction, while Philips gave about 6.7% (±1.2%). The olfactory deposition appeared to be insensitive Fig. 9 Point release with the mesh nebulizer: (a) four locations of the point release, (b) surface deposition patterns, (c) sub-regional deposition fractions quantified with the colorimetry method. The inhalation flow rate is 10 L/min. to the inhalation rate in both nebulizers, even though increasing the inhalation rate persistently reduced the olfactory deposition. The olfactory dosages at 10 L/min were also quantified using the colorimetry method and the results were validated against those from mass weighing, as shown in the lower Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast 1537 Fig. 10 Olfactory depositions utilizing point release approach: (a) deposition pattern and (b) olfactory deposition fraction quantified with the colorimetry method. The comparison of olfactory depositions between the colorimetry and the direct mass weighing method is shown in the lower panel of (b). panel of Fig. 10b. Good agreement was achieved between these two approaches for both Pari Sinus and Philips, even though the colorimetry approach slightly underestimated the direct measurements. DISCUSSIONS AND CONCLUSION For the four nasal sprays considered in this study, the majority of aerosol deposition occurred in the nasal vestibule-valve region. There were indeed small fractions of aerosols that penetrated into the superior meatus and deposited in the olfactory region for nasal sprays with a narrow plume. The underlying mechanism that drove aerosols to the olfactory region is the high inertia from the spray pumps, which, on the other hand, would inevitably lose most droplets to the walls of the complex nasal passages due to inertial impaction. Considering that neurological medications, such as steroids and peptides, are typically costly and can have adverse side effects on the respiratory epitheliums, the nasal spray pump does not seem to be an appropriate device for targeted olfactory drug delivery. Results from the nasal nebulizers showed substantial enhanced deposition beyond the nasal valve in comparison to the nasal spray pumps, which is consistent with the scintigraphy studies of Suman et al. (6) and Kundoor et al. (11). Among the four nebulizers, the mesh nebulizer gave the lowest deposition in the front nose and the highest in the upper nose, presumably due to the small, monodisperse droplet size and low droplet speed. On the other hand, the ultrasonic nebulizer gave the worst performance. As discussed before, even though both techniques use ultrasound, the former applies the vibration to a fine-pore mesh to drive the liquid through, whereas the latter applies the vibration to the liquid solution itself to excite droplets from the liquid interface. As a result, the sizes and distributions of the generated droplets are different (Table I). In addition, the vibrating mesh technique does not require carrier flows, and with suspending small droplets, is more controllable be means of breathing maneuvers and device adaptions. The second most optimal performances were found in Pari Sinus. This device generates somewhat similar patterns of aerosols (Fig. 4 and Table I) and has a supplemental pulsating airflow (45 Hz, 24 mbar in amplitude). Surprisingly, no substantial difference was observed in deposition rates in the upper nose using Pari Sinus with and without the pulsating flow, indicating negligible impact from the superimposed pulsating airflow in this study. Upper nose deposition using the Philips (jet) nebulizer exhibited little dependence on the inhalation flow rate, a characteristic similar to the nasal spray pump. Despite different performances among the four nebulizers, overall very low deposition rates (2.2 − 8.0%) were measured in the upper nose for all nebulizers. Negligible deposition was found in the olfactory region, which was delineated in Fig. 1b. It is acknowledged that each device has its specific recommended usage and purpose. This study was not intended to compare which device is superior when operated as recommended, but rather to test these devices as candidates with new delivery protocols for a new purpose, i.e., to deliver aerosols to the olfactory region. Author's personal copy 1538 The point-release administration technique leverages the interplay between the air flow and particle motion in the nose, and selectively releases particles that are most likely to penetrate into the olfactory region. With the optimized releasing position, flow condition, and particle properties, much enhanced olfactory deposition is expected, which further improves therapeutic outcomes and minimizes adverse