Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
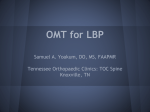
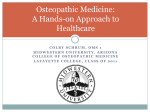
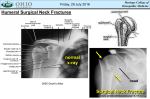
Osteopathic Medicine The Heart Luc Peeters & Grégoire Lason The Heart Luc Peeters & Grégoire Lason All rights reserved. Osteo 2000 bvba © 2013. No part of this e-book may be reproduced or made public by printing, photocopying, microfilming, or by any means without the prior written permission of the publisher. Contact: Osteo 2000, Kleindokkaai 3-5, B – 9000 Ghent, Belgium Mail: [email protected] Web: http://osteopedia.iao.be and www.osteopathie.eu Tel: +32 9 233 04 03 - Fax: +32 55 70 00 74 ISBN: 9789074400275 The International Academy of Osteopathy – I.A.O. 2 Content Content ....................................................................................................................... 3 1. Introduction ............................................................................................................ 6 2. Anatomy ................................................................................................................. 7 2.1. Position ............................................................................................................ 7 2.2. Anatomical Fixations .................................................................................... 11 3. Physiology ............................................................................................................ 14 3.1. General ........................................................................................................... 14 3.2. Function of the Valves .................................................................................. 16 3.3. Arterial Blood Supply ................................................................................... 17 3.4. Venous Drainage ........................................................................................... 18 3.5. Blood Pressure .............................................................................................. 18 3.5.1. General ..................................................................................................... 18 3.5.2. Short-term Control of the Blood Pressure ................................................ 20 3.5.3. Chemoreceptors in the Macula-Densa of the Kidney ............................... 22 3.5.4. Long-Term Control of the Blood Pressure ................................................ 24 3.6. Innervation ..................................................................................................... 24 3.6.1. Autonomic Regulation .............................................................................. 24 3.6.2. Parasympathetic Control of the Heart Rate .............................................. 25 3.6.3. Sympathetic Control of the Heart Rate ..................................................... 26 3.7. Control of the Extracellular Fluid Volume .................................................. 28 3.7.1. The Chemoreceptors ................................................................................ 28 3.8. Reflexes ......................................................................................................... 29 3.8.1. Bainbridge Reflex ..................................................................................... 29 3.8.2. Vagal Cardiopulmonary Reflexes ............................................................. 29 3.8.3. The Trigeminocardiac Reflex .................................................................... 29 3.8.4. The Occulocardiac Reflex (Aschner Reflex) ............................................. 29 3.8.5. Carotid Sinus Reflex ................................................................................. 30 3.8.6. Cervical Manipulation ............................................................................... 30 3.8.7. Spinal Lesions .......................................................................................... 30 4. Mobility ................................................................................................................. 31 5. Patient History and Physical Diagnosis ............................................................ 33 5.1. Risk Factors ................................................................................................... 33 5.2. Coronary Heart Disease ............................................................................... 33 5.3. Congestive Heart Failure .............................................................................. 34 5.4. Arrhythmia ..................................................................................................... 36 5.5. The Athletic Heart ......................................................................................... 36 5.6. Congenital Heart Disease ............................................................................. 37 5.7. Endocarditis .................................................................................................. 37 5.8. Conditions of the Valves .............................................................................. 37 5.9. High Blood Pressure ..................................................................................... 37 3 5.10. Low Blood Pressure ................................................................................... 40 6. Clinical Diagnosis ................................................................................................ 41 6.1. Observation ................................................................................................... 41 6.1.1. Internal Jugular Vein ................................................................................. 41 6.1.2. External Jugular Vein ............................................................................... 42 6.2. Palpation ........................................................................................................ 43 6.3. Auscultation .................................................................................................. 45 6.4. Percussion ..................................................................................................... 