Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
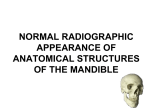
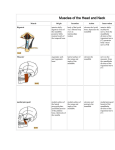
Contents Introduction History Indications Advantages Disadvantages Principles of panoramic image formation Rotation center Focal trough Equipment Step by step procedures Common errors Normal anatomic landmarks of maxilla Normal anatomic landmarks of mandible Air space images seen on panoramic radiographs Soft tissue images seen on panoramic radiographs Introduction Panoramic radiography is an extraoral radiographic technique that is used to examine the upper and lower jaws on a single film. This is a curvilinear variant of conventional tomography and is also based on the principle of reciprocal movement of an x-ray source and an image receptor around a central plane, called the image layer, in which the object of interest is located. The movement of the film and tubehead produces an image through the process known as tomography. The term tomo means section; tomography is a radiographic technique that allows the imaging of one layer or section of the body while blurring images from structures in other planes. History • Dr H Numata of Japan in 1933 and later, Dr YV Paatero of Finland in 1948 first gave the techniques of rotational panoramic radiography. • In 1985, Kashima et al reported the implementation of computed panoramic radiography. • Later, McDavid et al introduced direct digital panoramic imaging using a linear array of silicon photodiodes. Indications 1. To evaluate impacted teeth. 2. To evaluate eruption patterns, growth and development. 3. To detect diseases, lesions and conditions of jaws. 4. To determine the extent of large lesions. 5. To evaluate trauma Advantages 1. Broad coverage of facial bones and teeth. 2. Low patient radiation dose. 3. Convenience of examination for the patient. 4. Ability to be used in patients unable to open their mouth. 5. Short time required to make a panoramic image, usually in the range of 3 to 4 minutes. 6. Patient’s ready understandability of panoramic films, making them a useful visual aid in patient education and case presentation. Disadvantages 1. Does not display fine anatomic detail available on intraoral periapical radiographs. So not useful in detecting small carious lesions, fine structure of marginal periodontium, or periapical disease. 2. Unequal magnification and geometric distortion across the image. 3. Occasionally the presence of overlapping structures, such as cervical spine, can hide the odontogenic lesions, particularly in the incisor region. 4. Clinically important objects may be situated outside the plane of focus and may appear distorted or not present at all. Principles of panoramic image formation In panoramic radiography the film and x-ray tubehead move around the patient. The x-ray tube rotates around the patient’s head in one direction while the film rotates in the opposite direction. The patient may stand or sit in a stationary position, depending on the type of panoramic x-ray machine that is used. During exposure cycle, the machine automatically shifts to one or more additional centers of rotation. The rate of movement of receptor behind the lead collimator slit is regulated to be the same as that of the central ray sweeping through the dental structures on the side of the patient nearest the receptor. Structures on the opposite side of the patient (near the x-ray tube) are distorted and appear out of focus because x-ray beam sweeps through them in the direction opposite that in which the image receptor is moving. In addition, structures near the x-ray source are so magnified (and their borders so blurred) that they are not seen as discrete images on the resultant image. These structures only appear as diffuse phantom or ghost images. Because of both these circumstances, only structures near the receptor are usefully captured on the resultant image. Structures located more centrally in the body relative to the jaws, such as hyoid bone and epiglottis, appear on the right, left and sometimes central areas of final image. Rotation center In panoramic radiography, the film or cassette carrier and x-ray tubehead are connected and rotate simultaneously around a patient during exposure. The pivotal point, or axis, around which the cassette carrier and x-ray tubehead rotate is termed a rotation center. Depending on the manufacturer, the number and location of rotational canters differ. Three rotation centers used in the panoramic x-ray machines are as follows: 1. Double center rotation 2. Triple center location 3. Moving center rotation Double center rotation: there are two centers of rotation. One is for the right and one for the left side of the jaws. Triple center rotation: there are three center of rotation and create an uninterrupted radiographic image of the jaws. Moving center rotation: machine rotate around a continuously moving center that is similar to the arches, creating an uninterrupted image of the jaws. Focal trough (image layer) In panoramic radiography, the focal trough is a theoretical concept used to determine where the dental arches must be positioned to achieve the clearest image. The focal trough can be defined as a three-dimensional curved zone in which structures are clearly demonstrated