Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
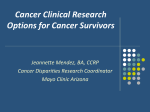
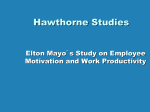
NeurosciencesUpdate Neurologic Surgery and Clinical Neurology News INSIDE THIS ISSUE Surgery and ICU: 3 4 6 Sports-Related Concussion: Managing Long-Term Effects Although repeated concussive head trauma is a purported risk factor for later neurodegenerative disease, the problem is far from fully elucidated. “Some, but certainly not all, people with repeated concussion develop neurodegenerative problems later in life. But does the risk increase a little bit or Autoimmune a lot?”says Bradley F. Boeve, M.D., a consultant in Dementia: Defining Neurology at Mayo Clinic in Rochester, Minnesota. a Treatable Disorder At the severe end of the spectrum of possible effects is chronic traumatic encephalopathy (CTE), experienced by a minority of athletes (Figure 1). DBS for OCD and Other athletes might have long-term cognitive or Tourette Syndrome neuropsychological problems (Figure 2), but the timing and mechanism of symptom onset and specific risk factors that might predispose individuals with sports-related concussion (SRC) to develop neurodegenerative disease aren’t clear. Mayo Clinic devotes considerable clinical and research expertise across multiple specialties to athletes with concussive injuries, from peewee to professional leagues. The goal is to relieve patient symptoms, uncover risk factors for long-term effects of SRC and make evidence-based recommendations for increasing the safety of sports. “We have an integrated system of expertise, with a common will and drive to improve the care of people with concussive injuries and their ability to function later in their lives,”says Rodolfo Savica, M.D., Ph.D., a consultant in Neurology at Mayo Clinic’s campus in Minnesota. Figure 1. Photomicrograph of tau-immunoreactive Patients have comprehensive lesions (stained brown) in a former professional U.S. football player. Image provided by Dennis W. Dickson, evaluations from consultants M.D., and Kevin F. Bieniek, Mayo Clinic. in behavioral neurology, brain Collaborating for the Best Outcomes Vol. 12, No. 4, 2015 rehabilitation and neuropsychology, headache neurology, and sports medicine.“Even if we find no definitive evidence of neurodegenerative disease, our role as clinicians is to treat the patient’s symptoms,”says Allen W. Brown, M.D., division chair of Brain Rehabilitation at Mayo Clinic’s campus in Minnesota.“It’s very common for us to see individuals who have had sports-related concussive injuries and are experiencing many symptoms unrelated to brain dysfunction.” Large population at risk It’s generally accepted that among people who experience symptoms from concussion, approximately 70 to 80 percent are no longer experiencing them two weeks later.“But that leaves 1 in 5 people who don’t recover within seven to 10 days. That’s a huge population at risk,”says David W. Dodick, M.D., a consultant in Neurology at Mayo Clinic in Phoenix/Scottsdale, Arizona.“The accepted number of sports-related concussions is on the order of 3.5 million to 4 million in the United States each year. I would say it’s at least double that.” Concussion is significantly underreported because it can be asymptomatic, and recovery is tricky to pinpoint.“When we say ‘recover,’ we mean the athlete is no longer reporting symptoms and the neurological evaluation is normal,” Dr. Dodick says.“However, residual symptoms may be quite vague — a little irritability or trouble sleeping — and may not be attributed to the concussion. Moreover, an athlete can truly have no symptoms, but the brain might actually not have recovered yet. “Sometimes athletes are reluctant to report,” Dr. Dodick adds.“One professional athlete told Bradley F. Boeve, M.D. Rodolfo Savica, M.D., Ph.D. me, ‘Concussion is a four-letter word in the locker room.’ Athletes know that if they report symptoms, they will be taken out of the game, see a lot of doctors and undergo tests, and they might lose their positions on the team. Previous concussions may also affect the way they are viewed by future teams. That’s true if you’re a 12-year-old Pop Warner football player. It’s even more true if you’re a professional athlete.” To discern specific risk factors for long-term effects, Mayo Clinic researchers are conducting a longitudinal study of people with traumatic brain injury (TBI) who later developed Alzheimer’s disease or related conditions. The study cohort is drawn from the Rochester Epidemiology Project, a collection of medical data covering virtually all residents of Olmsted County, Minnesota. “We hypothesize that we will find no association between TBI and neurodegenerative disease overall,” Dr. Brown says.“But we predict we are likely to find an increased risk of developing Alzheimer’s disease and related conditions after TBI in subsets of the cohort with clinical features that have been suspected of increasing this risk, such as multiple injuries or injuries of increased severity. If so, we hope to determine the factors that isolate that group.” Allen W. Brown, M.D. David W. Dodick, M.D. Figure 2. On the top, PET scan using fluorodeoxyglucose (FDG) appears normal. Below, FDG-PET scan after a long-standing traumatic injury in the left frontal lobe, visible in the MRI on the right. 2 MAYO CLINIC | NeurosciencesUpdate “We have many questions that need answers,” Dr. Savica adds.“Is a concussion in a car accident the same as one when playing a sport? Are some sports less likely to have long-term consequences? Is some direction or vector of trauma better than others?” Mayo Clinic’s work with SRC is enhanced by the center’s broad expertise in neurodegenerative disorders. Dr. Boeve notes that tau, the primary abnormal protein in CTE, is a target of emerging therapies for Alzheimer’s disease and other tauopathies. “There are tau-active drugs that are starting clinical trials. If they prove to be safe and effective for Alzheimer’s or related conditions, they might be applicable to CTE,”he says.“Athletes can benefit from Mayo Clinic’s expertise in Alzheimer’s disease and related neurodegenerative diseases, imaging, and brain injury rehabilitation.” Evidence to make sports safer To further safeguard athletes’ health, Mayo Clinic is at the forefront of efforts to promote change in contact sports.“To truly prevent concussion, you must understand the mechanisms of injury and then come up with strategies that are not only effective but pragmatic,”says Michael J. Stuart, M.D., co-director of the Sports Medicine Program at the Rochester campus of Mayo Clinic and chief medical and safety officer for USA Hockey.“Evidence-based decision-making is critical. We’re trying to make sports safer.” In an evidence-based action plan published in the March 2015 issue of Clinical Journal of Sport Medicine, Mayo Clinic researchers and colleagues called for the elimination of head hits and fighting from all levels of professional and amateur ice hockey and changes in body-checking policies. “Concussion prevention is multifaceted, involving behavior modification, education, enforcing existing rules and modifying rules,”Dr. Stuart says. Equipment design is necessary but not sufficient. Dr. Stuart notes that in contrast to football helmets,“hockey helmets have a very poor suspension system, often with a very loose strap that doesn’t engage the chin. Therefore, the helmet moves around on the head and often comes off. We’re very interested in improving the design and materials of the hockey helmet.” However, a better helmet can’t prevent all concussions in ice hockey or football.“When an athlete has a blow to the body, force is transmitted through the body to the head. The combined linear and rotational acceleration and deceleration to the brain can cause concussion without a direct blow to the head,” Dr. Stuart says.“In ice hockey, we are addressing that with various strategies — body control and awareness, open-ice awareness, sportsmanship and mutual respect.” “We’re slowly starting to understand what’s actually happening inside the brain — the cascade of molecular, chemical and electrical events that can lead to progressive damage,”Dr. Dodick adds.“But this field is really in its infancy in terms of understanding the biology of concussion and how to manage it, how to identify those at risk for long-term consequences, and how to mitigate or prevent the long-term effects.” For more information Smith AM, et al. Ice hockey summit II: Zero tolerance for head hits and fighting. Clinical Journal of Sport Medicine. 