Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
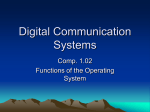
Design of an automated peripheral resistance Renske Hoeben BMTE 08.44 October 2008 Supervisor: dr.ir. M.C.M. Rutten 1. Abstract To evaluate the function and the assist properties of ventricular assist devices, a mock circulation, featuring the properties of the (diseased) heart and the systemic circulation may prove to be a valuable tool. The goal of this research was to expand a recently developed mock circulation system (MCS) with an automated total peripheral resistance and to remodel the corresponding circulation model accordingly. The circulation model only described the systemic circulation. It consisted of two parts: the controlling software and the MCS. The controlling software contained a contraction model to control the left ventricular pressure and baro- and cardiopulmonary reflex to regulate the heart rate and peripheral resistance. The MCS is the hydraulic hardware of the control loop consists of a left ventricle, preload, afterload and vessels. The heart model was switched from a healthy to a pathological heart to review the influence of the baro- and cardiopulmonary reflex and to determine if the resistance control functioned. Currently the link between hardware, software and control is in working order. There is a servomotor operated needle valve in place as the peripheral resistance and it responds to changes in aortic pressure by moving to a new position corresponding to the desired peripheral resistance. The idea is that eventually the circulation model, contraction model and the mock circulatory system will enable evaluation of LVADs and their role in heart function relief in terms of lowered left-ventricular pressure, lower cardiac output and possibly heart rate reduction. The conclusion of this research is that baroreflex and cardiopulmonary reflex are not very important regulation mechanisms of the peripheral resistance and it is therefore important to include cardiac output regulation (autoregulation and renal reflex functions) into the circulation model and mock circulatory system. Keywords: mock circulatory system, peripheral resistance, circulation model 2 2. Table of contents 1. Abstract ................................................................................................... 2 2. Table of contents..................................................................................... 3 3. Introduction.............................................................................................. 4 4. Materials and Methods ............................................................................ 8 4.1 The circulation model ..................................................................................8 4.1.1 The mock circulatory system ................................................................8 4.1.2 The controlling software........................................................................9 4.2 The adjustable resistance .........................................................................14 4.3 Measurement protocol...............................................................................17 5. Results .................................................................................................. 18 5.1 Simulation results ......................................................................................18 5.2 Experiment results.....................................................................................20 6. Discussion ............................................................................................. 23 7. Conclusion............................................................................................. 24 8. Future research ..................................................................................... 25 9. Appendices............................................................................................ 26 9.1 Resistance test measurement data .......................................................26 9.2 References ............................................................................................27 3 3. Introduction A ventricular assist device (VAD) is a mechanical pump that helps a weakened heart to pump blood through the body. VADs were originally intended for shortterm use to support a failing heart until a donor heart became available. Some VADs are now used for long-term therapy in severe heart failure patients who are not candidates for heart transplants. A VAD does not replace the heart. Instead, it works with the patient’s own heart to pump sufficient blood through the body. The VAD consists of a pump, a control system, and an energy supply. In a VAD, blood flows from the ventricles into a pump. A left ventricular assist device (LVAD) receives blood from the left ventricle and delivers it to the aorta. A right ventricular assist device (RVAD) receives blood from the right ventricle and delivers it to the pulmonary artery.1 Figure 1: An implanted LVAD 1 To evaluate the function and the assist properties of ventricular assist devices, a mock circulation, featuring the properties of the (diseased) heart and the systemic circulation may prove to be a valuable tool. The goal of this research was to expand a recently developed mock circulation model2 with an automated total