Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
23
Chapter 2
The role of the sympathoadrenal system in exercise
Exercise calls for an acute increase in oxygen and fuel supply to the contracting
muscle, and these needs are met through the sympathoadrenal (SA) activation of
cardiorespiratory system and through the release and increased utilization of metabolic
fuels. Increased metabolism during exercise can deplete fuel resources and exceed the
capacity of homeostatic mechanisms to maintain constancy of interior environment.
During the recovery from exercise, the parasympathetic (PS) and enteric divisions of the
autonomic nervous system (ANS) coupled with various behavioral responses correct
the deviations in the internal environment and mediate trophic and growth-promoting
functions.
Endocrine messengers control many of the same functions as does ANS in
exercise. Although endocrine and autonomic systems are capable of acting in isolation,
a fact that has fostered an artificial notion of their functional separation, in reality they
work in concert and engage in complex reciprocal interactions. The ANS plays a central
role in coordinating the neural and hormonal responses to exercise and recovery from
exercise. Although the sympathetic (S) activation usually produces "fear, fight, or flight
response" (Cannon, 1929), that is, a global activation of a large number of functions, it
can also differentially activate only some actions in response to particular stressors
such as hypoglycemia (Young et al 1984). Autonomic, endocrine and behavioral
compensatory responses cooperate in regulation of the internal environment. This
chapter addresses the functional role of the ANS and its involvement and interactions
with the chemical messengers in exercise.
Autonomic nervous system controls visceral functions necessary for the
maintenance of the internal environment. It consists of three divisions: sympathetic
(SNS), parasympathetic (PNS), and enteric (ENS). The functions of the three divisions
of the ANS are to increase cardiorespiratory function and metabolism, biosynthetic
processes, and nutrient digestion and absorbtion, respectively. The S and PS divisions
include receptors, sensory nerves and associated ganglia, central nervous centers
subserving integration of autonomic responses, and motor nerves and associated
ganglia innervating the smooth muscles and endocrine and exocrine glands (the
viscera), although traditionally only the motor component of this complex system has
been recognized as ANS and discussed. The viscera are the origin of dual sensory
input to the central nervous system via S and PS afferent neurons that travel along with
efferent fibers in respective autonomic nerves. S receptors sense pain and PS receptors
monitor chemical, endocrine and mechanical changes in the visceral organs. The
smooth muscles and endocrine and exocrine glands receive dual motor innervation
from both S and PS neurons with the exception of sweat glands which receive only S
innervation.
23
24
Another feature of the ANS is that
the autonomic efferent nerves
consist of two nerve cells, a preganglionic and a postganglionic neuron (Figure 16). The
PS preganglionic cells have longer axons than the S pregangionic neurons and synapse
with postgangionic neurons in ganglia that lie close to, or within, the walls of smooth
muscles and glands. The S preganglionic cells are shorter and form synapses in the
ganglia in paired paravertebral sympathetic trunks adjacent to the spinal cord or in
prevertebral ganglia (solar plexus) located at the points where celiac, superior, and
inferior mesenteric arteries branch from the aorta.
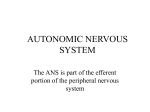
Figure 16. Composition and neurotransmitters of autonomic motor nerves.
The autonomic efferent nerves consist of a preganglionic and a postganglionic cell.
ACH is the neurotransmitter in preganglionic SNS and PNS cells, and it activates
nicotinic receptors (NR) on postganglionic cells. Preganglionic PS cells are longer than
S preganglionic cells because S ganglia are located some distance from target tissues
and PS ganglia are located adjacent or inwalls of target tissues. Postganglionic PS
cells use ACH as a messenger and it acts muscarinic receptors (MR). Postganglionic S
neurons use NE as neurotransmitter, and adrenal medullary cells (developmentally
derived from S postganglionic cells), a mixture of NE and E. Catecholamines (NE and
E) activate adrenergic receptors (AR).
____________________________________________________________________
Both types of preganglionic neurons use ACH as a neurotransmitter and activate
nicotinic cholinergic receptors on postganglionic neurons (Figure 16). The
postganglionic PS neurotransmitter is ACH which activates muscarinic cholinergic
receptors on target cells. The S postganglionic neurons release NE and predominantly
act on alpha adrenergic receptors on target cells. The exception are fibers to the sweat
glands which, like the postganglionic PS neurons, release ACH as a neurotransmitter
24
25
and act on muscarinic receptors. The
chromaffin cells of the adrenal medulla
differentiate under the influence of cortisol into endocrine cells capable of converting NE
into E (Figure3). In addition to NE, other chemical messengers have been found in
sympathetic postganglionic neurons. The neuropeptide Y (NPY, Pernow & Lundberg,
1988) and the ATP (Burnstock & Kennedy 1986) are colocalized with NE and are
implicated in vasomotor control. The calcitonin gene-related peptide (CGRP) and the
vasoactive intestinal polypeptide (VIP) are colocalized with ACH (Landis & Fredieu
1986) and participate in sudomotor control.
The sympathetic division of the ANS.
The S afferents transmit pain or nociceptive information from the viscera in S
nerves to the higher brain centers where it reaches consciousness (Cervero &
Foreman, 1990), and their cell bodies are in segmental dorsal root ganglia (Figure 17).
In contrast to PNS, S afferent input contributes only 20% of fibers to the splanchnic
nerves, and most of these fibers are unmyelinated. The S sensory fibers project to
laminae I and V in the the spinal gray matter of the thoracic and upper two lumbar spinal
segments. Here they are joined by ten times more numerous sensory fibers from
receptors in the muscles and the skin. Because of the quantitatively limited afferent S
input and convergence of visceral and the more numerous somatic afferents, visceral
pain is generally referred to skin areas. The heart pain in angina pectoris is felt in the
superficial areas of arms and upper chest, while the pain in esophagus, gall bladder and
duodenum is referred to the overlying superficial areas of the body (Wall & Melzack,
1985).
The visceral nociceptive information is transmitted in several centripetal
pathways to the higher brain centers (Figure 18) from where the autonomic, emotional,
and behavioral responses are organized. The lateral (LSTT) and medial spinothalamic
tracts (MSTT) carry, respectively, the information about the location of the pain from
neurons in laminae I and V, and about tonic aspects of pain, associated with
motivational and emotional responses, from deeper parts of spinal gray matter to the
ventroposterolateral and medial thalamus, respectively (Figure 18). The spinoreticular
tract to pontine reticular formation, and the spinomesencephalic tract to brachium
conjunctivum (BC) and the periaqueductal gray (PAG) in the pons, that end in thalamus
and cortical pain areas, are additional relays for pain . Pain afferents also reach the
lateral hypothalamic area (LHA) and brainstem nuclei (nucleus of the tractus solitarius,
NTS and parabrachial nucleus (PB), that are involved in the central integration of
autonomic function (Menetrey & Basbaum, 1987).
25
26
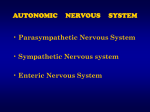
Figure 17. Anatomical arrangement of the S nerves
The arrangement of afferent and efferent (right) S nerves form a spinal reflex arc. The
bodies of visceral afferent neurons (left) are located in the dorsal root ganglia, and their
central dendrites synapse with neurons in laminae I and V of the gray matter in the
spinal dorsal horn. Their peripheral dendrite travels through the white ramus (WR) of
the spinal nerve, the S ganglion, and splanchnic nerve to peripheral pain receptors.
PS afferents can make contact with and influence postganglionic S neurons in
prevertebral ganglia. S neurons that innervate blood vessels of the skin and muscle
(A) terminate in the paravertebral ganglia. Their postganglionic cell leaves the S trunk
in gray communicating rami (GR) and reach the skin in segmental somatic nerves.
Preganglionic S neurons that innervate the gastrointestinal tract (B) traverse the
paravertebral ganglia to form synapses with postganglionic cells in prevertebral gangia.
Spinal internuncial neurons connect afferent and preganglionic neurons and are the
anatomical basis of the simplest autonomic reflexes.
____________________________________________________________________
26
27
Figure 18. Projections of the afferent S fibers
S fibers carry information about visecral pain from laminae I and V of the spinal gray
matter to the thalamus (A) in the lateral and medial spinothalamic tracts, to the
brainstem reticular formation (B) in the spinoreticular tract, and to the BC and
periaqueductal gray (C) in the spinomesencephalic tract.
BC=brachium conjunctivum, IC=inferior colliculus, ML=medial lemniscus, NC= central
nucleus of the thalamus, PT=pyramidal tract, PAG=periaqueductal gray, SC= superior
colliculus, TG= tegmental gray in the brainstem reticular formation, VPL=
ventroposetrolateral nucleus of the thalamus.
_____________________________________________________________________
The outcome of S activation is increased cardiorespiratory function, constriction
of all or selected vascular beds and mobilization and increased utilization of metabolic
fuels. While definitive identification of circuits selectively responsible for these effects is
not complete, a limitied number of forebrain and brain stem areas have been implicated
27
28
in the integration of autonomic sensory
input and direct facilitation of S outflow.
They are (Figure 19), insular cerebral cortex, paraventricular hypothalamic nucleus
(PVN), A5
Figure 19. Brain controls of S outflow
The excitatory brain areas with connections to preganglionic cells in the IML area of the
spinal cord are insular cerebral cortex, paraventricular nucleus of the hypothalamus
(PVN, plane A), the noradrenergic cell groups in the pons (A5, plane B) and medulla
(A1, plane C), and RVLM and caudal raphe nuclei in the medulla (plane C)..
IML=intermediolateral column of the spinal gray matter, PVN=paraventricular
hypothalamic nucleus, raphe obscurus and pallidus =caudal raphe nuclei, RVLM=
rostral ventrolateral medulla.
