Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Psychopharmacology wikipedia , lookup
Epinephrine autoinjector wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug interaction wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacokinetics wikipedia , lookup
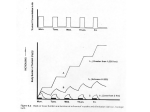
1st Medicon Valley Inhalation Symposium Explore the Inhalation Opportunity 17 October 2012 09.00–17.00 Medicon Village, Lund, Sweden inhalationsymposium.com Platinum sponsors Gold sponsor CI Informatics Ltd. Nolato MediTech Silver sponsors Oxford Lasers Pharmaterials Ltd Det Medicinska Malmö ExIS AB Epsilon AB QSCL Q Scientific Consulting The secrets of dry powder inhalation from a solid state perspective Lars-Erik Briggner, 121017 Adroit Science Medicon Village, Lund Content Particle size… Consquences of size reduction… Mitigation… Humidity interaction… Electrostatics… In the best of worlds… Dry Powder Inhalation of drugs need, Too large particles do not reach the lung – impacts in the throat and is then swallowed Too small particles do not reach the lung – exits with the exhalations 100 Exhaled Deposition, % Throat 50 Lung 0 0.01 0.1 1 Particle size, µm 10 100 with some implications for the drug! Material intended for dry powder inhalation administration has to… 1.…cope with the particle reduction technique, e.g. micronisation by a Jet mill, providing a reasonable through put in the mill (yield, no clogging etc) 2.…be possible to administer in an efficient way into the lung. Potential agglomerates have to deaggregate into small aggregates and/or primary particles during the actual inhalation process in order to follow the airstream into the lung (and not Particle size reduction Many different techniques in theory… Micronisation Spray drying Super critical techniques Specialized crystallization techniques … …but with different drawbacks Amorphicity Scale of production Universatility with respect to API properties Stability/solubility/compatibility … Micronisation is by far the most common… Fluidized Jet milling (micronisation) Consequences of micronisation… Reducing particle size is a high energy process, relying on collisions between walls and/or particles, potentially resulting in… around 50 °C in mill!! …specific particle size distribution …more rounded shape …aggregates and/or agglomerates …solid state transitions …local melting events …drying out of semi stable hydrates …charging of the powder (electrostatic) …disordered/amorphous regions Effect of milling pressure Common region for modern drug candidates From Article (L-E Briggner et al) : Int J Pharm 105 (1994) 125-135) μ-calorimetry, Glass ampoule exp. P/mW 2.4 “Microhygrostate” Saturated salt Solution; EtOH, H2O etc 1.8 II 1.2 Sample 0.6 I – Humidity adsorbtion II - Crystallization I 0.0 0 50 100 Time/min 150 Measure enthalpy of crystallistion (and sorption effects) High sensitivity (<0.5%), with flow cell <0.1%) High reproducability Timescale ½-5 hours FPF for micronised material Examples from dose withdrawal at different RH Conditioning (restore crystallinity) Conditioning is normally based on plasticizing (lowering of Tg)… increasing molecular mobility) by means of vapor (small molecules) and/or increased temperatures leading to controlled recrystallisation Concerns Specific surface area decreases significantly Issues with particle growth “bridge formation” between particles Hydrophilic or hydrophobic compounds Hydrate/solvate formation Chemical stability Increasing RH on micronised mtrl Crystallisation H2O efficient plasticizer due to its low Tg, -135 °C Increasing temp. on micronised mtrl 0.05 1.4 0.14 Rev Heat Flow (W/g) Heat Flow (W/g) 0.00 Crystallisation 0.9 76.59°C 83.58°C 3.060J/g 73.16°C 0.05815J/g Tg 0.4 98.63°C 0.12 -0.05 Nonrev Heat Flow (W/g) 168.46°C 78.08°C(I) 0.10 164.51°C 60.92J/g -0.1 0 Exo Down 50 100 150 Temperature (°C) 200 -0.10 250 Universal V4.4A TA Instruments Intensity (cps) XRPD before and after conditioning 60 50 40 30 20 10 0 5 10 15 20 25 30 35 2Theta (°) FPF after conditioning Fine Particle Fraction (<5um of dd) 30 25 20 15 10 5 0 0% RH to 0% RH 0% RH to 75% RH Examples from dose withdrawal at different RH Humidity Interaction – GVS Sample: AZD2230 fri bas Size: 5.9940 mg Method: HADES-metod 0.00005 %/min Comment: Mikroniserad, SN1069901086 (ej nya hydratformen) File: \\...\PoB_GVS\TA\HADES\AZD2230.001 Operator: ED/LAB Run Date: 2007-07-04 10:50 Instrument: TGA Q5000 V3.3 Build 250 3 80 2 1 0.7552% 40 0 Relative Humidity (%) Weight Change (%) 60 20 -1 -2 0 200 400 600 800 Time (min) 1000 1200 1400 0 1600 Universal V4.4A TA Instruments Humidity Interaction – GVS cont. Sample: AZD2230 fri bas Size: 5.9940 mg Method: HADES-metod 0.00005 %/min Comment: Mikroniserad, SN1069901086 (ej nya hydratformen) File: \\...\PoB_GVS\TA\HADES\AZD2230.001 Operator: ED/LAB Run Date: 2007-07-04 10:50 Instrument: TGA Q5000 V3.3 Build 250 -0.6 -0.7 30 -0.9 20 -1.0 0.5953%/min -1.1 Relative Humidity (%) Weight Change (%) -0.8 10 -1.2 690.36min -1.3 689.5 690.5 Time (min) 0 691.5 Universal V4.4A TA Instruments FPF for a Channel Hydrate 45 Fine Particle fraction 40 35 30 25 FPF (% of dd) 20 15 10 5 0 0-75%RH D55190-0%RH behaves quite OK at dry conditions while a withdrawel at weighed weighed 75% RH induce a major decrease in FPF Powder Properties Characterization 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% plastic adhesion steel adhesion cohesion respirable fraktion Electrostatics, example of results Untreated Powder ”Discharged Powder Ideally... Particle generation possible... •...especially micronisation “default method”. Thermally stable to... • ...avoid thermal transitions at low (Requires ingoing material to be crystalline.) •...using standard milling technologies for formulation development temperature • ...facilitate