Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
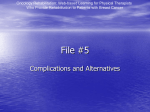
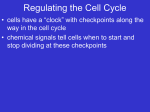
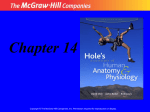
Significance of level III lymph nodes located in the anterior fat recess between the sternocleidomastoid muscle, thyroid cartilage and jugular vein in head and neck tumors Poster No.: C-0678 Congress: ECR 2014 Type: Educational Exhibit Authors: L. Oleaga Zufiría , J. Berenguer , E. Verger , I. Valduvieco , J. 1 2 1 2 2 2 2 Blanch ; Bilbao/ES, barcelona/ES Keywords: Head and neck, CT, Diagnostic procedure, Pathology DOI: 10.1594/ecr2014/C-0678 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 27 Learning objectives To show the anatomy of the anterior fat recess between the sternocleidomastoid muscle, thyroid cartilage/gland and internal jugular vein To describe the fixation jugular vein sign associated to metastatic lymph nodes located in this area To emphasize the relevance of evaluating this region on imaging studies Background The anterior fat recess between the sternocleidomastoid muscle (SCM), thyroid cartilage/ gland, carotid artery and the internal jugular vein (IJV) is a small triangle filled with fat (Figures 1,2). The superior belly of the omohyoid muscle represents the anterior and inferior anatomic landmarkfor this region. Page 2 of 27 Fig. 1: Anatomical boundaries of the anterior fat recess (level III) (yellow triangle). T- Thyroid cartilage, CA- Carotid Artery, IJV- Internal Jugular Vein, SCMSternocleidomastoid muscle. References: Department of Radiology, Hospital Clinic Barcelona Page 3 of 27 Fig. 2: Close view of the anatomical boundaries of the anterior fat recess (level III) (yellow triangle). T-Thyroid cartilage,CA- Carotid Artery, IJV- Internal Jugular vein, SCM- Sternocleidomastoid muscle. References: Radiology Department Hospital Clinic Barcelona It is bordered anterolaterally by the sternocleidomastoid muscle, anteromedially by the thyroid cartilage lamina/gland and posteromedially by the internal jugular vein and the Page 4 of 27 carotid artery. The superior limit is the hyoid bone and the inferior limit is the cricoid cartilage. The deep cervical lymph nodes lie along the course of the internal jugular vein. The vein passes deep to the interval between the two heads of the sternocleidomastoid muscle. Level III contains the middle jugular lymph nodes located around the middle third of the IJV. It is the caudal extension of level II. The upper level II lymph nodes lye along the lateral and anterior margins of the internal jugular vein; however the lymph nodes in the anterior margin nearly disappear in the middle group. It is limited cranially by the inferior edge of the body of the hyoid bone, and caudally by the inferior edge of the cricoid cartilage. The anterior limit is the posterolateral border of the sternohyoid muscle and the anterior border of the SCM muscle, and the posterior limit is the posterior edge of the SCM muscle Laterally level III is limited by the medial edge of the SCM muscle and medially by the medial edge of the internal carotid artery and the scalenius muscles. Level III receives efferent lymphatics from levels II and V, and some efferent lymphatics from the retropharyngeal, pretracheal and recurrent laryngeal nodes. It also receives the lymphatics from the base of the tongue, tonsils, larynx, hypopharynx and thyroid gland. Level III nodes can be located in the anterior fat recess or in the posterior fat recess. Lymph nodes located in the anterior fat recess can go unnoticed. This is a narrow region with closed anatomical limits (Figure 3). Page 5 of 27 Fig. 3: Level III lymph node in the anterior fat recess. ln- lymph node, T- Thyroid gland, CA- Carotid Artery, IJV- Internal Jugular Vein, SCM- Sternocleidomastoid muscle. References: Radiology Department, Hospital Clinic Barcelona Most level III nodes are located in the posterior fat recess, this is a wider space with no anatomical tight boundaries, lymph nodes in this recess are easier to depict on imaging studies (Figures 4,5). Page 6 of 27 Fig. 4: Posterior fat recess (blue triangle). T- Thyroid, CA- Carotid Artery, IJV- Internal Jugular Vein, SCM- Sternocleidomastoid muscle. References: Radiology Department, Hospital Clinic Barcelona Fig. 5: Diagram showing both the anterior (yellow triangle) and posterior fat recesses (blue triangle), corresponding to the location of level III lymph nodes. Page 7 of 27 References: Radiology Department, Hospital Clinic Barcelona Imaging techniques are important tools that can improve