Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
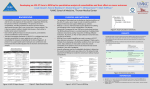
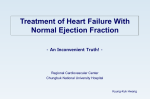
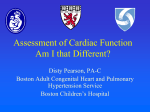
Peter Kenneth Ndege, MD Consulting Physician Kenyatta National Hospital Honorary Lecturer University of Nairobi School of Medicine Founder and Executive Director, Center for Addiction Studies in Africa Email: [email protected] Tel: +254 722 642 744 Medical Comorbidities Medical Co-Morbidities in the Substance Using Patient GOALS • Understand that alcohol and drug use can become disorders, that are chronic medical conditions • Understand the epidemiology and harm associated with alcohol and other drug use • Understand the complex relationship between alcohol and other drug use with other disease processes Medical Comorbidities OUTLINE • Discuss the harm and other diseases associated with the use of the “big three” substances: – Alcohol – Opioids – Cocaine • Discuss (briefly!) the harm and other diseases associated with the use of “non-bigthree” substances • Discuss the complexity of defining and clinically dealing with co-morbidities • Summarize and further discussion Medical Comorbidities BACKGROUND • Alcohol and other drug use patients who present for treatment often have other medical problems • These medical conditions are consequences – of both their current and their past high risk behaviors – Injection or route of drug use – direct toxic effects of illicit drugs or caustic agents • Clinicians should screen for and treat (or refer for treatment) common comorbid medical conditions Medical Comorbidities BACKGROUND • Treating alcohol and other drug use in an office based settings provides a unique opportunity to integrate the delivery of substance abuse treatment with screening and management, increasing effectiveness and patient compliance • Clinicians should know the common comorbid medical conditions found in alcohol and other drug use patients and promote preventive health care for these patients Medical Comorbidities Medical Comorbidities ALCOHOL USE and DISORDERS: HARM and MEDICAL CO-MORBIDITIES Medical Harm of Hazardous Drinking • Hazardous drinking is associated with an increased risk for: – – – – – – – All-cause mortality Hypertension Cardiomyopathy Diabetes Trauma Stroke More serious alcohol disorders – Cancers ~ particularly upper GI and breast cancers Medical Comorbidities Figured from Babor et al (World Health Organization), AUDIT Guidelines for Use in Primary Care, 2001 Brief Primer of Physical Exam Features for Alcohol Use • • • • • • • • Tachycardias Tremor Hypertension Hepatosplenomegaly and a tender liver edge Peripheral neuropathy Spider angiomata Conjunctival injection Unexplained trauma Medical Comorbidities Some Associations with Hazardous Drinking • • • • • • Injuries Infections Gastritis and duodenitis Hematologic effects Early hepatic injury Cardiac effects Medical Comorbidities Injuries • Due to – Fights and homicide attempts – Auto accidents ~ 50% of injuries involve some alcohol consumption – Drowning and other accidents – Suicide attempts • Patient neglects injuries until the next day – Injuries not painful until the following day Medical Comorbidities Infections • Heavy drinkers are more susceptible to pneumonia and other infections – Pneumococcal infections – Pseudomonas infections – Gram-negative infections • Heavy drinkers have impaired immunity – – – – Increased sequestration of neutrophils Decreased fixed macrophage phagocytic capacity Decreased white blood cell production Decreased cell mediated immunity Medical Comorbidities Gastritis and Duodenitis • Most commonly observed effects – – – – Epigastric pain Morning nausea and vomiting Melena Gastric Esophageal Reflux Disease (GERD) • Eventually – Consequences of liver disease including varices and portal hypertension Medical Comorbidities Hematologic Effects • Macrocytosis – Due to direct cytotoxic effects – Due to vitamin deficencies • Decreased platelets (may be down to 30,000 to 50,000) • Anemia usually due to – Bleeding from gastrointestinal tract – Folic acid deficiency – Also remember other vitamin deficiencies Medical Comorbidities Hepatic Effects • Alcoholic hepatitis in 10% to 15% of alcoholics – – – – Increased liver enzymes and bilirubin Enlarged tender liver 80% can progress to cirrhosis 20% result in