Manufacturing/Synthesising.. • ...make processing (micronisation, compression etc.) possible • ...facilitate storage, transport High Crystallinity to... •...accurately assess Biopharm risk (i.e. accurate solubility measurement) • ...be easier to manufacture • ...provides route for purification • ...improved chemical & physical stability Non-hygroscopic so that... • ...the compound will have sufficient chemical stability • ...inhalation can be possible (otherwise risk for agglomeration leading to non-inhalable material) • ...no analytical problems associated with changing humidity will occur “Formulability” in order to... • ...prepare relevant solution/suspension e.g. must not gel etc. (often the case for amorphous compounds) How to get high FPF – some thoughts Low bulk density… Beneficial morphology… “Hedgehog” surfaces!? Non-sticky surfaces (adhesivity and cohesivity)… Non deforming particle, no “shear planes” in the structure… Optimal particle size distribution… “Small” humidity dependence… (channel hydrates!!) No amorphous surfaces – conditioned… Low static charge built up www.adroitscience.com Inhalation – puts a new twist on pharmacology 1st MVIC symposia Lund 2012‐10‐17 Karin von Wachenfeldt Whygoinhaled? Maximize local exposure Convenient administration route Minimize systemic exposure Positioning Localeffect‐ lungrelatedindications • Local effect desired, e.g. for treatment of asthma and COPD. • Rapid delivery to the right location • Bronchodilators ‐ rapid onset of action is crucial • Hit‐and‐run effect • Long‐term exposure at the right location • Glucocorticoids – long‐term “low” level exposure • Mechanisms for lung retention • +/‐ Systemic exposure • Systemic exposure to beta‐agonists associated with side‐effects • Some exposure to glucocorticoids desired for maximal efficacy. DeliveringLungefficacy Adapted from G. Hochhaus PATS 2004 Drugsmetabolizedboth inlungandliver Lung metabolism Smoking induces lung specific CYPs Liver metabolism Adapted from G. Hochhaus PATS 2004 Inhaleddrugsforsystemicexposure ① Inhalation circumvents the “hostile” gut environment. ② Delivery to the lungs for systemic exposure – provides a direct route to the brain. Frequently exploited for delivery of aneastetics. Routes of Drug Administration Oakley, R. & Ksir, C. (1996) Drugs, Society, and Human Behavior, 7th Ed ….aswellascigarettesmoke. Mode‐of‐Action • What types of drugs are suitable for inhalation? • Local exposure mostly agonists. • Hit‐and run principle. Compounds that are rapidly cleared from lungs can still have good effect. • Antagonist effects often require long‐term target inhibition. • Compounds need to have long lung‐retention. Needs to be engineered into molecule from start. • Several strategies can be used; • Low solubility • Active retention in lung cells • Binding kinetics Budesonide‐ theidealinhalationsteroid? Epithelial Cell Budesonide retained within epithelial cells. Increases duration of action. BUD Ciclesonide – thedesignerinhaledGCS Ciclesonide Pro‐drug Des‐CIC Active metabolite Des‐CIC oleate Retained From Nave R, Meyer W, Fuhst R, et al 2005. Wheredoyouneedtheeffect? ① Achieve exposure in the right place. ② Dry powder vs. nebulized solution. ③ Particle size ④ Device Peripheral deposition Central “bronchial” deposition Summary • Inhalation – what do you want to achieve? • Focus the effect, or simply deliver the drug? • Reduction of systemic side‐effect profile. • Important to consider need for systemic exposure. • Different metabolism, lung vs. liver. • Different metabolism in healthy vs. diseased lung. • Where in the lung is the effect needed? • Through a smart inhalation strategy you can reach your target. • Differentiation • An effective inhaled drug is less threatened by generic competition – also after patent expiration for your compounds. 1st Medicon Valley Inhalation Symposium 2012‐10‐17 SUCCESSFUL INHALATION STARTS WITH COMPOUND DESIGN THOMAS BRIMERT www.redglead.com WHY INHALATION ? 1. For systemic effect: • Large surface area • Thin alveolar epithelium • Less metabolism • Active transport • Consider making a prodrug 2. For local effect: • Avoid side effects from systemic exposure • Poor oral availability • Consider making a soft drug Inhalation can turn your weaknesses into strenghts www.redglead.com DEFINITION OF PRODRUG A prodrug is a pharmacological substance that is administered in an inactive (or less than fully active) form, and is subsequently converted to an active pharmacological agent through normal metabolic processes • Injected or inhaled (free base) • Passes bbb • Metabolized to morphine (active) www.redglead.com MED. CHEM. DEFINITION OF SOFTDRUG Soft drugs are drugs which are characterized by a predictable and controllable in vivo destruction (i.e. metabolism) to non-toxic products after they have achieved their therapeutic role. Budesonide is quickly oxidized in the liver to 16α‐hydroxyprednisolone www.redglead.com DESIGNED FOR INHALATION EXAMPLE 1 How to utilize specific transporters in the lungs through a prodrug Transporters in the lung Carnithine From : P. Zarogoulidis et al. Int. J. Nanomedicine, 2012, 7, 1551–1572 Prednisolone www.redglead.com PDSC • PDSC = prednisolone linked with carnitine • Actively transported by organic carnitine transporters OCTN1 and OCTN2 • PDSC displayed 1.79‐fold increase of uptake compared to prednisolone • in vitro LPS‐induced IL‐6 production from BEAS‐2B was more and longer suppressed by PDSC than prednisolone X. Sun et al., Mol. Pharmaceutics, 2011, 8 (5), 1629–1640 www.redglead.com DESIGNED FOR INHALATION EXAMPLE 2 Soft drug long‐acting β2‐agonists (LABAs) for Asthma and COPD • How to improve duration of action • Minimize cardiovascular sideeffects • Minimize risk for Drug‐Drug‐Interactions Examples of current therapies: Salmeterol Formoterol