2015;25:78. Michael J. Stuart, M.D. Surgery and ICU: Collaborating for the Best Outcomes As a fully integrated practice, Mayo Clinic has the breadth of expertise to offer the best possible neurological care to critically ill patients. Collaboration between neurological surgeons and neurointensivists helps provide excellent functional outcome even for patients with aneurysmal subarachnoid hemorrhage (aSAH), historically considered a devastating disease. A study published in the February 2015 issue of the Journal of Neurosurgery found that 63.3 percent of patients treated for aSAH at Mayo Clinic’s Minnesota campus from 2001 to 2013 had excellent functional outcome — defined as modified Rankin Scale score of 0 or 1 (no symptoms or mild symptoms, but no disability) at last follow-up visit within one year of aSAH. The retrospective review of 373 patients included the severe cases referred by tertiary centers to Mayo Clinic’s neurointensive care unit (neuro-ICU). “We believe that our outcomes are a reflection of our multidisciplinary approach and a lack of turf battles in our group practice,” says Alejandro A. Rabinstein, M.D., a consultant in Neurology at Mayo Clinic in Rochester, Minnesota.“Our neurointensivists and surgeons have a very close relationship A throughout a patient’s acute course and follow-up treatment.” Continuity of care “The degree of expertise that a single patient receives is unparalleled,”adds Giuseppe Lanzino, M.D., a consultant in Neurosurgery at the Rochester campus of Mayo Clinic.“Each one of us brings to the table particular expertise, and by working closely together we ensure continuity of care.” When a patient with aSAH is referred to Mayo Clinic, the neuro- intensivist and neurosurgery groups communicate while the patient is en route.“A physician from both groups goes to meet the patient as soon as the patient arrives at our ICU,”Dr. Rabinstein says. “We work together because those first few hours are essential to the outcome of the patient.” The neurointensivists focus on aspects of care such as ventilation, oxygenation, stabilization of blood pressure and treatment of brain swelling, while the surgeons treat hydrocephalus.“There is a multidisciplinary conversation about the best treatment for the patient,”Dr. Rabinstein says. “For example, if there is a question of sacrificing a certain blood vessel during treatment, the surgeon might ask the neurointensivists if they think the patient will tolerate that.” At Mayo Clinic, neurological surgeons have experience in both endovascular and surgical treatment of aneurysm (Figure).“Once the patient is sufficiently stable, we transfer the patient to our angiography suite and, if possible, treat the aneurysm there,”Dr. Lanzino says.“But if the aneurysm is not amenable to endovascular treatment, then we fix it with surgery and a clip.” B C Alejandro A. Rabinstein, M.D. Giuseppe Lanzino, M.D. D Figure. A. CT scan of a patient with severe aneurysmal subarachnoid hemorrhage before treatment. Hemorrhage, brain swelling and hydrocephalus are visible. The patient was in a coma when she arrived. B. Arrow indicates the clip used to treat a ruptured superior cerebellar artery aneurysm. C. Ventricular drain used to treat the symptomatic hydrocephalus. D. CT scan at the time of the patient’s discharge from Mayo Clinic Hospital, Saint Marys Campus. At six weeks, the patient had returned to her previous function without any limitation. MAYO CLINIC | NeurosciencesUpdate 3 After treatment for aSAH, patients generally spend at least 10 to 14 days in the neuro-ICU. At Mayo Clinic, patients in the neuro-ICU aren’t routinely kept sedated and intubated for the duration of acute treatment.“We try to wake up the patient as soon as we can,”Dr. Rabinstein says.“Induced coma generally doesn’t prevent secondary complications such as brain swelling. Whenever possible, we want to assess the patient through physical examination rather than relying on brain-monitoring devices, which are commonly invasive.” The most notable complication experienced by these patients is vasospasm, which puts them at risk of stroke.