Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
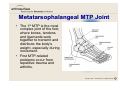
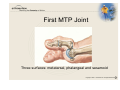
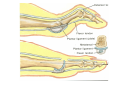
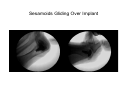
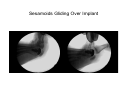
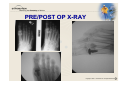
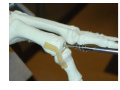
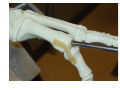
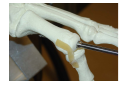
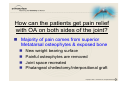
Great Toe Resurfacing System • • • • Indications Anatomy Treatment Options Arthrosurface System Indications • Degenerative and Posttraumatic arthritis in the first metatarsal joint in the presence of good bone stock • Hallux Rigidus / Limitus • Hallux Valgus* • Unstable or painful metatarsal / phalangeal (MTP) joint * In combination with corrective osteotomy Disarticulated bones of the foot • From above (The talus and calcaneus remain articulated) • 1 Calcaneus 2 Talus 3 Navicular 4 Medial cuneiform 5 Intermediate cuneiform 6 Lateral cuneiform 7 Cuboid 8 First metatarsal 9 Second metatarsal 10 Third metatarsal 11 Fourth metatarsal 12 Fifth metatarsal 13 Proximal phalanx of great toe 14 Distal phalanx of great toe 15 Proximal phalanx of second toe 16 Middle phalanx of second toe 17 Distal phalanx of second toe Metatarsophalangeal MTP Joint • The 1st MTP is the most complex joint of the foot, where bones, tendons and ligaments work together to transmit and distribute the body’s weight, especially during movement. • First MTP-related problems occur from repetitive trauma and arthritis. Foot Function– Truss and Tie-Rod • • • Walking generates a force in the forefoot equal to 80% of the body’s weight. Running increases it to 250% of body weight. Calcaneous and talus serving as the posterior strut, the remainder of the tarsals and the metatarsals serving as the anterior strut, and the plantar aponeurosis serving as a tensed tie-rod. Weighting of the foot will compress the struts and create additional tension in the tie-rod. The plantar aponeurosis holds together the anterior and posterior struts when the body weight is loaded on the triangle. First MTP Joint Three surfaces: metatarsal, phalangeal and sesamoid Sesamoids Gliding Over Implant Sesamoids Gliding Over Implant Sesamoids Gliding Over Implant Extension and Flexion • Arthritis reduces the natural extension and flexion of the great toe • The 1st MTP joint is instrumental in all sports that involve foot contact with the ground. • The Great Toe is the final structure in contact with the ground on push-off. First MTP Arthritis • • • • • • Hallux Rigidus/Limitus Hallux Valgus Rheumatoid arthritis Bunions Gout Post traumatic arthritis Hallux Rigidus • • • • Males mostly ages 20 – 60 years old Progressive arthritis from top to bottom Staged I, II or III depending on severity Sesamoid complex is last to be involved The Pain of Beauty • Shoes should be low heeled, stiff soled with a wide square shaped toe box. NOT • Women today are wearing shoes that clearly do not fit the profile Hallux Valgus • >85% Females; ages 40 – 60 years old • Pain in joint when active, especially on push-off • Swelling around the joint • Deformed mechanical axis • A bump, like a bunion or callus, that develops on the top & side of the foot • Stiffness in the great toe and an inability to bend it up or down Surgical Options: • Cheilectomy: (ky-lek-toe-me) Mild to moderate damage. Removes bone spurs • Arthrodesis (Fusion): Fusing the bones together (arthrodesis) has often been recommended when the damage to the cartilage is severe. Pins, screws, or a plate are used to fix the joint in a permanent position. • Arthroplasty: The joint surfaces are removed and an artificial joint is implanted. This procedure may relieve pain and preserve joint motion. Cheilectomy Resection arthroplasty (Keller) Arthrodesis (fusion) Arthroplasty (implant) Cheilectomy • PRO: – Keeps joint motion – No