Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 76
HEALTH POLICY AND PLANNING; 15(1): 76–84
© Oxford University Press 2000
The impact of financing and quality changes on health care
demand in Niger
MUKESH CHAWLA1 AND RANDALL P ELLIS2
1Department of Population and International Health, Harvard School of Public Health, Boston, MA, USA and
2Department of Economics, Boston University, Boston, MA, USA
This paper assesses the demand effects of a cost recovery and quality improvement pilot study conducted
in Niger in 1993. Direct user charges and indirect insurance payments were implemented in government
health care facilities in different parts of the country, and were preceded or accompanied by quality changes
in these facilities. Decision-making by patients is modelled as a three-stage process of reporting an illness,
seeking treatment and choice of provider; and multinomial nested logit techniques are used to estimate the
parameters of the decision-tree. Overall, the results give a reasonably favourable impression of the policy
changes. In neither case is there evidence of serious reductions in access or increases in cost. Particularly
notable is that despite an increase in formal user charges, the observed decline in rates of visits is statistically insignificant, suggesting the success of measures to improve quality of health care in public facilities.
The observed increase in the probability of formal visits in the district with indirect payments is also striking. Both contrast with the control region of Illela, where neither user charges were introduced nor were any
efforts made to improve quality. The data suggest that higher utilization of formal care, probably due to
improvements in quality, outweighed the decrease in utilization that may have come about due to introduction of cost recovery, so that the net effect of the policy changes was an increase in utilization. Quality considerations appear to be important in ensuring the long-term success of cost sharing.
1. Introduction
Constrained economic circumstances and stagnant growth of
the health sector have led many developing countries to consider cost recovery as a means of financing health care production. This paper assesses the impact of an experiment in
health care cost recovery, preceded or accompanied by
quality improvements, conducted in three districts in Niger.
Using a model of the illness and treatment-seeking process,
we analyze and discuss the policy implications of the results.
In May 1993, cost recovery was substantially augmented in two
of the three study districts in Niger.1,2 In Say district, a direct
method of payment was implemented for outpatient treatment
at government facilities, with charges of 200 FCFA (equivalent
to US$0.66 at the time of the test) per episode of treatment for
adults and 100 FCFA ($0.33) per episode for children under 5
years. In Boboye district, over 100 km east of Say, an indirect
method of payment was implemented. Revenues were generated primarily through a regional tax of 200 FCFA per household, earmarked specifically for financing health care, with
moderate fees of 50 FCFA ($0.16) per episode of treatment for
adults and 25 FCFA ($0.08) for children. The revenues so
generated in Boboye, from fees and taxes, were pooled at the
district level to create a district fund that was managed by
health committees comprising representatives of the district’s
population.2 In both Boboye and Say, the handicapped,
schoolchildren, prisoners, soldiers and indigents were
exempted from paying the taxes and fees. The population
paying taxes and fees thus knew their contributions were being
used to finance health care. In Illela district, over 400 km
north-east of Say, existing low levels of cost recovery were
maintained, and the only sources of revenue for public health
facilities were traditional sources of government finance
(direct and indirect taxes and tariffs), not collected through the
health sector. Illela thus serves naturally as a control site.
It is important to note that in addition to the substantial
expansion of cost sharing, diagnostic-treatment protocols, the
availability of essential drugs and health management
systems were improved at government health facilities.3 In
Boboye region, improvements in diagnostic and treatment
protocols preceded the cost-recovery experiment by three
years, while in Say the two took place more or less simultaneously. Specifically, four interventions were implemented
to improve efficiency at public health facilities: 4 (1) improvement in drug availability; (2) training of health personnel in
the use of standard diagnosis and treatment protocols; (3)
strengthening management capacity; and (4) improving
supervisory and managerial capacity.
The observed changes in treatment patterns in the two
experimental districts can thus be attributed to both cost
recovery and the beneficial effects of facility enhancements.
The impacts that we document are those of the combined
effect of cost sharing and quality enhancements, not pure
demand or pure quality effects. Since there were no major
changes in either pricing policy or quality in the control site
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 77
Impact of cost-recovery on health care demand
of Illela district, we use data from Illela to infer how the introduction of price and quality improvements in Say and Boboye
affected demand.