“We deal with vasospasm not only with medical treatment — typically, raising the blood pressure while maintaining adequate fluid balance — but also by pursuing endovascular therapy if medical treatment fails,”Dr. Rabinstein says. After a patient returns home, surgical and neurointensivist groups continue to follow up. Appointments with both groups are typically scheduled at four to six weeks and at six months after treatment. “It’s important for patients to go to centers that have expertise and all the services that they need,”Dr. Rabinstein says.“We think we can benefit even patients who are severely ill. When I was in medical school, a case of subarachnoid hemorrhage was a spectacular success if the patient was able to walk and talk after treatment. Now, although outcomes for aSAH have generally improved, there is still an acceptance that some deficits are unavoidable. At Mayo Clinic, our definition of success is essentially a patient who is back to baseline at six weeks.” For more information Pegoli M, et al. Predictors of excellent functional outcome in aneurysmal subarachnoid hemorrhage. Journal of Neurosurgery. 2015;122:414. Autoimmune Dementia: Defining a Treatable Disorder Eoin P. Flanagan, M.B., B.Ch. Sean J. Pittock, M.D. Daniel A. Drubach, M.D. 4 Encephalopathies — typically characterized by confusion, seizures, memory loss and behavioral changes — have been well-recognized as having an autoimmune cause. In contrast, patients with progressive dementia without delirium have usually been classified as having neurodegenerative disease. Building on the pioneering work of Vanda A. Lennon, M.D., Ph.D., a consultant in the Mayo Clinic Neuroimmunology Research Laboratory, neurologists at Mayo Clinic in Rochester, Minnesota, have found that patients whose symptoms mimic those of neurodegenerative dementias can actually have an autoimmune cause for their conditions. Although autoimmune dementia responds to immunotherapy, the disease often goes untreated because of misdiagnosis as a neurodegenerative or psychiatric condition. “It can be devastating for patients to be labeled with a neurodegenerative disease but actually have an immune-mediated dementia, because they’re missing out on a treatment that can reverse their symptoms,” says Eoin P. Flanagan, M.B., B.Ch., a consultant in Neurology at Mayo Clinic in Rochester, Minnesota. “If treatment is delayed, patients tend not to respond as well. It’s important to recognize this condition because you might miss your opportunity for treatment.” A nose for atypical disease Among patients at Mayo Clinic who responded to immunotherapy for autoimmune dementia from 2002 to 2009, 35 percent were initially misdiagnosed with a neurodegenerative dis- MAYO CLINIC | NeurosciencesUpdate order. Mayo Clinic neurologists have also used immunotherapy to successfully treat patients who experienced a rapidly progressing dementia and were initially diagnosed with CreutzfeldtJakob disease. Patients with autoimmune dementia typically present with some, but certainly not all, clinical and laboratory features associated with limbic encephalitis. Clinical and laboratory features of autoimmune dementia include: • Subacute onset • Fluctuating course • Tremor • Headache • Personal or family (first-degree relative) history of autoimmunity Figure 1. On the left, MRI shows abnormal T2 hyperintensity in the left mesial temporal lobe in a patient with autoimmune dementia due to antibodies to the leucine-rich, glioma-inactivated 1 (LGI1) protein, a component of the voltage-gated potassium channel complex. On the right, MRI shows abnormal T1 hyperintensity within the basal ganglia in a patient with autoimmune dementia and accompanying faciobrachial dystonic seizures due to LGI1 autoantibodies. History of recent or past neoplasia Evidence of central nervous system inflammation from cerebral spinal fluid or MRI • Detection of neural antibody MRI might show abnormalities in the limbic lobes or elsewhere (Figure 1); PET imaging might show hypometabolism (Figure 2). Cognitive decline, particularly memory loss, is the predominant symptom. But patients can also have hallucinations and a fluctuating course of disease. “It’s important to look for atypical disease,” says Daniel A. Drubach, M.D., a