Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Phase I Trial Designs
Jud Blatchford, PhD
BIOM 6649 – Clinical Trials
April 9th, 2015
Table of Contents
1.
2.
3.
4.
Orientation
Introduction
Components of a Phase I Trial
Phase I Trial Designs
A. Rule-Based Designs
B. Statistical Designs
5. References
Jud Blatchford, PhD
Phase I Trial Designs
2
ORIENTATION
Jud Blatchford, PhD
Phase I Trial Designs
3
Orientation
• Features of a Clinical Trial (CT)
◦ Study of human beings
◦ Prospective
◦ Uses an intervention (i.e. changes some aspect of the
subjects)
◦ Protects the safety of the subjects
◦ Follows an approved protocol
Jud Blatchford, PhD
Phase I Trial Designs
4
Orientation
• Phases of Clinical Trials
◦ Phase I – First time an experimental drug or treatment is
tested in humans to examine how well the drug is tolerated
◦ Phase II – Trials designed to examine if the drug or
treatment has a biological treatment effect
◦ Phase III – Trials designed to assess the treatment effect on
a clinically meaningful endpoint
◦ Phase IV – Post-marketing studies to gain additional
information regarding the safety of the drug or treatment
Jud Blatchford, PhD
Phase I Trial Designs
5
Orientation
• Components of Study Design
◦ Rationale – Establishing a legitimate reason for the study
◦ Design – Detailed description of what treatments will be
administered, how they are administered, including a
timeline of administration
◦ Subjects – Determining the group to be studied and how
they will be assigned to treatment groups
◦ Data – Endpoint(s), obtaining data, and QA
◦ Sample Size Justification – Ensuring the study will be able
to answer the scientific question with adequate power
◦ Study Closure – Archiving study data, analysis files
Jud Blatchford, PhD
Phase I Trial Designs
6
INTRODUCTION
Jud Blatchford, PhD
Phase I Trial Designs
7
Introduction
• Phase I Clinical Trials
◦ An experimental drug, treatment, chemotherapeutic agent,
cytotoxic agent, is studied—hereafter referred to as “drug”
◦ Primary Goal: Safety
Investigate whether the new drug or combination of
drugs can be administered safely to subjects
Investigate optimal dosing and administration of drug
◦ Secondary Goal: Efficacy
Offer a treatment option to subjects who have failed
other treatment regimens
Jud Blatchford, PhD
Phase I Trial Designs
8
Introduction
• Underlying Assumptions
◦ The drug kills both cancer cells and other cells
◦ The effect is dose-dependent, therefore:
1. The efficacy of the drug increases with the dose
2. The toxicity of the drug increases with the dose
◦ Logically, it would be optimal to give the subjects the
highest dose of a drug that can be administered without
unacceptable toxicity
◦ Fundamental Question: What is this dose?
Jud Blatchford, PhD
Phase I Trial Designs
9
Maximum Tolerated Dose (MTD)
• Definition of MTD:
◦ The highest dose without observing an unacceptable rate
of toxicity
• Aliases:
◦ Recommended Phase 2 Dose (RP2D)
◦ Phase 2 Recommended Dose (P2RD)
Jud Blatchford, PhD
Phase I Trial Designs
10
COMPONENTS OF A PHASE I TRIAL
Jud Blatchford, PhD
Phase I Trial Designs
11
Components of a Phase I Trial
• Definition of a Dose-Limiting Toxicity (DLT)
◦ Clarify time-frame for experiencing a DLT
• Dose Levels
◦ How many dose levels will be tested?
◦ What will the smallest dose be?
◦ What will the starting dose be?
• Subjects
◦ How many subjects will be tested?
◦ Will single subjects or cohorts be tested at each dose?
• What dose-escalation scheme will be employed?
Jud Blatchford, PhD
Phase I Trial Designs
12
Definition of a DLT
• DLTs are typically defined
using the National Cancer
Institute’s (NCI) Common
Terminology Criteria for
Adverse Events (CTCAE).
• DLTs are often grade ≥ 3
non-hematological and grade
≥ 4 hematological toxicities,
which are definitely,
probably, or possibly related
to the drug.
