Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
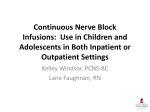
Downloaded from http://inpractice.bmj.com/ on May 2, 2017 - Published by group.bmj.com NURSING Nursing critically ill patients in the intensive care unit Elle Haskey Critically ill patients present a challenge to the whole veterinary team because they require invasive diagnostic tests, advanced procedures and intensive nursing care. It is important to start with an assessment of the patient to prioritise concerns and develop a care plan tailored for the individual. The nursing process involves the implementation and delivery of this plan, followed by evaluation of the nursing/treatments. This is a cyclical process that is repeated over and over again as the patient’s key parameters are reassessed and a further plan is made. The aim of this article is to explore some key aspects of critical care nursing, including infection control and hand hygiene, the management of tubes and lines, and dealing with recumbent patients. Infection control and hand hygiene A health care-associated infection (HCAI) has been defined by the World Health Organization (WHO) in 2011 as: ‘an infection occurring in a patient during the process of care in a hospital or other health-care facility which was not present or incubating at the time of admission. This includes infections acquired in the hospital, but appearing after discharge, and also occupational infections among staff of the facility.’ WHO estimated that the prevalence of HCAIs in people in 2010 was 7.6 per cent, and this increased to 30 per cent in patients in an intensive care unit due to several factors: ■■ Invasive devices in situ; ■■ Immunosuppression; ■■ Trauma; ■■ Reduced nutritional intake; ■■ Fatal disease process. While the prevalence of HCAIs in animals is unknown, we can assume it is similar to the level in people. It is imperative that measures are implemented to minimise the risks to the patient because the impact of an HCAI includes resistant pathogens, financial burden, a longer hospital stay and an increase in both morbidity and mortality. Elle Haskey, Queen Mother Hospital for Animals, Royal Veterinary College, Hawkshead Lane, North Mymms, Hertfordshire AL9 7TA, UK e-mail: [email protected] Many studies highlight that one of the most effective methods for reducing the transmission of pathogens between patients is effective hand hygiene. Veterinary clinics should have a hand hygiene policy that draws attention to: ■■ ■■ ■■ Hand care (actions that reduce skin irritation or damage); Hand decontamination (with both hand wash and alcohol hand rub); Surgical hand preparation; ■■ A ppropriate use of both sterile and nonsterile gloves. The WHO and Centers for Disease Control and Prevention (CDC) have both published guidelines on hand hygiene (CDC 2002, WHO 2009). The area around sinks should be kept fully stocked and clean at all times. Hand decontamination takes up to 60 seconds with a hand wash and only 20 seconds with an alcohol hand rub. Veterinary nurses should abide by the WHO (2011) recommendation of ‘five moments for hand hygiene’: ■■ Before touching a patient; ■■ Before a clean/aseptic procedure; ■■ A fter body fluid exposure risk; ■■ A fter touching a patient; ■■ A fter touching a patient’s surroundings. According to WHO (2013), adherence to hand hygiene policies is around 45 to 65 per cent, with reasons for poor compliance including inadequate staffing levels (too busy), forgetfulness, poor education and no role models. Audits should be carried out to highlight areas for further training to improve adherence and help reduce the risk to patients of HCAI. Managing tubes and lines Many critical patients will have multiple lines, tubes or drains in situ during the management of their disease. As mentioned previously, invasive devices increase the risk of an HCAI, so it is important to manage such devices appropriately and have policies in place so that all staff adhere to the same management protocol. Intravenous catheters Critical patients require venous access for the administration of fluid therapy, medications and blood products, which involves the placement of intravenous (IV) catheters. These tubes can also be used for haemodynamic monitoring and haemodialysis. A short, wide-bore catheter