peripheral resistance and to update the corresponding simulation model accordingly. An automated resistance is desirable because it is more accurate when the resistance can be regulated by aortic pressure and cardiac output instead of manually tuning it. The current model does not contain a regulated resistance. Therefore a literature research has been conducted to determine the relation between cardiac output, aortic pressure and the peripheral resistance. Adding the resistance has been accomplished by determining the mathematical relation between the resistance, pressure and flow in de systemic circulation and implementing that relationship in the existing simulation model. The resistance also needed to be added to the hydraulic model. Currently the model only comprises the systemic circulation; when that part is optimized and in working order the pulmonary circulation will be added. For the control of the mock circulatory system (MCS) a simulation model of the circulation was necessary. This model needed to contain the most important reflex loops which will regulate the pressure, heart rate, and the resistance. Many 4 circulatory models are available in literature (e.g. Guyton, Karaaslan) and the most appropriate one(s) have been selected (and combined). The ideal model accounts for all the desired behaviours with minimal complexity. Several cardiovascular circulation models have already been developed. Many of them are too elaborate for our purposes, because a model which could account for the entire spectrum of dynamical behaviours would describe many features that are irrelevant for LVAD function. The circulatory system has several feedback mechanisms that are responsible for acute and long-term control of arterial pressure, such as the baroreceptor reflex and renal body fluid feedback system. Not all of these mechanisms have been included in the model. The more important pressure regulatory mechanisms are3: 1. The baroreceptor reflex pressure regulating mechanism An increase in arterial pressure excites stress receptors in the carotid sinuses and the walls of large arteries. The resulting signals cause reflex decrease in cardiac activity and dilation of the peripheral blood vessels which in effect leads to a reduction of the cardiac output and the peripheral resistance. As a result the arterial pressure returns to normal. If the arterial pressure drops below normal this mechanism operates in reverse. 2. The chemoreceptor mechanism for arterial pressure regulation When the arterial pressure drops below reasonably low values the blood flow through to the carotid and aortic arteries decreases, causing an oxygen shortage and carbon dioxide accumulation. This is registered by the chemoreceptor cells in these arteries. The changes in saturations trigger the transmission of signals to the brain and circulatory system that lead to an increase in cardiac activity and peripheral resistance. In summary a decrease in arterial pressure elicits a chemoreceptor reflex that tends to increase the pressure back toward normal. 3. The central nervous system ischemic response When the arterial pressure drops below approximately 60 mmHg the vasomotor centre (an area in the brain) becomes directly excited probably because the blood flow becomes too small to remove all carbon dioxide generated by the brain tissue. In response powerful signals are sent to the circulatory system (through autonomic nerves) to increase cardiac activity and the peripheral resistance, thereby regulating the arterial pressure back toward normal. 4. Stress-relaxation of the circulation An elevated pressure will cause the vessels to stretch almost immediately due to their elastic characteristics. When the pressure remains elevated the vessels will stretch extra over time, this will reduce the peripheral resistance. Consequently the pressure in the circulation will tend to return to their original value. 5 5. Transfer of fluid through the capillary membranes In some conditions the increase in arterial pressure simultaneously causes an increase in capillary pressure. When this happens fluid filters from the circulation into the interstitial spaces (edema), causing a reduction in blood volume. In turn this reduces the overall flow through the circulation and thereby returns the arterial pressure back toward normal. 6. The renin-angiotensin-vasoconstrictor system When the arterial pressure drops below normal the kidneys start to secrete a substance called renin. This triggers a pathway that eventually causes constriction of the peripheral vessels and thus increases peripheral resistance. The net effect is an increase in arterial pressure back tot normal. 