Previous studies on the demand for health care have typically
found small price effects. In a study of demand for health care
in rural Malaysia, Heller5 found that total annual medical
visits were not significantly influenced by prices. Similarly,
Akin et al.6 also concluded that prices were not an important
determinant of demand for medical care in a rural region of
the Philippines. In a study of the demand for health care in
rural Cote d’Ivoire, Gertler and van der Gaag7 found the
utilization of health services to be price unelastic. In a study
that analyzes the determinants of demand for health care in
urban Bolivia, Ii8 found that though demand for medical care
is responsive to changes in prices, the price elasticities tend to
be very low.
Other studies have found that cost recovery has a negative
impact on utilization of health services. In a study of the effect
of a price increase in health facilities in Zaire, de Bethune et
al.9 found a decrease in utilization after an abrupt increase in
prices. Waddington and Enyimayew10 found a general fall in
health facility utilization following a price increase in the
Ashanti-Akim district in Ghana. Mwabu et al.11 estimated that
utilization of health facilities dropped by 38% during 1989–90
in the four facilities they examined, though Huber12 attributes
much of the drop in demand to insufficient use of exemptions.
However, there is some evidence of improvement in access to
health facilities following increases in both costs and quality of
care, as found by Litvack and Bodart13 in Cameroon.
The remainder of this paper is organized as follows. The data
used are introduced briefly in section 2. Section 3 discusses
the methodology, section 4 presents the results, and the paper
ends with a discussion in section 5.
2. The data
The analysis in this paper uses data from household surveys1–3
conducted both before and after the policy change, with an
interval of 12 months between the two. Data were collected
in the three districts of Say, Boboye and Illela, which were
chosen by the Ministry of Health, Government of Niger. The
first set of surveys was done in October–November 1992, 6
months before the introduction of the cost-recovery systems,
while the second surveys were carried out in October–
November 1993, 6 months after the intervention.
77
and 13 051 individuals (1836 households) were interviewed in
the second stage. Not all the households interviewed in the
first stage were interviewed in the second stage. This analysis
combines the data from the two sets of surveys in all three
study sites.
3. Methodology
Two statistical methods were used: univariate comparisons of
sample statistics across regions and over time, and a multivariate nested logit model of the decision process underlying
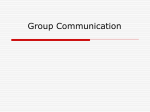
individual illness and treatment seeking. For the nested logit
specification, the decision tree modelled is as shown in Figure
1. Although usefully thought of as a sequential decision, the
assumed specification only imposes restrictions on the correlation structure of the error terms affecting different choices.
It is consistent with all stages of decisions being made simultaneously.14,15
The first stage of the decision tree is the decision to report an
illness. This first stage of the decision process is important in
order to distinguish whether observed changes in patterns of
treatment-seeking reflect differences in illness (possibly due
to environmental factors that are unrelated to the policy
change in the short run) or differences in treatment-seeking
behaviour once ill, which may be influenced by price and
quality changes. Although in the long run differences in rates
of illness could be due to changes in cost sharing and quality
at government facilities, in the short run significant changes
are unlikely. We model this stage as dependent upon individual and household level demographic variables, dummy
variables for the region in which an individual lives, average
price, travel time, and drug availability on dummy variables
for the policy changes in each region, and on a term called the
inclusive value, which picks up the expected utility of seeking
treatment should one report an illness.i
The second stage of the decision tree is the decision to seek
treatment from a formal provider or healer conditional on
reporting an illness. For this study, we define formal providers
to include hospitals, medical centres, medical posts, rural dispensaries, maternity hospitals and private clinics. Because the
use of private clinics is extremely rare in our sample (with
fewer than 25 cases in our sample of 27 357 individuals) we
The sampling criteria used was based on the population
Census of 1988, and data on the distribution of health facilities in Niger in 1988. Each of the selected districts was divided
into two parts: one part had a health facility, for which five
census districts (‘grappes’) were included, while the other
part had no health facility, for which 29 census districts were
included. A three-stage stratified cluster design was used to
select households in each of these census districts.
The surveys collected data on 612 households in each census
district in each of the two periods. A total of 14 410 individuals (1836 households) were interviewed in the first stage
Figure 1. The decision tree for the patient treatment-seeking
process
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 78
78
Mukesh Chawla and Randall P Ellis
were unable to model this choice separately. We chose
instead to group them together with the formal public facilities, even though they need not have changed prices in line
with the policy experiment. ‘Informal providers’ are defined
to include traditional practitioners (healer) and ‘others’
(which include friends, other relatives, and pharmacies).