consultant in Neurology at Mayo Clinic’s campus in Minnesota. “For example, when a patient is diagnosed at 45 years of age with schizophrenia, that raises a red flag. I have seen many patients with an autoimmune-based dementia who were in psychiatric hospitals.” “It comes down to the clinician having a good nose for this diagnosis,” adds Sean J. Pittock, M.D., a consultant in Neurology and director of the Center for Multiple Sclerosis and Autoimmune Neurology at Mayo Clinic’s campus in Minnesota. “You look for the clues that tell you this isn’t just run-of-the-mill neurodegenerative disease.” Mayo Clinic has developed a standardized approach to diagnostic evaluation of suspected autoimmune neurological disorders, based on three M’s: • Maximum reversibility — also called the “diagnostic test” — determined by comparison of objective baseline testing of main deficits compared with post-immunotherapy testing • Maintenance of reversibility, using long-term immunotherapy in chronic autoimmune diseases • Minimal therapeutic dosage to reduce the side effect profile To assist with diagnosis, Mayo Clinic is the first center in the U.S. to offer biomarker testing for autoimmune dementia. Serum and cerebral spinal fluid are evaluated for neural antibodies associated with the condition. Consultative comments from Mayo Clinic neurologists accompany test findings. “The panel results must be interpreted in the clinical context because there are patients with Alzheimer’s disease who have low titers of some of these antibodies,” Dr. Pittock says. Mayo Clinic consultants are also available to discuss test results over the telephone with referring neurologists. • • Treatment and response Acute treatment for autoimmune dementia generally involves intravenous steroids once a day for five days. “If patients improve, and do indeed have an autoimmune dementia, it usually occurs within the first week of treatment. A smaller minority will start to improve Figure 2. Top image, PET scan of a 68-year-old woman with a history of lupus and a 10-year history of cognitive difficulties. The scan shows prominent hypometabolism with a pattern suggestive of Alzheimer’s disease. Bottom image, PET scan of the patient after treatment with immunosuppressants. Normalization of the scan was associated with dramatic improvement in cognitive abilities. within the first month,” Dr. Flanagan says. For more-sustained improvement, patients sometimes have immunotherapy once a week for six to 12 weeks. To measure cognitive change, patients are given the Kokmen Short Test of Mental Status or more-detailed neuropsychological testing at the beginning and end of treatment. MRI and spinal fluid testing are also often done before and after treatment. “Patients may not go back to normal,” Dr. Drubach says. “But they may do better than those without treatment.” At Mayo Clinic, patients benefit from the close interaction between physicianresearchers with expertise in autoimmunity and in behavioral neurology. Dr. Flanagan has training in both. “It’s generally thought that dementias are always neurodegenerative,” he says. “But we’re at only the tip of the iceberg in terms of discovering neural antibodies. It’s important to look out for these atypical dementia cases because they can respond very well to immunotherapy.” Autoimmune Dementia Evaluation A comprehensive autoimmune dementia evaluation for serum and cerebral spinal fluid is available from Mayo Medical Laboratories. The evaluation provides neurologists with neural antibody testing for patients with symptoms of autoimmune dementia. Mayo Clinic neurologists provide interpretation of test results and are available for consultation with referring physicians. Testing must be ordered by a hospital laboratory. MAYO CLINIC | NeurosciencesUpdate 5 DBS for OCD and Tourette Syndrome Kendall H. Lee, M.D., Ph.D. Mark A. Frye, M.D. Figure. Functional MRI reveals areas of cortical activation that result from DBS for OCD (top) and Tourette syndrome (bottom). 