the accuracy of nodal neck staging for better management of patients with head and neck tumors. Recently, several authors have advocated the concept of limited treatment; selective neck dissection and/or selective neck irradiation, for limited stage tumors and there have been established consensus guidelines (DAHANCA, EORTC, GORTEC) and in North America (NCIC, RTOG) on how to treated nodal disease in head and neck tumors. It has been suggested that more selective treatment could decrease the radiation dose on critical organs such the parotids, but an inadequate selection of target volumes could have negative effects on disease control and prognosis. Detection and classification of metastatic lymphadenopathy on imaging, in patients with head and neck tumors, relays upon evaluation of nodal morphology and size. Nodal size is one of the most important morphologic features to detect metastatic nodal disease from head and neck tumors. However the sensitivity and specificity of morphologic and size criteria is limited. Images for this section: Page 8 of 27 Fig. 1: Anatomical boundaries of the anterior fat recess (level III) (yellow triangle). T- Thyroid cartilage, CA- Carotid Artery, IJV- Internal Jugular Vein, SCMSternocleidomastoid muscle. Fig. 2: Close view of the anatomical boundaries of the anterior fat recess (level III) (yellow triangle). T-Thyroid cartilage,CA- Carotid Artery, IJV- Internal Jugular vein, SCMSternocleidomastoid muscle. Page 9 of 27 Fig. 9: (Table 1) Relation of patients with level III lymph nodes located in the anterior fat recess with the fixation sign in the anterior wall of the jugular vein Page 10 of 27 Fig. 3: Level III lymph node in the anterior fat recess. ln- lymph node, T- Thyroid gland, CA- Carotid Artery, IJV- Internal Jugular Vein, SCM- Sternocleidomastoid muscle. Page 11 of 27 Fig. 6: Normal lymph node in the anterior fat recess. No depression or fixation of the anterior wall of the jugular vein (yellow arrows). Page 12 of 27 Fig. 7: Small metastatic lymph node with no size criteria for malignancy, producing depression and fixation of the anterior wall of the jugular vein (red arrows). Page 13 of 27 Findings and procedure details Petite normal lymph nodes can be found in the anterior fat recess (Figure 6). Fig. 6: Normal lymph node in the anterior fat recess. No depression or fixation of the anterior wall of the jugular vein (yellow arrows). References: Radiology Department Hospital Clinic Barcelona Small metastatic lymph nodes, with no size criteria for malignancy, growing in the carotid triangle can infiltrate local structures such the jugular vein, producing fixation and depression of the anterior wall (Figure 7). Page 14 of 27 Fig. 7: Small metastatic lymph node with no size criteria for malignancy, producing depression and fixation of the anterior wall of the jugular vein (red arrows). References: Radiology Department, Hospital Clinic Barcelona The jugular vein wall fixation can represent the first sign of malignancy, before the metastatic lymph nodes enlarge to a size considered pathologic. It is important to check for nodes located in this recess and always look for this sign. The posterior triangle compartment is larger with no tight boundaries, lymph nodes can enlarge with no effect on the jugular vein wall (Figure 8). Page 15 of 27 Fig. 8: T4N2c left pyriform sinus tumor. Large level III lymph node (LN) in the posterior triangle, pushing and producing a small deformity on the psoterior wall of IJV (red arrow). References: Radiology Department, Hospital Clinic Barcelona We present 19 cases of head and neck tumors with level III nodes in this anterior fat recess with the associated fixation and depression sign on the jugular vein. Page 16 of 27 Fig. 9: (Table 1) Relation of patients with level III lymph nodes located in the anterior fat recess with the fixation sign in the anterior wall of the jugular vein References: Department of Radiology, Hospital Clinic Barcelona Page 17 of 27 Fig. 10: T1N0 lateral right lingual edge squamous cell carcinoma. Small lymph node with no size criteria for malignacy, no necrosis or extranodal extension (red arrow). On CT a depression of the anterior wall of the IJV is depicted (small red arrows). The patient underwent surgery of the lingual mass with no lymphadenectomy. References: Radiology Department, Hospital Clinic Barcelona Page 18 of 27 Fig. 11: Same patient as the one shown in Figure 8. Six months after surgery The same lymphn node has increased in size (red arrow), with more depression of the anterior wall of the