Jud Blatchford, PhD
• CTCAE Grades
◦
◦
◦
◦
◦
◦
0 – No AE
1 – Mild
2 – Moderate
3 – Severe
4 – Life threatening
5 – Death
• Degrees of Related
Phase I Trial Designs
◦
◦
◦
◦
◦
Unrelated
Unlikely
Possibly
Probably
Definitely
13
Definition of a DLT
• The length of observation within which a DLT
occurrence is “counted” should be explicitly stated
in the protocol
• Typical lengths used are the first cycle of
chemotherapy (often 3 weeks)
• Weight the trade-off between observation time
for a DLT and efficiency in enrolling subjects
Jud Blatchford, PhD
Phase I Trial Designs
14
Choosing the Starting Dose
• Goals:
◦ Dose high enough to have chance of efficacy
◦ Dose low enough to avoid a DLT
• Use data from animal pre-clinical studies
• Scale dose by body surface area (mg/m2)
• Studies that aren’t “first-in-human” studies may
be informed from previous studies using the same
drug
Jud Blatchford, PhD
Phase I Trial Designs
15
Choosing the Starting Dose
• Choices Used:
◦ First find dose that is lethal in 10% of mice (LD10)
Standard starting dose was 10% of this dose (MELD10),
if no grade 4+ AEs observed in other species (rats, dogs,
etc.)
◦ Find the highest dose for which the most sensitive animals
investigated had no AEs
Starting dose is 1/3 of this level (scaled)
◦ Find the minimal dose for which any toxicity is seen (TDL)
Starting dose is 1/3 of the TDL
Jud Blatchford, PhD
Phase I Trial Designs
16
Choosing the Number of Dose Levels
• Testing more dose levels to accurately estimate
the MTD creates a more cumbersome trial, and
may require more subjects
• Common number of levels is 4 to 7
• Observed number has ranged from 3 to 14
Jud Blatchford, PhD
Phase I Trial Designs
17
Choosing the Dose Levels
• Desire to progress through possible doses in a
quick (e.g. exponential) manner
• Ethical considerations should guide the dose
escalation scheme used
• Linear sequence of numbers may be inefficient
◦ 20, 40, 60, 80, 100, 120, 140, …
• Famous sequence of increasing numbers:
◦ 1, 1, 2, 3, 5, 8, 13, 21, 34, 55, 89, 144, 233, 377, 610, 987, …
Jud Blatchford, PhD
Phase I Trial Designs
18
The Fibonacci Sequence
Term (n)
Value (fn)
Ratio (fn / fn-1)
1
1
-
2
1
1.000
3
2
2.000
4
3
1.500
5
5
1.667
6
8
1.600
7
13
1.625
8
21
1.615
9
34
1.619
10
55
1.618
11
89
1.618
Jud Blatchford, PhD
Phase I Trial Designs
19
The Golden Ratio
Jud Blatchford, PhD
Phase I Trial Designs
20
The Golden Ratio
Jud Blatchford, PhD
Phase I Trial Designs
21
Fibonacci Sequence in Nature
Jud Blatchford, PhD
Phase I Trial Designs
22
Spirals in a Pine Cone
Clockwise from Center
Jud Blatchford, PhD
Counter-clockwise from Center
Phase I Trial Designs
23
Modified Fibonacci Dose Escalation (MFDE)
Ratio (fn / f1)
Fib. Seq.
1
-
1.00
1
2
2.00
2.00
1
3
1.67
3.33
2
4
1.50
5.00
3
5
1.40
7.00
5
6
1.33
9.33
8
7
1.33
12.44
13
8
1.33
16.59
21
9
1.33
22.12
34
10
1.33
29.50
55
11
1.33
39.33
89
Jud Blatchford, PhD
Phase I Trial Designs
Comparison
Conservative
Ratio (fn / fn-1)
Similar
Term (n)
24
Ethical Considerations
• Approach the MTD from below (under-estimates
MTD)
◦ Bracketing the MTD is unbiased and more efficient
• Expected efficacy is minimal
◦ Historical response rate is 11%; temp. stable rate is 34%
◦ 40% expect a cure
• Subjects suffer significant toxicity
◦ Rate of grade 4 toxicity is 14%; death rate is 0.5%
• What subjects are told is very important
Jud Blatchford, PhD
Phase I Trial Designs
25
PHASE I TRIAL DESIGNS
Jud Blatchford, PhD
Phase I Trial Designs
26
Rule-Based Designs
1.
2.
3.
4.
5.