www.redglead.com 2 violations of Lipinski’s rule of 5 Rat in vivo clearance 103 ml/min/kg Rat plasma protein binding 95% Caco‐2 (B‐A)/(A‐B) > 13 (efflux) Rat in vivo p.o. bioavailability < 5% Dog in vivo PF610335 Salmeterol Formoterol lung ED50 DoA at ED50 TI lung vs CV 0.1 µg >8 h ≥10 1 µg 4 h 1 0.1 µg 4 h 1 Pfizer compound PF610355 Site for glucuronidation => mixed metabolism Dimethyl to balance lipophilicity And remove one chiral center Acidic sulfonamide and basic amine form zwitterion => Excellent crystallinity P.A. Glossop, C.A.L. Lane et al.,J. Med. Chem. 2010, 53 (18) 6640‐6652 www.redglead.com DESIGNED FOR INHALATION EXAMPLE 3 Soft drug inhaled p38 kinase inhibitors VX‐745 Clinical findings of oral p38 inhibitors • Skin disorders • Infections • CNS‐toxicity • Elevation of liver transaminases • Lack of efficacy Improve selectivity and Duration of Action (DoA) BIRB‐796 Examples of oral p38 kinase inhibitors www.redglead.com BIRB‐796 Slow koff Pfizer hit Very potent and selective • Potent • Selective • Slow koff www.redglead.com Site for glucuronidation => mixed metabolism Chlorine make phenol more acidic • • CYP450 oxidation of sulfur to less active metabolites Rat i.v. Cl 33.8 ml/min/kg Rat ppb 99.8% Rat p.o. F <5% Selectivity was >1000 x primary pharmacology in 68 of 68 targets (CEREP ligand profiling) Clean in 4 day rat tox 2.8 mg/kg/day Hydroxyethylene to increase solubility D. S. Millan et al., J. Med. Chem. 2011, 54, 7797‐7814 www.redglead.com • Lungs are different ! • You can design molecules to utilize specific pharmacology in the lungs • You can design a molecule with local effect in the lung and low systemic exposure Thank you ! Physics in Inhalation Devices Björn Ullbrand Office Locations 1 Staffanstorp, Sweden. Head office. 3 2 Kista, Sweden. 2 1 3 Rognan, Norway. Areas of Expertise • Validus Engineering AB specializes in product development in combination with FEA, Finite Element Analyses, and CFD, Computational Fluid Dynamics • Our competence is based on over 20 years of industrial experience and our connection to the academic society • Member of MVIC Outline • Computational Fluid dynamics (CFD) • Dry particle physics (DPI) • Wet particle physics (pMDI) • Moisture transport Computational Fluid Dynamics (CFD) • Standard tool for simulating airflow and particles in inhalation applications • Powerful computers are required to allow massive parallel computations CAD MESH CFD Process Throat geometry from www.isam.org RESULTS Computational Fluid Dynamics (CFD) • Important tool for analysing: • Flow distributions within devices (by‐pass flow etc.) • Pressure drop (inhalation resistance) • Indirect methods (no particles) • Turbulence intensity (de‐aggregation) • Wall shear stress (retention analyses) • Direct methods • Multiphase flows with particles or droplets • Cavity emptying • Deaggregation • Deposition Flow distribution & pressure drop (DPI) • DPI’s typically rely on the patient to provide the energy for dose delivery and deaggreagation during inhalation • Goal: Max deaggregation and min retention for min pressure loss • Simulation gives information about total flow rate, flow distribution and pressure loss locations Total pressure distribution Velocity distribution Turbulence • Turbulence is a very complex phenomenon • • • • Transition from laminar to turbulent flow Large range of scales Computationally expensive to resolve turbulence (DNS/LES) Often approximated by using time averaged models (RANS) LES Large Eddy Simulation RANS Reynolds Averaged Navier Stokes Flow optimisation • Flow distribution and geometry is important for optimisation of performance • Example: Cavity de‐aggregation and dose delivery optimisation • Optimisation of Q1 flow (pipe dimension and direction) • Increasing velocity in cavity to reduce retention. Q1 Q2 Velocity magnitude Baseline Mod #1 Mod #2 Flow optimisation • Increasing turbulent kinetic energy in cavity to increase de‐ aggregation • Significant increase is seen for Mod #1 and #2 Turbulent kinetic energy Baseline Mod #1 Mod #2 Flow optimisation • Wall shear stress can be used as an indicator of retention • Low shear stress – high retention • High shear stress – low retention • Average wall shear stress along cavity wall is showing significant increases for Mod #1 and #2 Wall shear stress 0.34 N/m2 1.51 N/m2 Baseline Mod #1 2.54 N/m2 Mod #2 Dry particles physics (dilute) • Normally treated as a light phase not affecting the fluid flow • 1‐way coupling (particles not affecting carrier fluid) • Momentum transfer only • Equation of motion solved in a Lagrangian reference frame: du p dt FD (u u p ) g ( p ) p F • Used for DPI particle analyses Dry particles (USP 100 l/min) 20 micron particle tracks 20 micron particle deposition pattern Dry particles (USP 100 l/min) • Validation of the numerical models are essential for successful application in inhalation projects Experimental data from Blomgren C-H, Simulation of throat deposition using Large Eddy Simulations, ISSN 0282-1990 Dry particles physics (dense) • Situations with dense particles also occurs in inhalation devices, typically in cavities where particles are stored • This leads to a stronger interaction between the two phases and can be analysed with e.g. two‐phase Eularian models where both phases are treated as a continuum Analysis of optimised cavity • Cavity partly filled with 30 micron lactose particles • Findings from indirect method verified by two‐phase model analysis Baseline Mod #2 Dry particles physics (DEM) • Discrete Element Methods (DEM) can also be used for dense particle systems where large number of particles are tracked including particle‐particle interaction • 3rd party software can be used for particle models to simulate various shapes and agglomerates • Could be used for de‐aggregation analyses