is often placed in a peripheral vein in the emergency situation Fig 1: Placement of a short-term, over-the-needle, peripheral intravenous catheter In Practice FOCUS November 2016 25-29 Haskey.indd 25 25 27/10/2016 16:32 Downloaded from http://inpractice.bmj.com/ on May 2, 2017 - Published by group.bmj.com carried out as per a shortterm catheter. There is no recommendation to change central venous catheters routinely. De-instrumenting should occur when the catheter is no longer required or a peripheral IV catheter can be placed as it is associated with a lower risk of complication (CDC 2011). Arterial catheters Fig 2: Triple lumen medial saphenous long-stay line in a cat for prompt access (Fig 1). These catheters are readily available, simple to place and cheap. Long-stay lines may be preferable in critical patients because they provide some additional benefits. They: ■■ ■■ Cause less thrombophlebitis (because they are made from materials that induce less reaction) (CDC 2011); Allow blood sampling; ■■ A llow multiple drugs to be administered at the same time through separate lumens; ■■ Allow central venous pressure monitoring. Arterial catheters are extremely useful in critical patients, allowing the monitoring of arterial Fig 3: Arterial line in the dorsopedal artery of a postoperative blood pressure and patient. The line was connected to a transducer for invasive blood pressure measurement. The tape is clearly labelled with the word sampling of arterial blood ‘arterial’ to prevent drugs being administered into the artery gas. The placement of arterial catheters takes practice and can be spillage onto the patient’s leg during the very difficult in conscious and small patients procedure should be cleaned as thoroughly as (particularly cats). They are placed and possible. managed in a similar manner to short-term Once placed, the catheter should be IV catheters, with the only difference being covered with a sterile dressing to keep it clean that they are prone to occlusion and should be and prevent patient interference. The dressing flushed with saline hourly; alternatively, there should be removed daily to assess the leg are systems for monitoring blood pressure that for signs of infection or inflammation. If the allow continuous flushing. catheter is not being used for IV fluids, it should Patients with arterial catheters should be flushed every four to eight hours. There is ideally be monitored closely because no evidence that heparinised saline is superior detachment of the bung can result in rapid to saline for maintaining catheter patency blood loss. The lines should be clearly labelled (Ueda and others 2013). There is, however, so that no drugs are administered into the evidence that catheter-related complications artery (Fig 3), and removed when no longer are associated with increased duration of required because they cause limb ischaemia in IV catheter placement (Seguela and Pages cats (Mazzaferro 2009, Bowlt and others 2013). 2011, Parkes 2015). It is therefore sensible to Tracheostomy tubes consider replacing IV catheters after 72 hours. Tracheostomy tubes (Fig 4) are used to bypass Long-stay lines should be placed aseptically the upper airway in patients with an airway with skin preparation as for the placement obstruction (eg, as a result of laryngeal of short-term catheters. A sterile dressing oedema, masses or trauma). Patients with should be applied over the insertion site once these tubes must be supervised constantly in situ. Transparent dressings are ideal as it because tube occlusion will cause asphyxiation. is possible to view the site without having to change the dressing each time. Alternatively, a sterile gauze dressing can be used. These lines should be checked daily in a sterile manner and observed for signs of infection or inflammation. Flushing should be The tubes are usually placed centrally (eg, in the jugular vein), but can also be placed in larger peripheral vessels (eg, medial/lateral saphenous vein) (Fig 2). Contraindications include coagulopathies; jugular placement should be avoided if there is a concern about increased intracranial pressure. There are several strategies that can reduce the risk of complication during the placement and management of IV catheters. Irrespective of the site for short-term