6 Deep brain stimulation (DBS) has been used at Mayo Clinic to successfully treat hundreds of patients with essential tremor, Parkinson’s disease and dystonia. Mayo Clinic neurosurgeons are now offering DBS as a treatment option for patients with refractory obsessive-compulsive disorder (OCD) and Tourette syndrome. DBS for OCD is provided through a humanitarian device exemption granted by the Food and Drug Administration; DBS for Tourette is available in limited cases for clinical care. Although the number of patients treated so far is fairly small,“we are seeing that DBS can be highly effective for OCD and Tourette,” says Kendall H. Lee, M.D., Ph.D., a consultant in Neurosurgery at Mayo Clinic in Rochester, Minnesota. “From a psychiatric perspective, refractory OCD is one of the most disabling diseases in psychiatry,”notes Mark A. Frye, M.D., chair of Psychiatry and Psychology at Mayo Clinic’s campus in Minnesota.“For the right patient, this intervention can be life-restoring and life-saving.” Refractory, severe conditions Patients who have DBS treatment for OCD at Mayo Clinic typically haven’t responded to two or three types of conventional pharmacotherapy, augmentation strategies and structured cognitive behavioral therapy (CBT).“We do a careful assessment to make sure that the evidence base for how we treat OCD has been utilized, because we don’t want to use DBS if conventional treatments haven’t been tried,” Dr. Frye says. The conditions of patients who haven’t responded to conventional treatment can be disabling. Dr. Frye cites a young man with OCD and a history of 10 psychiatric hospitalizations, and secondary complicating features of depression. “He was plagued by recurring thoughts of sanitation and disorderliness, and compulsive behavior where he would spend hours washing his hands, engaging in ritualistic behavior, and counting,” Dr. Frye says.“Activities that most people might do for several seconds a day, he would do for several hours a day.”The patient was unable to finish college or to develop a social support network or a significant-other relationship. Since treatment with DBS, the young man has returned to college and is looking for parttime work.“By all the rating scales we’re using, his symptoms are 60 to 70 percent better,” Dr. Frye says.“The associated functional improvement has really been dramatic.” As for Tourette, Dr. Lee cites a young man with a severe tic that caused his neck suddenly to swivel powerfully. Although the patient was on MAYO CLINIC | NeurosciencesUpdate strong medication and, as a result, experienced constant sleepiness, the tic remained severe, prompting concern of possible cervical spinal injury. After DBS, the patient’s tic significantly abated, and he was able to reduce his medication. The January 2012 issue of Mayo Clinic Proceedings contained a report on that patient and two others with refractory Tourette, all of whom had excellent outcomes after treatment with DBS. Stimulation was generally well-tolerated, and some degree of efficacy against tics was noted immediately. One year after treatment, the patients had a mean reduction of 70 percent in the Yale Global Tic Severity Scale score. DBS, then CBT The procedure for performing DBS for OCD is similar to the DBS procedure for movement disorders. Patients are awake, with their heads in a stereotactic frame, so they can speak with the surgeon.“It is very helpful for us to know the effect of stimulation intraoperatively,” Dr. Lee says. The ventral capsule/ventral striatum is targeted. However, for Tourette, DBS is often done under general anesthesia.“A lot of these patients have such severe neck tics that it would be very dangerous to have them awake in a stereotactic frame,” Dr. Lee says. The target for Tourette syndrome is the centrum-median/parafascicular nucleus of the thalamus. After DBS, it is important for patients to resume CBT.“The neurosurgical intervention can alleviate terribly disabling symptoms and the associated complete functional disability related to those. But more work is needed beyond the neurosurgical procedure,” Dr. Frye says.“In fact, we find that after surgery, patients can engage in therapy in a much more beneficial way than before surgery.” The mechanism by which DBS benefits patients isn’t fully understood.“But over the past 10 years in our Neural Engineering Laboratory, we have discovered — using fMRI, electrochemistry and electrophysiology — that we are really modulating neurocircuits in the brain,” Dr. Lee says (Figure).