51 6.5. Body Mass Index (BMI) ................................................................................. 51 6.6. Specific Tests ................................................................................................ 52 6.6.1. Mobility Test of the Lower Ribs in the Frontal Plane ................................ 52 6.6.2. Mobility Test of the Lower Ribs in the Sagittal Plane ............................... 53 6.6.3. Mobility Test of the Lower Ribs in the Horizontal Plane ........................... 53 6.6.4. General Mobility Test ................................................................................ 54 6.6.5. Elasticity Test in Anteroposterior Direction ............................................... 54 7. Osteopathic Techniques ..................................................................................... 55 7.1. Stretch of the Intrathoracic Fascia .............................................................. 55 7.2. Stretch of the Left Intrathoracic Fascia ...................................................... 56 7.3. Thorax Recoil ................................................................................................ 56 7.4. Diaphragm Recoil .......................................................................................... 57 7.5. Mobilisation of the Intrathoracic Fascia ..................................................... 58 7.6. Relaxation of the Cardiac Plexus ................................................................ 58 7.7. Doming Technique ........................................................................................ 59 7.8. Doming Technique with Rib Lift .................................................................. 59 7.9. Osteopathic Techniques .............................................................................. 60 7.10. Neurolymphatic Reflex Points ................................................................... 60 8. Bibliography ......................................................................................................... 62 9. About the Authors ............................................................................................... 66 10. Acknowledgements ........................................................................................... 67 11. Visceral Osteopathy .......................................................................................... 68 11.1. Introduction ................................................................................................. 68 11.2. Motion Physiology ...................................................................................... 69 11.2.1. The Motions of the Musculoskeletal System .......................................... 69 11.2.2. The Motions of the Visceral System ....................................................... 69 11.2.2.1 The Diaphragm ................................................................................. 69 11.2.2.2. The Heart ......................................................................................... 70 11.2.2.3. Peristalsis ......................................................................................... 70 11.3. Visceral Interactions ................................................................................... 70 11.3.1. General ................................................................................................... 70 11.3.2. Relationships .......................................................................................... 71 11.3.2.1. Gliding Surfaces ............................................................................... 71 4 11.3.2.2. Ligamentous Suspensory System ................................................... 71 11.3.2.3. The Mesentery ................................................................................. 71 11.3.2.4. The Omenta ..................................................................................... 72 11.3.2.5. The Turgor Effect and the Intracavitary Pressures .......................... 72 11.4. Mobility Loss ............................................................................................... 72 11.4.1. Diaphragm Dysfunction .......................................................................... 72 11.4.2. Adhesions ............................................................................................... 72 11.4.3. Retractions ............................................................................................. 73 11.4.4. Trophic Tissue Changes ......................................................................... 73 11.4.5. Congestion ............................................................................................. 73 11.4.6. Postural Disorders .................................................................................. 73 11.4.7. Visceral Mobility Loss ............................................................................. 74 11.5. Visceral Hypermobility ............................................................................... 75 11.6. Osteopathic Visceral Examination ............................................................ 75 11.7. Bibliography Visceral Osteopathy ............................................................. 76 12. Abbreviations ..................................................................................................... 77 13. Specific Terms ................................................................................................... 78 14. All Videos ........................................................................................................... 79 5 1. Introduction One of the principles in osteopathic medicine is optimisation of the circulation in the region of complaint. The heart obviously plays an important role in this. How can the osteopath improve the local circulation if the heart is not in an optimal state of function? The correction of cervical, upper thoracic, costal, diaphragm and craniosacral lesions*, together with stretching of intrathoracic fascial retractions, the mobilisation of the blood pressure regulating organs and advice related to diet and general lifestyle are therefore important. Heart dysfunctions often dominate the complaint of a patient without there being a specific heart complaint as such. The osteopath can quickly identify this by way of somatic dysfunctions in the region T1-T5. In this e-book, the functional anatomy, physiology and neurology are discussed as well as the heart mobility and the ways in which the osteopath deals with such dysfunctions. For readers who are unfamiliar with the osteopathic visceral approach, please refer to Chapter 11 at the end of this e-book. * PS: a lesion is a functional loss of mobility. The term lesion has another meaning in osteopathy than in classic medicine where it refers to a structural defect in the human structure. 