catheter placement, hair should be removed with a wide clip to avoid contamination, and the skin then prepared with a skin disinfectant (ie, chlorhexidine) and alcohol before placement. Hand hygiene should be carried out by the person placing the catheter. Consumables should be prepared and contained on a clean surface (not Fig 4: Tracheostomy tubes. (a) Obturator, (b) closed lumen the floor) before starting inner cannula, (c) twist–lock lumen inner cannula, (d) cuffless the procedure. Any blood tracheostomy tube 26 Fig 5: Canine patient with a tracheostomy tube. The stay sutures aid placement In Practice FOCUS November 2016 25-29 Haskey.indd 26 27/10/2016 16:32 Downloaded from http://inpractice.bmj.com/ on May 2, 2017 - Published by group.bmj.com Fig 7: Closed suction drain in a dog with septic peritonitis Fig 6: Dog with a chest drain after a thoracotomy. There is a light dressing at the insertion site, a clamp and one-way valve to achieve occlusion, and a string vest to prevent interference A sterile replacement tube should be readily available at all times (preferably next to the patient’s kennel), together with a calculated dose of anaesthetic agent for an emergency situation. Patients should be preoxygenated for about two minutes before the tube is changed/ removed/suctioned. Tubes with inner cannulae are desirable as these enable easy cleaning. The inner cannula is removed by gently twisting to unlock it (with clean, washed hands and disposable gloves), placed under running water to remove debris/ secretions and then rinsed in sterile saline. If it is encrusted, special tracheostomy brushes can be used for cleaning. Do not use a bottle brush or cotton wool buds to clean the inside of the tube as this will lead to abrasions that allow debris and secretions to adhere to the surface. Tubes for smaller patients do not have inner cannulae because their presence would excessively reduce the inner lumen of the tube. Therefore, these types of tubes should be replaced every 24 hours after a period of preoxygenation (Fudge 2009). Nebulisation and humidification can help prevent the airway and secretions from drying, and can be carried out every four to eight hours. Suctioning of the airway is recommended in many texts and may be useful to remove excessive secretions. This should be performed with care as it may cause mucosal injury and actually increase secretion production. A sterile suction catheter is inserted into the tracheostomy tube in an aseptic manner with sterile gloves to the estimated level of the carina (tracheal bifurcation). The catheter width should be no more than 50 per cent of the width of the internal diameter of the inner cannula of the tracheostomy tube. A new sterile suction catheter should be used for each suctioning attempt. This procedure should be abandoned if the patient becomes distressed. When tracheostomy tubes are placed in cats, shredded paper should be used instead of normal cat litter due to the risk of inhalation through the tracheostomy tube. Harnesses should be used instead of neck leads for dogs. There should be stay sutures present around the tracheal rings dorsal and ventral to the tracheal incision, allowing rapid ‘opening’ of the tracheostomy site and replacement of the tube (Fig 5). Chest drains Thoracostomy tubes (chest tubes) are used to drain air or fluid from the pleural space and, as for animals with tracheostomy tubes, constant monitoring of patients with these tubes is required. Indications for chest drain placement include: ■■ ■■ ■■ Post-thoracotomy; Medical management of a pleural effusion (chylothorax or pyothorax); Pneumothorax (ongoing air leakage); ■■ T ension ■■ pneumothorax; Penetrating chest injury. All chest drains should be handled with strict asepsis due the increased risk of HCAI (Sigrist 2009). The drain insertion site should be dressed with a light sterile dressing and inspected twice daily for signs of infection, inflammation, migration or leakage. Patients should wear a vest made from a stretchy material (Surgifix) or T-shirt to protect the tube and prevent it from being accidentally removed, as well as an Elizabethan collar to prevent interference. All drains should be clamped and/or occluded with a three-way tap/one-way valve (Fig 6). The frequency of draining depends