Traditional Escalation Rule
Variations of the Traditional Escalation Rule
Best of 5 Rule
Up-and-Down Designs
2-Stage Designs
Jud Blatchford, PhD
Phase I Trial Designs
27
Traditional Escalation Rule (TER)
3 subjects receive
dose di
0 DLTs
1 DLT
2 or 3 DLTs
Escalate - 3 subjects
receive dose di+1
3 more subjects at
dose di
Stop escalation
De-escalate to di-1
0 DLTs
(1/6 with DLT)
1—3 DLTs
(≥ 2/6 with DLT)
Escalate - 3 subjects
receive dose di+1
Stop escalation
De-escalate to di-1
De-escalate until a level is reached where at least 6 subjects are treated and at most 1 DLT occurs.
MTD is the highest dose where at least 6 subjects were treated with at most 1 DLT.
Jud Blatchford, PhD
Phase I Trial Designs
28
Evaluating the TER
Benefits
Criticisms
• Conservative escalation
• Ease of implementation
• Many subjects treated at
low, ineffective doses
• At least 2 subjects treated
at level above MTD
• The true MTD is
underestimated
◦ Rules regarding dose assignment
are clear
◦ Statistical models not fit after
each subject
• Design is robust
• Will arrive at reasonable
estimate of MTD
Jud Blatchford, PhD
Phase I Trial Designs
29
Variations to TER
• After escalation stops, fill out all lower levels until
at least 6 subjects are treated at each level
• Treat subjects at a dose level between the level
where escalation stopped and the next lower level
Jud Blatchford, PhD
Phase I Trial Designs
30
Best of 5 Rule
3 subjects receive
dose di
0 DLTs
1 or 2 DLTs
3 DLTs
Escalate to dose di+1
1 more at dose di
Stop escalation
1/4 with DLT
2/4 with DLTs
3/4 with DLTs
Escalate to dose di+1
1 more at dose di
Stop escalation
2/5 with DLTs
3/5 with DLTs
Escalate to dose di+1
Stop escalation
MTD is the dose prior to the dose on which escalation stopped.
Jud Blatchford, PhD
Phase I Trial Designs
31
Up-and-Down Design (UaD)
1 subject receives
dose di
0 DLT
1 DLT
Escalate to dose di+1
De-escalate to di-1
Perform UaD for a pre-specified number of subjects (j).
MTD is the dose that would be assigned to the j+1st subject.
Jud Blatchford, PhD
Phase I Trial Designs
32
Storer’s C Design (UaD-C)
1 subject receives
dose di
0 DLT
1 DLT
If 2 consecutive
subjects with 0 DLT,
escalate to dose di+1;
else give dose di
De-escalate to di-1
Perform UaD for a pre-specified number of subjects (j).
MTD is the dose that would be assigned to the j+1st subject.
Jud Blatchford, PhD
Phase I Trial Designs
33
Stage 1
Storer’s Two-Stage BC Design (UaD-BC)
1 subject receives
dose di
0 DLT
1 DLT
Escalate to dose di+1
De-escalate to di-1
Stage 2
1 subject receives
dose di-1
0 DLT
1 DLT
If 2 consecutive
subjects with 0 DLT,
escalate to dose di;
else give dose di-1
De-escalate to di-2
Perform UaD for a pre-specified number of subjects (j).
MTD is the dose that would be assigned to the j+1st subject.
Jud Blatchford, PhD
Phase I Trial Designs
34
Accelerated Titration Designs
Extension by Simon of Storer’s work
Design 1: TER
Designs 2—4
Stage 1: Single subjects until first DLT or second grade 2 AE
Stage 2: TER
Design 2: Toxicities observed in first cycle only
Design 3: Toxicities may be observed in any cycle
Design 4: Same as 3 except escalation factor is 2.0
Jud Blatchford, PhD
Phase I Trial Designs
35
Statistical Designs
Dose escalation guided by a statistical model of the
relationship between dose and toxic response
1. Continual Reassessment Method
2. Modifications to the CRM
3. 2-Stage CRM Designs
4. TITE-CRM
Jud Blatchford, PhD
Phase I Trial Designs
36
Continual Reassessment Method (CRM)
• First proposed by O’Quigley in 1990
• Subjects are enrolled individually
• A dose-toxicity function is assumed
◦ f(d | α) = Pr{DLT | α}
• After each patient completes observation, the
estimate of α is updated
• Strategy is to assign the dose closest to the