7. The renal-body fluid feedback pressure control system When the arterial pressure rises above normal the rate of loss of salt and water in urine increases rapidly. This causes a decrease in blood volume, filling pressure of the circulation, venous return and cardiac output. The reduction of cardiac output reduces the arterial pressure back toward normal. When the arterial pressure drops below normal the mechanism operates in reverse. The regulation of arterial pressure occurs at different time scales. Some pressure mechanisms are able to act extremely rapidly (the nervous mechanisms, baro-, chemoreceptors and central nervous ischemic response), at intermediate time intervals (stress-relaxation, fluid transfer and renin-angiotensin vasoconstriction) or over extremely long time periods (renal-body fluid feedback). When more blood than required flows through a tissue the local resistance to blood flow increases progressively until the blood flow returns toward normal. Part of the autoregulation reaction occurs in less than a minute; however, in most parts of the body a longer period of time is necessary (typically 30 minutes). The peripheral vascular resistance is influenced by autoregulation (baroreflex, vasoconstriction and renal autoregulation) and depends on the aortic pressure and cardiac output. In order to regulate the resistance a model was needed that describes the relation between baroreflex, vasoconstriction, renal autoregulation and the peripheral resistance. At a later stage more parameters will be added. The model then needs to be valid for short- mid- and long-term regulation. The model of Guyton3 was used as a basis for many of the models available in literature. This is a very extensive model. It contains all the regulatory mechanisms and it describes short term and long term effects. The model has been experimentally validated. Due to its completeness it also becomes a complex model. The autoregulation mechanism is less important in short-term than the baroreflex; however, after a while the autoregulation gain starts to increase and becomes dominant. In most models the peripheral resistance is described as the sum of a baroreflex, autoregulation and a noise element. However, in Guyton’s model the baroreflex and autoregulation are multiplied. 6 Due to the complexity of Guyton’s model it is difficult to isolate and use just a small part. A more recent study by Karaaslan4 combined Guyton’s model with a few other studies. The model proposed in his study focused on the long-term renal influence on the circulation. All the mathematical relations are described extensively. When the research reaches the stage where the kidneys and bladder will be added to the MCS this model could provide a basis for the simulation model. It described the total peripheral resistance as the sum of the arterial resistance and a constant basic venous resistance. The described arterial resistance depends on the mean arterial pressure and cardiac output. In long term the kidneys become the dominant influence on the resistance over the baroreflex. Therefore the model contains baroreflex saturation. Aljuri5 developed a model describing the changes in total peripheral resistance due to baroreflex and autoregulation. This relation depends on the aortic pressure and cardiac output. The model has been experimentally validated and seems to mimic short-term behaviour quite well. This model seems to satisfy our needs, as it completely describes the mathematical relations between cardiac output, aortic pressure and total peripheral resistance. Regrettably the coefficients of the model have not been documented and the author has refused to answer any questions regarding these coefficients. The model previously used in this research has been developed by Wesseling and edited by van Roon6. This model was developed to study short-term cardiovascular effects of mental workload. An advantage of this model is that all mathematical equations, their parameters and their sources have been extensively documented. Unfortunately this model is only suitable for short-term studies. Despite the limitations of van Roon’s model it has remained the basis for the simulations, because a better model was lacking. The baroreflex saturation, vasoconstriction influenced by the cardiac output and eventually renal autoregulation need to be added to this model afterwards. 7 4. Materials and Methods The previous circulation model had a fixed peripheral resistance. For this research an adjustable resistance needed to be designed and tested before implementation into the MCS. The simulation model has been used to determine the expected response patterns of e.g. aortic pressure and cardiac output. At a later stage the simulation model processed the measurements from the MCS. 4.1 The circulation model The circulation model had two main parts: the MCS and the controlling software. 4.1.1 The mock circulatory system The mock circulatory system used in this study (figure 2) only described the systemic circulation. The hydraulic hardware of the control loop consisted7 of a servomotor operated piston pump acting as the left ventricle (linear servoactuator type ETB32, Parker Hamilton, Oldenzaal, the Netherlands). The afterload consisted of a flexible tube and a four element windkessel. A compliance chamber between the peripheral resistance and the mitral valve served as the preload. The left ventricle also included two tri-leaflet polyurethane valves (Hemolab, Eindhoven, the Netherlands). The hydraulic system generated the left ventricular volume Vlv. This was transformed into the corresponding left ventricular pressure Plv by the heart model. The pressure error was fed into the controller, which adjusted the left ventricular contraction/relaxation velocity accordingly. The systemic pressure, as measured in the hydraulic system, controlled the heart rate by the reflex functions. In the setup the left ventricular pressure (Plv), aortic flow (qao) and aortic pressure (Pao) were constantly measured. (flowmeter PAX28A