on the underlying disease process and severity. Continuous suction may be required in some circumstances, whereas intermittent draining is sufficient in others. When manual draining is performed, sterile gloves should be worn. All fluid or air produced should be recorded. If the patient is showing signs of respiratory distress, aspiration of the chest tube should be attempted. Drains should be removed when they are no longer required or when the volume of air or fluid produced is less than 2 ml/kg/24 hours (Sigrist 2009). Closed suction drains There are many different closed suction drains available. They are commonly used for abdominal drainage after a contaminated surgery (ie, septic peritonitis) but can also be placed in contaminated wounds or wounds with a large dead space. The skin insertion site should be separate from the surgical wound, should be dressed with a light sterile dressing and inspected in a sterile manner every 24 hours (or more frequently if the dressing is struck through). These drains are often bulky and need to be attached to the patient to allow mobility. This can be achieved using a couple of butterfly wings on the tubing attached to the skin, or tubular netting can be helpful (Fig 7). Drains should be emptied wearing sterile gloves and the frequency depends on the drain and its function. They should always be emptied if full or if negative pressure has been lost. As for chest drains, closed suction drains should be removed when they are no longer required or when the volume produced is less than 2 ml/kg/24 hours (Szabo and others 2011). Urethral catheters Indications for urethral catheterisation are to: ■■ Obtain a urine sample; ■■ P erform ■■ R elieve ■■ a radiographic contrast study; a urethral obstruction; Measure urine output; ■■ I mprove nursing care in a critical patient or after surgery to the lower urinary tract. Urethral catheters are sometimes placed intermittently but are more often indwelling and the duration of catheterisation will depend on the reason for placement. The catheters are made from a variety of materials with varying stiffness, tissue reactivity and minimisation of biofilm formation. Foley catheters are chosen for indwelling catheter placement because the balloon at the end of the catheter can be inflated to hold the catheter in place. Urinary tract infections (UTIs) are the most common HCAI in human hospitals. In the veterinary literature, Smarick (2009) reported that 10 to 52 per cent of cats and dogs develop UTIs. Prophylactic antibiosis is not recommended as this can lead to the growth In Practice FOCUS November 2016 25-29 Haskey.indd 27 27 27/10/2016 16:32 Downloaded from http://inpractice.bmj.com/ on May 2, 2017 - Published by group.bmj.com Fig 8: Urinary catheter with a closed collection system. The collection bag is double bagged to prevent contamination and is anchored to the patient’s leg to reduce tension on the urinary tract if the patient moves around of resistant bacteria (Ogeer-Gyles and others 2006). The best way to reduce the likelihood of a catheter-associated UTI is to follow good hygiene principles. The CDC has published guidelines for urinary catheter placement and management (CDC 2009). All urinary catheters should be placed in a sterile manner (including the use of sterile gloves), whether they are placed intermittently or indwelling. Hair should be clipped from the preputial/vulval area, with care taken not to cause trauma to the skin as this may increase the likelihood of an infection. The skin should be prepared with a chlorhexidine or iodine skin disinfectant. An appropriately sized catheter should be selected for the patient – larger catheters may cause increased irritation to the urinary tract, thus increasing the risk of infection. Lubrication of the catheter can prevent trauma to the urethra and aid placement. A closed urine collection system should be attached to any indwelling urinary catheter so that urine output can be quantified and the risk of a UTI is reduced (Ogeer-Gyles and others 2006, CDC 2009, Smarick 2009). In addition, a closed system increases patient comfort by preventing leakage and urine scald. Urinary catheters can be anchored to the patient’s tail or leg with tape to prevent constant pulling on the catheter and trauma to the