Wet particle (droplets) physics • Similar to dry particle physics but more interaction with light phase • 2‐way coupling (droplets also affect carrier fluid) • Momentum transfer • Mass transfer • Heat transfer • Atomization process is very complex • Initial size, velocity and direction at nozzle exit needs to be defined pMDI spray Wet particles (pMDI spray simulation) • Rosin-Rammler droplet initial size distribution (1-20 micron) • HFA propellant in liquid and gas phase • Boiling point 255 K • Rapid evaporation of droplets into vapour phase • Instant evaporation upon wall impact (no bouncing or break-up) • Volatile fraction set to 97% leaving a solid core particle Throat geometry from www.isam.org Wet particles (pMDI spray simulation) • Rosin-Rammler droplet initial size distribution (1-20 micron) • HFA propellant in liquid and gas phase • Boiling point 255 K • Rapid evaporation of droplets into vapour phase • Instant evaporation upon wall impact (no bouncing or break-up) • Volatile fraction set to 97% leaving a solid core particle Throat geometry from www.isam.org Wet particles (pMDI spray simulation) Wall temperature Instantaneous deposition pattern Moisture transport in devices • Important for drug stability (shelf‐life and in‐use) • Many substances are sensitive to humidity • Can be simulated by using analogy to heat transfer • Temperature is replaced with relative humidity etc. • Experimental data normally required for material properties • Validation is performed by comparing to stability testing data Moisture transport in devices (example) • Device with drug compartment placed in humid/hot condition Substance compartment Al-foils (seal) 40oC/75%RH HDPE (plastic material) Desiccant (Silica-Gel) Moisture transport in devices (example) • Moisture is transported through side walls • RH level in substance compartment is increasing but remains relatively dry for long time • Simulation time: 30 minutes for 1000 days of real time Conclusions • Fluid dynamics analysis is important in inhalation projects in order to visualize and understand the physics involved and as an aid in the optimization process • Simulations needs to be performed in parallel with experimental work for validation and verification of the models applied • Flow rate & distribution, pressure drop, turbulence intensity and wall shear stress are typical physical parameters of interest. • Indirect methods can be a very effective alternative to more complex methods, reducing the time and cost requirement • Dry and wet particle physics can be included in the flow analysis and be used for e.g. deposition and deaggregation analyses • Using an analogy with heat transfer it is possible to efficiently simulate moisture ingress in inhalation devices Formulation Manufacturing Challenges A broader perspective QbD Product Development Nils Ove Gustafsson, Galenica AB Galenica AB • • • • • • • Contract Development Organization Formulation and Process Development Analytical Development CTM Manufacturing Tech Transfer All Different Kinds of Dosage Forms Located in Malmö, Sweden Formulation Manufacturing Challenges • Inhaled drugs are complex products! • Their function is a combination of a formulation and a device, both the device and the formulation being complex • Due to the complex nature of inhaled products, the use of a Quality by Design approach in development is encouraged QbD Short Version • Use good science when developing your product • Understand your product and processes, use the knowledge gained during development and manufacturing and share it with the regulatory agencies QbD Slightly Longer Version • Set the design target for the product • Identify what critical attributes that describes the quality of the product (safety and efficacy) • Identify the factors with potential effects on the critical quality attributes • Use a risk based approach to rank the factors and investigate the most critical factors further • Use the gained knowledge to define the control strategy of the product • Use the gained knowledge during manufacturing for continuous improvements QbD Even Longer Version • ICH Q8 (R2) Pharmaceutical Development • ICH Q9 Quality Risk Management • A number of presentations, seminars, courses, workshops, mock-up papers etc…. Formulation Manufacturing Challenges Armanni et al. http://www.ipacrs.com/PDFs/Posters/RESP_On-screen%20version_IPAC2008%20Poster.pdf QbD, What’s new? • • • • • Encouraged by Regulatory Agencies More Structured Approach Common Language Linking Risk Assessment to Science Increased Regulatory Flexibility Post Approval Manufacturing Challenges Manufacturing Challenges Define the manufacturing scale! What governs the manufacturing scale • Commercial considerations – Future markets and estimated sales? • Manufacturing site – Current equipment? – New equipment? – CMO? • Technical aspects When do we know the manufacturing scale? A BROADER PERSPECTIVE Two very good thing to have when developing a product: • Target Product Profile • Product Development Plan Target Product Profile What do we want to develop? Product Development Plan How do we develop it? Product Development Plan Includes: • API and Preformulation • Formulation development • Device development • Preclinical development • Clinical development • Process development and scale up • Regulatory strategy • Manufacturing • Market considerations • ……. Product Development Plan • Living document • Refine and fill in as the development progress • Better to have something than nothing! • A number of competences needed when preparing the plan • Might also be a valuable asset! Product Development Plan Start CTM development Unit Dose Device New Multi Dose Device POC / Early stage clinical trials New Multi Dose Device New Multi Dose Device Late stage clinical trials Finished Product