systematic side effects. With the point-release technique, up to 9.0% (±1.7%) of administered aerosols were deposited in the olfactory region, leading to an order of magnitude increase relative to the standard (entire-nostril) administration. Considering that a treatment will be effective only if sufficient drug is delivered directly to the required site, it is anticipated that a clinically relevant olfactory dosage is possible only with excessive drug loss by using standard devices such as nebulizers. Olfactory dosage is not only sensitive to the nose architecture and to delivery devices, but also to the definition of the olfactory region. It is generally accepted that the olfactory mucosa is located on top of the superior meatus, but there is no consensus on the exact location and the area where drug molecules can be effectively absorbed into the brain. This lack of consensus makes it difficult to compare results between different studies. The reported area of the olfactory region varied dramatically, ranging from 5.0 cm2 (31), 6.8 cm2 (19), 10 cm2 (32), to 35 cm2 (33). There are also biopsy studies suggesting that olfactory nerves extend 1–2 cm beyond the olfactory cleft (34). The area available for the nose-to-brain transport may be larger than the often cited 3–8% of the nasal mucosa from cadaver studies (35). Previous studies have defined the extent and location of the olfactory region in different ways. A crescent-shaped olfactory region was defined in Si et al. (20) and Shi et al. (36) at the very top of the superior meatus. In contrast, gamma scintigraphy studies often prescribed the upper nose to be equivalent to the olfactory region (37–40). Recently, Schroeter et al. (33) measured particle deposition in a nose model and reported a maximum olfactory deposition rate of 5% at a particle size of 10.3 μm. The olfactory region was defined as the dorsal posterior region of the upper nose, as depicted in Fig. 11. In contrast, Wang et al. (14) reported an astounding 73.5% deposition rate in the olfactory region in a nose model that was divided into three portions (i.e., lower, middle, top), with the top purported as the olfactory region. However, the model realism and the quantification method of regional deposition in an enclosed cavity were not provided in the above study. The seemingly unrealistic olfactory deposition rate from a nasal pump highlights the importance of the anatomical accuracy of the nose model in olfactory dosimetry studies. To demonstrate the influence of the olfactory extent and area, we quantified the olfactory dosages based on four different olfactory definitions using the colorimetry approach, as illustrated in Fig. 11. Significant discrepancies were obtained, with a factor of 6.5 between the maximum and minimum olfactory dosages (15.7% vs. 2.4%). Xi et al. Furthermore, the olfactory dosages differ at a factor of 2.9 for case B and C (7.7% vs. 2.7%), which have a similar area but different locations. The deposition is extremely low or zero at the very top of nose and increases as it is moving away from the top. This deposition increase makes the olfactory doses highly dependent on the increased areas. A slight over delineation of the olfactory boundary may cause a disproportional increase in olfactory dosage. As a result, a guideline for the olfactory position and extent is needed for future olfactory dosimetry studies in general, and for the outcome report of newly developed olfactory delivery devices in particular. It is also noted that the nerve filaments are not evenly distributed in the olfactory region, presumably having more nerves (and quicker absorption) in the top olfactory cleft and less in the peripheral regions. It is arguably assumed that the rate of nose-to-brain transport of drug molecules is heterogeneous across the olfactory region. A new colorimetry-based method to quantify regional or local deposition rate was proposed and calibrated with complementary in vitro measurements in this study. The working principle of this method is that a quantitative correlation exists between the color change of Sar-Gel and the mass of applied aerosol droplets. Compared to the mass weighing method, the colorimetry method consistently under-predicted the deposition rates by 32% (±4%) (Fig. 6b). As a result, adding a correction factor (for instance, 1.52) to Eq. 1 can be used in the colorimetry correlation to account for the systematic underestimation, such as, m ¼ 2:72−1:52⋅logðx Þ−0:677 ð2Þ Compared to gamma scintigraphy, the Sar-Gel based method has the following advantages: a constant formulation may be used, no radiolabeling is required, and it is simple, direct, and