bladder/urethra (Fig 8). There is no veterinary study describing the risk of UTI with/without cleaning the prepuce/ Fig 9: Faecal management system for a dog with parvovirus vulva while the patient is catheterised. However, there are recommendations to wipe the outside surface of the catheter (proximal to distal) with chlorhexidine swabs and to flush the prepuce/vulva at regular intervals (Smarick 2009). The collection bag should be kept below the level of the patient to prevent reflux and an unobstructed urine flow should be maintained at all times. Bags can be emptied as necessary by disinfecting the drainage port before/ after drainage to minimise the number of microorganisms entering the collection bag. Routine flushing of the urinary catheter is unnecessary and will increase the risk of infection (Hooton and others 2010) so should only be considered if there is an obstruction in flow and should be carried out in a sterile manner. Recumbent patient management Recumbent patients are at risk of developing pressure sores (decubital ulcers) and urine and faecal scalding. The placement of a urinary catheter may be contraindicated in some situations, so patients need to be managed carefully to reduce the risk of urine scald. Ideally, patients should be kept clean and dry at all times on bedding that wicks fluid away (eg, Vetbed). If a patient becomes soiled, a mild unmedicated shampoo should be used to cleanse the soiled areas; it is important that hair and skin are thoroughly dried. This can be hugely time consuming for veterinary staff as bathing may be required on a frequent basis until the patient is ambulatory. There is little evidence to support the use of petroleum jelly or zinc oxide cream for managing scald, Fig 10: Ocular care involves flushing the eyes with saline although cornstarch 28 powder can be a useful adjunct as it helps to dry the patient after bathing. A faecal management system can be considered for recumbent patients with profuse diarrhoea (Fig 9) (MILA International 2014). It is inserted into the rectum and inflated (similar to a Foley urinary catheter) with a built-in closed collection system. In my experience, it is well tolerated and a time-saving tool when caring for a recumbent patient with diarrhoea. Frequently moving a recumbent patient can help to minimise the risk of pressure sores developing. Ideally, the animal should be turned every two to four hours, with its front end propped up to allow both lungs to inflate. Foam wedges, pillows and duvets are useful for padding beds. A passive and active range of movement routines and massage can keep patients supple and promote blood/lymph flow. Hoists are useful for large patients so that they can be stood up and encouraged to walk without putting staff at risk of injury. Once patients are ambulatory, physiotherapy sessions can be extended to include sling walks, balancing exercises and even hydrotherapy. Ocular and oral care Many critical patients have reduced tear production and reduced blink. This predisposes to corneal ulcer formation and eye infections. Cats receiving high doses of analgesia such as ketamine should have their eyes lubricated to prevent drying and corneal ulcer formation (Plumb 2008). Ulceration can be avoided by applying sterile waterbased eye lubrication every two to four hours (Clare 2009). If it is suspected that a patient is developing a corneal injury, a fluorescein stain of the cornea should be performed. Eyes can be flushed with saline once to twice daily (Fig 10) and if there are concerns with regards to infection, topical antibiotics should be administered. Mechanically ventilated patients must also receive oral care. These patients may not be able to swallow and are at risk of developing pneumonia as a result of oral bacterial contamination of the lower airways. Hospitalacquired pneumonia is 20 times more likely to In Practice FOCUS November 2016 25-29 Haskey.indd 28 27/10/2016 16:32 Downloaded from http://inpractice.bmj.com/ on May 2, 2017 - Published by group.bmj.com occur in mechanically ventilated patients than others (Nakamura and Tompkins 2012). Oral care should be performed wearing gloves to minimise the transfer of bacteria onto the hands of the nurse. Suctioning of the mouth and pharynx may be beneficial if there are copious oral