estimated MTD to each subject
Jud Blatchford, PhD
Phase I Trial Designs
37
Considerations for the CRM
• Number of dose levels
• Initial estimates of toxicity rates at each dose level
• Target rate of DLT (θ)
• Dose-toxicity function
• Escalation restrictions
• Number of subjects to be treated
Jud Blatchford, PhD
Phase I Trial Designs
38
Considerations
Number of Dose Levels
Initial Estimates of Toxicity
• Typically between 3 and 8
• In general, as the number of
dose levels in the trial
increases, the number of
subjects needed to
accurately estimate the MTD
will increase
• The estimates should bound
the target rate (θ)
Jud Blatchford, PhD
Phase I Trial Designs
◦ The CRM is not robust when
doses tested do not induce
toxicity
39
Choosing a Dose-Response Function
Logistic Function
Logistic Regression
Let p = Pr{DLT}
𝑝
ln
= 𝛽0 + 𝛽1(𝐷𝑜𝑠𝑒)
1−𝑝
Solving for p we have:
𝑝 =
𝑒 𝛽0+𝛽1(𝐷𝑜𝑠𝑒)
1+𝑒 𝛽0+𝛽1(𝐷𝑜𝑠𝑒)
One-parameter model:
𝑒 3+α(𝐷𝑜𝑠𝑒)
𝑝=
1 + 𝑒 3+α(𝐷𝑜𝑠𝑒)
Jud Blatchford, PhD
Phase I Trial Designs
40
Choosing a Dose-Response Function
Hyperbolic Tangent Function
𝑇𝑎𝑛ℎ =
Jud Blatchford, PhD
𝑒 𝑥 −𝑒 −𝑥
𝑒 𝑥 +𝑒 −𝑥
=
𝑒 2𝑥 −1
𝑒 2𝑥 +1
Scaled Tanh Function
Pr{DLT}=
Phase I Trial Designs
𝑒 2(𝐷𝑜𝑠𝑒) −1
1
+
2𝑒 2(𝐷𝑜𝑠𝑒) +2
2
−α
41
Choosing a Dose-Response Function
CDF of Normal Distribution
2
P{DLT}=
Jud Blatchford, PhD
Phase I Trial Designs
𝐷𝑜𝑠𝑒 −(𝑥−𝜇)
1
𝑑𝑥
2𝜎2
𝑒
2𝜋𝜎 −∞
42
The Method of CRM
• Dose-toxicity function and θ are chosen a-priori
• Function is re-fit (i.e. new estimate of α is
obtained) after each subject’s observed toxicity
◦ New function is determined from the a-priori function and
the vector of observed toxicities
◦ Curve shifts to the right without toxicity; left with toxicity
• Next subject is treated at the dose level whose
Pr{DLT} is closest to θ
Jud Blatchford, PhD
Phase I Trial Designs
43
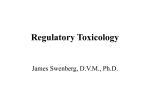
Distributions of DLT Occurrence By Dose
Priors for Subject 1
Priors for Subject 26
• High degree of overlap of
probabilities between doses
• Separation between dose
levels becoming clearer
Jud Blatchford, PhD
Phase I Trial Designs
44
Evaluating the CRM
Benefits
Criticisms
• Few subjects are treated at
low, ineffective doses
• Subjects are treated at doses
believed at the time to be
the most efficacious, yet safe
• Starting dose is too high
• Dose escalation is too
aggressive
• Trial length is too long
Jud Blatchford, PhD
Phase I Trial Designs
45
Modified CRM
• Start at the lowest dose level under consideration
• Enroll two or three subjects at each cohort
• Constrain dose escalation to increase by at most
one dose level
Jud Blatchford, PhD
Phase I Trial Designs
46
“Practical” CRM
• Proposed by Piantadosi
• Based on pre-clinical toxicity data:
◦ Choose dose that would produce low (10%) rate of DLT
◦ Choose dose that would produce high (90%) rate of DLT
◦ Estimate dose/toxicity curve that fits these 2 points
• Use the dose/toxicity curve to find dose for θ
• Treat three subjects at this level, then re-estimate
the dose-toxicity curve, dose for θ, and tx 3 more
• Repeat until target dose changes by < 10%
Jud Blatchford, PhD
Phase I Trial Designs
47
2-Stage CRM Designs
• Stage 1: TER
◦ “2 + 2” is a more common first stage than “3 + 3”
◦ Continue until first toxicity is observed
• Stage 2: CRM
◦ After first toxicity, fit the dose-response curve using the
toxicity data accrued thus far
◦ Choose dose for next cohort of 2 as dose with estimated
rate of DLT closest to θ
Jud Blatchford, PhD
Phase I Trial Designs
48
Time-to-Event CRM (TITE-CRM)
• Builds on the CRM described thus far
• Uses information from subjects accrued, even if
they haven’t finished observation period
◦ Subjects with DLT are given full weight
◦ Subjects without DLT are given weight t/T.