___________________________________________________________________
28
29
noradrenergic cell group and
reticular formation in the pons, and
in the medulla, noradrenergic A1 cell group,caudal raphe nuclei (obscurus and pallidus)
and reticular rostral ventrolateral medullary nucleus (RVLM). The insular cerebral cortex
is involved in emotions of startle, fear and rage that influence cardiorespiratory function
because of the connections with the hypothalamic and brainstem sympathoexcitatory
circuit (Cechetto & Saper, 1990). The PVN is thought to be the key coordinator of the
entire autonomic outflow (Brown & Fisher, 198 , Luiten et al., 1987, Strack et al. 1989)
and through its chemically-coded neurons to play a key role in the regulation of body
fluids and energy and immune responses (see later). Another hypothalamic area, the
dorsomedial nucleus (DMN) has been implicated in patterning of respiratory and
locomotor rhythm during exercise (Eldridge 1985, Marshall & Timms, 1980). The
catecholamine A1 and A5 cell groups provide noradrenergic input, and A5
noradrenergic cells may control regional redistribution of blood from the viscera to
themuscle (Stanek et al, 1984) that occurs during exercise. The caudal raphe nuclei
provide serotonergic activating influence to S outflow. Raphe nuclei also contain TRH
and substance-P releasing neurons (Guyenet 1990).
A characteristic of these S centers is that they are tonically active, and the RVLM
neurons in the medullary reticular formation that include NE fibers also impose a
rhythmic discharge pattern to cardiac and respiratory neurons. The RVLM neurons are
also responsible for the vasoconstrictor tone (Gebber 1990, Guyenet 1990, Loewy,
1990). The are caudal to the Botzinger complex that initiates and times respiratory
movements (Richter & Spyer, 1990), and this provides a neural basis for the respiratory
control over cardiovascular function. The brain areas that generate a S response are
integrative centers that receive both S and PS input, project to both S and PS
preganglionic neurons, and have complex reciprocal connections.
The paraventricular hypothalamic nucleus (PVN) deserves special notice because of its
central role in coordination of S responses, regulation of energy and fluid balance, and
activation of immune response. The PVN has three functionally differentiated parts that
can have discrete actions or act together. The lateral part of PVN (and the supraoptic
nucleus, SO) are magnocellular (Figure 20), and their large cells synthetize hormones
AVP or ADH and oxytocin (OXY), transport them in axons along with neurophysins I
and II that are byproducts of prohormone processing, through the hypothalamohypophyseal stalk, and store them in posterior pituitary (Harris & Loewy, 1990). The
AVP and OXY are released into capillaries of the inferior hypophyseal artery and reach
systemic circulation through efferent veins. The magnocellular SO and PVN neurons
discharge in a characteristic bursting pattern, and their coordinated discharge is
facilitated by cell coupling through tight junctions . The two AVP secreting nuclei receive
projections from brain areas involved in body fluid regulation and from autonomic
centers that regulate cardiovascular function. Two of the eight circumventricular organs
(CVOs) and MPON are structures involved in regulation of body fluids that have neural
connections with PVN. The CVOs are brain areas without the blood-brain barrier with
29
30
receptors that allow them to monitor
and, in
chemical changes in systemic circulation
Figure 20. Role of PVN in antidiuresis and cardiovascular control.
The lateral, magnocellular part of the PVN along with the SO nucleus
participates in release of AVP (and OXY). Sensory information from angiotensin II
receptors in SFO, from osmoreceptors and sodium receptors in SFO and OVLT and
from atrial receptors and arterial baroreceptors reaches the PVN and leads to release of
AVP and antidiuretic action on the kidney. At higher stimulus intensities, greater
amounts of AVP are released to also influences the cadiovascular system by
enhancing baroreflex, increasing neurotransmission in S ganglia, and by causing
30
31
peripheral vasoconstriction. The
circumventricular organs (ME, OVLT, PB,
PP, OVLT, SCO, and SFO) are shown in the upper left .
AVP= arginine vasopressin, ME=median eminence, OC=optic chiasm, OVLT=
organum vasculosum of lamina terminalis, P=pineal gland, PP=posterior pituitary gland,
PVN=paraventricular hypothalamic nucleus, SCO= subcommissural organ,SO=
supraoptic hypothalamic nucleus.
_____________________________________________________________________
some of them, in cerebrovascular space. Among the CVOs, AP is involved in the control
of both food and fluid homeostasis and receives input from carotid baroreceptors,
vagus, and dorsomedial and PVN hypothalamic nuclei.
It sends projections to the commissural NTS and PB nucleus (Johnson & Loewy,
1990). The OVLT acts as central osmoreceptor and sodium receptor, and SFO has
receptors for angiotensin II as well as osmoreceptors and sodium receptors. The
cardiovascular involvement of the magnocellular PVN includes a tonic inhibition by atrial
receptors and the baroreceptors, input from A1 noradrenergic cells secreting NE and
NPY, C1 adrenergic cells acting on alpha1 receptors, and pontine and tegmental
projections (Harris & Loewy, 1990).
The AVP is secreted in response to hypovolemia signalled by atrial receptors, to
fall in blood pressure detected by arterial baroreceptors, and to increased osmolarity
detected by osmoreceptors. The AVP has two effects, an antidiuretic effect on the V2
receptors on distal convoluted tubules in the kidney (hence the term ADH), and at
higher concentrations associated with massive fluid losses, a vasoconstrictor action.
The vasoconstrictor effect is the outcome of threefold AVP action, on the brain
(probably on the CVO AP) where it potentiates baroreflexes (Cowley et al., 1984), on
the sympathetic ganglia where it enhances neurotransmission (Peters & Kreulen, 1985),
and on the on V1 receptors on smooth muscle of blood vessels where it causes
contraction (Altura & Altura, 1984).
The AVP can also be released in response to activation of pain receptors (group
III, myelinated and IV, unmyelinated) in muscles and their arteries, or by injection of
bradykinin (Yamashita et al, 1984). This is the probable mechanism of reflex AVP
release during intense isometric exercise . Reduction in muscle blood flow raises
metabolite concentration and triggers a reflex increase blood pressure (metaboreflex)
through muscle arteriole vasoconstriction caused by both by increased S discharge
(Rowell & O'Leary, 1990) and increased AVP release.
31
32
Figure 21. Role of PVN in CRF release and in S elicitation of E secretion.
The medial parvocellular part of the PVN (horizontal hatching) secretes CRF into
hypophyseal portal vessels in the external layer of the ME. CRF stimulates release of
ACTH from the anterior pituitary, and the ACTH, in turn, stimulates cortisol secretion
from the adrenal cortex. The dorsal and ventral portions of the PVN (vertical hatching)
are involved in activation of S outflow and adrenomedullary E secretion. Cortisol also
stimulates biosynthesis of E in the adrenal cortex, and E stimulates ACTH secretion
from the pituitary.
__________________________________________________________________
The medial PVN contains small cells ("parvocellular") that synthesize CRF and
secrete this hormone into the hypophyseal portal vessels in the external layer of the
median eminence (ME, Figure 21). The CRF stimulates the anterior pituitary
corticotrophs to secrete ACTH from the POMC precursor (Figure 12). The ACTH, in
turn, stimulates cortisol secretion from the fascicular zone of the adrenal cortex (Figure
6).
32
33
Figure 22. Role of PVN in activation of immune response.
The PVN controls S outflow to lymphoid organs, spleen, thymus, bone marrow and
lymph nodes and release of activated immune cells from lymphoid organs. Monocytes
and microphages release IL-I which stimulates CRF release from the parvocellular
PVN. IL-1 may reach the PVN through circulation, by paracrine action from monocytes
that migrate out of blood vessels into brain tissue, or from neural hypothalamic circuits
that use IL-1 as a neurotransmitter. Besides its action on CRF neurons, IL-1 may
directly stimulate ACTH production from pituitary corticotrophs. The cortisol that is
released as a result of ACTH stimulation of adrenal cortex, inhibits IL-1 production
probably through negative feedback at the PVN.
ACTH=adrenocorticotropic hormone, CRF=corticotropin releasing factor, IL1=interleukin-1.
__________________________________________________________________
33
34
The parvocellular part of PVN is
sensitive to corticosteroid feedback,
and almost all of PVN stimulatory actions on food intake and ingestion of carbohydrates
to NE stimulation of alpha2 receptors and to NPY administration (Tempel & Leibowitz,
1993) require glucocorticoid presence and feedback. Although the remaining dorsal and
ventral portions of the PVN are involved in the activation of sympathetic outflow and
adrenomedullary E secretion, their elicitation of E release (Figure 22) also depends on
presence and action of CRF (Fisher et al. 1982). In effect, PVN appears to be one of the
few brain centers that regulates the entire S outflow (Strack et al, 1989). In addition to
the facilitatory role of CRF in S outflow from the PVN, cortisol also stimulates
biosynthesis of E in the adrenal medulla and E stimulates ACTH secretion from the
pituitary thus illustrating multiple reciprocal interactions between PVN endocrine and
autonomic actions.
The parvocellular PVN also plays two key roles in the control of immune
responses (Figure 22). As the center controlling the S outflow, PVN is involved in the
stimulation of lymphoid organs, spleen, thymus, bone marrow and lymph nodes which
receive direct S innervation (Friedman & Irwin, 1997). An important outcome of such
stimulation (Hori et al., 1995) during stress and exercise (Mackinnon 1992) is release of
activated immune cells from lymphoid organs. The interleukin-1, a chemical mesenger
released from activated macrophages and monocytes, triggers CRF release from
parvocellular PVN (Berkenbosch et al. 1987). The IL-1 may reach PVN through
circulation, by paracrine action from monocytes and microphages that migrate out of
blood vessels into brain tissue, or from neural hypothalamic circuits that use IL-1 as a
neurotransmitter. Thus in stress, the SNS activates the immune response, and the
immune-system chemical messengers stimulate in turn the pituitary stress response.
Besides its action on CRF neurons, the IL-1 may directly stimulate ACTH production
from pituitary corticotrophs (Ruzicka & Akil, 1995). The cortisol that results from the
ACTH stimulation of adrenal cortex, inhibits IL-1 production probably through a negative
feedback at the PVN (Uehara et al. 1989).
The cell bodies of S preganglionic neurons are located in the intermediolateral
column (IML) of the spinal gray matter (Figure 17). Although there are about 25 pairs of
segmental paravertebral ganglia extending from the cranial through the sacral end of
the spinal cord, the preganglionic S nerves leave the spinal cord only through the 12
thoracic and the first two lumbar segments and thus form the thoracico-lumbar S outflow
(Figure 23). From the IML column, their myelinated axons leave the spinal cord in white
communicating rami to synapse on S ganglia. Some preganglionic fibers terminate on
neurons in S trunk ganglia. The neurons destined to sweat glands, blood vessels and
piloerector muscles of the skin, leave paravertebral ganglia through the gray
communicating rami and travel in segmental somatic nerves (Figure 17).