secretions but this may not be possible in conscious animals. Dilute chlorhexidine mouthwash (Corsodyl; GSK) (diluted 1:1) can be used to clean the mouth and wipe around the teeth, helping to reduce the bacterial load (Clare 2009). Care must be taken in neurologically impaired patients to prevent the nurse from being bitten. The tongue should always be kept inside the mouth to prevent it from drying or becoming swollen. ‘Big little things’ Nurses should work at creating a patient bond by providing ‘TLC’ and grooming. The area of the hospital where the critical patients are housed should be quiet, with minimal traffic. There should be the ability to dim lights to mimic day/night and allow periods of quiet time and rest. Sleep is an important medicine that is often forgotten in veterinary hospitals. Treatments should be appropriately grouped to allow periods of rest and avoid disturbing the patient unnecessarily. Noisy/stressed animals should have measures taken to help them settle and prevent them from upsetting others (eg, quiet music can sometimes help). It is amazing what can be achieved with anxious patients if you just take things slowly and talk to them. If there is time to bath/groom a patient or transport it outside on a trolley to get some fresh air this can help to motivate it to do a little more. In some situations, it can be beneficial to arrange owner visits, particularly in ‘depressed’ patients or perhaps those that are not eating. However, if this stresses the patient, it may be wise to avoid future visits. As nurses are often busy and stretched, the ‘big little things’ are lower on the priority list. Try to remember how you would want somebody to treat your pet if it was in the hospital. The critical cat Cats behave differently from dogs in the hospital environment; their response to disease processes is often different from their canine counterparts and being generally much smaller creates different challenges in their management for nurses. If there are some nurses within the team who have that magic cat-whispering talent, make sure they are used more for nursing feline patients. Other nurses who are less confident can then work alongside them to learn and improve their cat knowledge and handling skills. Provisions should be made to reduce stress in hospitalised feline patients. The International Society of Feline Medicine has published recommended guidelines on handling and nursing feline patients (Rodan and others 2011, Carney and others 2012). Summary Nursing critically ill patients can sometimes be overwhelming because there is so much to think about. Nursing frameworks (such as Kirby’s Rule of 20) can be useful to give direction and enhance efficacy and efficiency (Barton 2009). Policies and protocols can be developed to ensure there is consistency between staff members and to reduce the risk of HCAIs. It can also be demanding and frustrating, requiring input from the whole veterinary team. Clear communication and teamwork can lead to positive outcomes and patients making a recovery, which is hugely rewarding for all involved. I am happy to be contacted to discuss specific questions about aspects of critical care nursing related to the article. References BARTON, L. (2009) Daily assessment of the critically ill patient. In Small Animal Critical Care Medicine. Eds D. Silverstein, K. Hopper. Saunders Elsevier. pp 852-856 BOWLT, K., BORTOLAMI, E., HARLEY, R., MURISON, P. & WALLACE, A. (2013) Ischaemic distal limb necrosis and Klebsiella pneumoniae infection associated with arterial catheterisation in a cat. Journal of Feline Medicine and Surgery 15, 1165-1168 CARNEY, H. C., LITTLE, S., BROWNLEE-TOMASSE, D., HARVEY, A. M., MATTOX, E., ROBERTSON, S. & OTHERS (2012) AAFP and ISFM feline-friendly nursing care guidelines. Journal of Feline Medicine and Surgery 14, 337-349 CDC (2002) CDC guidelines for hand hygiene in health-care settings. www.cdc.gov/mmwr/PDF/rr/ rr5116.pdf. Accessed October 12, 2016 CDC (2009) CDC guideline for prevention of catheterassociated urinary tract infections 2009. www.cdc. gov/hicpac/pdf/CAUTI/CAUTIguideline2009final.pdf. Accessed October 12, 2016 CDC (2011) CDC Guidelines for the prevention of intravascular catheter- related infections. www.cdc. gov/hicpac/pdf/guidelines/bsi-guidelines-2011.pdf. Accessed October 27, 2016 CLARE, M. (2009) Care of the ventilator patient. In Small Animal Critical Care Medicine. Eds D. Silverstein, K. Hopper. Saunders Elsevier. pp 912-916 FUDGE, M. (2009) Tracheostomy. In Small Animal Critical Care Medicine. 