Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
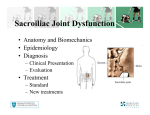
SIJ – A COMMON CAUSE OF LBP? Kathryn Dunbar Clinical Specialist Connect Physical Health Centres AIMS To give a basic understanding of the SIJ and how to identify a dysfunction AIMS Does the SIJ move? Anatomy, stability and function Predisposing factors Symptoms, aggravating and easing factors Quick examination techniques Piriformis syndrome Treatment and advice THE PELVIS Pelvic Girdle Osseo cartilaginous ring made up from sacrum, coccyx and 2 innominate bones Joints within or on the girdle: Pubic Symphysis Sacroiliac joints Hip joints L5 / S1 SACRUM Varies in shape Can be more triangular – greater stability More rectangular – less stability Frequent bony anomalies Does the SIJ move? Part synovial, part fibrous Sacral surface is covered by articular (hyaline) cartilage The ilium’s surface is covered by fibrocartilage Both surfaces are reciprocal although they are very irregular and not congruent There is a disc like substance found in 30% of SIJ’s STABILITY For walking the SIJ needs optimal joint mobility as well as stability The shape of the sacrum and innominates and the irregularity of the joint surfaces give some form closure Several muscles, ligaments and the thoraco-lumbar fascia all contribute to force closure (compression) This combination of form and force closure is termed as selfbracing or self-locking mechanism Functions of the Sacroiliac Joint 1. Transmission of forces from the trunk through the lumbo-sacral junction to the sacrum. 2. Shock absorption There is evidence of increased disc degeneration in the lumbar spine after deterioration of the SIJ. (Shaw 1992 and Scholten 1988) 3. Stability of the pelvis. 4. The pelvis provides protection to the viscera and foetus in pregnancy DYSFUNCTIONS OF THE SIJ 1. Of 88 patients with low back pain, 71 (88%) had evidence of SIJ dysfunction. 73% of the 71 had unilateral low back pain." Cibulka 1992 2. In our study of 1,000 consecutive patients with low back pain, 98% had a mechanical dysfunction of the sacroiliac joints as a major cause of their LBP."Joseph L. Shaw 1992 3. The presence of unilateral low back pain alerts the clinician that a patient may have a sacroiliac problem." Greenman 1992, also Bourdillon 1982, Wells 1986, Ramamurti 1979, Cibulka 1992. HISTORY Pregnancy / childbirth Menopause Following gynae examination or obs and gynae surgery Bladder ops, prostatectomy Repetitive movements involving twisting in forward stoop position or sitting forward, lateral lifting e.g. nurse, physio, housewife, desk worker, check out operator in shop HISTORY Sport – e.g. golf, athletics, fast bowling, football, horse riding, martial arts, aerobics, rowing Trauma – lifting, fall onto ischial tuberosity / coccyx, fracture around pelvis, femur, lumbar spine, stepping down heavily, RTA, post THR Stiff hips, stiff lumbar spine, tight hamstrings, poor core stability, actual LLD, hypermobility Standing unevenly, sitting crossed legged Hamstring problems, recurrent groin strains and lower abdominal tears and conjoint tendon problems SYMPTOMS Usually unilateral pain, more often felt below the level of the iliac crest Referral into buttock, lower abdomen, groin, pubis, posterior thigh, medial thigh Pain from SIJ can be felt below knee to the foot ‘Sciatic nerve’ symptoms from piriformis syndrome Pins and needles in buttock from sacrotuberous ligament syndrome SYMPTOMS Local pain over SIJ can be minimal Pubic symphysis can cause groin pain radiating to the medial thigh Clicking over pubic symphysis Anaesthesia / paraesthesia N.B. Check for testicular symptoms, abdominal symptoms, saddle anaesthesia, urinary symptoms, Gilmore’s groin Be aware that SIJ and Lumbar spine problems can coexist BEHAVIOUR OF SYMPTOMS Can be constant or intermittent with any degree of severity and irritability Dull aching or stabs of pain Hind quarters feel twisted, out of place Leg can feel heavy, dead Giving way (can be due to dysfunction of iliopsoas, diastasis or hypermobility) SIJ asymmetry can inhibit pelvic floor function and may be responsible for the secondary coccydinia experienced by a number of patients with