34
35
Figure 23. General plan of autonomic ganglia and nerves.
The superior cervical, middle cervical, stellate and about 22 pairs of segmental ganglia
form the paired paravertebral S trunks adjacent to the spinal cord. The celiac, superior
mesenteric, and inferior mesenteric ganglia are called prevertebral S ganglia (or solar
plexus), and they lie some distance from the spinal cord at branching points of the
celiac, superior mesenteric and inferior mesenteric arteries from the aorta.
Preganglionic S outflow is through the thoracic and the first two lumbar segments.
These neurons either form a synapse in the paravertebral ganglia or pass through these
ganglia in greater thoracic (gtsn), lesser thoracic (letsn), lowest thoracic (ltsn), and
lumbar splanchnic nerves (lsn) to form synapses in prevertebral S ganglia.
Postganglionic S fibers then make contact with smooth muscles and glands throughout
the body. The PS nerves leave the spinal cord in four cranial nerves, oculomotor (III),
facial (VII), glossopharyngeal (IX) and vagus (X), and in pelvic splanchnic nerves arising
in sacral spinal cord . The postganglionic PS neurons in the first three cranial nerves
35
36
innervate head and neck glands and
smooth muscles, pelvic splanchnic nerves
innervate genital organs and glands and the hind gut, and the vagus nerve all other
visceral organs throughout the body. The geniculate, petrosal and nodose ganglia
contain afferent cell bodies of facial, glossopharyngeal and vagus afferent fibers,
respectively.
__________________________________________________
The first three pairs of paravertebral ganglia, the superior cervical, the middle
cervical and the stellate, are located in the neck, from where the postganglionic fibers
from the first one innervate the eye, the glands and the smooth muscles of the head.
When the SNS is activated during exercise or in stress, dilator muscles to the pupil
contract causing pupilary dilatation (Loewy, 1990a). The fibers from the other two
ganglia, along with the postganglionic neurons from the first five thoracic ganglia,
project to the heart, lungs, bronchi and trachea as the thoracic S cardiac nerves (Figure
23).
Some preganglionic S neurons do not form synapses in the paravertebral ganglia
but instead travel (Figure 17) in splanchnic S nerves to prevertebral ganglia. The
neurons from fifth through twelfth thoracic segments travel in the greater, lesser and
lowest thoracic splanchnic nerves to synapse with postganglionic neurons in the celiac
ganglion and in the adrenal medulla (Figure 23). Their postganglionic neurons then
reach the foregut and its associated organs and the kidney. The preganglionic neurons
from the third and fourth lumbar segments of the spinal cord travel in lumbar splanchnic
nerves to the superior and inferior mesenteric ganglia. Their postganglionic neurons
innervate, respectively, the mid-gut, and the hind-gut and the pelvic organs.
The parasympathetic division of the ANS.
The PS afferents principally convey sensory information from the viscera, the
tongue, and the smooth muscle and participate in reflexes controlling lung inflation,
heart rate, blood pressure, plasma volume, digestion, and energy regulation. Most of
this sensory information does not reach cerebral cortex and is not consciously
perceived. An exception is taste information that is consciously perceived and
associated with affective states, and the role glucose and sodium receptors play in
specific cravings, respectievly for sweet or salty substances in situations of energy
deficit and sodium deficiency. The PS afferent fibers are about four times more
numerous than the efferent fibers in the PS nerves (Prechtl & Powley, 1990). The cell
bodies of PS afferent neurons are in the ganglia of cranial nerves (for instance,
geniculate ganglion of the VII nerve, petrosal ganglion of the IX nerve, and nodose
ganglion of the vagus nerve) and in the sacral dorsal root ganglia. The receptors
innervated by PS afferent fibers include mechanoreceptors, chemoreceptors, special
ion (sodium) receptors and hormone receptors.
Four sets of mechanoreceptors monitor blood pressure in peripheral circulation
36
37
(Spyer, 1990). The high-pressure arterial
baroreceptors in the carotid sinuses and
the aortic arch, and the renal baroreceptors in the juxtaglomerular apparatus (JGA)
sense changes in systemic blood pressure. The low-pressure atrial receptors at the
confluence of great veins with the atria monitor changes in plasma volume and venous
return to the heart. The stretch receptors in the lungs and the airways react to alveolar
stretching. The arterial baroreceptors relay blood pressure information to the central
nervous system (CNS) through the sinus nerve, a branch of glossopharyngeal nerve,
and the other mechanoreceptors through the vagus nerve. Different receptors project
both to discrete regions of the NTS and to a common integrative area (commissural
NTS).
The osmoreceptors, sodium receptors and angiotensin II and atrial natriuretic
factor (ANF) receptors for hormones involved in body fluid homeostasis are located in
CVOs (Johnson & Loewy,1990). The chemoreceptors monitoring changes in arterial
pCO2 and pO2 are located in the carotid body, aortic sinus and the ventral surface of
medulla oblongata. Additional chemoreceptors are located in the muscles where they
monitor changes in the metabolic state (Kniffki et al. 1981) and promote
cardiorespiratory responses to exercise (Kaufman et al 1983).
Chemo- and mechanoreceptors that monitor stimuli associated with ingestion
and digestion of nutrients include stretch receptors in the stomach, chemoreceptors in
liver, stomach, duodenum, and brain that detect changes in concentration and
availability of nutrients and hormones, and taste receptors. As all but taste are located
within the gastrointestinal tract and associated organs or the brain areas receiving their
afferents, they will be discussed in the section on the ENS.
The taste receptors are chemoreceptors located on the tongue, epiglottis and
soft palate (Figure 24). Taste receptors in the fungiform papillae on the anterior two
thirds of the tongue relay sensory information in the chorda tympani nerve, a branch of
the facial nerve. Taste information from the circumvallate and foliate papillae at the back
of the tongue travels in lingual, a branch of the IX th nerve . Additional taste afferents
from the epiglottis and soft palate travel, respectively in the vagus and a branch of the
facial nerve. The taste afferents project to the most rostral part of the NTS, from where
some projections go to the motor nuclei of cranial nerves that control chewing and
swallowing, and the others ascend to PB nucleus (pontine taste area), hypothalamus
(LH and PVN), limbic forebrain (CNA, BNST, and substantia innominata,SI), and taste
area of the insular cortex (Loewy, 1990).
37
38
Figure 24. Taste afferents and their CNS projections
Taste receptors in the anterior tywo thirds of the tongue, the posterior part of the tongue
and the epiglottis and soft palate send afferent fibers, respectively, in branches of VIIth,
IXth , and Xth nerves to the rostral NTS. From there taste information ascends to the
pontine taste area (BC), hypothalamic nuclei controlling energy balance (LH and PVN),
limbic forebrain (CNA, BNST, and SI) and cortical taste area (insular cortex). AC=
anterior commissure, BC=brachium conjunctivum, BNST= bed nucleus of the stria
terminalis, CNA= central nucleus of the amygdala, CT= chorda tympani, branch of VII
nerve, DVN=dorsal vagal nucleus, GG=geniculate ganglion, GP=greater petrosal nerve,
branch of VII nerve, LH= lateral hypothalamus, NA= nucleus accumbens, NG=nodose
ganglion, NTS= nucleus of the solitary tract, PG=petrosal ganglion, PVN=
38
39
paraventricular nucleus of the
hypothalamus, SI= substantia innominata.
Figure 25. Projections of the afferent PS neurons
The PS chemoreceptor and mechanoreceptor afferents project to discrete areas of
the NTS as well as to a common integrative commissural area of this nucleus. The
ascending connections of the NTS are with nuclei in medullary reticular formation
(raphe, RVLM, and VMM nuclei); pons (BC, A5); mesencephalic central gray (see
39
40
Figure 19 C); hypothalamus (PVN, DM,
and LH); limbic forebrain (CNA and
BNST); and insular and prefrontal cerebral cortex. The PS preganglionic neurons in
the DVN and NA receive projections from the cerebral cortex, hypothalamus, midbrain
central gray, pontine nuclei and medullary reticular formation. AP= area postrema,
APR=anterior periventricular region, BNST=bed nucleus of stria terminalis, CNA=central
nucleus of amygdala, DM=dorsomedial hypothalamic nucleus, DVN=dorsal vagal
nucleus, IML=intermediolateral cell column, LC= locus coeruleus, LH=lateral
hypothalamic area, MCG=mesencephalic central gray, MPON=medial preoptic nucleus,
NA=nucleus accumbens, NTS=nucleus of the solitary tract, PB=parabrachial nucleus,
PVN=paraventricular hypothalamic nucleus, RVLM=rostral ventrolateral medulla,
VMM=ventromedial medulla. Planes represent, respectively, A= forebrain septum, B=
hypothalamus (diencephalon), C=pons, D=rostral medulla, E=caudal medulla,
F=thoracic spinal cord.
___________________________________________________________________
The mechano- and chemoreceptors involved in the regulation of
cardiorespiratory function, the gastrointestinal receptors, receptors in CVOs associated
with fluid regulation, and taste receptors, all have projections to the NTS and its
immediate vicinity. From the NTS, ascending nerve fibers make connections with the
pontine and forebrain areas (Figure 25.) The cardiorespiratory afferents terminate in
adjacent parts of the NTS as well as in a common commissural part of this nucleus.
Afferents from the gastrointestinal organs converge in the same area. The area
postrema (AP), one of the CVO that receives information from the hormone, sodium,
osmo- and glucoreceptors in plasma and in cerebrospinal fluid, relays this information,
as does the commissural NTS to the ascending central autonomic network (Loewy,
1990). The main parts of the integrative central autonomic network are, rostral
ventrolateral (RVLM) nucleus in the medullary reticular formation; lateral parabrachial
nucleus (PB) and noradrenergic A5 cell group in the pons; mesencephalic central gray
(see Figure 18 C); paraventricular (PVN), dorsomedial (DM) nuclei and lateral area (LH)
of the hypothalamus; central nucleus of the amygdala (CNA) and bed nucleus of stria
terminalis (BNST) in the limbic forebrain; and prefrontal cerebral cortex.