• Allows subjects to be enrolled without waiting for
prior cohorts to finish
◦ Benefits studies with delayed toxicity (e.g. radiation
studies)
Jud Blatchford, PhD
Phase I Trial Designs
49
Example of a TITE-CRM Trial
• Subject accrual is instantaneous
• The majority of doses administered are near MTD
Jud Blatchford, PhD
Phase I Trial Designs
50
Additional TITE-CRM Considerations
• Choice of weight function
◦ Uniform toxicities may use a linear function
◦ Expecting late toxicities may use a convex function
◦ Expecting early toxicities may use a concave function
• Setting a Margin (i.e. upper limit) on toxicity
◦ If θ = 0.20 and Margin = 0.05, dose for next subject will be
dose closest to 0.20 and not greater than 0.25
• Determine cumulative time exposure (B) before
allowing escalation (e.g. B = 2)
Jud Blatchford, PhD
Phase I Trial Designs
51
Design Comparisons
• Fitting a model to the data will improve the
accuracy of the MTD found by rule-based designs
• Model-guided designs only perform well if
assumptions are met (θ in range of doses tested)
• Conflicting results when designs compared
• Few comparisons made on “level playing field”
• Both rule-based and model-guided designs are in
common use, for good reason
Jud Blatchford, PhD
Phase I Trial Designs
52
Important Future Work
• “Individualized” Designs
◦ Development of designs allowing for within-subject dose
escalation
◦ Development of designs for targeted agents
• Designs for trials expecting minimal toxicity
Jud Blatchford, PhD
Phase I Trial Designs
53
Pharmacokinetic Profiles
• Often of interest in a phase 1 study
• Studies how the body processes the drug
• Parameters of interest are typically:
◦
◦
◦
◦
◦
Cmax – Maximum concentration of drug
Tmax – Time until the maximum concentration of drug
λ – Elimination constant – describes rate of loss from body
T1/2 – Half-life of the drug
AUC – Area under the concentration curve
Jud Blatchford, PhD
Phase I Trial Designs
54
Calculation of PK Parameters
• Cmax & Tmax – Directly from table of results
• λ = Taken from regression of ln(C) on time
• T1/2
◦ Create exponential decay equation from above regression
◦ Solve for T when the concentration is half of reference amt
• AUC = AUC0-t + AUCt-∞
◦ AUC0-t – Use trapezoidal rule
◦ AUCt-∞ = Ct / λ
Jud Blatchford, PhD
Phase I Trial Designs
55
Example Calculations
• From regression of ln(C) on time we get:
◦
◦
◦
◦
◦
◦
◦
ln (C) = 2.25 – 0.58 T, so λ = 0.58 (not -0.58)
C = exp(2.25) * exp(-0.58)T
C = 9.5(-.56)T
4.75 = 9.5(-0.56)T
to solve for T1/2
½ = -0.56T
ln(1/2) = T*ln(-0.56)
T = 1.19 so T1/2 = 1.19 hours
• AUC = 12.03 + 0.06/0.58 = 12.18
Jud Blatchford, PhD
Phase I Trial Designs
56
PK Design Considerations
• Sampling Times
◦ Important to have accurate estimates of Cmax
◦ Cluster several times around expected Tmax
• Sampling Period
◦ Important to have accurate estimate of λ
◦ US FDA requires times to capture at least 3 half-lives after
Tmax
• Bioequivalence Trials
◦ Create 90% CIs for ln[µ(A)] - ln[µ(B)], µ = PK parameter
◦ Check if all CIs are within 0.80 to 1.25 range
Jud Blatchford, PhD
Phase I Trial Designs
57
REFERENCES
Jud Blatchford, PhD
Phase I Trial Designs
58
References
1989. Storer BE. Design and Analysis of Phase I Clinical Trials. Biometrics, 45, 925—937.
1990. O’Quigley J, Pepe M, and Fisher L. Continual Reassessment Method: A Practical Design for
Phase I Clinical Trials in Cancer. Biometrics, 46, 33—48.
1993. Korn EL, and Simon R. Using the Tolerable-Dose Diagram in the Design of Phase I
Combination Chemotherapy Trials. Journal of Clinical Oncology, 11 (4), 794—
801.
1993. Mick R, and Ratain MJ. Model-Guided Determination of Maximum Tolerated Dose in
Phase I Clinical Trials: Evidence for Increased Precision. Journal of the National
Cancer Institute, 85 (3), 217—223.