1st edn. Eds D. Silverstein, K. Hopper. Saunders Elsevier. pp 75-77 HOOTON, T., BRADLEY, S., CARDENAS, D., COLGAN, R., GEERLINGS, S., RICE, J. & OTHERS (2010) Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 international clinical practice guidelines from the Infectious Diseases Society of America. Clinical Infectious Diseases 50, 625-663 MAZZAFERRO, E. (2009) Arterial catheterisation. In Small Animal Critical Care Medicine. 1st edn. Eds D. Silverstein, K. Hopper. Saunders Elsevier. pp 206-208 MILA INTERNATIONAL (2014) Medical instrumentation for animals. 2014 catalogue. www. milainternational.com/MILA_MEDIA/MilaCatalog. pdf. Accessed October 12, 2016 NAKAMURA, R. K. & TOMKINS, E. (2012) Nosocomial infections. Compendium on Continuing Education for the Practicing Veterinarian 34, E1-E11 OGEER-GYLES, J., MATHEWS, K. & BOERLIN, P. (2006) Nosocomial infections and antimicrobial resistance in critical care medicine. Journal of Veterinary Emergency and Critical Care 16, 1-18 PARKES, G. (2015) A clinical analysis of complications associated with peripheral intravenous catheter placement in cats and dogs. In Proceedings of the British Small Animal Veterinary Congress. Birmingham, UK, April 9 to 12, 2015 PLUMB, D. (2008) Ketamine. In Plumb’s Veterinary Drug Handbook. 6th edn. Blackwell. 513-517 RODAN, I., SUNDAHL, E., CARNEY, H., GAGNON, A. C., HEATH, S., LANDSBERG, G. & OTHERS (2011) Bacterial and fungal colonisation of peripheral intravenous catheters in dogs and cats. Journal of Small Animal Practice 52, 531-535 SEQUELA, J. & PAGES, J. P. (2011) Bacterial and fungal colonisation of peripheral intravenous catheters in dogs and cats. Journal of Small Animal Practice 52, 531-535 SIGRIST, N. E. (2009) Thoracostomy tube placement and drainage. In Small Animal Critical Care Medicine. Eds D. Silverstein, K. Hopper. Saunders Elsevier. pp 134-137 SMARICK, S. (2009) Urinary catheterization. In Small Animal Critical Care Medicine. Eds D. Silverstein, K. Hopper. Saunders Elsevier. pp 603-606 SZABO, S. D., JERMYN, K., NEEL, J. & MATHEWS, K. G. (2011) Evaluation of postceliotomy peritoneal drain fluid volume, cytology, and blood-to-peritoneal fluid lactate and glucose differences in normal dogs. Veterinary Surgery 40, 444-449 UEDA, Y., ODUNAYO, A. & MANN, F. A. (2013) Comparison of heparinised saline and 0.9% sodium chloride for maintaining peripheral intravenous catheter patency in dogs. Journal of Veterinary Emergency and Critical Care (San Antonio) 23, 517-522 WHO (2009) WHO guidelines on hand hygiene in health care first global patient safety challenge clean care is safer care. http://apps.who.int/iris/ bitstream/10665/44102/1/9789241597906_eng.pdf. Accessed October 12, 2016 WHO (2011) Report on the Burden of Endemic Health Care-Associated Infection Worldwide. www.who. int/gpsc/country_work/burden_hcai/en/. Accessed October 27, 2016 WHO (2013) Five moments for hand hygiene. www. who.int/gpsc/tools/Five_moments/en. Accessed October 27, 2016 doi: 10.1136/inp.i6051 Elle Haskey graduated from the University of Bristol in 2008 with an honours degree in veterinary nursing and practice administration. She worked in a mixed practice in the Midlands before returning to the University of Bristol as senior ICU nurse. She gained the AVECCT Veterinary Technician Specialist (Emergency and Critical Care)qualification in 2012, and, in 2013, moved to join the Royal Veterinary College ECC team where she is now head ECC nurse. In Practice FOCUS November 2016 25-29 Haskey.indd 29 29 27/10/2016 16:32 Downloaded from http://inpractice.bmj.com/ on May 2, 2017 - Published by group.bmj.com Nursing critically ill patients in the intensive care unit Elle Haskey In Practice 2016 38: 25-29 doi: 10.1136/inp.i6051 Updated information and services can be found at: http://inpractice.bmj.com/content/38/Suppl_4/25 These include: References Email alerting service This article cites 9 articles, 1 of which you can access for free at: http://inpractice.bmj.com/content/38/Suppl_4/25#BIBL Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/