Transonic Systems Maastricht the Netherlands, pressure sensors P10EZ, Becton Dickinson Belgium) Figure 2: Experiment set-up 8 4.1.2 The controlling software The controlling system was the simulation model developed by Vaes2 extended with the cardiopulmonary control of the peripheral resistance by van Roon6 and appended to this is the position control of the automated resistance. The heart model is based on the master thesis of Cox8. The current model describes the baroreflex and cardiopulmonary reflex. These reflex loops describe the mechanisms that regulate the peripheral resistance and heart rate. An increase in arterial pressure excites the baroreceptors (stretch receptors) in the wall of the aortic arch and carotid arteries. The resulting signals are sent to brain stem structures, where they are further processed with the result of vagal and sympathetic efferents adjusting the various effector systems involved in blood pressure control. The most important vagally controlled effector is heart rate and it often dominates sympathetic influences on heart rate. The sympathetic effectors influence the peripheral resistance. An increase in pressure sensed by the baroreceptors, causes reflex decrease in cardiac activity and reflex dilatation of the peripheral blood vessels, which causes a decrease in cardiac output (CO) and peripheral resistance. A decrease in pressure causes the opposite3. The activation of cardiopulmonary receptors is directly related to changes in venous pressure. In response they influence the heart rate and systemic pressure the same way as the baroreceptors.9 The peripheral resistance is mainly controlled by the small arteries. A change in perfusion pressure causes a change in vascular tone, ensuring a constant blood flow5. As stated above the resistance responds to stimulation from the baroreceptors and cardiopulmonary receptor. An increase in cardiac output precedes an increase in peripheral resistance, due to vasoconstriction mechanisms.10 No relevant literature has been found that contains a mathematical description of autoregulatory control by the cardiac output. Therefore the resistance will only be controlled by cardiopulmonary and baroreflex at this stage. The mathematical description of the set-up was divided into three parts: the hemodynamic preload, afterload and the piston pump and the heart valves. The preload and afterload were described by a lumped parameter model11. The piston pump was described as a mass with friction. The aortic and mitral valves were described as short tubes in which flow was dominated by inertia and pressure drop. A schematic representation of the setup is shown in figure 3. Combination of pump, piston and hemodynamic preload and afterload results in a seventh order system of differential equations which are implemented in the driver. An extensive description can be found in the report of Vaes2. 9 Figure 3: Schematic representation of the systemic circulation The simulation model consists of four components: the heart model, heart model driver, controller and regulation model. The simulation model was implemented in Matlab 7.2 Simulink. See figures 4 and 5. Regulation model Figure 4: The control model • Heart model The heart model regulates the contraction of the heart muscle. The model is based on the master’s thesis of Lieke Cox8. The heart model in this study is based on the model by Bovendeerd12. It consists of four parts, describing ventricular wall mechanics, myocardial constitutive properties, intramyocardial pressure and the circulation. The model of the ventricular wall mechanics describes how left ventricular pressure and volume are related to local tissue properties, i.e. fiber stress and strain, and radial wall stress and strain. Bovendeerd et al. modeled the left ventricle as a thick walled sphere, consisting of a set of nested thin spherical shells. On the basis of earlier studies they concluded that in the normal left ventricle, muscle fiber stress and strain are homogeneously distributed, so that they may be approximated by single values. Furthermore they found that, when assuming rotational symmetry and homogeneity of mechanical load in the wall, the dimensionless ratio of muscle fiber stress to left ventricular 10 pressure depends mainly on the dimensionless ratio of cavity volume to wall volume. In the model, left ventricular pressure is given by: Plv = V 1 (σ f − 2σ m,v )ln(1 + w ) 3 Vlv Plv = left ventricular pressure Vw = wall volume σ f = fiber stress σ m,v = radial wall stress Vlv = cavity volume The muscle fiber stress is a time-dependent function of the active (σa, with contraction) and passive (σm,f, without contraction) stresses in the fiber. σ f = σ a + σ m.f σ a (c, l s , t a ,v s ) = cσ ar f (l s )g (ta )h(v s ) 0 f (l s ) ls − ls ,a 0 l − l s ,ar s ,a 0 0 t g (ta ) sin2 (π a ) tmax 0 v 1− ( s ) v0 h(v s ) = v 1 + cv s v0 for ls ≤ ls ,a 0 for l s > l s,a 0 for t a < 0 for 0 ≤ t a ≤ tmax for t a > tmax c = contractility cv = governs the shape of the stress-velocity relation σ ar = reference stress ls = sarcomere length ls ,a 0 = sarcomere length below which active stress becomes zero ls ,ar = sarcomere length to which the reference stress is referred to ta = time elapsed since activation tmax = duration of twitch v s = sarcomere shortening velocity v 0 = unloaded sarcomere shortening velocity The heart model can switch from a healthy to a pathological heart. When the heart is in a state of decompensation the contractility (c) diminishes, while the wall volume (Vw) and cavity volume (Vlv) increase. 