The PVN, LH, ventromedial hypothalamic nucleus (VMH), CNA and BNST are
considered to be part of a central integrative autonomic circuit. The CNA connects with
the medial prefrontal cortex that was shown to inhibit cardiorespiratory function
(Cechetto & Saper, 1990). The descending projections from the central integrative
autonomic circuit include mesencephalic central gray matter, locus coeruleus (LC), PB,
NTS, dorsal vagal nucleus (DVN), nucleus ambiguus (NA), and IML (Luiten et al, 1985).
The preganglionic cells of the efferent vagus nerve to the gastrointestinal organs and
muscles of the upper alimentary canal and trachea are in DVN, while vagal cells
supplying the heart and the respiratory muscles originate in the NA (Figure 25).
40
41
The enteric nervous system (ENS) and
gastrointestinal hormones.
The ENS is a diffuse network of sensory, internuncial, and motor nerve cells that
that are located in several layers within the walls of the gut and associated hollow
organs (Furness & Costa,1980). Although the heart and blood vessels are excluded
from this definition, they also have neural plexuses with features similar to the ENS. The
gastrointestinal hormones (Desbuquois, 1990) and their receptors represent the second
chemical messenger system in the GI organs that parallels and communicates with
another similar system in the brain (Pearse, 1969).
Figure 26. Enteric autonomic nerve plexuses
Enteric plexuses in the intestinal wall, moving from the mucosal to the serosal end are
the periglandular, the submucous or Meissner's, the circular intramuscular, the
myenteric or Auerbach;'s, the longitudinal intramuscular, and the subserous plexuses.
____________________________________________________________________
The gastrointestinal organs are supplied with receptors that monitor mechanical
and chemical changes associated with ingestion and digestion of food. After the initial
chemical stimulation of taste receptors, gastric distension is sensed by the stretch
41
42
receptors in the stomach wall ( Berthoud & Powley, 1992), and glucoreceptors
(Nagase et al., 1993), amino acid receptors (Niijima & Meguid, 1995), osmoreceptors
(Niijima, 1969) and sodium receptors (Contreras & Kosten, 1981) have been described
in the liver (Lautt, 1980). The duodenum also has gluco- and sodium receptors (Walls et
al., 1995), and receptors for several hormones appear to be located on the on vagal
terminals or cell bodies of vagal efferents, among them cholecystokinin (CCK, Ritter et
al., 1989), angiotensin II (Speth et al., 1987 ) , galanin (Calingasan & Ritter, 1992b) and
others.
The enteric plexuses in the intestinal wall, moving from the mucosal to the
serosal end are the periglandular, the submucous or Meissner's, the circular
intramuscular, the myenteric or Auerbach;'s, the longitudinal intramuscular, and the
subserous plexuses (Figure 26). In the heart, there are cardiac and coronary plexuses.
The intrinsic neurons in the autonomic plexuses use several peptidergic messengers
(Pearse 1969, Costa et al. 1986). Most common in the submucous and myenteric
plexuses are neurons using VIP and enkephalin as messengers, and CCK is the least
common. Other neuropeptides in the ENS are somatostatin or somatotropin-releaseinhibiting factor (SRIF), dynorphin, NPY, substance-P and serotonin, and frequently
more than one peptide is colocalized in the same neuron. There is differential chemical
coding of neurons located in different GI plexuses (Costa et al. 1986).
As is the case with other targets of ANS, ENS receives dual afferent and efferent
innervation from SNS and PNS. The S afferents and efferents reach the GI organs
through several sympathetic splanchnic nerves (Figure 23). The NE fibers inhibit GI
motility and ganglia embedded in the plexuses and increase contraction of sphincters.
The SNS fibers colocalizing with NPY vasoconstrict splanchnic circulation, and the
fibers containing NE and somatostatin inhibit GI secretion (Costa et al. 1986). The PS
afferents and efferents innervate the foregut and midgut through the vagus, and the
hindgut and reproductive organs through the pelvic splanchnic nerves. The PS ganglia
and postganglionic cells are embedded within the ENT plexuses (Willems et al. 1985).
The cholinergic fibers stimulate myenteric (Holst et al. 1997) and submucous ganglia
(Berthoud et al., 1991), gastric motility, and GI secretory activity.
The mucosa of the stomach and intestine contains endocrine cells that produce a
number of different hormones (Desbuquois, 1990). Serotonin and somatostatinsecreting cells are found throughout the entire extent of GI tract. The cells producing
secretin, cholecystokinin (CCK), gastrin colocalized with CCK, beta-endorphin,
neurotensin, and gastric inhibitory peptide (GIP) are mostly found in duodenum and
jejunum, and glucagon-secreting cells are more prevalent in jejunum, ileum, and colon.
Most of the GI cells producing hormones communicate by endocrine route, and secretin
was the very first hormone discovered by Bayliss and Starling in 1902. Some GI
hormones are distributed by endocrine as well as paracrine route (SRIF), and a few of
them are also released into the GI lumen (gastrin, SRIF, secretin).
42
43
The function of GI hormones is to
control digestion of food and GI
growth. The digestion is achieved through the control of gut motility, splanchnic
circulation, modulation of the pH of the chyme (mixture of food and gastric secretions),
and secretion of enzymes and hormones. The hormones that increase GI motility are
motilin, SP, CCK, and enkephalins, while secretin, glucagon, VIP, GIP, NPY, and
neurotensin inhibit it. Almost all of the GI hormones stimulate GI blood flow, particularly
SP and neurotensin, except NPY which is a potent vasoconstrictor.
Figure 27. GI endocrine reflexes in control of digestion
Serial elicitation of GI hormone release by the passage of food through the GI tract.
Food elicits gastrin release, and fat and protein the release of CCK. Both hormones
stimulate gastric motility and CCK causes contraction of gall bladder and release of bile
acids necessary for the emulsification of fats. Gastrin action is to release hydrochloric
acid as the preliminary step in digestion of proteins. The acidity of chyme is the stimulus
for secretin release from duodenum, and its action is to trigger secretion of bicarbonate
and digestive enzymes from the pancreas. Many GI hormones facilitate the release of
insulin with the exception of SRIF which inhibits it. The GI hormones released early in
the digestive process stimulate release of other GI hormones. Those released late in
the digestive process inhibit the secretion of GI hormones.
__________________________________________________________________
Food digestion is facilitated by a series of GI endocrine reflexes (Figure 27). The
43
44
ingested food constitutents are the
principal stimulus for the release of
gastrin, CCK, motilin, GIP, SRIF, and neurotensin, and in the case of CCK, fats and
amino acids. These hormones are released serially according to their regional
distribution throughout the GI tract. The initial release of gastrin results in secretion of
hydrochloric acid which lowers the pH of the chyme to 2 and aids in the initial digestion
of proteins. Increased acidity of chyme is the stimulus for the subsequent release of
secretin, the effect of which is secretion of bicarbonate (and of digestive enzymes) from
the pancreas and the restoration of neutral pH of the chyme. The dietary fats trigger the
release of CCK, and the main CCK action is to release bile acids from the gall bladder
and assist in emulsification and digestion of fats. The food also triggers secretion of
SRIF throughout the GI tract and of enteroglucagon from the colon. These two
hormones as well as serotonin, inhibit secretion of gastrin and of gastric acid secretion.
SRIF also inhibits secretion of all other GI and pancreatic hormones. The presence of
SRIF is necessary for the GIF, VIP, and GIP to inhibit gastrin release. All GI hormones
stimulate secretion of pancreatic insulin, pancreatic polypeptide (PPP), glucagon, and
SRI, known also as the incretin effect. Thus GI hormones that are released early in the
digestive process facilitate the release of GI and pancreatic hormones released
subsequently, and the action of hormones released later in digestive process is to
terminate the early steps of this endocrine cascade (Figure 27).
Autonomic reflexes.
The simplest form of autonomic action is a reflex. A number of reflexes controlled
by the ANS operate autonomously or as part of complex neuroendocrine and behavioral
responses to disturbance in the internal environment. Some of the more common
cardiorespiratory and endocrine reflexes are listed below .
Atrial mechanoreceptor reflex is a response to change in plasma volume
detected by the low-pressure baroreceptors at the junction of venae cavae with the
atria. The Increases in venous return produce bradycardia and reduced vasomotor tone,
particularly to the kidney, and diuresis. The latter is in part a result of increased
glomerular filtration rate and in part a response to the reflex release of atrial natriuretic
peptide (ANP).
Baroreflex normalizes systemic blood pressure when it has deviated outside the
normal range (Spyer, 1990). The discharge rate of the carotid and sinus nerve afferent
fibers innervating arterial high-pressure baroreceptors is directly proportional to arterial
blood pressure and triggers reflex reduction in peripheral vasoconstriction, particularly in
the muscle and less so in the skin, and in heart rate (bradycardia) and heart contractility
(Figure 28). The reflex arc entails a baroreceptor afferent projection to NTS and an
efferent vagal output from NA. At the same time baroreceptors exert an inhibitory
influence over the S cardioaccelerator nerves by way of internuncial neurons in the
medial prefrontal cortex and CNA that suppress the rhythmic cardiac and vasomotor
drive from the medullary reticular formation (RVLM and raphe nuclei).
44
45
Figure 28. The baroreflex
The discharge rate of carotid sinus and aortic arch baroreceptors is proportional to
arterial blood pressure, while in the S cardiac nerves it is inversely proportional. The cell
bodies of the afferent neurons innervating the two baroreceptors are, respectively, in
petrosal and nodose ganglia and their dendrites project to NTS in sinus and aortic
nerves. The inhibition of the heart rate and contractility, and reduction in
vasoconstriction of blood vessels, is carried out by vagus with preganglionic neurons in
NA. Baroreceptors also activate internuncial neurons that inhibit the RVLM nucleus, the
origin of cardiovascular S drive.