1994. Faries D. Practical Modifications of the Continual Reassessment Method for Phase I Cancer
Clinical Trials. Journal of Biopharmaceutical Statistics, 4 (2), 147—164.
1996. Piantadosi S, and Liu G. Improved Designs for Dose Escalation Studies Using
Pharmacokinetic Measurements. Statistics in Medicine, 15, 1605—1618.
1996. Smith TL, Lee JJ, Kantarjian HM, Legha SS, and Raber MN. Design and Results of Phase I
Cancer Clinical Trials: Three-Year Experience at M. D. Anderson Cancer Center.
Journal of Clinical Oncology, 14 (1), 287—295.
1997. Durham SD, Flournoy N, and Rosenberger WF. A Random Walk Rule for Phase I Clinical
Trials. Biometrics, 53, 745—760.
Jud Blatchford, PhD
Phase I Trial Designs
59
References (Continued)
1997. Simon R, Freidlin B, Rubinstein L, Arbuck SG, Collins J, and Christian MC. Accelerated
Titration Designs for Phase I Clinical Trials in Oncology. Journal of the National
Cancer Institute, 89 (15), 1138—1147.
1998. Friedman LM, Furberg CD, and DeMets DL. Fundamentals of Clinical Trials. Springer.
1998. Whitehead J, and Williamson D. Bayesian Decision Procedures Based on Logistic
Regression Models for Dose-Finding Studies. Journal of Biopharmaceutical
Statistics, 8 (3), 445—467.
1999. Reiner E, Paoletti X, and O’Quigley J. Operating Characteristics of the Standard Phase I
Clinical Trial Design. Computational Statistics and Data Analysis, 30, 303—315.
2000. Cheung YK, and Chappell R. Sequential Designs for Phase I Clinical Trials with Late-Onset
Toxicities. Biometrics, 56, 1177—1182.
2000. Eisenhauer EA, O’Dwyer PJ, Christian M, and Humphrey JS. Phase I Clinical Trial Design in
Cancer Drug Development. Journal of Clinical Oncology, 18 (3), 684—692.
2000. Wang O, and Faries DE. A Two-Stage Dose Selection Strategy in Phase I Trials with Wide
Dose Ranges. Journal of Biopharmaceutical Statistics, 10 (3), 319—333.
2001. Lin Y, and Shih WJ. Statistical Properties of the Traditional Algorithm-Based Designs for
Phase I Cancer Clinical Trials. Biostatistics, 2 (2), 203—215.
Jud Blatchford, PhD
Phase I Trial Designs
60
References (Continued)
2001. Ishizuka N, and Ohashi Y. The Continual Reassessment Method and Its Applications: A
Bayesian Methodology for Phase I Cancer Clinical Trials. Statistics in Medicine,
20, 2661—2681.
2002. Potter PM. Adaptive Dose Finding for Phase I Clinical Trials of Drugs Used for
Chemotherapy of Cancer. Statistics in Medicine, 21, 1805—1823.
2003. Agrawal M, and Emanuel EJ. Ethics of Phase I Oncology Studies: Reexamining the
Arguments and Data. Journal of the American Medical Association, 290 (8),
1075—1082.
2003. Ivanova A, Montazer-Haghighi A, Mohanty SG, and Durham SD. Improved Up-and-Down
Designs for Phase I Trials. Statistics in Medicine, 22, 69—82.
2004. Stylianou M, and Follmann DA. The Accelerated Biased Coin Up-and-Down Design in
Phase I Trials. Journal of Biopharmaceutical Statistics, 14 (1), 249—260.
2005. Horstmann E, McCabe MS, Grochow L, Yamamoto S, Rubinstein L, Budd T, Shoemaker D,
Emanuel EJ, and Grady C. Risks and Benefits of Phase I Oncology Trials, 1991
Through 1992. New England Journal of Medicine, 352, 895—904.
2006. Crowley J, and Ankerst DP. Handbook of Statistics in Clinical Oncology. Chapman and
Hall/CRC.
Jud Blatchford, PhD
Phase I Trial Designs
61
References (Continued)
2006. Potter DM. Phase I Studies of Chemotherapeutic Agents in Cancer Patients: A Review of
the Designs. Journal of Biopharmaceutical Statistics, 16, 579—604. DOI:
10.1080/10543400600860295.
Jud Blatchford, PhD
Phase I Trial Designs
62