liver failure • Cirrhosis – 40% have a 5-year survival if they continue to drink – 77% have a 5-year survival if they stop drinking • Liver cancer (also esophageal, laryngeal, and nasopharyngeal cancers) Medical Comorbidities Early Hepatic Markers • Increased gamma-glutamyl transpeptidase (GGT) up to 3 times normal in 20% to 30% of heavy drinkers • Liver enzymes – AST/SGOT > ALT/SGPT • Production Problems – Coagulopathies in end stage alcoholic liver disease • Don’t forget the pancreas! – Acute and chronic pancreatitis – Complications: ~ Diabetes, Steatorrhea, Pseudocyst Medical Comorbidities Cardiac Effects • Increased blood pressure – From withdrawal – Without withdrawal • Increased ischemic heart disease • Cardiomyopathy • Arrhythmias – – – – Especially tachyarrhythmias Atrial flutter Atrial fibrillation – “Holiday Heart” Paroxysmal Atrial Tachycardia Medical Comorbidities Nervous System Effects • • • • • Headaches Sleep disorders Wernicke syndrome Korsakoff psychosis Organic brain disease – Cognitive – Memory • Peripheral neuropathy Medical Comorbidities Nervous System Effects C – Confusion O – Ophthalmalplegia A – Ataxia T – Early Thiamine Deficiency (Wernicke’s) R – Retrograde Amnesia A – Anterograde Amnesia C – Confabulation and meager Conversation K – Korsakoff Syndrome (Also lack of INsight and Greater apathy) Medical Comorbidities Fetal Alcohol Spectrum • Growth retardation – Head circumference, height, and weight less than tenth percentile • Facial malformation – Palpebral fissure – Philtrum – Thin upper lip • Neurodevelopmental delay – – – – – – Intelligence Boundaries Memory Aggression Motor skills Right/wrong Medical Comorbidities Fetal Alcohol Spectrum • Defects occur before most women know they are pregnant • No known safe level of drinking for pregnant women – Binging may be worse than daily drinking – The higher the blood level of alcohol, the greater the chance of damage Medical Comorbidities Associations with Other Diseases • There exist many diseases that co-exist with alcohol use disorders that may complicate the treatment of either disorder – – – – – HIV Major Depressive Disorder Hepatitis Cirrhosis (Social morbidities – homelessness) • Emerging research is examining treatment modalities for co-morbid conditions Medical Comorbidities Alcohol Use of the Elderly • Of the 80% of elderly persons who have ever consumed alcohol, two-thirds continue to drink, often at hazardous levels of consumption • Of the elderly: – 15% drink alcohol at levels considered hazardous – 5% have diagnosis of abuse or dependence – many more drink sporadically in binge episodes • The problem drinking elderly consist of : – 30% of the hospitalized elderly – 10% of the elderly primary care – 50% of the mentally ill elderly Medical Comorbidities Alcohol Use of the Elderly • With mild alcohol consumption, compared to the non-elderly, the elderly are at increased risk for: – greater numbers of harmful medication interactions – increased falls – more cognitive deficits – greater sleep impairments – increased sexual dysfunction – greater numbers of hip fractures – more psychiatric problems compared to younger populations Medical Comorbidities Alcohol and Breast Cancer • More than 30 epidemiologic studies have evaluated a possible association between alcohol intake and breast cancer • Alcohol consumption is associated with a linear increase in breast cancer incidence in women over the range of consumption reported by most women (Smith-Warner) • In a recent study of 70,000 women, a drink a day increased their risk by 10 percent, and more than three daily drinks by 30 percent (Lew) • Women's Health Study, daily alcohol intake again was shown to modestly increase risk (Zhang) – The relative risk for each 10 gram increase in daily alcohol intake was 1.11 (95% CI 1.03-1.20) for ER and PR+ cancer Medical Comorbidities Smith-Warner SA, JAMA 1998; Lew: Ameri. Assoc. for Cancer Research 2008; Zhang SM, Am J Epidemiol. 