11 • • • Driver During the simulation this block contains all the differential equations necessary to calculate several variables e.g. cardiac output and pressure in the aorta2. During the experiments the data from the model is fed through this driver, which then contains all the hardware, so the measured flow and pressure data are the output. The driver will also regulate the movement of the resistance. Controller The controller ensures that the prescribed pressure is maintained. During the simulation the gain sometimes needed to be tuned. This is due to the modelling choice of the heart valves; they open and after a while close instantly. This is not very realistic and sometimes causes spurious oscillations. During the experiment this tuning was not necessary. The controller also contains the controller signal of the actuator. Regulation model This block contains all the reflex loops effecting the peripheral resistance and heart rate. All the reflex loops are shown in detail in figure 4. The reflex loops have been copied from the model by van Roon6,9, and describe the baroreflex and cardiopulmonary reflex. The only new components are a few unit conversions and the calculation of the position. The calculated resistance will be converted to a position using the derived characteristic of the needle valve. In the future the cardiac output control of the resistance will be added here. During normal respiration the heart rate increases during inspiration and decreases during expiration. The respiration influences the vagal part of the heart rate control and the thoracic pressure changes as well. This influences the pressure experienced by the baroreceptors. It is not always convenient to have breathing noise in the signal therefore there it is possible to choose a constant signal. Throughout this study the constant signal was used. 12 Figure 5: the reflex loops 13 4.2 The adjustable resistance The peripheral resistance in the previous MCS needed to be tuned manually. To make the model more accurate the resistance must respond to a change in pressure and/or cardiac output automatically. Therefore the simulation model has been expanded with reflex loops influencing the peripheral resistance (baroreflex and cardiopulmonary reflex). In the MCS the existing resistance was replaced by an automated resistance. The location of the adjustable resistance in the MCS can be seen in figure 2.The resistance was designed as a servomotor operated needle valve. The resistance can be moved to block or unblock the tube, simulating vasoconstriction or – dilation. The linear actuator provides a horizontal motion of maximum 25 mm (type M230.25, Physik Instrumente, Karlsruhe, Germany). Figure 6: schematic of the adjustable resistance The resistance has been designed to fit into a windkessel setup. This windkessel served as the afterload in the MCS. The resistance needed to be tested to ensure it is watertight and to determine a relation between measured flow, pressure and the position of the resistance. This relation has been implemented into the controlling software and will be the driver of the resistance. See figure 4, the positioner (orange) contains the relation between resistance and position. The relation between the peripheral resistance and the position of the adjustable resistance has been determined by measuring the flow and the pressure at different settings of the resistance. The characterization is conducted in stationary flow conditions; therefore the compliance of the windkessel is irrelevant at this stage. The flow was measured using a flowmeter (type ME25PXN, transonic systems Maastricht Netherlands) and the pressure was is determined using pressure sensors (P10EZ, Becton Dickinson Belgium). The test set-up is shown in figure 7. The resistance was measured in stationary flow conditions, therefore the following equation holds: R= ∆P Q With R the resistance, ∆P pressure drop and Q the flow rate. (1) Figure 7: schematic of the resistance test set-up In order to determine whether or not the resistance was flow dependent the measurements have been conducted with three different flow values. All measurements were repeated twice and the mean value was used as input. The expected relation between the position and the resistance is a hyperbolic function. When the opening is shut the resistance becomes infinite and beyond a certain position the resistance will not decrease anymore. This relation will be implemented in the simulation model. c +b (2) resistance = position − a The constants will be determined by fitting this hyperbolic function on the data. Since the same windkessel set-up will be used in the MCS the equation should also be valid there. During a steady flow the resistance has been moved to several positions and the flow and pressure corresponding to this position were noted. Using the pressure and flow the resistance was calculated, equation 1. The resistance was plotted against the position. The measurements were conducted for three different steady flows. Finally a hyperbolic function has been fit through the data, equation 2. (Matlab curve fitting toolbox) In figure 8 you can see the results of the test. 15 Figure 8: results of the measurements and in red the hyperbolic fit to the experimental data. The resistance between 4 and 8 mm is the most important and most sensitive. Therefore this section has been used to fit a hyperbolic function to. The equation c + b , with a=3.3 mm, for the hyperbolic function is: resistance = position − a b=-1.5e7 Pa s m-3 and c=3.9e8 Pa s m-4. This derived function was implemented into the circulation model. All the raw measurement data can be found in Appendix 9.1. 