Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
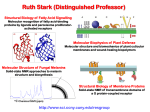
Oral cancer: Insights into etiology and molecular basis and implications for prevention and treatment Nikolaos G. Nikitakis, MD, DDS, PhD Diplomate, American Board of Oral and Maxillofacial Pathology Associate Professor, Dept. of Oral Pathology and Medicine, University of Athens, Greece Lecture Outline The problem Molecular carcinogenesis Methods for studying molecular markers and targets Investigated molecular markers and targets in oral cancer Limitations and challenges Conclusions Oral Cancer Epidemiology The sixth most common cancer worldwide MEN ASR: 5.2/100,000/year WOMEN ASR: 2.5/100,000/year Globocan 2008: Incidence of Oral Cancer Oral cancer Changing trends in oral cancer epidemiology Decrease in the overall incidence of oral and oropharyngeal cancer in the last decades – Decreases in smoking habit Increase in the incidence of cancers in specific anatomic subsites and in younger individuals – ?Role of HPV infection The problem Galen, 130-201 AC Despite significant progress in the fields of surgery, radiotherapy and chemotherapy, oral cancer prognosis remains dismal Clinical and histopathological parameters are not always accurate predictors Available therapeutic modalities are associated with significant side effects and are not always effective The problem To accurately determine diagnosis and prognosis e.g. – the likelihood of malignant transformation (MT) in oral PMD – the possibility of lymph node metastasis (LNM) in oral cancer Hippocrates, 460-370 BC To select the most appropriate treatment – Higher efficacy with less side effects Malignant transformation in oral PMD A subset of oral PMD (e.g. leukoplakia and erythroplakia) will progress into invasive cancer Clinical and histopathological features alone (e.g. degree of epithelial dysplasia) cannot reliably predict which lesions will progress Lymph node metastasis of oral cancer Metastasis of oral cancer to regional lymph nodes: the single most important adverse prognostic factor and indicator of survival – Detection of LNM reduces the 5year survival rates by about 50% Preoperative nodal status assessment is crucial for the selection of the optimal therapeutic approach The use of molecular markers and targets Advanced knowledge of the molecular basis of cancer has prompted the investigation of a number of biomarkers as possible biomarkers and targets Molecular basis of carcinogenesis The various types of cancer represent different diseases characterized by specific molecular alterations The Hallmarks of Cancer Hanahan D, Weinberg RA. Cell 2000:57–70 The hallmarks of cancer and the novel molecular events in OSCC-related inflammation Wu R et al. J DENT RES 2010;90:561-572 Copyright © by International & American Associations for Dental Research Oncogenes and Tumor Suppressor Genes Various genes and corresponding protein products have been found to participate in the regulation of cell proliferation, survival and spreading of cancer cells Oncogenes: promoters of tumor growth Τumor suppressor genes: inhibitors of tumor growth Molecular alterations and monoclonality Carcinogenesis relies on the accumulation of molecular alterations Tumor formation is based on the proliferation of a cellular clone derived from a specific precursor cell with critical molecular alterations The progress of carcinogenesis The various carcinogens act by inducing multiple alterations in critical molecules Theory of biphasic carcinogenesis – Action of initiators and promoters Theory of multistep carcinogenesis “ In the survival of favoured individuals and races, during the constantlyrecurring struggle for existence, we see a powerful and ever-acting form of selection. ” Charles Darwin, 1859 Multistep Carcinogenesis Colon Adenocarcinoma Vogelstein et al. Multistep Oral Carcinogenesis Normal Hyperplasia EGFR 9p21 del p16/p14 Trisomy 7 Telomerase Dysplasia 3p del 17p13 (p53 mut) Tetraploidy SCC CIS 11q13 13q21 8p del Cyclin D1 Aneuploidy 18q del 10q23 3p26 pTEN Califano, Sidransky et al. Field cancerization Presence of one or more mucosal areas harboring cancer-associated genetic or epigenetic alterations Provides an explanation for the high frequency of recurrences and second primary tumors in a large mucosal area Has been associated with – Diffuse exposure to carcinogens – Lateral expansion and migration of a monoclone of genetically altered cells Braakhuis et al. Nat Rev Cancer. 