pelvic girdle dysfunction AGGRAVATING FACTORS Weight bearing Stand on one leg Rolling over in bed Walking Running Jumping AGGRAVATING FACTORS Sit stand Sit crossed legged Prolonged position In and out of car Coughing can increase pain with hypermobile SIJ’s and especially with pubic symphysis diastasis (distinguish by compression through greater trochanters) Groin pain aggravated by kicking, hurdling, step aerobics, golf swing, crossing legs, horse riding EASING FACTORS Gentle movement Changing position Sleep with pillow between knees Keeping knees together when turning e.g in and out of car Foetal position Pulling knees to chest Sit in posterior pelvic tilt / leaning forwards Bath DIFFERENTIAL DIAGNOSIS Constant unvarying night pain unrelated to movement Consider general health e.g. Appendicitis, UTI’s, Diabetes, Pagets disease, T.B., evidence of primary neoplasm elsewhere (breast, bronchial etc), Prostate Cancer, Avascular necrosis, Reiters disease, Anky Spon, Psoriatic arthritis, Osteitis pubis, Osteomyelitis, Inguinal hernia, IBS EXAMINATION Palpation ASIS’s PSIS’s Iliac Crests Sacral sulcus Ischial tuberosities EXAMINATION Squish Test – Posterior Ilial Glide Patient in supine lying Glide the SI joint in a posteromedial direction in line with forearms (elbows flexed to 15º) Slowly glide one side (should take 4-6 secs), then the other side (do not fix contralateral side) Looking for quality and quantity of motion and end feel Not looking for pain Positive test on hypomobile side EXAMINATION Leg Length Supine and Long Sit Ensure patient is straight on bed Check level of medial malleoli in supine Ask patient to sit in long sit and assess for change in medial malleoli levels A change indicates SIJ dysfunction No change indicates actual leg length discrepancy EXAMINATION Differentiation Waiters Bow If patient complains of pain with Lumbar flexion, repeat keeping lumbar spine straight. If pain implicates Lumbar spine, if pain or no change indicates SIJ or hip To differentiate hip further can put foot on a chair or internally rotate (any change in pain with lumbar flexion implicates hip) EXAMINATION Differentiation Greater Trochanter compression With pain on Lumbar flexion, repeat flexion with compression through the greater trochanters. pain implicates SIJ PIRIFORMIS SYNDROME Sciatic nerve goes through or under piriformis Sustained tension in this muscle can lead to the formation of trigger points resulting in the compression of the sciatic nerve and possibly the dysfunction of the SIJ. This tension in the Piriformis results in symptoms that are easily confused with those of a herniated disc. Recognition of piriformis symptoms may avoid needless laminectomy and orthopaedic referral. PIRIFORMIS SYNDROME Symptoms May be a mixture of seemingly unrelated symptoms. Pain and paraesthesia may be apparent in one or more of these areas: Lumbar Spine Groin Perineum Buttock Hip Back of the thigh Leg and foot or the SI joint. PIRIFORMIS SYNDROME Symptoms Swelling can occur in the painful leg and sexual dysfunction can occur. Sitting, getting up, activity or standing can aggravate the condition. It can also cause the buttock muscles to atrophy. Numbness of the foot and loss of proprioception can lead to an unstable walk. PIRIFORMIS SYNDROME Assessment Palpation of trigger points Side lie on uninvolved side Flex hips to 90º Palpate from the greater trochanter to the sacrum Looking for tenderness or reproduction of symptoms PIRIFORMIS SYNDROME Assessment Length test Flex knee onto chest with knee in midline Maintain midline position and pull lower leg across midline Can add hip hitch to increase stretch PIRIFORMIS SYNDROME Assessment SLR with resisted external rotation (below 60º SLR) SLR with resisted internal rotation (above 60º SLR) TREATMENT Muscle Energy Techniques Mobilisation Manipulation Core stability exercises SI belt bracing Sclerosing injection Corticosteroid injection Orthotics Surgery to fuse the joint ADVICE Pillow between knees in side lie Pillow under knees in supine Keep knees together in / out car Gluts contraction Avoid asymmetrical positions e.g. sitting cross legged, standing with more weight through one leg ANY QUESTIONS?