IJV (small red arrows). Lymphadenectomy performed this time revealed metastatic squamous cell carcinoma. References: Radiology Department, Hospital Clinic Barcelona Page 19 of 27 Fig. 12: T4N2b supraglottic tumor. Small level III lymph node in the anterior fat recess(red arrow), demonstrating the depression and fixation sign on the anterior wall of the IJV (small red arrows). References: Radiology Department, Hospital Clinic Barcelona Page 20 of 27 Fig. 13: Same patient as Figure 12. After treatment with Chemotherapy and Radiation the lymph node has desappeared and the IJV recovers the usual shape. References: Radiology Department, Hospital Clinic Barcelona Page 21 of 27 Fig. 14: T3N1 right laryngeal tumor. Right level III lymph node with the fixation sign on the anterior wall of IJV (small red arrows). Surgery+Lymphadenectomy. Histology demonstrated squamous cell infiltration in level III node. References: Radiology Department, Hospital Clinic Barcelona Fig. 15: T2N1 left pyriform sinus tumor. Small left level III node in the anterior recess, showing the fixation sign on the anterior wall of IJV (red arrows). Page 22 of 27 References: Radiology Department, Hospital Clinic Barcelona Fig. 16: T2N1 left pyriform sinus tumor after Chemotherapy and Radiotherapy, same patient as the one shown in Figure 15. The small left level III node in the anterior recess has decreased in size and the IJV has recover the regular shape (yellow arrows). References: Radiology Department, Hospital Clinic Barcelona Page 23 of 27 Fig. 17: T4N2b supraglottic tumor (T). Level III large lymph node with necrosis and fixation sign in the anterior wall of the IJV (red arrows) References: Radiology Department, Hospital Clinic Barcelona The depression and fixation sign of the IJV may be useful to identify pathologic lymph nodes without morphological or size to be considered such. It can contribute to improved N staging of head and neck tumors, allowing to better plan selective surgery and/or radiotherapy. Images for this section: Page 24 of 27 Fig. 16: T2N1 left pyriform sinus tumor after Chemotherapy and Radiotherapy, same patient as the one shown in Figure 15. The small left level III node in the anterior recess has decreased in size and the IJV has recover the regular shape (yellow arrows). Page 25 of 27 Conclusion Optimal outcome in squamous cell carcinomas of the head and neck depends on effective management of cervical lymph nodes. Selective removal of lymph node groups at risk, or modified neck dissections are appropriate in many patients. Careful selection of the type of neck dissection and the use of postoperative radiation therapy can optimize treatment and improve the prognosis and quality of life of these patients. Proper nodal staging using imaging studies can lead to a better therapeutic decision. We believe it is important to look for lymph nodes in the anterior fat recess and check for the internal jugular vein fixation sign on imaging studies (CT and MRI) to detect and recognize lymphadenopathies even if they do not fulfill size criteria to be considered as pathologic. We want to emphasize the relevance of identifying lymph nodes in this recess with the fixation sign in the jugular vein that may go unnoticed because most of the lymphadenopathies at level III are located in the posterior triangle. Personal information Laura Oleaga Hospital Clinic Barcelona. Spain [email protected] References 1- Essig H., , Warraich R., Zulfiqar G., 2, Rana M., 1, Eckardt A., 1, Gellrich N., Rana M. Assessment of cervical lymph node metastasis for therapeutic decision-making in squamous cell carcinoma of buccal mucosa: a prospective clinical analysis. World Journal of Surgical Oncology 2012 10:253 Page 26 of 27 2- Ojiri H., Mancuso A., Mendenhall W., Stringer S. Lymph nodes of patients with regional metastases from head and neck squamous cell carcinoma as a predictor of pathologic outcome: size changes at CT before and after radiation therapy. AJNR Am J Neuroradiol 2002; 23:1627-1631 3- Zhang Z., Helman J., Li L. Lymphangiogenesis, lymphatic endothelial cells and lymphatic metastasis in head and neck cáncer. A review of mechanisms. Int J Oral Sci 2010; 2: 5-14 4- Bartlett E., Walters T., Yu E. Can axial-based nodal size criteria be used in other imaging planes to accurately determine ''enlarged'' head and neck lymph nodes?. ISRN OtolaryngologyVolume 2013, article IG 232968, 7 pages 5- Corlette T., Cole I., Albsoul N., Ayyash M. Neck dissection of level IIb: Is it really necessary?. Laryngoscope 2005; 115: 1624-1626 Page 27 of 27