16 4.3 Measurement protocol In order to evaluate the functioning of the circulation model four different situations have been tested. 1. 2. 3. 4. no regulation: heart rate and peripheral resistance constant regulation: heart rate and peripheral resistance were regulated regulated heart rate and constant peripheral resistance constant heart rate and regulated peripheral resistance To review the function of the reflex loops halfway during the measurement the heart was switched from healthy to pathological. For a pathological heart the contractility and cavity volume diminish and the wall volume increases. The contractility becomes .55 instead of 1, wall volume 200e-6→225e-6 m3 and cavity volume 0.4*→0.3*wall volume. For the simulations the assigned constant value for the heart rate (hr) was 1.16 Hz and for the peripheral resistance (pr) 1.37e8 Pa s m-3. These values are the resting values for a healthy heart and have been derived from a simulation with hr and pr regulation. After 70s the heart model was switched to a pathological heart. The ‘healthy’ part of the simulations is the same due to the choice in constants, but the ‘pathological’ part demonstrates the effect of the resistance and heart rate regulation. For the experiment the constant value for the heart rate was 1.25 Hz and for the peripheral resistance 1.5e8 Pa s m-3. These values differ from the ones used in the simulation; this will be explained in the discussion. The preload at the beginning of the experiment is marked on the windkessel and kept constant during the four experiments. The preload for the pathological heart is higher than that of the healthy heart. During the simulations and the experiment the following variables were recorded: time, left-ventricular pressure (Plv), aortic pressure (Pao), heart rate (hr), cardiac output (CO), peripheral resistance (pr) and left ventricular volume (Plv). Pressure-volume loops have been constructed from the Vlv and Plv. 17 5. Results 5.1 Simulation results The first 20 seconds of the simulation the model experiences transient effects because the heart rate commences at zero. This causes a very low pressure and an overshoot in the resistance. After an off-set of about 20 seconds the peripheral resistance, pump and aortic pressure and the heart rate frequency stabilize. During the first part of the simulations (for a healthy heart and with heart rate and peripheral resistance regulation) the resting values are: - the peripheral resistance is 1.37e8 Pa s m-3 - the aortic pressure is 120 above 83 mmHg - the cardiac output is 5.8e-5 m3/s - the heart rate is 1.16 Hz These values correspond to the resting values of a healthy person described in literature13. Figure 9: Overview of the pressures and cardiac output and results of all four simulations for the heart rate and peripheral resistance. The overviews are from the simulation with heart rate and peripheral resistance regulation. Figure 8 clearly demonstrates the transition from a healthy to a pathological heart and the drop in pressure and cardiac output that is the result. Figure 9 contains a close up of two periods of the aortic pressure and cardiac output in the healthy and pathological case. For cardiac output the difference between regulation or not is .41e-5 m3/s (2.46e-1 L/min) and for the aortic pressure the difference between regulation or not is 2.7 mmHg. Figure 9 indicates the effect of the heart rate regulation, the period between heart beats becomes shorter. In the pathological case the heart rate increases from 1.16 to 1.4 Hz. The resistance increases from 1.37e8 to 1.56e8Pa s m-3. Table 2: results of the simulation simulation hf and pr constant hf and pr regulation hf regulation and pr constant hf constant and pr regulation cardiac output healthy pathological 3 3 [m /s] [m /s] 5.83e-5 3.29e-5 5.80e-5 2.88e-5 5.83e-5 3.24e-5 5.80e-5 3.04e-5 average aortic pressure healthy pathological [mmHg] [mmHg] 94.2 61.8 94.2 64.5 94.3 62.8 94.3 63.4 Figure 10 contains the pressure volume loops of the left ventricle. The pathological heart has a diminished stroke volume and lower afterload. Again there is not much deviation between the four simulations. Figure 10: pressure volume loops for a healthy (left) and pathological heart (right) Red: hr and pr regulation Purple: hr regulation and pr constant Blue: hr and pr constant Green: hr constant and pr regulation 19 5.2 Experiment results Figure 11 shows the desired peripheral resistance position and the position the resistance was sent to. It shows that the control is sufficiently accurate. Figure 11 contains the results of an experiment with heart rate and peripheral resistance regulation. When there are abrupt changes in the resistance the control mechanism experiences an overshoot which could lead to the actuator getting stuck. Therefore the regulation