Product Development Plan Start CTM development Development Development Unit Dose Device New Multi Dose Device Development POC / Early stage clinical trials Development New Multi Dose Device New Multi Dose Device Finished Product Late stage clinical trials Conclusions • It is important to know where you want to go and the way to get there • It takes a lot of different competences involved in a project, already in an early stage, to reach the goal in an efficient way • Do not forget to document your work properly Comments? Questions? - Confidential - OUR INNOVATION STRENGTH BECOMES YOUR COMPETITIVENESS WITHIN INJECTION, INHALATION AND CONNECTIVITY/COMPLIANCE Device as the Strategic Weapon in a Saturated Inhalation Market Morten Nielsen, CEO Bang & Olufsen Medicom a/s MVIC Symposium - 17th October 2012 ” Our innovation strength ... ... becomes your competitiveness” 1 - Confidential - A few words on MEDICOM ... Key figures 16.000.000 14.000.000 ~9,5 MEUR (2012) Employees: “We deliver solutions that are not already out there” 10.000.000 8.000.000 6.000.000 4.000.000 2.000.000 ‐ 2008 Revenue 12.903.000 2009 2010 2011 2012 forecast 2013 forecast 15.053.000 10.662.000 7.914.000 10.700.000 11.898.000 < 2007: 100% owned by Bang & Olufsen a/s > 2007: 65%: Maj Invest Equity and Management 35%: Bang & Olufsen a/s Copenhagen • • • • Our Services Device Strategy & Technology Device Feasibility & Concept Device Development Pilot and low-volume production • • • • • Our Technology Innovation Devices for Injection Devices for Inhalation Devices for Connectivity Integrated Mechatronics Design and User-Centricity The Medicom Pulse Injection >> << Connectivity Inhalation >> ” Our innovation strength ... ... becomes your competitiveness” 60 12.000.000 Ownership “We help our clients meet the unmet needs in their markets” Struer - HQ 8 MEUR (2011) EUR Revenue: “We deliver innovative and benefit-driven drug delivery device solutions” 2 Strategy & Technology Service Strength • Specialist insight in injection, inhalation and connectivity • Understanding endto-end technology drivers and consequences • Understanding combining drug and device solutions Feasibility & Concept Service Strength • Integrated mechanics and electronics (including QA & RA demands) • Close integration with clinical device production • Strong partner network of industry specialists Highlights • Technology and Device mapping • Device & Drug assessment • Device strategy options • Patent assessment Development Service Strength • Strong design and usability insight • Strong device architectural and conceptual skills within both mechanics and electronics • Fast prototyping skills (fast to demo) Highlights • Future electronic injector concepts • Future electronic concepts • Advanced pump concepts • Advanced dosing concepts Highlights • Electronic autoinjectors • Dual-shot autoinjectors • Electronic stethoscopes • Advanced inhalers Clinical Low-volume production Service Strength • Flexible and manual • Experience from electro-mechanical production • Outsource sub-parts and sub-systems to far-east suppliers Highlights • Auto injectors • Pen injectors and accessories • Electronic stethoscopes • Inhalers • Electronic compliance devices Device as the Strategic Weapon in a Saturated Inhalation Market Basic delivery + Industrial design + Ease of use, automation, feedback + Connectivity + Service - Confidential - Let’s start with a little story on Asthma/COPD ... Annual lost productivity resulting from poor asthma control in the EU is estimated to 9.8 billion € ***) Annual cost of asthma in the EU is estimated to 17.7 billion € ***) In the UK it is estimated that 75% of hospital admissions due to asthma could be avoided *) Successful management of asthma preventing exacerbations would reduce cost 3.5 times ****) Hospitalization for acute exacerbation of COPD is a major annual cost contributor **) http://www.asthma.org.uk/news-centre/facts-for-journalists, ** http://www.who.int/gard/publications/chronic_respiratory_diseases.pdf *** ”The economic burdon of occupational asthma in Europe”, Huo Jinhai, Umeå university, 2010, **** ”Risk factors and costs associated with an asthma attack”, Hoskins, G et al, Thorax ” Our innovation strength ... ... becomes your competitiveness” 4 - Confidential - The step-change device innovations driven by industry is not impressive! pMDI’s have been around since the 50’ties “Numerous studies have shown that patients didn’t know that they should keep track and patients ended up calling 911” Dose counters were only reluctantly added to pMDI’s when FDA made a requirement Why so reactive? “The pharmaceutical companies focus have traditionally been the Drug” DPI’s are inherently Breath Actuated and dose counters are typically easy to implement ”We will sell the Drug in a bucket if possible” No “new” thinking on -Ease of use -Adherence “Old wine on new bottles” thinking ” Our innovation strength ... ... becomes your competitiveness” 5 - Confidential - Paradigm shift in thinking ... Devices can be a strategic weapon! • Improve adherence • Improve Inhalation Technique • Improve Quality of Life • Increase productivity of patient • Reduce hospitalization cost • If DCT is high, numerous options are available • If DCT is low, options are reduced, but they are still there and requires a new thinking on device cost structures Market Opportunities Treatment and trends Treatment and context Therapy Value chain Stakeholder Network Disease knowledge Treatments and drugs Diagnostics methods Monitoring Treatment environment Geographic market segments Work load distribution Cost of treatment Reimbursement Major players Roles (decision power and competences) Interactions (strong/weak) Present device options Future competition Market Technical solutions Service solutions Primary