2007 Societal Costs of Alcohol Dependence Total Cost: $184.6 Billion $24,093 (13%) $10,085 (5%) $7,466* (4%) $15,963 (9%) $2,909 (2%) $1,253 (1%) $36,499 (20%) Specialty alcohol services Medical consequences (except FAS) Medical consequences of FAS Lost future earnings due to premature deaths Lost earnings due to alcohol-related illness Lost earnings due to FAS Lost earnings due to crime/victims Crashes, fires, criminal justice, etc $86,368 (47%) Medical Comorbidities Harwood H, NIH Publication No. 98-4327 1998 Medical Comorbidities OPIOID USE and DISORDERS: HARM and MEDICAL CO-MORBIDITIES Balloons, Bags, and Pills Medical Comorbidities New Prescription Drug Users Past Year Initiation of Non-Medical Use of Prescription-type Psycho-pharmaceutics Age 12 or Older: In Thousands from 1965 to 2005 3000 New Users (x 1000) 2500 2000 1500 1000 500 0 6 5 96 7 96 9 97 1 97 3 97 5 97 7 97 9 98 1 98 3 98 5 98 7 98 9 99 1 99 3 99 5 99 7 99 9 00 1 00 3 00 5 19 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 2 2 Analgesics Tranquilizers Stimulants Sedatives Medical Comorbidities NSDUH, SAMHSA, 2005 Opioid Withdrawal • • • • • • • • • • • • Severe flu-like symptoms including shaking chills Anxiety Hyperactivity Drooling Lacrimation/Tearing Rhinorrhea/Runny nose Anorexia Nausea Vomiting Diarrhea Myalgias Muscle spasms Medical Comorbidities Street Stuff • Sold in “stamp bags” and “balloons” • A opioid user will maintain a steady supply of opioids - not a binge addiction • Combination of abuse is important – Can be combined with a stimulant (ala speedball) – Rarely with a depressant Medical Comorbidities Changing Route of Heroin Administration Injection Inhalation Smoking Oral Other 100% 80% 60% 40% 20% 0% 1992 1993 1994 1995 1996 1997 1998 1999 2000 Medical Comorbidities Treatment Episode Data System, 1992-2000 Hepatitis B • DEFINITION – Hepatitis B (HBV) is a blood borne viral pathogen • EPIDEMIOLOGY – – – – Estimated 1.25 million chronically infected in U.S. Approximately 300,000 new cases per year Transmission by blood borne, sexual, or perinatal Approximately 50% of active injection drug users have serological evidence of prior exposure to HBV Medical Comorbidities Hepatitis B – Clinical Course • Early and mild viral hepatitis manifests with symptoms of hepatic inflammation and damage with elevated serum transaminases (> 10-20x normal) • Chronic viral hepatitis manifests as chronic liver disease with portal hypertension and poor hepatic synthetic function • Likelihood of developing chronic infection is related to age: – 80 to 90% of infants infected develop chronic disease – only 2 -10% of infected adults progress to chronic disease Medical Comorbidities Acute Hepatitis B Infection with Recovery Symptoms HBeAg anti-HBe Total anti-HBc Titer 0 4 anti-HBs IgM anti-HBc HBsAg 8 12 16 20 24 28 32 36 Medicalafter Comorbidities Weeks Exposure 52 100 Progression to Chronic Hepatitis B Infection Acute (6 months) Chronic (Years) HBeAg anti-HBe HBsAg Titer Total antiHBc IgM anti-HBc 0 4 8 12 16 20 24 28 32 36 52 Medical Comorbidities Weeks after Exposure Years Hepatitis C - Epidemiology • Hepatitis C (HCV) is the most common bloodborne infection in the U.S. – 1.8% of the U.S. population are infected – Of the 3.9 million people in the U.S. who are infected, 2.7 million are chronically infected • At least 30,000 new infections (cases) annually • Morbidity and mortality – Chronic liver disease – HCV-related: 40% - 60% – Deaths HCV chronic disease/year: 8,000-10,000 – Most common reason for (~40%) liver transplants Medical Comorbidities Hepatitis C - Epidemiology • In some series, greater than 90% of injection drug users have antibodies to HCV • HCV is more prevalent and more infectious than HIV – with 170,000,000 infected with HCV worldwide – In injection drug users, infection results from contact with contaminated needles, syringes, paraphernalia – Blood and blood products are more infectious than saliva, vaginal secretions, or semen Medical Comorbidities Hepatitis C: Acute Infection with Recovery antiHCV Symptoms +/- Titer HCV RNA ALT Normal 0 1 2 3 4 Months 5 6 1 Medical Comorbidities Time after Exposure 2 3 Years 4 Hepatitis C: Progression to Chronic Infection antiHCV Symptoms +/- Titer HCV RNA ALT Normal 0 1 2 3 4 Months 5 6 1 Medical Comorbidities Time after Exposure 2 3 Years 4 CHRONIC Hepatitis C: Clinical Course • Symptoms: 50% of patients report chronic fatigue and abdominal discomfort • Serum transaminases: – Persistently elevated – intermittently elevated – normal - 43% - 42% - 15% • Risk factors for disease progression: – alcohol use, hepatitis B virus, HIV (modifiable risks) – < 40 years old when infected, male sex Medical Comorbidities 30 Year Progression of Chronic