mechanism still needs to be fine-tuned. Figure 11: position regulation For the experiment the resting values of the heart rate and peripheral resistance differ from those in the previous simulations. The constant value used for the heart rate was 1.25 Hz and for the peripheral resistance 1.5e8 Pa s m-3. These chosen constant values turn out to be closer to the values of the pathological heart. The choice of these constant was based on previous simulations with a different contraction model. Table 3: results of the experiment hr and pr heart rate healthy [Hz] hf and pr regulation 0.96 hf regulation and pr constant 0.88 hf constant and pr regulation - pathological [Hz] 1.29 1.31 - peripheral resistance healthy pathological -3 -3 [Pa s m ] [Pa s m ] 1.24e8 1.6e8 1.22e8 1.6e8 Table 4: results of the experiment CO an Pao cardiac output healthy pathological 3 3 [m /s] [m /s] hf and pr constant 3.82e-5 2.68e-5 hf and pr regulation 5.00e-5 2.52e-5 hf regulation and pr constant 4.13e-5 2.70e-5 hf constant and pr regulation 5.00e-5 2.57e-5 average aortic pressure healthy pathological [mmHg] [mmHg] 105.6 53.1 94.8 55.5 101.0 53.4 96.8 56.0 As can be deduced from table 4, the same transition from a healthy to a pathological heart occurs in the experiments and again a drop in pressure and cardiac output is the result. For the cardiac output the difference between regulation or not is for a healthy heart 1.18e-5 m3/s (7.8e-1 L/min) and for a pathological heart 0.16e-5 m3/s (9.6e2 L/min). The aortic pressure difference between regulation or not is 10.8 mmHg when the heart is healthy and 2.3 mmHg for the pathological heart. In the case of the experiment the pathological measurements are identical and the healthy ones show a slight difference. In figure 12 you can see that the heart rate differs when regulated or not. But again there are no large deviations between the four situations. aortic pressure pathological cardiac output pathological Figure 12: results for aortic pressure and cardiac output of the experiments 21 The pressure volume loops of the experiment are given in figure 13. Figure 13: pressure volume loops for a healthy (left) and pathological heart (right) Red: hr and pr regulation Blue: hr and pr constant Purple: hr regulation and pr constant Green: hr constant and pr regulation The pv-loops of the simulations and experiment cannot be compared quantitatively due to a different choice in constants. Again the four situations are quite similar. 22 6. Discussion The developed mock circulation features a heart model capable of adapting its contractile behaviour as a function of time, left-ventricular volume and ejection rate. There is no cardiac output regulation yet and it comes as no surprise that there is little deviation between regulation or not. In reality it is more important to keep the cardiac output constant. The baroreflex and cardiopulmonary sensors do not have a very large influence on the peripheral resistance. Since the model by van Roon6 does not contain vasoconstriction (the autoregulation influenced by the cardiac output) and is only valid in the short-term, it is probably better to take a different model as a basis. During this research there was no time to develop a new and better model and that task is going to be the next stage of this project. This circulatory system describes only the left part of the heart. Therefore, the flow from the afterload is directly returned to the left-ventricular preload, which may lead to a too strong coupling between afterload and preload. A higher systemic pressure will yield more liquid storage in the afterload, so, because of the constant amount of liquid in the circulation, automatically the preload will be lowered, hence reducing the level of filling and thus the cardiac output14. Normally when a heart is in state of decompensation the preload starts to rise, due to the coupling of preload and afterload that is now not the case. When the pulmonary circulation is added these problems should be solved. The automated peripheral resistance does not appear to be flow dependant. When examining figure 7 the resistance at the lower positions varies more than for the other positions. This difference can be explained by the spring in the resistance. It is possible that at higher flows the spring in the resistance gets compressed creating a larger opening than intended. This might explain the difference between resistance values for the flow of 4 L/min and 1.7 L/min. The constants used in the experiment differ from those used in the simulations. That is because after the experiments were conducted the contraction model of the simulations was switched to the one used in the experimental model and all the simulations were repeated. Unfortunately there was not enough time to redo the experiments with the new resting values. The fact that the choice of constants during the experiment is not optimal is unfortunate but does not alter the end conclusion. The results from the simulations and experiment show that the baroreflex and cardiopulmonary reflex contribution to cardiac output and aortic pressure is minimal. In the pv-loops of figure 13 an effect of using the wrong constant value for the heart rate is visible. In the case of no regulation there is a lower stroke volume, this is because the chosen constant heart rate resembled the value of a pathological heart. 