NA= nucleus accumbens , NG=nodose ganglion of the X nerve , NTS=nucleus of the
tractus solitarius, PG=petrosal ganglion of the IX nerve, RVLM=rostral ventrolateral
45
46
medulla, S=sympathetic
Chemoreceptor reflex is a response to reduced arterial oxygen partial pressure
(pO2) detected by aortic sinus and carotid body chemoreceptors and to increased
carbon dioxide partial pressure (pCO2 ) monitored by cells on the ventral surface of the
medulla. It corrects these deviations through increases in minute ventilation (VE) and
cardiac output (Q), and to a lesser extent through changes in vasoconstriction. The
internuncial integrative circuits involve (Richter & Spyer, 1990) cardiovascular and
respiratory nuclei in the medulla (Figure 25, planes D and E) that act in coordinated and
cooperative fashion, and the inhibitory vagal influence from the NA . Neurons in
Botzinger complex that are responsible for initiation and timing of respiratory rhythmsare
adjacent and rostral to the RVLM nucleus that initiates and times cardiovascular
function so that functional interactions, and subordination of cardiovascular function to
respiratory control, as is the case in diving reflex, has an anatomical basis. The
patterning of cardiovascular and respiratory responses during exercise is also linked
and apparently controlled by posterior hypothalamus or dorsomedial hypothalamus
(Eldridge et al., 1985, Saper et al., 1976, Wardrop et al., 1988).
Diving reflex entails vagal suppression of the Q and of respiratory drive and
bronchoconstriction, mediated by the vagus nerve (Kawakami et al. 1967, Kobayashi &
Ogawa, 1973). The PS afferent discharge in the facial (VII) nerve to cooling of the face
initates the reflex that subordinates the chemoreceptor signals of reduced pO2 and
increased pCO2 to respiratory breath-holding. Reflex is well expressed in diving
mammals and less so in humans.
Metaboreflex entails vasoconstriction in response to build-up of metabolic
products in the muscle during ischemia that is associated with isometric muscle
contractions. It was described in the preceeding section.
Orthostatic or postural reflex entails redistribution of blood to the head and upper
regions of the body after a change in body position from recumbent to upright. It utilizes
afferent input from baro- atrial mechano- and chemoreceptors. Postural hypotension is
the condition where the orthostatic reflex operates sluggishly causing transient cerebral
ischemia and dizziness.
Sudomotor reflex also is a component of thermoregulatory response. It involves
reflex activation of eccrine sweat glands by the cholinergic sympathetic neurons.
Temperature change is detected by somatic temperature-sensitive neurons in the skin
or in the central nervous system. A greater change in internal or external temperature is
required to elicit this reflex than the vasomotor reflex (Stolwijk & Hardy, 1977).
Vasomotor reflex is a component of thermoregulatory response. It involves reflex
changes in the degree of vascular constriction in response to changes in blood or
ambient temperature and in selective constriction of peripheral or deep limb veins in
response to cold or hot stimulus, respectively. Changes in vascular tone are achieved
46
47
through variation in the degree of
vasoconstrictive S action. Temperature
change is detected by somatic temperature-sensitive neurons in the skin or in the
central nervous system. Selective activation of S motoneurons to skin blood vessels
and not to muscle vascular beds is controlled by the A5 noradrenergic cell group
(Stanek et al., 1984, Figure 25, plane C) and by the RVLM nucleus (Dampney &
McAllen, 1988, Figure 25, plane D) in response to thermoregulatory challenge.
The central control of thermoregulatory reflexes involves integration of afferent
input from central and peripheral thermoreceptors. Hypothalamic nuclei that also control
body fluid balance and hypothalamic areas responsible for S activation and heat
production are involved in the interaction, but the anatomical and functional details are
poorly understood (Strand et al 1986).
Autonomic control of endocrine reflexes.
There are numerous and complex reciprocal interactions between the ANS and
the endocrine systems. Only a few of these interactions will be mentioned here to show
their relationship to the ANS function. Additional details and more extensive discussion
of these reflexes can be found in the chapters dealing with receptor mechanisms (3),
exercise as an emergency (4), regulation of fuel use during exercise (5), and
temperature and fluid balance during exercise (8).
Adrenomedullary catecholamine release. The adrenomedullary catecholamine
release is triggered by the action potentials in preganglionic neurons originating in the
last three thoracic and first lumbar spinal segments (Figures 21, 23) that reach the
adrenal medulla through the lesser and lowest splanchnic sympathetic nerves. They
communicate through transmission of ACH and act on nicotinic receptors. Some
preganglionic neurons form synapses in the celiac ganglion and send postganglionic
fibers to blood vessels supplying the adrenal gland. They release NE and act on alpha
adrenergic receptors. Adrenal medulla also receives PS innervation through the two
celiac branches of the vagus nerve (Berthoud & Powley, 1993). The central control of
adrenomedullary hormone release (Edwards, 1990) is mediated by hypothalamic (PVN,
Figure 19, plane A) and medullary nuclei (caudal raphe, RVLM, VMM, and A5, Figure
19, planes B and C). This reflex is elicited by glucoprivation with concurrent supression
of the S activity (Egawa et al. 1989, Ritter et al. 1995) , a response that is mediated by
the PVN (Katafuchi et al. 1988). This reflex is elicited during exercise together with
activation of the SNS (Young & Landsberg, 1983).
The adrenomedullary catecholamines have cardiorespiratory and metabolic
actions. Both E and NE can activate either of two principal types of adrenergic
receptors, alpha and beta, but NE has higher affinity for alpha receptors while E has
higher affinity for beta receptors (Parkinson, 1990). Receptor distribution varies by
tissue types, which together with differential receptor affinities for the two hormones
allows for diverse biological effects. The two principal receptor types can be subdivided
47
48
into several variants. Table 6 lists the
principal adrenergic receptor types, their
biological effects, and some commonly used receptor agonists and antagonists..
Figure 29. Renin-angiotensin-aldosterone reflex
When blood pressure declines, renal S nerve triggers and potentiates renal release of
renin to hypovolemic stimulus. Renin converts circulating angiotensinogen into
angiotensin I. The endothelial converting enzyme transforms the angiotensin I into
angiotensin II. The angiotensin helps expand plasma volume through three actions. It
48
49
stimulates release of aldosterone from the adrenal cortex with the consequent
increased renal sodium reabsorbtion. It binds to the SFO, one of the circumventricular
organs and stimulates the magnocellular hypothalamic nuclei (SO,PVN) to release
ADH. Finally it enhances neurotransmission in the S celiac ganglion which causes renal
vasoconstriction and reduced glomerular filtration rate.
___________________________________________________________________
The adrenomedullary and adrenocortical hormones have reciprocal interactions.
While cortisol permits E synthesis, E stimulates pituitary ACTH release which in turn
triggers cortisol release (Figure 21). This positive feed-back loop may operate under
stressful conditions, including extreme exercise, when actions of both hormones are
complementary and beneficial.
Antidiuretic endocrine reflex of the posterior pituitarywas described in the context of
magnocellular PVN functions
Reflex release of plasma renin to hypovolemia. The loss of sodium from the
extracellular compartment with the consequent reduction in plasma volume is sensed by
the baroreceptors in the JGA, the specialized contact area between the ascending limb
of the kidney tubule (macula densa) and the afferent arteriole to the glomerulus. The
renal S nerve activity triggers renin secretion and potentiates its release to hypovolemic
stimuli (Kopp & DiBona, 1993, Saxena et al., 1992). The granular cells of the afferent
arteriole secrete renin, the principal action of which is to catalyze conversion of plasma
angiotensinogen into angiotensin I (Figure 29). The converting enzyme in the vascular
endothelia converts angiotensin I to the biologically active angiotensin II. Angiotensin II
stimulates secretion of aldosterone from the external glomerular zone of the adrenal
cortex and thereby increases reabsorbtion of sodium from tubular lumen into plasma. It
also potentiates the neurotransmission in the celiac ganglion causing renal
vasoconstriction and reduced glomerular filtration rate. The angiotensin II binds to the
SFO and stimulates PVN and SO nuclei to release ADH. By increasing sodium and
water reabsorbtion and reducing glomerular filtration, this reflex leads to expansion of
plasma volume. Finally, this messenger elicits both thirst and sodium hunger by acting
on the CVO angiotensin II receptors.
Autonomic control of pancreatic hormone release. The endocrine pancreas is
innervated by the preganglionic vagal fibers originating in DVN, preganglionic S fibers
from fifth through ninth thoracic segments and postganglionic S fibers originating in the
celiac ganglion. During exercise or other circumstances that elicit increased S outflow,
NE from S nerve terminals inhibits insulin secretion by acting on alpha2 receptors on
beta cells of pancreatic islets and stimulates glucagon and SRIF release by acting on
alpha1 and beta receptors located on alpha and delta cells, respectively (Edwards,
1990). The stimulation of beta adrenergic receptors has a stimulatory effect on insulin
release. The integrative centers needed for the reflex increases in hepatic
49
50
glycogenolysis and in E and glucagon
release during glucoprivation are NTS,
lateral PB, LC, AP, PVN, and DVN ( Ritter & Dinh, 1994) with the NTS and AP playing
the more critical role (Calingasan & Ritter, 1992 a). The PVN also is the site of receptors
where NE, NPY and cortisol increase (Tempel & Leibowitz, 1993), and serotonin
(Leibowitz et al. 1993) and CRF decrease carbohydrate intake (Bray 1993) after
glycogen depletion. Reduced oxidative utilization of lipids is monitored by different set of
peripheral receptors, peptide mediators (Akabayashi et al. 1994) and brain nuclei
governing selection of dietary fat (Ritter & Dinh, 1994).
During ingestion of food, cephalic-phase insulin secretion occurs before the
arrival of absorbed food into the blood. It is triggered by hepatic and intestinal
glucoreceptors and the respective branches of vagus (Berthoud & Powley, 1990). Upon
absorbtion, increased plasma concentrations of nutrients directly stimulate insulin,
glucagon, and pancreatic polypeptide secretion and inhibit SRIF release .In addition,
intestinal and hepatic glucoreceptors elicit reflex vagal stimulation of insulin and
glucagon secretion by acting on cholinergic muscarinic receptors while the activity of
hepatic splanchnic nerve is decreased . Concurrently the hepatic branch of the vagus is
also activated and stimulates glycogen synthesis (Niijima, 1989).
The role of autonomic nervous system in exercise.