packaging Delivery devices Monitoring devices Solutions maturity level Patient f orums Web based solutions Social network Support services Known plans Anticipated changes Competitor pipeline Future launches Patent expiration Anticipated competitor initiatives Likely product launches US / Western Europe Far East (India) Execution Device (%) options Product DCT Technical Product DCT options Device (%) Segmentation aspects • Breath actuation/coordination • Training devices • Dialogue tools between HCP and patient ” Our innovation strength ... ... becomes your competitiveness” < 0.1 % Internal Issues 0,1-4 % 100 $ Financial Technical Formal Economical Technical Formal Reimbursement Outcome improvement Time savings Cost of treatment Device expenses Service expenses Resources Financial Manning and capacity Market maturity Readiness Expectations Regulatory Explicit requirements Approval procedures Competition Existing IPR Expected LCM initiatives Timeline Supply chain Needed development time Use of existing platforms Feasibility of new equip. Technical risk Feasibility 6 Organization Training ability Sales and service skills User segments ► Entry product ► Market segment 0.1-0.4 $ Added features ► ► Added diversity Competition aspects New drugs Expected LCM ► ► Patent expiration ► Design identity Corporate aspects Single product ► Platforms Timing aspects Sequencial launch Direct and Indirect Constrains External Issues Cystic Fibrosis 0.4 – 3.8 $ Internal Issues Asthma/COPD External Issues One f its all Evolution and LCM aspects ► n/a ► Added service 7-15% n/a Parallel execution • Traditional thinking on cost structures for Inhaler market have put extreme cost pressures on the device - Confidential - Device categories How mature are you in your inhalation device strategy? Basic delivery + Industrial design + Ease of use, automation, feedback + Connectivity + Service Products Asthma/ COPD in DK Force reduction Dose counting pMDI Breath actuation Trainer, integrated/stand - alone Dose confirmation, dose registration Dose confirmation, dose registration, wireless connectivity Services Dose counting Trainer, integrated/stand - alone DPI Dose confirmation, dose registration Dose confirmation, dose registration, wireless connectivity ” Our innovation strength ... ... becomes your competitiveness” 7 Services - Confidential - Device categories Could there be a potential for other unmet needs .. .... if we take a look at the entire “disease chain” Basic delivery + Industrial design + Ease of use, automation, feedback Products Asthma/ COPD in DK + Connectivity + Service Unmet Needs to Explore Force reduction Dose counting pMDI Breath actuation Trainer, integrated/stand - alone Dose confirmation, dose registration Dose confirmation, dose registration, wireless connectivity Services Dose counting Trainer, integrated/stand - alone DPI Dose confirmation, dose registration Dose confirmation, dose registration, wireless connectivity ” Our innovation strength ... ... becomes your competitiveness” 8 Services - Confidential - Food for Thought ... To be competitive in a future cost-pressured market, the drug itself is not enough. Means for assuring that the drug gets timely to where it work will be essential to be a winner The pharmaceutical industry should increase their focus on the device and re-think the cost structure in an end-to-end setting Other high value therapies with high DCT might pave the way for new thinking, like it is happening in the injection field ” Our innovation strength ... ... becomes your competitiveness” 9 - Confidential - Thanks for listening ... Morten Nielsen CEO Bang & Olufsen Medicom a/s Gimsinglundvej 20 DK-7600 Struer DENMARK Tel: Mobile: +45 70 30 16 00 +45 20 75 37 01 E-mail: [email protected] LinkedIn:www.linkedin.com/in/mortennielsen ” Our innovation strength ... ... becomes your competitiveness” 10 What Makes Inhalation Clinical Trials Special? Lars Borgström, Ph.D. Lund [email protected] The short answer: The way of administration . . . and a longer one: Inhaled medication Device (unfilled) Formulation (for filling) Mechanical aerodynamic Physical chemical Product properties 2012-10-18 Lars Borgström, Clin Pharm, Lund 3 Inhaled medication Device (unfilled) Formulation (for filling) Mechanical aerodynamic Physical chemical Patient behaviours & patient properties Product properties Inhalation technique Throat geometry Lung deposition 2012-10-18 Lars Borgström, Clin Pharm, Lund 4 Types of clinical studies • • • • Lung deposition, local pharmacokinetics Systemic pharmacokinetics Clinical effect Bioequivalence LUNG DEPOSITION Pharmacokinetics of inhaled medication Lung deposition Vena porta Liver Gut Systemic circulation Metabolism Borgström and Nilsson, 1990, Pharm Res, 7:1068‐1071 Pharmacokinetics of inhaled medication Lung deposition Charcoal Vena porta Liver Gut Systemic circulation Borgström and Nilsson, 1990, Pharm Res, 7:1068‐1071 Charcoal block: substances • Terbutaline is hydrophilic. Systemic availability after charcoal block was 0.3%. – – • Budesonide is lipophilic. Systemic availability after charcoal block was 2.6%. – – • Systemic availability without charcoal block is around 10%. Thus, 97% of the orally ingested drug was adsorbed on the charcoal. Systemic availability without charcoal block is around 13%. Thus, 80% of the orally ingested drug was adsorbed on the charcoal. Formoterol has an intermediate lipophilicity. No formoterol could be detected in urine after oral administration and charcoal block. – Thus, close to all orally ingested drug was adsorbed on the charcoal. • Degree of adsorption needs to be validated for each substance under study. Borgström and Nilsson, 1990, Pharm Res, 7:1068-1071 Thorsson, Edsbäcker and Conradson, 1994, Eur Respir J. 7:1839-1844 AstraZeneca, data on file. Typical