on a panoramic radiograph. The structures located within the focal trough appear reasonably well defined on the resulting panoramic radiograph. The structures located inside or outside of the focal trough appear blurred or indistinct and are not readily visible on the panoramic film. The shape of the image layer varies with the brand of equipment used. The factors that affect its size are variables that influence image definition: arc path, velocity of the receptor and xray tubehead, alignment of the x-ray beam, and collimator width. The closer the rotation center is to the teeth, the narrower the focal trough. In most panoramic x-ray machines, the focal trough is narrow in the anterior region and wide in the posterior region. Equipment Equipment includes: 1. Panoramic x-ray unit 2. Screen films 3. Intensifying screens 4. Cassette Panoramic x-ray unit: The main components of the panoramic unit include the following: 1. X-ray tubehead 2. Head positioner 3. Exposure controls X-ray tubehead: similar to an intraoral x-ray tubehead. Each has a filament used to produce electrons and a target used to produce x-rays. Collimator: the collimator used in the panoramic x-ray machine is a lead plate with an opening in the shape of a narrow vertical slit. The function of collimator is to restrict the size and shape of the x-ray beam. The narrow x-ray beam that emerges from the collimator minimizes patient exposure to x-radiation. Head positioner: it consists of a chin rest, notched bite-block, forehead rest, and lateral head supports or guides. Exposure factors: the milliamperage and kilovoltage settings are adjustable and can be varied to accommodate patients of different sizes. The exposure time, however, is fixed and cannot be changed. Screen film: Screen film is used in panoramic radiography. This film is sensitive to the light emitted from intensifying screens. A screen film is placed between two intensifying screens in a cassette holder. When the cassette holder is exposed to x-rays, the screens convert the xray energy into light, which in turn exposes the screen film. Some screen films are sensitive to green light whereas others are sensitive to blue light. The film used in panoramic radiography is available in two sizes: 5x12 inch and 6x12 inch. Intensifying screens: Two basic types of intensifying screens: calcium tungstate and rare earth. Calcium tungstate screens emit blue light, and rare earth screens emit green light. Rare earth screens require less x-ray exposure than calcium tungstate screens and are considered ‘faster.’ Cassette: It is the device that is used to hold the extraoral film and intensifying screens. The cassette may be rigid or flexible, curved or straight, depending on the panoramic x-ray unit. All cassettes must be ‘light-tight’ to protect the film from exposure. The cassette must be marked to orient the finished the radiograph. Before exposure, a metal letter “R” can be attached to the front of cassette to indicate the patient’s right side; the letter “L” is used to identify the patient’s left side. Step by step procedures Equipment preparation: 1. Load the panoramic cassette in the darkroom under the safelight condition. 2. Cover the bite-block with a disposable plastic coverslip. 3. Set the exposure factors (kilovoltage, milliamperage) according to the manufacturer’s recommendations. Patient preparation: 1. Place a lead apron, without a thyroid collar, on the patient and secure it. A doublesided apron is recommended. 2. Remove all objects from the head and neck area that may interfere with film exposure. The patient must remove eyeglasses, earrings, necklaces, napkin chains, hearing aids, hairpins, and complete and partial dentures. Patient positioning: 1. Instruct the patient to stand or sit with the back straight and erect. 2. Instruct the patient to bite on the bite-block. The upper and lower front teeth must be placed in an end to end position in the groove (notch) that is found on the bite-block. This groove is used to align the teeth in focal trough. 3. Position the midsagittal plane perpendicular to the floor. The patient’s head must not be tipped or tilted. 4. Position the Frankfort plane parallel with the floor. 5. Instruct the patient to position the tongue on the roof of the mouth. 6. After the patient has been positioned, instruct the patient to remain still while the machine is rotating during exposure. 7. Expose the film and proceed with film processing. Common errors Patient preparation errors: Ghost images Ghost images: ghost image is a radiopaque artifact seen on a panoramic film that is produced when a radiodense object is penetrated twice by the x-ray beam. A ghost image resembles its real counterpart and is found on the opposite side of the film; it appears indistinct, larger, and higher than its actual counterpart. It occurs when metallic or radiodense objects (eyeglasses, earrings, necklaces, hairpins, removable partial dentures, complete dentures, orthodontic retainers, hearing aids) are not removed before the exposure is made. Solution: instruct the patient to remove all radiodense objects in the head and neck region before positioning the patient. Lead apron artifact: if the lead apron is incorrectly placed, or if a lead apron with a thyroid collar is used during the exposure, a radiopaque cone-shaped artifact results. Solution: always use a lead apron without a thyroid collar. The lead apron must be placed low around the neck of the patient so that it does not block the x-ray beam. Patient positioning errors: Teeth placed too posterior on bite-block Positioning of Frankfort plane upward: if the patient’s chin is positioned too high or tipped up, the Frankfort plane is angled upward, and the following results1. The hard palate and floor of the nasal cavity appear superimposed over the roots of the maxillary teeth. 