“We have some understanding of that process for patients with movement disorders, but we know much less about how it works in psychiatric circuits.” For more information Savica R, et al. Deep brain stimulation in Tourette syndrome: A description of 3 patients with excellent outcome. Mayo Clinic Proceedings. 2012;87:59. Research Highlights in Neurology and Neurosurgery New Diagnostic Criteria for NMOSD Neuromyelitis optica (NMO) is an inflammatory syndrome of the central nervous system (CNS) that is distinct from multiple sclerosis (MS) and is associated with serum aquaporin-4 immunoglobulin G (AQP4-IgG) antibodies. Prior NMO diagnostic criteria required optic nerve and spinal cord involvement, although more-restrictive or moreextensive CNS involvement may occur. An international consensus panel, chaired by consultants in Neurology at Mayo Clinic in Phoenix/Scottsdale, Arizona, and Mayo Clinic in Rochester, Minnesota, has introduced new diagnostic criteria. Using systematic literature reviews and electronic surveys to facilitate consensus, the panel defined the unifying term neuromyelitis optica spectrum disorders (NMOSDs), which is stratified further by serologic testing (NMOSD with or without AQP4-IgG). The core clinical characteristics required for patients with NMOSD with AQP4IgG include clinical syndromes or MRI findings related to optic nerve, spinal cord, area postrema, other brainstem, diencephalic or cerebral presentations. More-stringent clinical criteria, with additional neuroimaging findings, are required for NMOSD without AQP4-IgG or when serologic testing is unavailable. The international panel also proposed validation strategies and achieved consensus on pediatric NMOSD diagnosis and the concepts of monophasic NMOSD and opticospinal MS. Under the new criteria, a diagnosis of optic neuritis and myelitis is no longer required to identify NMOSD if an AQP4-IgG blood test proves positive. The criteria are expected to facilitate earlier and more-accurate diagnosis by identifying individuals who would have been diagnosed with idiopathic transverse myelitis, idiopathic optic neuritis or atypical MS. The criteria should also provide greater specificity for distinguishing both AQP4-IgG-seropositive and AQP4-IgG-seronegative NMOSD from MS. Early-stage diagnostic specificity is critical because recent observational data suggest that MS therapies (interferon-b, natalizumab and fingolimod) may aggravate NMOSDs. (Wingerchuk DM, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015;85:177.) Molecular Classifications of Gliomas The prediction of clinical behavior, response to therapy and outcome of infiltrative glioma is challenging. Studies of glioma biology have led to the discovery of hundreds of molecular alterations in grade II, III and IV gliomas. Among these molecular alternations, three are particularly noteworthy because they occur early during glioma formation, are prevalent in glioma or are strongly associated with overall survival. Researchers at Mayo Clinic in Rochester, Minnesota, and colleagues at the University of California, San Francisco, have classified gliomas into five principal groups on the basis of these three tumor markers: mutations in the telomerase reverse transcriptase (TERT) promoter, mutations in isocitrate dehydrogenase (IDH), and codeletion of chromosome arms 1p and 19q. Using the results of previous studies of tumor biology, the researchers scored tumors in 1,087 gliomas as negative or positive for each of the three markers. Using 11,590 controls, the researchers assessed associations between the top five molecular groups and known glioma germline variants. Patients within each of the five groups (triple-positive, TERT- and IDH-mutated, IDH-mutated only, TERT-mutated only, and triple-negative) had similar age of onset and overall survival. However, the five groups differed from one another in age at onset, overall survival and association with germline variants. The results imply that gliomas in the five groups are characterized by distinct mechanisms of pathogenesis. (Eckel-Passow JE, et al. Glioma groups based on 1p/19q, IDH and TERT promoter mutations in tumors. New England Journal of Medicine. 