6 2. Anatomy (Anderson & Wilcox 1998, Baert et al, Dalley & Agur 2004, Grant & Boileau 2004, Gray 2000, Kirklin & Barratt-Boyes 1993, Netter 2003, Schlant & Silverman 1986, Sobotta 2001, Spence 1986, Tortora & Grabowski 2000, Zimmerman 1966) 2.1. Position The heart: • Is approximately the size of a fist and is in the thorax, above the diaphragm and left of the sternum. • Is in the middle mediastinum (Figure 1, 2 and 3). • Is a hollow organ that weighs approximately 300 g and has 4 chambers. Posterior mediastinum: • descending aorta • oesophagus • azygos v. • sympathetic trunk • thoracic duct Anterior and anterosuperior mediastinum: • thymus • fat • lymph vessels Middle mediastinum: • heart • pericardium • aorta • trachea • bronchi • lymph nodes Figure 1 - The mediastinum 7 4. Mobility Due to the fact that caudal surface of the heart is strongly related to the diaphragm, it will also follow the cranio-caudal movements of the diaphragm (Figure 30). (Holland et al 1998, Mc.Leish et al 2002, Peeters 2005, Porat et al 2000, Wang et al 1995) The movement of the heart as influenced by respiration is a global translation. Dorsal Ventral Figure 30 - The mobility of the heart During inhalation the diaphragm descends. The heart follows this displacement caudally (Figure 31). This results in traction along the vertebropericardiac, bronchopericardiac and tracheopericardiac ligaments and along the superior sternopericardiac lig. If these ligaments are trophically changed and their elasticity is reduced, this caudal force will be directly transferred to the spine at T2-T4, the sternum and the trachea and the bronchi (Figure 31). This is most likely why periostial sensitivity is so frequently found at T2-T4. Such vertebropericardiac traction could play an important role in complaints of the trachea, bronchi and thyroid (Figure 31). The “thoracic outlet” is significantly influenced and “thoracic outlet” symptoms are likely to result. 31 External jugular v. 4 tot 5 cm Height of the observed distension Height of the sternal angle 45° Figure 34 - Observation of the external jugular vein 6.2. Palpation Palpation of the cardiac pulse is done with the right hand flat upon the left hemithorax; thenar and hypothenar on the sternum and the index finger under the nipple. For female patients the right hand is placed under the left breast. The osteopath pays attention to: • Is there a point of maximum pulsation that can be localised at the height of the apex of the left ventricle? Try to localise this point with the fingertip. • Normally this point is the size of a coin along the midclavicular line at the height of the 5th intercostal space. • In cases of left ventricle enlargement (previous infarct(s)) this point will be displaced laterally. An obvious enlargement can mean that the point is found along the axillary line. • If this pulse point is not readily found this does not always indicate pathology. Palpation of the point with the patient lying on the left side can aid the palpation. Palpation of the apex: Video 1 - Palpation of the apex 43 7. Osteopathic Techniques 7.1. Stretch of the Intrathoracic Fascia (Figure 52) The patient is supine, the legs straight and with the level of T2-3 on the edge of the table. The head is supported in the hands of the osteopath. Central fascias The osteopath applies traction from the occiput, protecting the cervical spine by avoiding lordosis, and asks the patient to breath in deeply – first via the abdomen, then via the thorax. The patient is requested to breath in as deep as possible, to hold the shoulders against the table and to avoid any lumbar lordosis. This is repeated until less caudal resistance is felt via the head. Lateral fascias The osteopath brings the head of the patient into opposite sidebending (C7) and ipsilateral rotation (C6), gives traction on the occiput, protecting the cervical spine by avoiding lordosis, and asks the patient to breath in deeply – first via the abdomen, then via the thorax while holding the shoulders against the table. This is repeated until less caudal resistance is felt via the occiput. If, after four repetitions, the fascias are not loosening there are musculoskeletal lesions that are limiting the motion. These must be corrected. Video 8 - Stretch of the intrathoracic fascia 55 9. About the Authors Grégoire Lason Gent (B), 21.11.54 Luc Peeters Terhagen (B), 18.07.55 Both authors are holders of university degrees, namely the Master of Science in Osteopathy – University of Applied Sciences, and are very active with the promotion and academic structuring of osteopathy in Europe. In 1987 they began The International Academy of Osteopathy (IAO) and are, to this day, the joint-principals of this academy. The IAO is since several years the largest teaching institute for osteopathy in Europe. Both osteopaths are members of diverse professional organisations, including the American Academy of Osteopathy (AAO), the International Osteopathic Alliance (IOA), the World Osteopathic Health Organisation (WOHO), as part of their mission to improve osteopathic development. This osteopathic encyclopaedia aims to demonstrate the concept that a proper osteopathic examination and treatment is based upon the integration of three systems: the musculoskeletal, visceral and craniosacral systems. 66 This e-book is a product of Osteo 2000 bvba. If you are interested in publishing an e-book or if you have questions or suggestions, please contact us: Mail: [email protected] Fax: +32 55 70 00 74 Tel: +32 9 233 04 03 Web Osteopedia: http://osteopedia.iao.be Web The International Academy of Osteopathy – IAO: http://www.osteopathie.eu 80