Hepatitis C Acute hepatitis C >85% (10 years) Chronic hepatitis C 20% - >50% (20 years) Cirrhosis < 20% < 20% Hepatic failure HCC (30 years) Medical Comorbidities Hepatitis C: HIV Co-infection • 30% of HIV positive patients in the U.S. are co-infected with HCV • In HIV infected injecting drug users, the prevalence of HCV is 50 to 90% • HIV has a significant effect on progression of liver disease in HCV-infected patients • Must balance hepatotoxicity of HIV therapy with need to treat HIV in HCV-infected patients, while HIV therapy can worsen the symptoms of HCV Medical Comorbidities Hepatitis C: Treatment in Drug Users • Standard recommendation: >/=6 months “clean” • Arguments for not treating: poor adherence, side effects, re-infection, non-urgent treatment – but data supporting these arguments are lacking, some drug users may do well • Treatment should be based on individual riskbenefit assessments – Edlin BR et al. NEJM 345:211-214, 2001 Medical Comorbidities Hepatitis C: Treatment in Drug Users • The 2002 NIH Consensus Guideline on the Treatment of HCV is available at – Active injecting drug use should not exclude patients from HCV treatment – HCV treatment of active injecting drug users should be considered on a case-by-case basis – Web site: http://www.guideline.gov Medical Comorbidities HIV/AIDS: Epidemiology • Approximately 1.1 million cases in the US • 0.7 - 34% (median 15%) seroprevalence entering substance abuse treatment • IV Drug Use (IVDU) associations – From 1993-1999 IVDU persons living with AIDS jumped from 48,244 to 88,540 – 15-20% long-term IVDUs infected (43% of women AIDS) – 25% of the approximately 40,000 new HIV infections/year through IVDU Medical Comorbidities HIV/AIDS: Treatment in Drug Users • High risk for non-receipt of antiretrovirals: – 2-3 times as likely not to be on antiretroviral treatment if not in SA treatment • High risk for non-adherence: – 1998 CDC guidelines recommend delaying HAART until active opioid use has been addressed Medical Comorbidities Tuberculosis: Epidemiology • Worldwide, approximately 2 billion people (1/3 of world population) are infected with M. tuberculosis • Since the HIV pandemic began in the U.S. in the mid-1980s, there has been increased concern about TB since it is more common in this population • Tuberculosis is also more common in alcohol users and injection drug users in general and in patients with alcohol use disorders Medical Comorbidities Opioid Dependence is Costly • Medical Costs • Mental illness • An environmental and disease stressor • Co-morbid interactions • Trauma and infections • Hepatitis and HIV • Medical Cost • $20 billion per year total costs • $1.2 billion per year health care costs Medical Comorbidities How Do They Get Hooked? Medical Comorbidities COCAINE USE and DISORDERS: HARM and MEDICAL CO-MORBIDITIES Cocaine • Cocaine is a product of the alkaloid extract from leaves of the Erthroxylon plant originally grown in the Andes Mountains of western South America • Evidence of use in 500 AD - coca leaves in tombs in Bolivia and Peru • Cocaine was used by Sigmund Freud • William Halsted used cocaine for anesthesia in 1884 • Today, cocaine is still used (sparingly) as a local anesthetic in the upper respiratory tract in concentrations of 4% Medical Comorbidities Cocaine • As many as 20 million people in the United States have used cocaine at least once in their lifetime • In New York City, cocaine use is extremely prevalent and in one survey 26% of people sustaining fatal injuries had evidence of cocaine metabolites in their urine or blood • Of pregnant women, an estimated 11% are substance abusers and cocaine is the most commonly abused drug other than alcohol • Cocaine has increasingly been associated with criminal behavior Medical Comorbidities Street Stuff • Cocaine exists in many forms – Powder – Freebase – Rock (crack) • Crack is convenient – The soft mass that develops becomes hard when dry – The crack can then be smoked (potent!) – Usually it is smoked in a glass pipe or regular pipe or by mixing it with tobacco or marijuana – Crack is thought to be termed by the sound of cocaine crystals ‘popping” when smoked Medical Comorbidities Cocaine Intoxication • Clinically significant maladaptive behavioral or psychological changes that developed during, or shortly after, use of cocaine. • Two (or