2011;11:9-22. Methods for studying molecular markers Protein assays – – – – Immunohistochemistry ELISA Western blot Proteomics Two dimensional gel electrophoresis Mass spectrometry mRNA assays – RT-PCR (Real Time) – Serial analysis of gene expression (SAGE) – RNA protection assays (RPAS) – Northern blot – Genomics cDNA Microarrays Methods for studying molecular markers DNA & Chromosomes – PCR – Southern blot – Fluorescence in situ hybridization – FISH (multiplex FISH) – Flow cytometry – Comparative genomic hybridization (CGH) – Spectral karyotyping (SKY) and cytogenetics – Gene sequencing for mutational analysis – Single nucleotide polymorphism (SNP) – LOH analysis Restriction fragment length polymorphism analysis Microsatellite analysis Adjuvant techniques – Laser capture microdissection – Tissue microarrays Schema of omics technologies, their corresponding analysis targets, and assessment methods Wu R et al. J DENT RES 2010;90:561-572 Copyright © by International & American Associations for Dental Research Investigated molecular markers and targets in oral PMDs Cytogenetics – Loss of heterozygocity (LOH) – Aneuploidy Cell cycle regulation Loss of Heterozygosity (LOH) Allelic imbalance: One copy of a polymorphic marker may be lost (LOH) or amplified (allelic gain) LOH – loss of normal function of one allele of a gene (in which the other allele was already inactivated) – results in absence of a functional TSG in the lost region Loss of Heterozygosity (LOH) in oral PMDs LOH at 3p, 9p21, 17p13 and 8p22-24 and other loci harboring important TSG (such as p16 and p53) Association with MT rate – Mao et al. 1996: 37% of patients with LOH at 3p and 9p progressed to cancer (vs. 6% of patients without LOH) – Partridge et al. 2000: Up to 75% risk of tumor development if ΑΙ at 2 or more key microsatellite markers Loss of Heterozygosity (LOH) in oral PMDs Association with MT rate – Lee et al. 2000: Original cohort of 70 patients – Zhang et al. 2012: prospective cohort of 296 patients with mild/moderate dysplasia High-risk lesions (3p and/or 9p LOH): 22.6fold increase risk of progression Using additional markers (4q and 17p): 65.4fold increase for the high-risk group Aneuploidy Abnormal number of chromosomes Imbalanced DNA content Percentage of aneuploidy in oral cancer: 50-60% (up to 90%) Aneuploidy in Oral PMDs Percentage of aneuploidy in oral PMDs: 20-45% (up to 83%) Correlation with histological degree of dysplasia Aneuploid lesions may transform to malignancy at a higher rate Torres-Rendon et al. Oral Oncol. 2009;468-73 Aneuploid Aneuploid Diploid Klanrit et al. Oral Oncol. 2007;43:310-6 Cell Cycle Regulation Cyclins and CDKs Rb family p53 family and CDKIs Cdc2 Cell division Cyclin B M Cell prepares to divide Cell grows p18,p19 C C INK4 p15,p16 Cdk4 /6 Cdc2 G1 G2 Cyclin D1/2/3 CIP/KIP p21, p27 Cyclin A Cdk2 Cyclin A C p57 Cdk2 Cyclin E DNA replication S Cyclin D1 in oral PMDs Kovesi et al. J Oral Pathol Med 2006: Correlation of Cyclin D1 expression with clinical severity Cyclin D1 – regulates cell cycle progress through G1 phase – overexpression in oral PMDs – correlation with degree of dysplasia – specific polymorphisms are associated with oral PMDs Retinoblastoma (Rb) and p16 Unphosphorylated Rb binds to and inhibits the transcriptional factor E2F Formation of cyclic D-CDK4 complex results in phosphorylation and inactivation of Rb p16: inhibits cyclin D-CDK4 complex E2F Rb E2F Active Inactive P P Rb E2F DP S Phase Genes Retinoblastoma (Rb) and p16 in oral PMDs pRb loss is associated with transition form hyperplasia to dysplasia p16: positive or negative correlation with degree of dysplasia (surrogate HPV marker) Total Rb Un-p-Rb p53 Guardian of the genome – Regulation of cell cycle, apoptosis, differentiation and DNA repair The most frequently inactivated TSG in cancer p53 and cancer Kussie et al, Science 274:948, 1996 Mechanisms of inactivation – Acquired mutations in both gene alleles – Hereditary p53 mutation – Interaction with HR-HPV E6 protein – MDM2 overexpression and p53 degradation p53 mutation prevalence in human tumors IARC Database, R8 p53 in oral PMDs Non MT MT Cruz et al. J Pathol. 1998;184:360-8 Increased IH detection due to stabilizing mutations and evasion of degradation Correlation with degree of dysplasia and risk of MT remains controversial Cell cycle dysregulation by HR-HPV Leemans et al. Nat Rev Cancer. 2011;11:9-22 Modes of HPV infection von Knebel Doeberitz and Vinokurova Archives Med Res. 2009 Biomarkers of neck metastasis Numerous studies have investigated the role of molecules that directly or indirectly participate in the metastatic cascade – Invasion of extracellular matrix – Vascular dissemination and homing of tumor cells – Angiogenesis and lymphangiogenesis – Miscellaneous Molecular Markers associated with Invasion Adhesion molecules – – – – Cadherins and Catenins Integrins CD44 Ep-CAM Lim et al. Clin Cancer Res 2004: Patients with low expression of E-cadherin should be considered a high-risk group for late cervical metastasis Molecular Markers associated with Invasion Proteolytic enzymes – Matrix metalloproteinases (MMPs) Collagen IV, Tissue inhibitors of