lung deposition values • Pressurised metered dose inhalers (pMDI): 10 to 20 % of nominal dose • Dry powder inhalers (DPI): 10 to 30 % of nominal dose. • Small volume nebulisers: 30 to 40 % of nominal dose • Thus a large variation. Inhalers do differ!! • Each device must be judged on its own merits • A DPI ≠ DPI • A pMDI ≠ pMDI Systemic pharmacokinetics • The systemic pharmacokinetics can be obtained in the same way as for orally given medication. • With an intravenous infusion as the reference. Fluticasone Budesonide Harrison, T W et al. Thorax 2003;58:258‐260 Disease may influence the balance between absorption and mucociliary clearance differently for different drugs and different formulations. Smoking may influence the rate of absorption of drugs from the lung: inhaled terbutaline smokers Same AUC (Area Under the Curve) Different Cmax non-smokers Schmekel B, Borgström L, Wollmer. 1991 Schmekel B, Borgström L, and Wollmer P. Thorax 1991; 46:225‐228 CLINICAL EFFECTS Clinical effects • The desired clinical effect is in most cases local. • The undesired clinical effect is in most cases systemic. Can also be local. • Systemic availability does not reflect lung availability • Thus, both local and systemic effects, and side effects, needs to be evaluated. Clinical effects • Measured by relevant clinical effect studies applying the usual treatment length and group size calculations. Inhalation for systemic treatment • Use the same approach as for ”Inhalation for local treatment” but with a focus on systemic effects/side effects. • Regional deposition can influence the rate and degree of absorption, and thus the resulting systemic effect. BIOEQUIVALENCE Bioequivalence is defined as: • “ . . . the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of action . . . “ • A statement about doses. • AUC and Cmax. • 0.8 – 1.25; 2‐sided 90% conf. interval • Systemic concentrations FDA, 2003, orally administered drugs Bioequivalence studies • Applied in evaluating formulation changes during development. • Applied by ”generic” companies to compare their own formulation with innovator formulation. • If new formulation found bioequivalent with innovator formulation the new formulation can be declared therapeutically equivalent with innovator formulation. Bioequivalence Two formulations in two different studies. Values given as AUC‐ratios. Mean AUC‐ratio Two‐sided 90% confidence interval Study I 1.18 1.13‐1.24 Study II 1.14 1.07‐1.22 Both studies showed a significant difference in AUC between the formulations. Both studies showed that the formulations were bioequivalent with regard to AUC AstraZeneca, data on file Estimates of bioequivalence Study A Bioeq. interval 80% 100% Study B 125% Both studies A and B outcomes indicate bioequivalence. Bioequivalence, inhaled medication • “ . . . the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of action . . . “ • Both the local and the systemic exposure should be evaluated. • AUC and Cmax • 0.8 – 1.25; 2‐sided 90% conf. Interval • This means that both the local and the systemic comparison needs to fulfil the BE criteria. • For two‐combination products all four comparisons need to fulfil the BE criteria. Design of clinical effect studies for therapeutic equivalence • In analogy with the in vivo PK studies both the desired local effects and the undesired systemic effects needs to be evaluated. • Two dose levels for at least the reference formulation need to be included. Also for combination products. • Failure to show a significant difference in clinical effect between the two dose levels renders the study inconclusive. The same situation as for other administration forms. Estimates of equivalence based on therapeutic ratio Study A Equivalence interval X% 100% Study B Y% The goal posts X and Y has to be agreed with the regulatory agencies before study start. Both studies A and B outcomes indicate therapeutic equivalence. Turbuhaler vs. pMDI 140 FEV (% of baseline) 1 TBH 0.50 TBH 0.25 pMDI 0.50 pMDI 0.25 120 100 0 1 2 3 4 Hours since dose administration Borgström et al. Am J Resp Crit Care Med, 1996, 153: 5 6 Thank you for your attention! 1 Evaluation of inhalation devices using human-like in vitro approaches Mårten Svensson and Elna Berg, EMMACE Consulting AB Dennis Sandell, S5 Consulting 2 Outline • • • Analytical testing on inhalation products Pharmacopeia – how to perform the tests More patient-like testing - improving the in-vitro in-vivo correlation • • • Which parameters are important? Experimental approaches Examples 3 Unique analytical tests for inhalation products • • • • • Delivered dose uniformity (through inhaler life) Aerodynamic characterisation (quality of the aerosol cloud) Spray pattern Plume geometry Droplet size distribution 4 Aerodynamic aerosol characterisation • Aerodynamic characterisation (quality of the aerosol cloud) • • • Impactors are extensively used Fractionating the aerosol particles based on their aerodynamic size How particles behave in different air flow pattern (eg lung geometry) 5 Aerodynamic aerosol characterisation • Air flow according to Pharmacopeia • • • • pMDI: 30 lpm (NGI), 28.3 lpm (Andersen) Nebulizers: 15 lpm DPI: flow that produce a pressure drop of 4 kPa over the inhaler, eg 30-100lpm Air volume : 4 litres 4 kPa 6 Aerodynamic aerosol characterisation • Impactors, different types available (decribed in Pharmacopeaia) NGI Twin Impinger MLI MMI Andersen 7 Quality control vs prediction of In-vivo • The purpose of many of the tests is to control the quality of the product • The tests not necessarly good prediction tools for InVivo outcomes More sophisticated tools are available! 