more) of the following developing during or shortly after cocaine use: – – – – – – – – Tachycardia or bradycardia Pupillary dilation Elevated or lowered blood pressure Perspiration or chills Nausea or vomiting Evidence of weight loss Psychomotor agitation or retardation Muscular weakness, respiratory depression, chest pain, or cardiac arrhythmias – Confusion, seizures, dyskinesias, dystonias, or coma Medical Comorbidities Morbidity and Co-morbidity of Cocaine • Can be deadly in intoxication – Mainly due to adrenergic stimulus ~ Think that you are injecting epinephrine into the blood – Morbidity can occur secondary to social consequences as well as direct effects • Long term – – – – Cardiac - cardiomyopathy, hypertension, arrythmias Pulmonary – if smoked Renal – rhabdomyolysis and “tea colored urine” Cerebral – TIAs and strokes Medical Comorbidities Cocaine Physical Exam • • • • Track marks (injection use) Burnt lips/face/hair Hand findings Look for nasal perforation or hyperemic nares Medical Comorbidities OTHER DRUG CO-MORBIDITIES (briefly!) Methamphetamine: Don’t be fool!!! Faces to remember Medical Comorbidities Methamphetamine effects on families Children of Methamphetamine Addicts are filling the foster care system across the country Medical Comorbidities Methamphetamine effects Disrupt sleeping patterns, suppresses appetite, and causes irritability/aggression Medical Comorbidities Methamphetamine effects on the state of mind Psychotic, Paranoia, Hallucination, and agitation Medical Comorbidities Methamphetamine effects on the Penal System The Penal System is flooding with Methamphetamine Addicts. Recovery Centers are increasing at an alarming rate. Medical Comorbidities Methamphetamine effects on health Increase pulse rate, increase blood pressure, increase hyperthermia, stroke and death Medical Comorbidities Methamphetamine effects on behavior Repetitive behavior, obsessive behavior, and delusional thinking Medical Comorbidities Methamphetamine effects on health Nervousness, anxiety, convulsions and Heart attack Medical Comorbidities Methamphetamine effects on the community Homelessness, theft, and crime Medical Comorbidities Methamphetamine effects on society Sexual Transmitted Diseases to include HIV/AIDS Medical Comorbidities Methamphetamine effects on dreams loss of job, loss of ambition, and loss of direction Medical Comorbidities Methamphetamine effects on recidivism Chronic Relapse, loss hope, and loss dreams Medical Comorbidities Medical Comorbidities The term”narcotic” generally refers to opium and to painkilling drugs made of opium. These include heroin, morphine, and codeine. Codeine is legally, but not medically, classified in the United States, but is an illicit narcotic drug. Narcotics depress the brain and result in feelings of pleasure, strength and superiority, followed by lethargy, drowsiness, confusion, and depression of the heart rate. Intravenous (IV) drug users risk exposure to the AIDS virus when they use or share contaminated needles. IV drug users form the group with the fastest growing number of persons with AIDS (PWAs). Medical Comorbidities Inflammation of the liver is one of the most common problems seen in heroin addicts. It is caused by a virus which is transmitted from one person to another through contaminated needles. The liver becomes swollen, and irregular patters of light-colored inflammation can be seen seen scattered throughout. Hepatitis causes weakness, loss of appetite, tenderness in the abdomen, dark-colored urine, and a yellowish Medical Comorbidities change in the color of the skin and A dangerous complication can occur when blood cloths in the veins of an addict’s arms break off and float through the bloodstream to the heart and lungs. A well-formed blood clot can be seen extending almost completely through the course of this pulmonary artery within the lungs. This patient will die because the blood cloth has shut off the Medical Comorbidities blood supply to the When germs are injected into the bloodstream from an unsterile needle, they may travel through the body and lodge in the brain. In this illustration, note the ragged, abscessed cavity filled with pus. Medical Comorbidities High fever, convulsions, coma, and If germs enter the bloodstream from an unclean needle, they may spread throughout the body and lodge in the valves