metalloproteinases (TIMPs) – Cathepsins (-B, -D, –L) Katayama et al. Clin Cancer Res 2004: Expressions of MMP-9 and TIMP-2 have predictive value for tumor metastases Molecular Markers associated with Angiogenesis and Lymphangiogenesis Angiogenesis: formation of new vessels Prerequisite for the growth of tumor cells in a hypoxic environment Angiogenesis and lymphangiogenesis provide passageways to the circulation that allow metastatic spread Regulators of angiogenesis: – A long list of promoting and inhibiting factors, that exhibit various mechanisms of action Molecular Markers associated with Angiogenesis and Lymphangiogenesis Microvessel density (MVD) – Methology for quantification of angiogenesis and correlation with LNM remain controversial Guttman et al. Oral Oncology 2004: Lymph node metastasis was positively correlated with the microvessel count using the CD-34 marker Anti-CD34 Molecular Markers associated with Angiogenesis and Lymphangiogenesis Sauter et al. Clin Cancer Res 1999: Vascular endothelial growth factor is a marker of tumor invasion and metastasis in squamous cell carcinomas of the head and neck Vascular endothelial growth factor (VEGF) family members: – VEGF-A, -B, -C, -D, -E and PlGF – Bind to VEGF receptors on endothelial cells promoting migration, proliferation and vascular permeability – Play a prominent role in angiogenesis and lymphangiogenesis Molecular Targets in Oral Cancer Aberrant molecular events in oral cancer can serve as potential specific and effective therapeutic targets – Preclinical models Cell lines, Animal models – Clinical trials Phase I, II and III Molecular Targets in Oral Cancer In recent years, novel molecular targeted therapies have been applied in the treatment of oral cancer – Cetuximab (mAb against EGFR) – Erlotinib (TKI against EGFR) – Dual or pan-HER TKIs – Angiogenesis inhibitors (e.g. bevacizumab) – Other inhibitors (against IGF-1R, MET, PI3K/AKT/mTOR) Molecular Targets in Oral Cancer Le Tourneau and Siu, Curr Opinion Oncol 2008;20:256-63 Cell Signaling Dysregulations in cell signaling pathways are frequent and crucial events in carcinogenesis Many signaling pathways are involved in oral oncogenesis – – – – – EGFR/TGF-α TGFβ/SMAD c-MET PI3K/Akt/mTOR Stat3 Molecular Targets in Oral Cancer Howard et al. Oral Oncol. 2012;48:10-7 Stat3 signaling in oral neoplasia TGF-α gp80 IL6 Src JAK JAK EGFR Stat3 JAK gp130 MEKKs Mek1/2 MEK4/7 Mek3/6 Stat3 ERK JNK p38 SOCS PIAS3 Stat3 Bcl-XL Cyclin D1 Survivin IL-6 1a TGF-α 1a 2a IL-6R/ 1b gp130 JAKJAK P P P P P P P P STAT P SRC Cytoplasmic negative regulators (e.g. SHP, SOCS) P 1b P EGFR P STAT 2b STAT dimer P Additional regulation (e.g crosstalk with MAPKs, serine phosphorylation) 2a Nuclear negative regulators (e.g. PIAS, phosphatase) P Transcription of specific target genes (e.g. Bcl-XL, Cyclin D1, VEGF) STAT dimer P Transcriptional Coactivators (e.g. p300/CBP) Nikitakis et al, Current Cancer Drug Targets, 2004, 4, 637-651 Overactivity of upstream kinases and insufficient negative regulation Availability of STAT molecules Recruitment and phosphorylation 1 P STAT dimer 2 Dimerization 3 P Nuclear translocation 4 P 5 DNA binding STAT dimer P 6 Interaction with transcriptional coactivators Transcriptional activation 7 Nikitakis et al, Current Cancer Drug Targets, 2004, 4, 637-651 Molecular targets in Oral Cancer Yedida et al. OOOO. 2013;33:482-9 Limitations and challenges Current inconsistency and lack of validation of obtained results hampers the use of biomarkers in a clinical setting Reasons for inconsistency: – Molecular heterogeneity Patient-specific and lesion-specific – Differences in methodology Use of different protocols and methods for analysis and interpretation of data Limitations and challenges Differences in experimental design – Patient and case selection Epidemiological factors, site, clinical characteristics, histological features Effects of diagnostic and therapeutic interventions Follow-up Study of a limited number of genes and their proteins underestimates the complexity of carcinogenesis: – Limited capacity of any single molecular biomarker to reliably predict outcome in individual patients – No “silver bullet” for the treatment of all oral cancers – Need for an individualized approach Conclusions Significant correlations between specific molecular markers and oral cancer prognosis and susceptibility to treatment have been established Molecular targeted therapies for oral cancer have been introduced and rapidly evolving Conclusions Improved understanding of the molecular basis of oral carcinogenesis, refinement of methodology and study design and further technologic advances will facilitate the discovery of reliable molecular predictors and targets Clinical application awaits further validation through large scale, multicenter, well controlled studies