2015;372:2499.) Neurosciences Research Brain Transcriptome Profiles in ALS Misregulated RNA processing and metabolism are recurrent themes in neurological disorders, but their involvement in amyotrophic lateral sclerosis (ALS) isn’t clearly established. Researchers at Mayo Clinic in Jacksonville, Florida, have identified widespread transcriptome changes in individuals with ALS carrying a C9orf72 repeat expansion (c9ALS) as well as in individuals with sporadic ALS. Utilizing next-generation RNA sequencing to analyze post-mortem brain tissue, the researchers found major misregulated RNA-processing events in ALS, several of which affected genes previously associated with the disease, such as ATXN2 and FUS. Several aberrant transcriptome changes were shared between people with c9ALS and people with sporadic ALS. However, overall, the c9ALS transcriptome was affected to a greater degree than that of sporadic ALS, with little overlap. This limited overlap may result from the presence of pathological features unique to c9ALS in the frontal cortex and cerebellum, as well as heterogeneity among sporadic ALS cases — for example, mutation in an unknown gene. Unexpectedly, more-robust transcriptome changes were found in the cerebellum than in the frontal cortex. The study results indicate that distinctive factors may contribute to c9ALS and sporadic ALS, with consequences for the development of therapies. (Prudencio M, et al. Distinct brain transcriptome profiles in C9orf72-associated and sporadic ALS. Nature Neuroscience. 2015;18:1175.) To read more about Mayo Clinic neurosciences research and patient care, visit www.MayoClinic.org/medicalprofs. MAYO CLINIC | NeurosciencesUpdate 7 MAYO CLINIC Neurosciences Update Medical Editors: Claudia F. Lucchinetti, M.D. Robert J. Spinner, M.D. Education 2015-2016 Neurology and Neurologic Surgery Continuing Medical Education Programs Editorial Board: Mark K. Lyons, M.D. James F. Meschia, M.D. Joseph I. Sirven, M.D. Robert E. Wharen Jr., M.D. December International Dementia with Lewy Bodies Conference 2015 Dec. 1-4, 2015 Marriott Harbor Beach, Fort Lauderdale, Fla. Science Writer: Barbara J. Toman Mayo Clinic Neurosciences Update is written for physicians and should be relied upon for medical education purposes only. It does not provide a complete overview of the topics covered and should not replace the independent judgment of a physician about the appropriateness or risks of a procedure for a given patient. Contact Us Mayo Clinic welcomes inquiries and referrals, and a request to a specific physician is not required to refer a patient. Phoenix/ Scottsdale, Arizona 866-629-6362 (toll-free) Jacksonville, Florida 800-634-1417 (toll-free) Rochester, Minnesota 800-533-1564 (toll-free) Resources MayoClinic.org/medicalprofs Clinical trials, CME, Grand Rounds, scientific videos and online referrals April 3rd Annual Southwest Laryngology Voice Rehabilitation Conference 2016 April 8-10, 2016 Taylor Auditorium, Mayo Clinic, Scottsdale, Ariz. Neurorehabilitation Summit: Regeneration, Recovery, Reintegration 2016 April 11-12, 2016 Leighton Auditorium, Mayo Clinic, Rochester, Minn. May Neuro and Intensive Critical Care: Review and Hands-on Workshops 2016 May 12-14, 2016 Loews Royal Pacific Resort, Orlando, Fla. November Neuroradiology: Practice to Innovation Course 2016 Nov. 14-18, 2016 The Ritz-Carlton, Grand Cayman, Cayman Islands Information and registration Mayo Clinic in Rochester, Minnesota Phone: 800-323-2688 (toll-free) or 507-284-2509 Email: [email protected] Mayo Clinic in Jacksonville, Florida Phone: 800-462-9633 (toll-free) or 904-953-0421 Email: [email protected] Mayo Clinic in Phoenix/Scottsdale, Arizona Phone: 480-301-4580 Email: [email protected] Website: www.Mayo.edu/cme/neurology-and-neurologic-surgery Expedited Patient Referrals to Mayo Clinic Departments of Neurology and Neurologic Surgery While Mayo Clinic welcomes appointment requests for all neurologic and neurosurgical conditions, patients with the following conditions are offered expedited appointments: 1. Cerebral aneurysms 2. Cerebral or spinal arteriovenous malformations 3. Brain, spinal cord or peripheral nerve tumors 4. Epilepsy with indications for surgery 5. Carotid disease MC5520-1015