of the heart, causing a serious infection know as bacterial edocarditis. The warty-like growths seen on these heart valves produce symptoms of fever, weakness, heart failure, and death. Tiny showers of clots and bacteria may be released from the growths on the infected heart valves. They may then spread to the kidneys and spleen. The results of these showers are seen as multiple red spots in the kidney, and as a grayish area of dead tissue at the Medical Comorbidities uppermost portion of the spleen. This usually results in the death of a drug user. When an addict’s veins are repeatedly punctured, particularly by unsterile needles, blood clots and Medical Comorbidities scarring may occur within the veins. TOBACCO Medical Comorbidities 80 • Buerger’s Disease. Blood vessels get blocked and this starves the body parts which may lead to amputation of arms. Medical Comorbidities 81 Medical Comorbidities 82 Smokeless tobacco can cause oral cancer, gum disease, increased tooth decay and periodontal bone loss. It may also lead to an increased risk of the upper digestive tract Medical Comorbidities 83 Medical Comorbidities 84 Medical Comorbidities 85 Khat (Miraa) Medical Comorbidities 86 Medical Comorbidities 87 Short-term Effects of Miraa • Excitation – likened to an intense sexual orgasm and sensation of extreme mental and physical power. • Palpitation, irregular heartbeats and high blood pressure • Rapid talking, Restlessness • Increased rate of respiration • Lack of sleep (insomnia) • Browning of teeth and foul breath • Poor concentration • False feeling of well-being • Psychological dependence Medical Comorbidities 88 Long term effects of Miraa • • Memory loss, personality disorders, depression Mouth, tongue and lip ulcers which may predisposes an individual to HIV/AIDS • Oral cancer • Nerve damage leading to numbness • Hallucinations • Excessive irritability • Chronic constipation-slow passage of food through the stomach and intestines Medical Comorbidities 89 Inhalants Medical Comorbidities 90 Medical Comorbidities 91 Inhalants: Classification • Inhalants are breathable chemical vapors that produce psychoactive (mind altering) effects • A variety of products common in the home and in the workplace contain substances that can be inhaled • Inhalants fall into the following categories: • Volatile Solvents • • Industrial or household solvents, including paint thinners or removers, degreasers, dry-cleaning fluids, gasoline, and glue • • Art or office supply solvents, including correction fluids, felt-tip-marker fluid, and electronic contact cleaners Medical Comorbidities 92 Inhalants: Classification… • Aerosols Household aerosol propellants and associated solvents in items such as spray paints, hair or deodorant sprays, fabric protector sprays, aerosol computer cleaning products, and vegetable oil sprays • • Gases Gases used in household or commercial products, including butane lighters and propane tanks, whipping cream aerosols or dispensers (whippets), and refrigerant gases • Medical anesthetic gases, such as ether, chloroform, halothane, and nitrous oxide (“laughing gas”) Medical Comorbidities 93 Inhalants: Classification… • Nitrites • Organic nitrites are volatiles that include cyclohexyl, butyl, and amyl nitrites, commonly known as “poppers.” Amyl nitrite is still used in certain diagnostic medical procedures. • Volatile nitrites are often sold in small brown bottles labeled as “video head cleaner,” “room odorizer,” “leather cleaner,” or “liquid aroma.” Medical Comorbidities 94 Health Hazards Harmful irreversible effects that may be caused by abuse of specific solvents include: Hearing loss—toluene (spray paints, glues, dewaxers) and trichloroethylene (dry-cleaning chemicals, correction fluids) Peripheral neuropathies, or limb spasms—hexane (glues, gasoline) and nitrous oxide (whipped cream dispensers, gas cylinders) Central nervous system or brain damage—toluene (spray paints, glues, dewaxers) Bone marrow damage—benzene (gasoline) Medical Comorbidities 95 Health Hazards… Serious but potentially reversible effects include: • Liver and kidney damage—toluene containing substances and chlorinated hydrocarbons (correction fluids, dry-cleaning fluids) • Blood oxygen depletion—aliphatic nitrites (known on the street as poppers, bold, and rush) and methylene chloride (varnish