From the preceding discussion of the functional properties of the ANS it is now
possible to highlight its several important roles in exercise. In evaluating the evidence
for the role of ANS in exercise it is useful to be reminded of limitations of different
methods used to assess ANS activity. Direct measurements of catecholamines in
circulation do not identify the relative contributions of the SNS and the adrenal medulla,
as the medulla secretes both catecholamines, and at high exercise intensities, NE
(Leuenberger et al., 1993) and NPY (Kaijser et al., 1994) spill over from the nerve
endings into plasma. Without additional information about NE appearance and
clearance rates, circulating concentrations give limited information.
Measurements of arteriovenous NE differences circumvent this limitation. Daily
urinary catecholamine output is another valid way to quantify sympathoadrenal activity
but is of limited use in studies examining S control in exercise. Pharmacological
blockade and stimulation can yield useful information when direct effects of such
manipulations on physical performance are assessed and controlled. An indirect
method of estimating PS and S activity in exercise is spectral analysis of heart rate
variability (Yamamoto & Hughson, 1991). It entails separating total spectral power (Pt)
of HR variability into harmonic and nonharmonic components, and harmonic component
into high (Ph) and low frequencies. (Pl). The ratios of Ph/Pt and Pl/Pt then represent
respective measures of PS and S effects on the heart, and by implication on the rest of
the body. Direct measurements of S nerve activity have also been done on the limbs
(Saito, 1995).
50
51
The three most important roles of
the ANS in exercise are, its
coordination of several different physiological functions during exercise, its capacity to
increase physiological responses in anticipation of actual needs, and its capacity to
maintain constancy of the internal environment by compensating for the perturbations
caused by exercise. The integrative role of catecholamines is inherent in their ability to
directly affect a number of different processes. The SNS and the adrenal medullary
hormones control the chronotropic (HR) and inotropic (heart contractility) functions of
the heart, contraction of vascular beds and as a consequence, blood pressure and
redistribution of blood from the splanchnic beds to muscle during exercise. The SNS
and the adrenal medullary hormones also control mobilization and utilization of
metabolic fuels, and reflecting the evolutionary function of physical activity in fight or
flight situations, controls over defense reactions such as aggregation of platelets (
Larsson et al., 1994) that is important in blood clotting, and activation of cells mediating
immune responses. The ANS contributes also to general arousal, increased pupillary
diameter, piloerection, and release of endogenous opiates that have analgesic
functions. Finally, the sympathoadrenal system engages other endocrine systems in
support of its cardiorespiratory, circulatory and metabolic functions in exercise, and
these will be explored in greater detail in later chapters.
The anticipatory function of the ANS is seen in increased cardiorespiratory
function prior to the onset of physical activity (Mason et al., 1973) and in the dosedependent release of catecholamines in proportion to the intensity or stressfulness of
exercise. While both the S nerve activity and adrenal catecholamines increase with
exercise intensity (Figure 30) , E requires greater stimulus intensities for its release than
is the case for S activation. The PS tone declines at low exercise intensities (Nakamura
et al. 1993) and increases during the recoveryphase when it can lead to post-exercise
fall in blood pressure (Halliwill et al.,1996) or increase in anabolic and biosynthetic
functions. The systematic relationship with exercise intensity is also seen in a number of
hormones that are released during exercise and are influenced by S nerve activity such
as dose-dependent decreases in plasma insulin and increases in secretion of glucagon
(Saltin & Gollnick, 1988 ), cortisol , ACTH , aldosterone (Luger et al., 1988 ), AVP
among others.
The third important role of the ANS in exercise is its regulation of the internal
environment during exercise and recovery from exercise. During exercise, homeostatic
control mechanisms often undergo readjustment to meet increased functional demands
of exercise. For instance baroreflex is reset to a higher pressure level to operate at
increased blood pressure ranges encountered during exercise ( Rowell & O'Leary,
1990). As exercise creates disturbances in the internal environment, the ANS generates
corrective reflexes or more complex responses. The priorities for maintenance of
different aspects of the internal environment shift during exercise. Increased heat
generated by muscle activity leads to excessive heat gain which is counteracted by
vasomotor and sudomotor reflexes and appropriate thermoregulatory behaviors. As a
51
52
consequence of increased sweating, an
imbalance develops in body fluid volume.
Conservation of plasma volume through AVP or renin-angiotensin-aldosterone reflexes
now assumes higher priority than the regulation of body temperature.
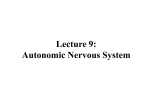
Figure 30. Time course and dose-dependence of the sympathoadrenal
exercise
responses to
A conceptual illustration of changes in the relative activities of S and PS nerves
and in secretion of adrenomedullary E as a function of intensity or duration of exercise
and during recovery from exercise. At the start of exercise, PS tone declines and is
transiently increased during recovery when it participates in restorative biosynthetic
actions. At the start of exercise, S tone increases in proportion to intensity or
stressfulness of exercise. Higher exercise intensities are required to elicit E secretion
which also is secreted in dose-dependent fashion. The decay of S nerve activity is
faster than the disappearance of E from circulation.
______________________________________________________________________
The control by the sympathoadrenal system of fuel mobilization and use during
exercise changes as a function of exercise intensity and duration (Young & Landsberg,
1983). These changes reflects variable contributions of alpha and beta receptor
stimulation as the relative activities of S nerves and adrenal E change under different
conditions of exercise. During the early stage of exercise or at low exercise intensities,
increased S nerve activity and NE release from the nerve terminals (Figure 30) results
52
53
in predominant stimulation of alpha
adrenergic receptors in the liver and the
adipose tissue (Table 6). These conditions facilitate hepatic glucose production via the
gluconeogenic Cori cycle, increased muscle glucose uptake and glycolysis and low
level of lipid utilization due to inhibitory alpha adrenergic effects on lipolysis and lack of
transport of FFAs from vasoconstricted splanchnic vasculature.
As the intensity or duration of exercise increase (middle part of Figure 30), fuel
metabolism is controlled by both increased S nerve activity and adrenal E secretion.
Catecholamines now stimulate glycogenolysis in the liver and in the muscle. In addition
to glycolysis, beta receptor activation stimulates carbohydrate oxidation. The alpha
adrenergic ation on the Cori gluconeogenic cycle is at its peak, so that this phase of
metabolism is characterized by carbohydrate dependence. At this stage, increased beta
adrenergic stimulation accelerates lipolysis in the adipose tissue and removes the
peripheral circulatory restraints over FFA release. This permits greater access of
albumin-bound FFAs to plasma and exercising muscle.
Table 6
Principal types of adrenergic receptors
ALPHA 1
ALPHA 2
BETA 1
BETA 2
vasoconstriction
vasoconstriction
∧ heart rate
broncholdilatation
vasodilatation
∧ heart contractility
∨ NE release
∧ heart
contactibility
glycogenolysis
(L,M)
gluconeogenesis
∨ lipolysis
∧ lipolysis
glycolysis
glycogenolysis (L)
∧ platelet
aggregation
renin release
oxidative
metabolism
∧ nutrient uptake
∨ insulin release
∧ insulin release
glycolysis
amylase secretion
sweating
piloerection
AGONISTS
53
54
salivation
salbutamol
AGONISTS
AGONISTS
AGONISTS#
rimiterol
methoxamine
clonidine*
prenaterol
albuterol
phenylephrine
alpha-methyl-NE
tolbutamine
terbutaline
tramazoline
tazolol
hexoprenaline
xylazine
dobutamine
soterenol
zinterol
clenbuterol
ANTAGONISTS
ANTAGONISTS
ANTAGONISTS
salmotamol
prazosin
yohimbine
ICI 89, 407
procaterol
BE 2254
idazoxan
paraoxyprenolol
epinephrine
corynanthine
rauwolscine
betaxolol
phetolamine
phentolamine
atenolol
ANTAGONISTS
practolol
ICI 118,551
metoprolol
IPS 338
propranolol
butoxamine
propranolol
#Beta 3 receptor has high affinity for the lipolytic action of NE (Yamashita et al., 1993)
When exercise intensity is not above the anaerobic threshold, the next stage of
exercise favors oxidative utilization of lipids. The shift from carbohydrate to lipid
oxidation in the muscle is facilitated by the glucose-fatty acid cycle (Newsholme, 1977) ,
low insulin concentration, and by reduced muscle sensitivity to alpha adrenergic
stimulation as a consequence on increased FFA delivery to the muscle (Burns et al.
54
55
1978). The pattern of sympathoadrenal
theses conditions of exercise.
activation favors lipid utilization under
During recovery from short-term exercise, there is a rapid rise in plasma insulin
(Wahren et al. 1973), probably reflecting a decline in S activity and an increase in PS
tone. This contributes to the fall in hepatic glucose output and increased glucose uptake
by the muscle. During recovery from long -term exercise that has resulted in glycogen
depletion and in a fall in plasma glucose, plasma insulin remains low and
adrenomedullary release of E and secretion of glucagon are sustained. Thus the S
adrenomedullary and pancreatic reflexes here compensate for the deficiencies in
regulation of plasma glucose and permit a more extended hepatic glucose production
by gluconeogenesis (Bjorkman & Wahren, 1988).
Habitual physical activity produces adaptations in sympathoadrenal function.
There is a decrease in plasma NE responses and adrenal E release (Hartley et al. 1972
) and increased PS tone (Goldsmith et al., 1993) at equivalent exercise loads
suggesting an active supression of S tone and facilitation of PS tone. The ANS thus
controls acute functional adjustments to oxygen and energy needs during acute
exercise bouts and participates in physiological adaptations to sustained high levels of
physical activity.
References
Akabayashi, A., Koenig, J.I., Watanabe, Y., Alexander, J.T. & Leibowitz, S.F. (1994).
Galanin-containing neurons in the paraventricular \tab nucleus: a neurochemical marker
for fat ingestion and body weight gain. Proceedings of the National Academy of
Sciences of the \tab United States of America, 91, 10375-10379.
Altura, B.M. & Altura, B.T. (1984). Actions of vasopressin, oxytocin, and synthetic
analogs on vascular smooth muscle. Federation Proceedings, 43 , 80-86.
Bayliss, W.M. & Starling, E.H. (1902). The mechanism of pancreatic secretion. Journal
of Physiology, 28 , 3125-353.