2. There is a loss of detail in the maxillary incisor region. 3. The maxillary incisors appear blurred and magnified. 4. A “reverse smile line” (curved downward) is apparent on the radiograph. Solution: carefully position the patient so that the Frankfort plane is parallel with the floor. Positioning the Frankfort plane downward: if the patient’s chin is positioned too low or is tipped down, the Frankfort plane is angled downward and following results1. The mandibular incisors appear blurred. 2. There is a loss of detail in the anterior apical regions. 3. The mandibular condyles may not be visible. 4. An “exaggerated smile line” (curved upward) is apparent on the radiograph. Solution: carefully position the patient so that the Frankfort plane is parallel with the floor. Positioning of teeth anterior to focal trough: If the patient’s anterior teeth are positioned too far forward on the bite-block or anterior to the focal trough, the anterior teeth appear “skinny” and out of focus on the radiograph. Solution: position the patient so that the anterior teeth are placed in an end to end position in groove on the bite-block. Positioning of teeth posterior to focal trough: if the patient’s teeth are positioned too far back on the bite-block or posterior to the focal trough, the anterior teeth appear “fat” and out of focus on the radiograph. Solution: position the patient so that anterior teeth are placed in an end to end position in the groove on the bite-block. Positioning of midsagittal plane: if the patient’s head is not centered, the ramus and posterior teeth appear unequally magnified on the panoramic radiograph. The side farthest from the film appears magnified, and the side closest to the film appears smaller. Solution: position the patient’s head so that the midsagittal plane is perpendicular to the floor while the midline is centered on the bite-stick. Positioning of spine: if patient is not standing or sitting with a straight spine, the cervical spine, the cervical spine appears as a radiopacity in the center of the film and obscures diagnostic information. Solution: instruct the patient to stand or sit “as tall as possible” with a straight back. Miscellaneous problems: Static electricity: Static electricity appears as black lines or dots on the film, often having a tree-branch appearance. It is caused by removing the film from the box or cassette too quickly, creating static discharge. Failure to remove appliances: Failure to remove complete upper denture before exposure. Failure to remove glasses Slight movement of the patient Double exposure Normal anatomic landmarks of maxilla Normal anatomic landmarks of maxilla and surrounding structures: 1. mastoid process, 2. styloid process, 3. external auditory meatus,4. glenoid fossa, 5. articular eminence, 6. lateral pterygoid plate, 7. pterygomaxillary fissure, 8. maxillary tuberosity, 9. infraorbital foramen, 10. orbit, 11. incisive canal, 12. incisive foramen, 13. anterior nasal spine, 14. nasal cavity, 15. nasal septum, 16. hard palate, 17. maxillary sinus, 18. floor of maxillary sinus, 19. zygomatic process of maxilla, 20. zygomatic arch, 21. hamulus Mastoid process: it is a marked prominence of bone located posterior and inferior to the temporomandibular joint(TMJ). Radiographic appearance: it appears as a rounded radiopacity located posterior and inferior to tha TMJ area. It is not seen on periapical radiograph. External auditory meatus: it is a hole or opening in the temporal bone located superior and anterior to the mastoid process. Radiographic appearance: it appears as a round to ovoid radiolucency anterior and superior to the mastoid process. The external auditory meatus is not seen on the periapical radiographs. Styloid process: it is a long, pointed, and sharp projection of bone that extends downward from the inferior surface of the temporal bone anterior to the mastoid process. Radiographic appearance: on a panoramic radiograph, it appears as a long radiopaque spine that extends from the temporal bone anterior to the mastoid process. It is not seen on periapical radiograph. Glenoid fossa: also known as mandibular fossa. It is a concave, depressed area of the temporal bone. The mandibular condyle rests in the glenoid fossa. The glenoid fossa is located anterior to the mastoid process and external auditory meatus. Radiographic appearance: it appears as a concave radiopacity superior to the the mandibular condyle. The glenoid fossa is not seen on periapical radiographs. Articular eminence: also known as articular tubercle. It is a rounded projection of the temporal bone located anterior to the glenoid fossa. Radiographic appearance: it appears as a rounded radiopaque projection of the