Because both formal and informal treatment at home (i.e.
treatment by persons other than family members) are relatively rare, and many people treated at home also receive
treatment outside of the home, we did not attempt to model
home treatment separately from treatment outside the home.
Hence for this study the decision to ‘seek treatment’ includes
the possibility of having a formal provider (i.e. doctor,
midwife or nurse) or informal provider (traditional healer or
‘other’) treat the patient in his or her home. Treatmentseeking behaviour is modelled similarly to the illness reporting decision, as depending upon the same set of demographic
variables, average price, drug availability and waiting time,
regional dummies and pre- and post-policy-change dummy
variables. We also include an inclusive value that captures the
expected value of treatment by formal and informal providers.
The third stage of the decision tree is the decision to seek
formal rather than informal treatment. A sizeable proportion
of the population in all districts paid and visited traditional
healers and other informal providers, hence any change in the
rates of treatment by these informal providers is important in
understanding the total financial burdens on individuals.
Variables included in this last stage are the same as for the
previous two stages.
4. Results
Base line survey results
From May through October 1992, baseline surveys were conducted in 1813 households containing 14 359 individuals.
Summary numbers from these household surveys are shown
in Table 1. The three districts show considerable similarity in
many demographic variables, with virtually identical averages for age, proportion male, marital status and levels of
secondary education. The three districts do differ in several
dimensions. Household sizes are smaller in Illela than the
other two districts, and our income measure (average estimated monthly consumption expenditures) is slightly lower
in Illela and higher in Boboye than the sample average.
Although days of illness are similar in the three districts, both
the percentage reporting illness in the base period and the
percentage seeking treatment are significantly lower in Say in
the base period. Treatment in the formal sector is quite rare
in all three districts, with only 2.7% of individuals seeking
treatment from a formal provider in the base period. Our
price measure was highest in Illela (1951 FCFA), relative to
Say (679) and Boboye (792). Reported drug availability was
similar in Say and Boboye, and slightly worse than in Illela,
before the policy change. Travel times were slightly worse in
Say than in Illela and Boboye.
Overall, the three regions were broadly similar prior to the
policy changes, although the Say sample appears to be slightly
healthier and that of Boboye slightly sicker than the control
site of Illela. Bearing these initial differences in mind, the
Table 1. Sample characteristics in districts of Say, Boboye and Illela, Niger, before policy change, all individuals
Number of individuals
Income (’000 FCFA)
Reported illness
Days ill
Seeking treatment
Treatment at home
Treatment outside home
Treatment by healer
Formal treatment
Total expenditures on illness
Price/1000
Drug availability
Travel time
Say
Boboye
Illela
Total
4685
12.95
(13.8)
0.1372
(0.344)
11.19
(10.6)
0.0783
(0.268)
0.0156
(0.123)
0.0201
(0.140)
0.0094
(0.096)
0.0188
(0.135)
396.5
(1400.0)
0.679
(1.089)
2.03
(0.568)
149.0
(109.0)
5566
14.97
(18.41)
0.2432
(0.4291)
11.301
(10.36)
0.1886
(0.3913)
0.0099
(0.0989)
0.0456
(0.2087)
0.0129
(0.1130)
0.0377
(0.1906)
788.3
(2540.0)
0.792
(0.764)
2.05
(0.537)
122.0
(79.7)
4108
11.57
(12.95)
0.2186
(0.4133)
1.98
(10.41)
0.1188
(0.3236)
0.0088
(0.0932)
0.0314
(0.1744)
0.0122
(0.1097)
0.0241
(0.1534)
795.0
(2863.0)
0.1951
(2.983)
2.38
(0.420)
123.0
(83.2)
14 359
13.34
(15.61)
0.2016
(0.4012)
11.36
(10.44)
0.1326
(0.3392)
0.0114
(0.1062)
0.0332
(0.1792)
0.0115
(0.1069)
0.0276
(0.1639)
662.5
(2350.0)
0.1087
(1.860)
2.14
(0.539)
130.9
(92.1)
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 79
Impact of cost-recovery on health care demand
79
Table 2. Sample characteristics in the districts of Say, Boboye and Illela pre- and post-policy change, individuals seeking treatment only
Number of individuals
Treatment at home
Treatment outside home
Treatment by healer
Formal treatment
Price/1000
Drug availability
Travel time
Say
––––––––––––––––––––––––––––
pre
post
Boboye
––––––––––––––––––––––––––––
pre
post
Illela
––––––––––––––––––––––––––––
pre
post
367
0.1717
(0.3776)
0.2343
(0.4242)
0.1008
(0.3015)
0.2262
(0.4189)
0.794
(1.080)
2.08
(0.545)
129
(112.0)
1050
0.0505
(0.219)
0.2371
(0.4255)
0.0648
(0.2462)
0.1981
(0.3988)
0.864
(0.790)
2.01
(0.507)
118
(82.7)
488
0.0697
(0.2549)
0.2561
(0.437)
0.0984
(0.2982)
0.1947
(0.3964)
2.101
(2.737)
2.3
(0.40)
127
(85.6)
514
0.1226
(0.3283)
0.2043
(0.4036)
0.0661
(0.2488)
0.2082
(0.4064)
0.685
(1.151)
2.35
(0.412)
139
(0.103)
sample provides a nice setting for a controlled experiment for
the impact of the two forms of cost sharing.