Berthoud, H.R. & Powley,T.L. (1990). Identification of vagal preganglionics that mediate
cephalic phase insulin response. American Journal of Physiology , 258 , R523-R530.
Berthoud, H.R. & Powley,T.L. (1992). Vagal afferent innervation of the rat fundic
stomach: morphological characterization of the gastric tension receptor. Journal of
Comparative Neurology, 319 , 261-276.
Berthoud, H.R. & Powley,T.L. (1993). Characterization of vagal innervation of the rat
celiac, suprarenal and mesenteric ganglia. Journal of the Autonomic Nervous System,
42 , 153-169.
Berthoud, H.R., Fox, E.A. & Powley, T.L. (1991). Abdominal pathways and central origin
55
56
of rat vagal fibers that stimulate gastric
acid. Gastroenterology 100 , 627-637.
Berkenbosch, F., van Oers, J., del Ray, A., Tilders, F. & Besedovsky, H. (1987).
Corticotropin-releasing factor-producing neurons in the rat activated by interleukin-1.
Science 238, 524-526.
Bjorkman,O. & Wahren, J. (1988). Glucose homeostasis during and after exercise. In
E.S. Horton & R.L.Terjung (Eds). Exercise, nutrition, and energy metabolism. (pp 100115), New York: Macmillan.
Bray, G.A. (1993). The nutrient balance hypothesis: peptides, sympathetic activity, and
food intake. Annals of the New York Academy of Sciences, 676 , 223-241.
Brown, M.R. & Fisher, L.A. (1985). Corticotropin releasing factor: Effects on autonomic
nervous system and visceral systems. Federation Proceedings 44 , 243-248.
Burns, T.W., Langley, P.E., Terry, B.E. & Robinson, G.A. (1978). The role of free fatty
acids in the regulation of lipolysis by human \tab adipose tissue cells. Metabolism, 27 ,
1755-1762.
Burnstock, G. & Kennedy, C. (1986). A dual function for adenosine-5'- triphosphate in
the regulation of vascular tone. Excitatory co- transmitter with noradrenaline from
perivascular nerves and locally released inhibitory intravscularagent. Circulation
research, 58 , 319-330.
Calingasan, N.Y. & Ritter, S. (1992a). Hypothalamic paraventricular nucleus lesions do
not abolish glucoprivic or lipoprivic feeding. Brain Research, 595 , 25-31.
Calingasan, N.Y. & Ritter, S. (1992b). Presence of galanin in rat vagal sensory neurons:
evidence from immunohistochemistry and in situ hybridization. Journal of the Autonomic
Nervous System, 40, 229-238.
Cannon, W.B.(1929). Bodily changes in pain, hunger, fear and rage. An account of
recent researches into the function of emotional excitement. 2nd ed. New York:
Appleton.
Cechetto, D.F. & Saper, C.B. (1990). Role of the central cerebral cortex in autonomic
function. In A. D. Loewy & K.M. Spyer (Eds.), } Central regulation of autonomic
functions (pp.168-188). New York:Oxford University Press.
Cervero, F. & Foreman, R.D. (1990). Sensory innervation of the viscera. In A. D. Loewy
& K.M. Spyer (Eds.), Central regulation of autonomic functions (pp.104-125). New York:
Oxford University Press.
Contreras, R.J. & Kosten, T.(1981). Changes in salt intake after abdominal vagotomy:
Evidence for hepatic sodium receptors. Physiology and Behavior, 26 , 575-582.
56
57
Costa, M., Furness,J.J., & Gibbons, I.L.
Progress in Brain Research, 68 , 217-239.
Chemical coding of enteric neurons. l
Cowley, A.W.,Jr., Merrill, D., Osborn, J. & Barber, B.J. (1984). Influence of vasopression
and angiotensin on baroreflexes in the dog. Circulation Research, 54 , 163-172.
Daly, M. de B. (1985). Interactions bewteen respiration and circulation (pp.). In :
Handbook of Physiology, The Respiratory System II. Bethesda: American Physiological
Society.
Dampney, R.A.L & McAllen, R.M. (1988). Differential control of \tab sympathetic fibers
supplying hind limb, skin, and muscle by subretrofacial neurones in the cat. Journal of
Physiology (London), 395 , 41-56.
Desbuquois, B. (1990). Gastrointestinal hormones. In E.-E. Baulieu & P.A. Kelly (Eds.),
Hormones: From molecules to disease. (pp.539-589). New York: Chapman & Hall.
Edwards, A.V. (1990). Autonomic control of endocrine pancreatic and adrenal function.
In A. D. Loewy & K.M. Spyer (Eds.), Central regulation of autonomic functions (pp.287309). New York: Oxford University Press.
Egawa, M., Yoshimitsu,H. & Bray, G.A. (1989). Lateral hypothalamic injection of 2deoxy-D-glucose supresses sympathetic activity. American Journal of Physiology, 257 ,
R1386-1392.
Eldridge, F.L., Millhorn, D.E. Kiley, J.P. & Waldrop, T.G. (1985). Stimulation by central
command of locomotion, respiration, and circulation during exercise. Respiratory
Physiology 59, 313-337.
Fisher, L.A., Rivier, J., Rivier, C., Spiess, J., Vale, W. & Brown, M.V. (1982).
Corticotropin releasing factor (CRF): Central effects on mean arterial pressure and heart
rate in rats. Endocrinology 110, 2222-2224.
Furness, J.B.& Costa, M. (1980). Types of nerves in the enteric nervous system.
Neuroscience, 5 ,1-20.
Gebber, G.L. (1990). Central determinants of sympathetic nerve discharge. In A. D.
Loewy & K.M. Spyer (Eds.), Central egulation of autonomic functions (pp.126-144). New
York: Oxford University Press.
Goldsmith, R.L., Bigger, J.T.,Jr., Steinman, R.C. & Fleiss,J.L. (1993). Comparison of 24hour parasympathetic activity in endurance- trained young men. Journal of the
American College of Cardiology, 20, 552-558.
Guyenet, P.G. (1990). Role of the ventral medulla oblongata in blood pressure
regulation. In A. D. Loewy & K.M. Spyer (Eds.), Central regulation of autonomic
57
58
functions(pp.145-167). New York: Oxford
University Press.
Halliwill, J.R., Taylor, J.A. & Eckberg, D.L. (1996). Impaired sympatheticb vascular
regulation in humans after acute dynamic exercise. Journal of Physiology, 495 , 279288.
Harris, M.C. & Loewy, A.D. Neural regulation of vasopressin-containing hypothalamic
neurons and the role of vasopressin in cardiovascular function, In A. D. Loewy & K.M.
Spyer (Eds.), Central regulation of autonomic functions (pp.224-246). New York: Oxford
University Press.
Hartley, L.H., Mason, J.W., Hogan, R.P., Jones, L.G., Kotchen, T.A., Mougey, E.H.,
Wherry, F.E., Pennington, L.L. & Ricketts, P.T. (1972). Multiple hormonal responses to
prolonged exercise in relation to physical training. Journal of Applied Physiology 33 ,
607- 610.
Holst, M.C., Kelly, J.B., & Powley, T.L. (1997). Vagal preganglionic projections to the
enteric nervous system characterized with Phaseolus vulgaris-leucoagglutinin. Journal
of Comparative Neurology, 381, 81-100.
Hori, T., Katafuchi, T., Take, S., Shimizu, N. & Niijima, A. (1995). The autonomic
nervous system as a communication channel between the brain and the immune
system. Neuroimmunomodulation, 2 , 203-215.
Johnson, A.K. & Loewy, A.D. (1990). Circumventricular organs and their role in visceral
function. In A. D. Loewy & K.M. Spyer (Eds.), Central regulation of autonomic functions
(pp.247-267). New York: Oxford University Press.
Kaijser, L., Pernow, J., Berglund, B., Grubbstrom, J. & Lundberg, J.M. (1994).
Neuropeptide Y release from human heart is enhanced during prolonged exercise in
hypoxia. Journal of Applied Physiology, 76, 1346- 1349.
Katafuchi, T., Oomura, Y.,& Kurosawa,M. (1988).Effects of chemical stimulation of
paraventricular nucleus on adrenal and renal nerve activity in rats. Neuroscience
Letters, 86 , 195-299.
Kaufman, M.P., Longhurst, J.C., Rybicki,K.J., Wallach,J.H., & Mitchell, J.H. (1983).
Effects of static muscular contraction in impulse activity of groups III and IV afferents in
cats. Journal of Applied Physiology, 55, 105-112.
Kawakami , Y., Natelson, B.H. & Du Bois, A.B. (1967). Cardiovascular effects of face
immersion and factors affecting diving reflex in man. Journal of Applied Physiology, 23,
964-970.
Kniffki, K.-D., Mense, S,L, & Schmidt, R.F. (1981). Muscle receptors with fine afferent
fibers which may evoke circulatory reflexes. Circulation research 48, I-25-31.
58
59
Kobayashi,S. & Ogawa,T. (1973). Effect of water temperature on bradycardia during
nonapneic facial immersion in man. Japanese Journal of Physiology,23, 613-624.
Kopp, U.C. & DiBona, G.F. (1993). Neural regulation of renin secretion. Seminars in
Nephrology, 13 , 543-551.
Landis, S.C. & Fredieu, J.R. (1986). Coexistence of calcitonin gene- related peptide and
vasoactive intestinal polypeptide in cholinergic sympathetic innervation of rat sweat
glands. Brain Research, 377 , 177-181.
Larsson, P.T., Wallen, N.H. & Hjemdahl, P. (1994). Norepinephrine- induced human
platelet activation in vivo is only partly counteracted by aspirin. Circulation 89, 19511957.
Lautt, W.W.(1980). Hepatic nerves: Areview of their functions and effects. Canadian
Physiology and Pharmacology, 58 , 105-123.
Leibowitz, S.F., Alexander, J.T., Cheung, W.K. & Weiss, G.F.(1993). Effects of
serotonin and the serotonin blocker metergoline on meal \tab patterns and
macronutrient selection.Pharmacology, Biochemistry and Behavior, 45 , 185-194.