bone located anterior to the glenoid fossa. It is not seen on the periapical radiographs. Lateral pterygoid plate: it is a wing shaped bony projection of the sphenoid bone located distal to the maxillary tuberosity region. Radiographic appearance: it appears as a radiopaque projection of bone distal to the maxillary tuberosity region. It is not seen on periapical radiographs. Pterygomaxillary fissure: it is a narrow space or cleft that separates the lateral pterygoid plate and the maxilla. Radiographic appearance: it appears as a radiolucent area between the lateral pterygoid plate and the maxilla. The zygoma is often superimposed on this region and obscures the pterygomaxillary fissure. This is not seen on periapical radiographs. Maxillary tuberosity: it is a rounded prominence of bone that extends posterior to the third molar region. Radiographic appearance: it appears as a radiopaque bulge distal to the third molar region. Infraorbital foramen: it is a hole or opening in bone found inferior to the border of the orbit. Radiographic appearance: the infraorbital foramen appears as a round or ovoid radiolucency inferior to the orbit. It may be superimposed over the maxillary sinus. It is not seen on the peripaical radiograph. Orbit: it is the bony cavity that contains the eyeball. Radiographic appearance: it appears as a round radiolucent compartment with radiopaque borders located superior to the maxillary sinuses. On most panoramic radiographs, only the inferior border of the orbit is visible, where it appears as a radiopaque line. Incisive canal: also known as nasopalatine canal. It is a passageway through bone that extends from the superior foramina of incisive canal to the incisive foramen. Radiographic appearance: the incisive canal appears as a tube like radiolucent area with radiopaque borders. It is located between the maxillary central incisors. Incisive foramen: also known as nasopalatine foramen. It is an opening or hole in bone that is located at the midline of the anterior of the hard palate directly posterior to the maxillary central incisors. Radiographic appearance: it appears as a small, ovoid or round radiolucency located between the roots of the maxillary central incisors. Anterior nasal spine: it is a sharp bony projection of the maxilla located at the anterior and inferior portion of the nasal cavity. Radiographic appearance: it appears as a V-shaped radiopaque area located at the intersection of the floor of the nasal cavity and the nasal septum. Nasal cavity: also known as nasal fossa. It is a pear shaped compartment of bone located superior to the maxilla. Radiographic appearance: it appears as a large radiolucent area above the maxillary incisors. Nasal septum: it is a vertical bony wall or partition that divided the nasal cavity into the right and left nasal fossae. Radiographic appearance: it appears as a vertical radiopaque partition that divides the nasal cavity. Hard palate: it is the bony wall that separates the nasal cavity from the oral cavity. Radiographic appearance: it appears as a horizontal radiopaque band superior to the apices of the maxillary teeth. Maxillary sinus and floor of maxillary sinus: the maxillary sinuses are paired cavities or compartments of bone located within the maxilla and are located above the maxillary premolar and molar teeth. Radiographic appearance: the maxillary sinuses appear as paired radiolucent areas located above the apices of the maxillary premolars and molars. The floor of the maxillary sinus is composed of dense cortical bone and appears as a radiopaque line. Zygomatic process of maxilla: it is a bony projection of the maxilla that articulates with the zygoma, or malar bone. Radiographic appearance: it appears as a J- or U-shaped radiopacity located superior to the maxillary first molar region. Zygoma: also known as malar process. It is the cheek bone and articulates with the zygomatic process of the maxilla. Radiographic appearance: it appears as a radiopaque band that extends posteriorly from the zygomatic process of the maxilla. Hamulus: also known as hamular process. It is a small, hook like projection of bone that extends from the pterygoid plate of the sphenoid bone. Radiographic appearance: it appears as a radiopaque hook like projection posterior to the maxillary tuberosity area. Normal anatomic landmarks of mandible Normal anatomic landmarks of mandible and surrounding structures: 1. condyle, 2. coronoid notch 3. coronoid process, 4. mandibular foramen, 5. lingula, 6. mandibular canal, 7. mental foramen, 8. hyoid bone, 9. mental ridge, 10. mental fossa, 11. lingual foramen, 12. genial tubercle, 13. inferior border of mandible, 14. mylohyoid ridge, 15. internal oblique ridge, 16. external oblique ridge Mandibular condyle: it is a rounded projection of bone extending from the posterior superior border of the ramus of the mandible. The mamndibular condyle articulates with the glenoid fossa of the temporal bone. Radiographic appearance: it appears as a bony, rounded radiopaque projection extending from the posterior border of the ramus of the mandible. It is not seen on the periapical radiographs. Coronoid notch: it is a scooped-out concavity of bone located distal to the coronoid process of the mandible. Radiographic appearance: it appears as a radiopaque concavity located distal to the coronoid process of the mandible. It is not seen on periapical radiographs. Coronoid process: it is a marked prominence of bone found on the anterior superior ramus of the mandible. Radiographic appearance: it appears as a triangular radiopacity posterior to the maxillary tuberosity region. Mandibular foramen: it is a round or ovoid hole in bone on the lingual aspect of the ramus of the mandible. Radiographic appearance: it appears as a round or ovoid radiolucency centered within the ramus of the mandible. It is not seen on periapical radiographs. Lingula: it is a small, tongue-shaped projection of bone seen adjacent to the mandibular foramen. Radiographic appearance: it appears as an indistinct radiopacity anterior to mandibular foramen. It is not seen on the periapical radiographs. Mandibular canal: it is a tube lioke passageway through bone that travels the length of the mandible. It extends from the mandibular foramen to the mental foramen. Radiographic appearance: it appears as a radiolucent band outlined by two thin radiopaque lines representing the cortical walls of the canal. Mental foramen: it is an opening or hole in bone located on the external surface of the mandible in the region of mandibular premolars. Radiographic appearance: it appears as a small, ovoid or round radiolucency located in the apical region of the mandibular premolars. Mental ridge: it is a linear prominence of cortical bone located on the external surface of the anterior portion of the mandible that extends from the premolar region to the midline. Radiographic appearance: it appears as a thick radiopaque band that extends from mandibular premolar region to the incisor region. Mental fossa: it is a scooped-out depressed area of bone located on the external surface of the anterior mandible above the mental ridge in the mandibular incisor region. Radiographic appearance: it appears as a radiolucent area above the mental ridge. Lingual foramen: it is a tiny opening or hole in bone located on the internal surface of the mandible near the midline. Radiographic appearance: it appears as a small radiolucent dot located inferior to the apices of the mandibular incisors. Genial tubercles: these are the tiny bumps of bone located on the lingual aspect of the mandible. Radiographic appearances: they appear as a ring-shaped radiopacity surrounding the lingual foramen. Inferior border of mandible: it is a linear prominence of cortical bone that defines the lower border of the mandible. Radiographic appearance: it appears as a dense radiopaque band that outlines the lower border of the mandible. Mylohyoid ridge: it is a linear prominence of bone located on the internal surface of the mandible that extends from the molar region downward and forward toward the lower border of the mandibular symphysis. Radiographic appearance: it appears as a dense radiopaque band that extends downward and forward from the molar region. Internal oblique ridge: it is a linear prominence of bone located on the internal surface of the mandible that extends downward and forward from the ramus. Radiographic appearance: it appears as a dense radiopaque band that extends downward and forward from the ramus. External oblique ridge: it is a linear prominence of bone located on the external surface of the body of the mandible. Radiographic appearance: it appears as a dense radiopaque band that extends downward and forward from the anterior border of the ramus of the mandible. Angle of mandible: it is the area of the mandible where the body meets the ramus. Radiographic appearance: it appears as a radiopaque bony structure where the ramus joins the body of the mandible. Air space images seen on panoramic radiographs Palatoglossal air space: it refers to the space found between the palate (palato) and tongue (glossal). Radiographic appearance: it appears as a horizontal radiolucent band located above the apices of the maxillary teeth. Nasopharyngeal air space: it refers to the portion of the pharynx (pharyngeal) located posterior to the nasal cavity (naso). Radiographic appearance: it appears as a diagonal radiolucency located superior to the radiopaque shadow of the soft palate and uvula. Glossopharyngeal air space: it refers to the portion of the pharynx (pharyngeal) located posterior to the tongue (glosso) and oral cavity. Radiographic appearance: it appears as a vertical radiolucent band superimposed over the ramus of the mandible. It is continuous with the nasopharyngeal air space superiorly and the palatoglossal air space inferiorly. Soft tissue images seen on panoramic radiographs Soft tissue images seen on panoramic films: 1. tongue, 2. soft palate and uvula, 3. lipline, 4. ear Tongue: it is a movable muscular organ located to the floor of the mouth. Radiographic appearance: it appears as a radiopaque area superimposed over the maxillary posterior teeth. Soft palate and uvula: they form a muscular curtain that separates the oral cavity from the nasal cavity. Radiographic appearance: it appears radiopaque extending posteriorly from hard palate over each ramus. References • White and Pharoah 6th edition • Haring and Howerton 3rd edition • www.harpercollege.edu • www.monroecc.edu • www.dent.ohio-state.edu