23 7. Conclusion The goal of this research was to expand a recently developed mock circulation model2 with an automated total peripheral resistance and to update the corresponding simulation model accordingly. That part has been accomplished. There is a servomotor operated needle valve in place as the peripheral resistance and it responds to changes in aortic pressure by moving to a new position corresponding to the desired peripheral resistance. The link between hardware, software and control is in working order. The idea is that eventually the circulation model, contraction model and the mock circulatory system will enable evaluation of LVADs and their role in heart function relief in terms of lowered leftventricular pressure, lower cardiac output and possibly heart rate reduction7. As for now, the conclusion of this project is that baroreflex and cardiopulmonary reflex are not very important regulation mechanisms of the peripheral resistance and it is therefore important to include cardiac output regulation (autoregulation and renal reflex functions) into the circulation model and mock circulatory system. 24 8. Future research Recommendations for further research: o Including autoregulation and renal reflex functions to the circulatory model. Either by extending the current model or by choosing a different model as basis. Preferably a model that can deal with short-, mid- and long term reflex mechanisms. o Fine tuning the resistance control mechanism, as it is sensitive to overshoot. o Extending to model as to describe the entire circulation (systemic and pulmonary). o Improving the modelling choice of the valves. Currently they open and after a while close instantly. This is not very realistic and sometimes causes spurious oscillations. 25 9. Appendices 9.1 Resistance test measurement data Table 5: measurement data of the resistance test pump setting [L/min] 1.7 L/min 3 L/min 4 L/min position [mm] 4.5 5 5.5 6 7 8 10 14 18 4 4.3 4.5 4.7 4.8 5 5.1 5.3 5.5 5.6 5.7 5.8 6 6.5 7 7.5 8 8.5 10 12 14 16 4.5 5 5.5 6 7 8 10 14 18 flow [L/min] 1.50 1.46 1.53 1.50 1.61 1.68 1.61 1.60 1.60 1.60 1.64 1.61 1.65 1.68 1.60 1.70 1.63 1.70 2.83 2.81 2.73 2.82 2.66 2.66 2.66 2.76 2.88 2.81 2.92 2.81 2.72 2.69 2.82 2.89 2.79 2.83 2.80 2.76 2.83 2.73 2.79 2.78 2.77 2.96 2.83 2.82 2.93 2.76 2.66 2.76 2.80 3.04 2.73 2.72 2.83 3.06 3.11 3.01 3.19 3.01 3.15 2.96 3.85 8.82 3.83 3.87 3.84 3.88 3.83 3.82 3.84 3.83 3.87 3.87 3.9 3.88 3.77 3.83 3.84 3.85 2.86 2.80 2.76 2.86 2.76 2.76 2.82 2.86 2.76 2.96 2.96 2.96 3.86 - ∆p [mmHg] 71.8 68.2 54.1 57.3 33.6 33.7 18.9 19.0 7.9 7.9 4.0 3.9 0.8 0.8 0.0 0.1 0.1 0.1 114.0 98.5 105.9 104.3 94.2 98.2 90.6 88.8 88.4 88.5 67.6 63.5 73.5 76.6 67.1 69.8 64.0 77.7 55.6 56.0 56.1 55.7 49.7 50.5 50.3 42.2 31.3 31.1 21.9 22 16.4 16.7 13.31 13.4 10.0 10.1 3.6 3.9 0.4 0.8 0.0 0.2 0.0 0.1 134.5 145.4 112.4 115.2 78.7 92.3 61.8 66.6 46.5 46.4 25.4 25.5 8.6 8.5 0.2 0.2 0.2 0.2 108 67.4 73.2 37.2 31.2 21.8 16.6 13.6 10.2 4.0 0.9 0.3 87.1 - 26 9.2 References 1 FDA heart health online, http://www.fda.gov/hearthealth/treatments/medicaldevices/vad.html, th accessed 18 of February 2008 2 Model based control of a mock circulatory system for left ventricular assist device evaluation, M. Vaes et al, 37, DCT 2007.085, Internal Report (2007) University of technology Eindhoven 3 Systems analysis of arterial pressure regulation and hypertension, A.C. Guyton et al, annals of biomedical engineering 1, 254-281,1972 4 Long-term mathematical model involving renal sympathetic nerve activity, arterial pressure and sodium excretion, F. Karaaslan et al, Annals of biomedical engineering, vol 33 no 11, November 2005, pp 1607-1630 5 Theoretical considerations in the dynamic closed-loop baroreflex and autoregulatory control of total peripheral resistance, N. Aljuri et al, Am J physiol heart circ physio 287: H2252-H2273, 2004 6 Short-term cardiovascular effects of mental tasks, physiology, experiments and computer simulations, M. van Roon, thesis available at the rijksuniversiteit Groningen, doctoraat van Psychologische, Pedagogische en sociale wetenschappen 7 Left-ventricular assist device evaluation with a model controlled mock circulation, M. Vaes, M. Rutten et al, SBC2007-176372, Proceedings of the ASME 2007 Summer Bioengineering Conference (SBC2007) June 20-24, Keystone Resort & Conference Center, Keystone, Colorado, USA 8 A method for optimizing hemodynamics during mechanical cardiac support, L. Cox, MSc Thesis, University of Technology Eindhoven, March 2007, BMTE 07.10 9 Introducing a baroreflex model for studying cardiovascular effects of mental workload, A.M. van Roon et al, psychophysiology, 41 (2004) 961-981, Blackwell publishing inc. 10 Whole body circulatory autoregulation and hypertension, T.G. Coleman, Supplement II to Circulation Research, Vols. XXVIII md XXIX, May 1971 11 Total arterial inertance as the fourth element of the windkessel model, N Stergiopulos, et al, Am J Physiol 276:81-88, 1999 12 Dependence of Intramyocardial Pressure and Coronary Flow on Ventricular Loading and Contractility: A Model Study, P.H.M. Bovendeerd et al, Ann Biomed Eng, volume 34, nr 12 p18331845, 2006 13 Metabolic and Cardiovascular Assessment in Moderate Obesity: Effect of Weight Loss, Elza Muscelli et al, the Journal of Clinical Endocrinology & Metabolism Vol. 82, No. 9 2937-2943 27