8 In-Vivo predicting tools • Two parameters are recognized important when establish better IVIVC: Throat geometry variation Inhalation flow variation flow flow time time 9 The inhalation profile – the standard approach • With the pharmacopeia set-up • • A square-wave air flow profile Possibility to vary: • Acceleration in the beginning (Flow Inspiratory Rate, (FIR)) • Maximum Flow, Plateau value (Peak inspiratory Flow, (PIF)) • Volume Air Flow PIF FIR Volume Time 10 The inhalation profile – Lung Simulators Weuthen, T. et. al., J. Aerosol Med., 15(2002) 297-303 Kamin, W.E.S. et. al., J. Aerosol Medicine, 15(2002) 65-73 Burnell, J. Aerosol Sci. Vol 29, no 8, p1011, 1998 11 Inhalation profiles – Mixing Inlet concept • • Whole dose analysed Impactor at fixed flow OP model • • Fairly simple Commercially available Piston Pressurised air Next Generation Impactor Mixing Inlet Vacuum Bo Olsson, RDD 2008 12 Throat inlets – Pharmacopeia throat Pharmacopeia throat 13 Anatomical throat models Alberta idealized throat P. Byron group The OP consortium throats • Different flows and throats will induce variability in “lung dose” – What’s the meaning of that??? 14 Lung deposition: variability vs lung dose • • • Borgström, 2006, JAM vol 19, No 4, 473 If high lung deposition is wanted a low variability is required If you develop a product with high variability – you will never reach high lung deposition Different inhalation flows and different throat geometries will aid this process 15 Example 1 – AstraZeneca Lung Dep Bo Olsson, RDD 2008 DPI_A DPI_B 80 % of mean delivered dose (MDD) % of nominal delivered dose 90 70 60 90 80 70 60 DPI_A DPI_B 50 40 30 20 10 0 in vivo EOM FPD DM Mean dose passing throat predicted mean lung deposition for both DPIs 50 40 30 20 10 0 in vivo Lung deposition in vitro Dose passing throat 16 Example 1 – AstraZeneca Lung Dep Bo Olsson, RDD 2008 DPI_A DPI_B 80 % of mean delivered dose (MDD) % of nominal delivered dose 90 70 90 80 70 60 50 40 30 20 10 0 DPI_A DPI_B in vivo EOM FPD DM Similar in vivo and in vitro variability by using OPC throats with different flows 60 50 40 30 20 10 0 in vivo lung deposition in vitro impactor deposition 17 Example 2 - pMDI versus DPI • Fixed flows, different OPC throats Förslag EB Example 3 – Asmasal Clickhaler • • • Filtering capacity differ at 4 kPa, but not at 2 kPa (p = 0.03) The smaller the cast, the more is captured in the cast Low product variability? 19 Example 4: Design of clinical studies • Design of clinical studies of your novel drug/product Pharmacopeia 4 kPa, cylinder throat Data from Emmace lab on two salbutamol (100µg) DPIs 20 Example 4: Design of clinical studies • Design of clinical studies of your novel drug/product Pharmacopeia 4 kPa, cylinder throat Variability Different throats and flows Will the clinical study be successful….? Data from Emmace lab on two salbutamol (100µg) DPIs 21 Example 4: Design of clinical studies • Design of clinical studies of your Generic Pharmacopeia 4 kPa, cylinder throat Variability Different throats and flows Data from Emmace lab on two salbutamol (100µg) DPIs 22 Example 4: Design of clinical studies • Design of clinical studies of your Generic Pharmacopeia 4 kPa, cylinder throat Variability Different throats and flows Data from Emmace lab on two salbutamol (100µg) DPIs Will the bioequivalence between Product 1 and Product 2 be successful….? 23 Summary • • In-Vivo realistic testing tools of inhalers are available today Using different inhalation flows (weak to strong) and different throat geometries (e.g. small to large) offer: • A guiding tool in product development Low lung dose variability in human population is a prerequisite for high lung deposition • Design input to clinical studies (new product and bioequivalence) 24 Thank you for your attention Biological Material – Your Treasure Gun Persson, CEO Helene Sonesson, CFO MVIC Symposium, Medicon Village, Lund‐Sweden, 17 October 2012 To reach the market… in time… Correct decisions must be made today! Today… • One substance – Many companies • Biological materials ‐ Not always kept • To have processes ‐ Cost • Legal demands ‐ Difficult to understand?! Tomorrow’s challenges! • Competition increases… ‐ Time to market ‐ Quality ‐ Global co‐operation • Legal demands will change and differ from country to country Biological material will be one key… The product’s sustainability from theory to practice • Research costs ‐ important to ensure that investments are sustainable • The clinic is not like normal clinical studies show Biological Material gives opportunities! • Correct biomaker gives power • Possibility to extend research… ‐ investigate AEs ‐ new biomarkers ‐ new indication ‐ multiple drugs To the market… Pre‐ Clinical Clinical Chain of Custody for samples On Market The Reality… Chain of Custody for samples Three major foundations Feasible Legal demands Quality Assurance What and How to do… Right thing Wrong way Wrong thing Right way Wrong thing Wrong way RIGHT THING RIGHT WAY AT THE RIGHT TIME Conclusion Biological Material… • • • • A company’s treasure Lasts longer than a study or program Possibilities for evidence & extended research Important for investors If you have global processes in place, it helps… • • • Your chain of custody You to get what you want You to get where you want We can promise ‐ this will save you time & money! Biological Material Your Treasure Treat it as it deserves! www.nordicbiocube.com Platinum sponsors Gold sponsor CI Informatics Ltd. Nolato MediTech Silver sponsors Oxford Lasers Pharmaterials Ltd Det Medicinska Malmö ExIS AB Epsilon AB QSCL Q Scientific Consulting Organizing committee Orest Lastow Karin von Wachenfeldt Charlott Brunmark Stefan Ulvenlund Martina Kvist Reimer Kia Rönngard Towa Carlsson Caroline Formby Sture Carlbom Jessica Lastow Thank you for attending and see you all next year 2nd Medicon Valley Inhalation Symposium 16 October 2013 09.00–17.00 Medicon Village, Lund, Sweden inhalationsymposium.com