removers, paint thinners) Medical Comorbidities 96 ADDRESSING CO-MORBIDITIES TREATMENTS IN PRACTICE CROSSING THE QUALITY CHASM • “Quality problems occur typically not because of failure of goodwill, knowledge, effort or resources devoted to health care, but because of fundamental shortcomings in the ways care is organized” • Trying harder will not work: changing systems of care will! a new HEALTH system for the 21st century (IOM, 2001) Medical Comorbidities SIX AIMS OF QUALITY HEALTH CARE 1. Safe – avoids injuries from care 2. Effective – provides care based on scientific knowledge and avoids services not likely to help 3. Patient-centered – respects and responds to patient preferences, needs, and values Medical Comorbidities SIX AIMS 4. Timely – reduces waits and sometimes harmful delays for those receiving and giving care 5. Efficient – avoids waste, including waste of equipment, supplies, ideas and energy 6. Equitable – care does not vary in quality due to personal characteristics (gender, ethnicity, geographic location, or socio-economic status) Medical Comorbidities SIX CRITICAL PATHWAYS FOR ACHIEVING AIMS AND RULES • New ways of delivering care • Effective use of information technology (IT) • Managing the clinical knowledge, skills, and deployment of the workforce • Effective teams and coordination of care across patient conditions, services and settings • Improvements in how quality is measured • Payment methods conducive to good quality Medical Comorbidities END GOD BLESS YOU Medical Comorbidities Medical Comorbidities MEDICAL AND SUBSTANCE-USE CONDITIONS • Pervasive – More than 33 million Americans treated annually ~ 20 % of all working age adults (18-54) ~ 21 % of adolescents ~ Millions more fail to receive care • Frequently intertwined – 15 - 40 % co-occurrence • Often influence general health – frequently accompany chronic illnesses – 20% of heart attack patients suffer from depression, tripling risk of death – associated with leading causes of outpatient visits; e.g., headache, fatigue and pain Medical Comorbidities MENTAL, SUBSTANCE-USE, & GENERAL HEALTH CONCLUSION • Improving care delivery and outcomes for any one of mental health, substance use, and general health disorders depends upon improving care and outcomes for the other two. OVERARCHING RECOMMENDATION • Health care for general, mental, and substance-use problems and illnesses must be delivered with an understanding of the inherent interactions between the mind/brain and the rest of the body. Medical Comorbidities CH 3. PATIENT CENTERED CARE RECOMMENDATIONS FOR CLINICIANS • Incorporate informed, patient-centered decision making throughout practices • To ensure informed decision making • Adopt recovery-oriented and illness selfmanagement practices that support patient preferences for treatment Medical Comorbidities CH 3. PATIENT CENTERED CARE RECOMMENDATIONS FOR CLINICIANS • Coercion should be avoided whenever possible. • When coercion is legally authorized, patientcentered care is still applicable and should be undertaken. Medical Comorbidities CH 5. COORDINATING CARE RECOMMENDATIONS FOR CLINICIANS • Implement policies and incentives to continually increase collaboration among providers to achieve evidence-based screening and care of patients. • Clinical practices should transition along a continuum of evidence-based coordination models: – – – – Formal agreements Case management Co-location Integrated practices Medical Comorbidities Core Components of Comprehensive Services Medical Financial Housing & Transportation Core Treatment Intake Assessment Child Care Treatment Plans Group/Individual Counseling Abstinence Based Pharmacotherapy Mental Health Urine Monitoring Case Management Continuing Care Self-Help (AA/NA) Family AIDS/HIV Risks Vocational Educational Legal Medical Comorbidities Etheridge, Hubbard, Anderson, Craddock, & Flynn, 1997 (PAB). Substance Abuse is a Chronic Medical Condition • Type 1 Diabetes: – 30% to 50% relapse each year requiring additional medical care – Significant societal consequences • Hypertension and Asthma: – 50% to 70% relapse each year requiring additional medical care – Significant societal consequences • Alcohol and Other Drug Diseases. – 40% to 60% relapse each year – Significant societal consequences – Few patients receive treatment! Medical Comorbidities McLellan, JAMA, 2000