less expensive. It is acknowledged that the colorimetry method proposed in this study necessitates the usage of the same material for deposition-colorimetry correlation development and deposition quantification. The lighting environment should also be the same to avoid image color distortion. Another limitation of this color-based method is that it only quantifies visible aerosols. Aerosols that are deposited under the nasal conchae or occluded by other structures have been neglected. The multi-sectional nasal casting, in combination with the Sar-Gel colorimetry approach, was demonstrated to provide a practical approach to visualize and quantify local depositions in the nasal airway. Advances of imaging and manufacturing technologies provide more control on cast preparation. An anatomically accurate nasal airway model that was previously reconstructed from MRI scans (21,41,42) was used to develop the hollow cast of the nasal airway by the means of stereolithographic and 3D rapid prototyping. To characterize the deposition patterns, the right nasal passage was incised Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast 1539 Fig. 11 Comparison of the olfactory deposition fractions based on different regions that had been referred to as the olfactory region: (a) upper nose, (b) superior meatus, (c) superior-posterior meatus, and (d) superior meatus (apex). The colorimetry-quantified deposition fractions in the four regions are compared in (e). into two parts (septum and turbinate) along the top ridge, which clearly unveiled the complex structure of the nasal turbinate (Fig. 1b). This cut-open nose cast had a unique advantage in the visualization and quantification of local depositions within the nose, whose small size and labyrinthine passage make it inaccessible to most measuring instruments. By separating the nasal septum from the turbinate, aerosol deposition patterns inside the nose can be directly displayed using colorchanging gels or fluorescent particles. To directly measure the delivery efficiency to the olfactory region, this region was separated from the main nasal cavity and was fabricated separately into two parts via 3D printing (Fig. 1b, right panel). The projected area (not the surface area) of the olfactory region is approximately 5.4 mm2. In comparison, Gamma scintigraphy has also been implemented to visualize and quantify the deposition pattern inside the nose. However, it generates a 2D image of varying brightness depending on the particle concentrations in the camera direction. As a result, it cannot differentiate depositions on different walls that overlap in that direction. Another setback of the gamma scintigraphy is that the perceptiveness of the radioactive particles can be influenced by the distance from the camera and by the physical properties of the nasal tissues/bones. Furthermore, radioactive substances are used. Even through proven to be nearly harmless, they are not readily available, need professional handling, and are generally costly. Assumptions that may limit the realism of this study include the usage of steady flows, a rigid nasal airway cast, and cast replicas based on one subject. Previous studies have emphasized the effect upon the airflow and aerosol dynamics from tidal breathing (43) and compliant walls (44). The nose replicas were developed from one subject only and did not account for discrepancies due to age, gender, race, weight, or height. Considering the potential effect of droplet inertia on nasal deposition, it was desirable to know the magnitude of the spray exit velocities from each pump. However, these velocities were not quantified in this study due to the lack of required equipment. Inthavong et al. (45,46) measured spray velocities in different spray regions using particle image velocimetry and reported an average spray velocity of 15 m/s. Kimbell et al. (47) reported average spray velocities ranging from 1.5 to 14.7 m/s that were measured using laser diffraction, high-speed video, and high-speed spark photography. Complementary numerical studies with more extensive and physiologically realistic test conditions are needed to gain further insights into the observations in this study, and to improve the drug delivery system for targeted olfactory drug delivery. In conclusion, four nasal spray pumps and four nebulizers based on different aerosol-generation techniques were tested with various delivery protocols to improve aerosol deposition in the olfactory region. Results show that standard nasal devices appear to be inadequate to achieve clinically significant deposition rate with the protocols tested in this study. It is anticipated that protocols relying on aerodynamic forces and aerosol inertia will fail due to the complete lack of control of the droplet motions and due to the convoluted paths leading from the nostril to the olfactory region concealed in the uppermost nasal cavity. New delivery techniques are needed that can help aerosol drugs to maneuver through the labyrinthine nasal passages with minimum loss to the anterior and turbinate epitheliums. ACKNOWLEDGMENTS AND DISCLOSURES The authors report no conflicts of interest in this work. REFERENCES 1. 