Leuenberger, U., Sinoway,L., Gubin, S., Gaul, L. Davis, D.& Zelis, R. (1993).Effects of
exercise intensity and duration on norepinephrine spillover and clearance in humans.
Journal of Applied Physiology 75, 668-674.
Loewy, A.D. (1990a). Autonomic control ofthe eye. In A. D. Loewy & \tab K.M. Spyer
(Eds.), Central regulation of autonomic functions (pp.268-285). New York: Oxford
University Press.
Loewy, A.D. (1990b). Central autonomic pathways. In A. D. Loewy & K.M. Spyer (Eds.),
Central regulation of autonomic functions (pp.89-103). New York: Oxford University
Press.
Luger.A., Deuster, P.A., Gold,P.W., Loriaux, D.L. & Chrousos, G.P. (1988). Horonal
responses to the stress of exercise. Advances in Experimental Medicine and Biology,
245 , 273-280.
Luiten, P.G.M., ter Horst, G.J., Karst, H. & Steffens, A.B. (1985). The course of
paraventricular hypothalamic efferents to autonomic structures in medulla and spinal
cord. Brain Research 329, 374-378.
Luiten, P.G.M., ter Horst, G.J. & Steffens, A.B. (1987). The hypothalamus, intrinsic
connections and outflow pathwaus to the endocrine system in relation to the control of
feeding and \tab metabolism. Progress in Neurobiology, 28 , 1-54.
Mackinnon, L.T. (1992). Exercise and immunology. Champaign: Human Kinetics
59
60
Publishers.
Marshall, J.M.& Timms, R.J. (1980). Experiments on the role of the subthalamus in the
generation of the cardiovascular changes during locomotion in the cat. Journal of
Physiology (London) 301 ,92P-93P.
Mason, J.W., Hartley, L.H., Kotchen, T.A., Mougey, E.H., Ricketts, P.T. & Jones, L.G.
Plasma cortisol and norepinephrine responses in anticipation of muscular exercise.
Psychosomatic Medicine 35, 406-414.
Menetrey, D. & Basbaum, A.I. (1987). Spinal and trigeminal projections to the nucleus
of the solitary tract: A possible substrate for \tab somatovisceral and viscerovisceral
reflex activation. Journal of Comparati ve Neurology, 255, 439-450.
Nagase, H., Inoue, S., Tanaka,K., Takamura, Y. & Niijima, A. (1993). Hepatic glucosesensitive unit regulation of glucose-induced \tab insulin secretion in rats. Physiology and
Behavior, 53, 139-143.
Nakamura, Y., Yamamoto, Y & Muraoka, I. (1993). Autonomic control of heart rate
during physical exercise and fractal dimension of heart rate variability. Journal of
Applied Physiology 74 , 875-881.
Newsholme, E.A. (1977). The regulation of intracellular and extracellular fuel supply
during sustained exercises. Annals of the New York Academy of Sciences 301 ,81-91.
Niijima, A.(1969) Afferent discharges from osmoreceptors in the liver of the guinea pig.
Niijima, A.(1989). Neural mechanisms in the control of blood glucose concentration.
Journal of Nutrition, 119 , 833-840.
Niijima, A. & Meguid, M.M. (1995). An electrophysiological study on amino acid sensors
in the hepato-portal system in the rat. Obesity Research, 3 Supplement 5: 741S-745S.
Parkinson, D. (1990). Adrenergic receptors in the autonomic nervous system. In A. D.
Loewy & K.M. Spyer (Eds.), Central regulation of autonomic functions (pp.17-27). New
York: Oxford University Press.
Pearse, A.G.E. (1969) The cytochemistry and ultrastructure of polypeptide hormoneproducing cells of the APUD series and the embryologic, physiologic and pathologic
implications of the concept. J.Histochemistry and Cytochemistry, 17 , 303-313.
Pernow, J. & Lundberg, J.M. (1988). Neuropeptide Y induces potent contraction of
arterial vascular smooth muscle via an endothelium- independent mechanism. Acta
Physiologica Scandinavica, 134 , 157-158.
Peters, S. & Kreulen, D.L. (1985). Vasopressin-mediated slow EPSPs in mammalian
sympathetic ganglion. Brain Research, 339, 126-129.
60
61
Prechtl, J.C. & Powley, T.L. The fiber
composition of the abdominal vagus of the
rat. (1990). Anatomy and Embryology, 181 , 101-115.
Richter, D.W. & Spyer, K.M. (1990). Cardiorespiratory control. In A. D. Loewy & K.M.
Spyer (Eds.), Central regulation of autonomic functions (pp.189-207. New York: Oxford
University Press.
Ritter, S & Dinh, T.T. (1994). 2-Mercaptoacetate and 2-deoxy-D-glucose induce Fos-like
immunoreactivity in rat brain. Brain Research, 641, 111-120.
Ritter, R.C., Ritter, S., Ewart,W.R. & Wingate, D.L. Capsaicin attenuates hindbrain
neuron responses to circulating cholecystokinin. American Journal of Physiology, 257,
R1162-R1168.
Ritter, S., Scheurink, A., & Singer, L.K. (1995). 2-Deoxy-D-glucose but not 2mercaptoacetate increases Fos-like immunoreactivity in adrenal medulla and
sympathetic preganglionic neurons. Obesity Research, 3 Supplement , 729S-734S.
Rowell, L.B. & O'Leary, D.S. (1990). Reflex control of the circulation during exercise:
chemoreflexes and mechanoreflexes. Journal of Applied Physiology, 69 , 407-418.
Ruzicka, B.B. & Akil, H. (1995). Differential cellular regulation of pro- opiomelanocortin
by interleukin-1-beta and corticotropin-releasing hormone. Neuroendocrinology, 61,
136-151.
Saito, M. (1995). Differences in muscle sympathetic nerve response to isometric
exercise in different muscle groups. European Journal of Applied Physiology and
Occupational Physiology 70, 26-35.
Saltin , B.& Gollnick, P.D. (1988). Fuel for muscular exercise:Role of carbohydrate. In
E.S, Horton & R.L.Terjung (Eds.), Exercise, nutrition, and energy metabolism (pp 4571). New York: Macmillan.
Saper, C.B., Loewy, A.D., Swanson, L.W. & Cowan, W.M. (1976). Direct hypothalamoautonomic connections. Brain Research, 117 ,305- 312.
Saxena, P.R. (1992). Interaction between the renin-angiotensin- aldosterone and
sympathetic nervous system. Journal of Cardiovascular Pharmacology 19, Suppl.6,
S80-S88.
Simon, E., Pierau, F.-K., & Taylor, D.C.M. (1986). Central and peripheral thermal control
of effectors in homeothermic temperature regulation. Physiological reviews, 66 , 235300.
Speth, R.C., Dinh, T.T. & Ritter, S. (1987). Nodose ganglionectomy reduces angiotensin
II receptor binding in the rat brainstem. Peptides, 8 , 677-685.
61
62
Spyer, K.M. (1990). The central nervous
organization of reflex circulatory control. In
A. D. Loewy & K.M. Spyer (Eds.), Central regulation of autonomic functions (pp.168188). New York: Oxford University Press.
Stanek, K.A., Neil, J.J., Sawyer, W.B. & Loewy, A.D. (1984). Changes in regional blood
flow and cardiac output after glutamate stimulation of the A5 cell group. American
Journal of Physiology, 246 ,H44- H51.
Stolwijk, J.A.J. & Hardy, J.D.(1977). Control of body temperature. In D.H.L. Lee, H.L.
Falk & S.D. Murphy (Eds.), Reactions of Environmental Agents, Handbook of
Physiology, Section 9 (pp45- 68). Bethesda: American Physiological Society.
Strack, A. m., Sawyer, W.B., Platt, K.B. & Loewy, A.D. (1989). CNS cell groups
regulating the sympathetic nervous outflow to adrenal gland as revealed by
transneuronal cell body labelling with pseudorabies virus. Brain Research, 491, 276296.
Tempel, D.L. & Leibowitz, S.F.(1993). Glucocorticoid receptors in PVN: interactions with
NE, NPY, and Gal in relation to feeding. American Journal of Physiology, 265 , E794E800.
Uehara, A., Sekiya,C., Takasugi, Y., Namiki, M. & Arimura, A. (1989). Anorexia induced
by interleukin 1: involvement of corticotropin- releasing factor. American Journal of
Physiology 257, R613-R617.
Wahren,J., Felig,P.Hendler,R., & Ahlborg, G.. (1971). Glucose and amino acid
metabolism during recovery after exercise. Journal of Applied Physiology 34 , 838-845.
Wall, P.D. & Melzack R. (Eds). (1985). Textbook of pain. Edinburg: Churchill,
Livingstone.
Waldrop, T.G., Bauer, R.M., & Iwamoto, G.A. (1988). Microinjection of GABA
antagonists into the posterior hypothalamus, locomotor activity and a cardiorespiratory
activation. Brain Research, 444 ,84- 94.
Walls, E.K., Phillips, R.J., Wang, F.B., Holst, M.C., & Powley, T.L. (1995). Suppression
of meal size by intestinal nutrients is eliminated by celiac vagal deafferentation.l
American Journal of Physiology, 269, R1410-R1419.
Willems, J.L.. Buglaert, W.A., Lefebvre, R.A., and Bogaert,M.G. (1985). Neuronal
dopamine receptors on autonomic ganglia and sympathetic nerves and dopamine
receptors in the gastrointestinal system. Pharmacological Reviews, 37, 165-207.
Yamashita, H. , Kannan, H., Inenaga,K. & Koizumi, K. (1984). The role of
cardiovascular and muscle afferent systems in control of body water balance. Journal of
the Autonomic Nervous System, 10 , 305-316.
62
63
Young, J.B. & Landsberg, L. (1984). The
sympathoadrenal system and exercise:
Potential metabolic role in trained and untrained states. In: K.T. Borer, D.W.Edington, &
T.P.White (Eds), Frontiers of Exercise Biology (pp 152-172). Champaign: Human
Kinetics Publishers.
Young, J.B., Rosa, R.M. & Landsberg, L. (1984). Dissociation of sympathetic nervous
system and adrenal medullary responses. Americal Journal of Physiology, 247, E35E40.
OC\MS\DOS280:\\manuscr\\anschapt.f98}
63