implants needed – Fast and easy to perform • CON – Only good in stage I with little joint involvement – 30% of patients will progress in arthritis – Quite often x-rays underestimate extent of disease Cheilectomy Resection arthroplasty (Keller) Arthrodesis (fusion) Arthroplasty (implant) Resection arthroplasty (Keller) • PRO: – Good for severe stages of arthritis (sesamoid arthritis) – Good relief of pain control – May weight bear immediately • CON: – High (40%) risk of deformity (varus/valgus/cock-up) – Severe loss of push-off strength – Only indicated for elderly and sedentary patients Arthrodesis - Fusion Arthrodesis • PRO: – Good relief of pain control – Good for sesamoid arthritis • CON: – Limits shoe wear for women – Increases stress on next joint – Hard to get patients to accept fusion – Long recovery from fusion (awaiting fusion) – Malpositioning is difficult to deal with BioPro Hemiarthroplasty Implant arthroplasty (hemi) • PRO: – Easy to perform – Good relief of arthritis pain – May weight bear immediately • CON: – Only for the proximal phalanyx – Does not work in sesamoid arthritis – Variable success rates Implant arthroplasty (total) • PRO: – Easy to perform – Good relief of arthritis pain – Allows immediate weight bearing – Either silastic or metal • Reflection – osteomed – accumed • CON: – Silastic has high failure rate and complications – Does not work in sesamoid arthritis, or loss of push off – Salvage/fusion is very difficult from bone loss – Joint subluxation is big problem (soft tissue balance) – success rates Interpositional arthroplasty • PRO: – Good relief of pain control – No artificial surfaces – Allows immediate weight bearing • CON: – Not for sesamoid arthritis – Causes significant stiffness and loss of motion – Variable success rates – High risk of postoperative deformity PRE/POST OP X-RAY HemiCAP Device • PRO: – Good relief of pain control – Addresses both sides of arthritis – Allows immediate weight bearing – Low incidence of postoperative deformity • CON: – Does not address sesamoid arthritis – No long term outcome studies yet Why this implant? • Very little bone resection so salvage (fusion) is much easier if fails. • Does not affect sesamoid complex so push off is normal. • With “Hasselman’s technique” both sides of the joint are resurfaced. • Allows women to wear their “other shoes” without sacrificing strength or pushoff. • Very easy to perform, no problems with instability or deformity because of soft tissue balance Algorithm by Age Conservative Tx Cheilectomy Age: <35 Bridging the Gap Hemi/Total Joint Replacement Fusion 35 - 60 >60 PRE/POST OP X-RAY INTRA-OP X-RAY PRE/POST OP X-RAY HemiCAP™ System Osteophytes No Cartilage Trial Reduction to assess Joint Space Main Objections How can the patients get pain relief with OA on both sides of the joint No joint space so how will HemiCAP™ address motion No cartilage left so how do you map surface Can you still do a fusion after this How can the patients get pain relief with OA on both sides of the joint? Majority of pain comes from superior Metatarsal osteophytes & exposed bone New weight bearing surface Painful osteophytes are removed Joint space recreated Phalangeal cheilectomy/interpositional graft How will HemiCAP™ address motion? Stiffness a result of osteophytes & pain Osteophyte removal for dorsiflexion New joint surface eliminates pain Phalangeal Chielectomy/Moburg osteotomy Joint line can be recessed No cartilage left so how do you map surface? Cartilage loss goes Superior→Inferior Use inferior and M/L cartilage references If no cartilage then boney references become the new surface elevations and joint will still be congruent with joint line slightly posterior Can you still do a fusion after this? Yes Remove implant and fixation component, then bone graft for screw arthrodesis Future possibility: remove implant and then use K-wire through fixation component to fuse