2. Born J, Lange T, Kern W, McGregor GP, Bickel U, Fehm HL. Sniffing neuropeptides: a transnasal approach to the human brain. Nat Neurosci. 2002;5(6):514–6. Valentine R, Athanasiadis T, Thwin M, Singhal D, Weitzel EK, Wormald PJ. A prospective controlled trial of pulsed nasal nebulizer in maximally dissected cadavers. Am J Rhinol. 2008;22(4):390–4. Author's personal copy 1540 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Xi et al. Moller W, Schuschnig U, Celik G, Munzing W, Bartenstein P, Haussinger K, et al. Topical drug delivery in chronic rhinosinusitis patients before and after sinus surgery using pulsating aerosols. PLoS ONE. 2013;8(9):e74991. Djupesland PG, Skretting A, Winderen M, Holand T. Breath actuated device improves delivery to target sites beyond the nasal valve. Laryngoscope. 2006;116(3):466–72. Washington N, McGlashan JA, Jackson SJ, Bush D, Pitt KG, Rawlins DA, et al. The effect of nasal patency on the clearance of radiolabeled saline in healthy volunteers. Pharm Res. 2000;17(6): 733–6. Suman JD, Laube BL, Lin TC, Brouet G, Dalby R. Validity of in vitro tests on aqueous spray pumps as surrogates for nasal deposition. Pharm Res. 2002;19(1):1–6. Guo Y, Laube B, Dalby R. The effect of formulation variables and breathing patterns on the site of nasal deposition in an anatomically correct model. Pharm Res. 2005;22(11):1871–8. Laube BL, Sharpless G, Shermer C, Nasir O, Sullivan V, Powell K. Deposition of albuterol aerosol generated by pneumatic nebulizer in the Sophia Anatomical Infant Nose-Throat (SAINT) model. Pharm Res. 2010;27(8):1722–9. Fleming JS, Conway JH, Bolt L, Holgate ST. A comparison of planar scintigraphy and SPECT measurement of total lung deposition of inhaled aerosol. J Aerosol Med. 2003;16(1):9–19. Bondesson E, Bengtsson T, Borgstrom L, Nilsson LE, Norrgren K, Trofast E, et al. Planar gamma scintigraphy–points to consider when quantifying pulmonary dry powder aerosol deposition. Int J Pharm. 2003;258(1–2):227–40. Kundoor V, Dalby RN. Assessment of nasal spray deposition pattern in a silicone human nose model using a color-based method. Pharm Res. 2010;27(1):30–6. Kundoor V, Dalby RN. Effect of formulation- and administrationrelated variables on deposition pattern of nasal spray pumps evaluated using a nasal cast. Pharm Res. 2011;28(8):1895–904. Cheng YS, Holmes TD, Gao J, Guilmette RA, Li S, Surakitbanharn Y, et al. Characterization of nasal spray pumps and deposition pattern in a replica of the human nasal airway. J Aerosol Med Pulm D. 2001;14(2):267–80. Wang J, Bentz J, Anderson R. Nasal device for delivery to the olfactory region. Patent: US 20070119451 A1; 2007. Gizurarson S. A method for administration of active substances to the olfactory region. Patent: CA 2298596 A1; 1999. Hoekman JD, Ho RJY. Effects of localized hydrophilic mannitol and hydrophobic nelfinavir administration targeted to olfactory epithelium on brain distribution. AAPS PharmSciTech. 2011;12(2):534–43. Hoekman JD, Ho RJY. Enhanced analgesic responses after preferential delivery of morphine and fentanyl to the olfactory epithelium in rats. Anesth Analg. 2011;113(3):641–51. Corley RA, Kabilan S, Kuprat AP, Carson JP, Minard KR, Jacob RE, et al. Comparative computational modeling of airflows and vapor dosimetry in the respiratory tracts of rat, monkey, and human. Toxicol Sci. 2012;128(2):500–16. Xi J, Kim J, Si XA, Corley RA, Zhou Y. Modeling of inertial depositions in scaled models of rat and human nasal airways: towards in vitro regional dosimetry in small animals. J Aerosol Sci. 2016; Accepted. Si X, Xi J, Kim J, Zhou Y, Zhong H. Modeling of release position and ventilation effects on olfactory aerosol drug delivery. Respir Physiol Neurobiol. 2013;186(1):22–32. Xi J, Longest PW. Characterization of submicrometer aerosol deposition in extrathoracic airways during nasal exhalation. Aerosol Sci Technol. 2009;43(8):808–27. Guilmette RA, Wicks JD, Wolff RK. Morphometry of human nasal airways in vivo using Magnetic Resonance Imaging. J Aerosol Med. 1989;2(4):365–77. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. Cheng KH, Cheng YS, Yeh HC, Swift DL. Deposition of ultrafine aerosols in the head airways during natural breathing and during simulated breath-holding using replicate human upper airway casts. Aerosol Sci Technol. 1995;23(3):465–74. Kelly JT, Asgharian B, Kimbell JS, Wong B. Particle depositon in human nasal airway replicas manufactured by different methds. Part I: Inertial regime particles. Aerosol Sci Technol. 2004;38: 1063–71. Schroeter JD, Kimbell JS, Asgharian B. Analysis of particle deposition in the turbinate and olfacotry regions using a human nasal computational fluid dynamics model. J Aerosol Med. 2006;19(3): 301–13. Xi J, Berlinski A, Zhou Y, Greenberg B, Ou X. Breathing resistance and ultrafine particle deposition in nasal-laryngeal airways of a newborn, an infant, a child, and an adult. Ann Biomed Eng. 2012;40(12):2579–95. Kimbell JS, Subramaniam RP. Use of computational fluid dynamics models for dosimetry of inhaled gases in the nasal passages. Inhal Toxicol. 2001;13(5):325–34. Subramaniam RP, Richardson RB, Morgan KT, Kimbell JS, Guilmette RA. Computational fluid dynamics simulations of inspiratory airflow in the human nose and nasopharynx. Inhal Toxicol. 1998;10(2):91–120. Xi J, Si X, Kim JW, Berlinski A. Simulation of airflow and aerosol deposition in the nasal cavity of a 5-year-old child. J Aerosol Sci. 2011;42(3):156–73. Xi J, Si X, Gaide R. Electrophoretic particle guidance significantly enhances olfactory drug delivery: a feasibility study. PLoS One. 2014;9(1):e86593. Gizurarson S. Anatomical and histological factors affecting intranasal drug and vaccine delivery. Curr Drug Deliv. 2012;9(6):566– 82. Landis MS, Boyden T, Pegg S. Nasal-to-CNS drug delivery: where are we now and where are we heading? An industrial perspective. Ther Deliv. 2012;3(2):195–208. Schroeter JD, Tewksbury EW, Wong BA, Kimbell JS. Experimental measurements and computational predictions of regional particle deposition in a sectional nasal model. J Aerosol Med Pulm Drug Deliv. 2015;28(1):20–9. Djupesland PG, Messina JC, Mahmoud RA. The nasal approach to delivering treatment for brain diseases: an anatomic, physiologic, and delivery technology overview. Ther Deliv. 2014;5(6):709–33. Leopold DA, Hummel T, Schwob JE, Hong SC, Knecht M, Kobal G. Anterior distribution of human olfactory epithelium. Laryngoscope. 2000;110(3):417–21. Shi H, Kleinstreuer C, Zhang Z. Laminar airflow and nanoparticle or vapor deposition in a human nasal cavity model. J Biomech Eng. 2006;128:697–706. Sengoku R, Matsushima S, Bono K, Sakuta K, Yamazaki M, Miyagawa S, et al. Olfactory function combined with morphology distinguishes Parkinson’s disease. Parkinsonism Relat Disord. 2015;21(7):771–7. Shiga H, Taki J, Okuda K, Watanabe N, Tonami H, Furukawa M, et al. Prognostic value of olfactory nerve assessment with olfactoscintigraphy in patients with olfactory disorders. Chem Senses. 2015;40(7):643–4. Kikuchi A, Baba T, Hasegawa T, Sugeno N, Konno M, Aoki M, et al. Differentiating Parkinson’s disease from multiple system atrophy by I-123 meta-iodobenzylguanidine myocardial scintigraphy and olfactory test. Mov Disord. 2013;28:S156. Prado GL, Itabashi Y, Noda H, Miura H, Mariya Y, Abe Y. Olfactory neuroblastoma visualized by Technetium-99m-ECD SPECT. Radiat Med. 2001;19(5):267–70. Xi J, Longest PW. Numerical predictions of submicrometer aerosol deposition in the nasal cavity using a novel drift flux approach. Int J Heat Mass Transf. 2008;51(23–24):5562–77. Author's personal copy Quantification of Olfactory Deposition in an Nasal Airway Cast 42. 43. 44. Si X, Xi J, Kim J. Effect of laryngopharyngeal anatomy on expiratory airflow and submicrometer particle deposition in human extrathoracic airways. Open J Fluid Dyn. 2013;3(4):286–301. Xi J, Longest PW, Martonen TB. Effects of the laryngeal jet on nano- and microparticle transport and deposition in an approximate model of the upper tracheobronchial airways. J Appl Physiol. 2008;104(6):1761–77. Berg EJ, Weisman JL, Oldham MJ, Robinson RJ. Flow field analysis in a compliant acinus replica model using particle image velocimetry (PIV). J Biomech. 2010;43(6):1039–47. 1541 45. Inthavong K, Fung MC, Tong X, Yang W, Tu J. High resolution visualization and analysis of nasal spray drug delivery. Pharm Res. 2014;31(8):1930–7. 46. Inthavong K, Yang W, Fung MC, Tu JY. External and near-nozzle spray characteristics of a continuous spray atomized from a nasal spray device. Aerosol Sci Technol. 2012;46(2):165–77. 47. Kimbell JS, Segal RA, Asgharian B, Wong BA, Schroeter JD, Southall JP, et al. Characterization of deposition from nasal spray devices using a computational fluid dynamics model of the human nasal passages. J Aerosol Med Pulm D. 2007;20(1):59–74.