Descriptive comparison of policy impact in the three
districts
Table 2 provides summary statistics of key variables before
and after the policy changes in each of the three regions for
all individuals seeking treatment of any kind. The first
numbers to notice are the large changes in the number of
people seeking treatment of any kind. In Say, where a direct
form of payment was implemented, the number of people
seeking treatment increased by 40%, from 367 to 514 individuals. In Boboye, where predominantly indirect payment
was implemented, the number seeking treatment declined by
26%, from 1050 to 778 individuals. In the control site of Illela,
the number seeking treatment increased by 9%, from 488 to
532 individuals.
The percentage seeking treatment at home only was highest,
but declined most sharply, in Say (17% pre, 12% post). In
Boboye it fell marginally (5% pre and 4% post) and rose marginally in Illela (7% pre and 8% post). The percentage
seeking treatment from formal providers decreased from 23
to 21% in Say, increased from 20 to 23% in Boboye, and fell
sharply in the control region of Illela, from 19 to 12%. The
average price of formal treatment fell in each of the three
study regions, with Say recording a fall of 14%, Boboye 36%
and Illela almost 66%. Drug availability rose substantially in
Boboye, followed by Say, but fell in Illela. Travel time
increased marginally in Boboye and Say, and fell marginally
in Illela.
The descriptive data provide some insights into the changes
in access, use of formal providers and prices – although for a
variety of reasons, it would be hasty to attribute these changes
entirely to cost recovery and quality improvement in the facilities.ii First, since the percentage of population seeking care
778
0.0373
(0.1896)
0.2429
(0.4291)
0.0373
(0.1896)
0.2301
(0.4212)
0.553
(0.667)
2.64
(0.271)
121
(80.0)
532
0.0771
(0.2669)
0.1561
(0.3632)
0.695
(0.2546)
0.1241
(0.3299)
0.717
(1.266)
2.20
(0.58)
125
(83.1)
from a formal provider is very small to begin with (about
2.7% in the base period), it is unlikely that any government
policy changes in the formal sector would bring about a
marked change in the overall treatment-seeking behaviour in
a 1-year period. Second, other factors affecting treatmentseeking behaviour could have changed in the year between
the preliminary baseline survey and the final survey, though
it is unlikely that such changes could affect behaviour in a
period as short as one year.
We note that between the baseline and final survey years, the
number of patients seeking any form of treatment fell by 4%,
with this fall being recorded in Boboye district only. Of all the
three districts, the percentage of patients seeking treatment
from formal providers increased solely in Boboye district,
where an indirect payment system was introduced, despite
the fact that quality improvement in the form of increased
drug availability was recorded in both Say and Boboye. Like
Say, Boboye also recorded a fall in the percentage of patients
seeking treatment at home. In contrast, the control region of
Illela experienced an increase in the percentage of patients
seeking treatment at home, and a fall in the percentage of
patients seeking treatment from formal providers. Notwithstanding the caveat mentioned in the preceding paragraph, all
these results are too consistent with the changes in cost recovery and quality protocols in the three districts for us not to
relate government policy changes to treatment-seeking
behaviour.
Finally, we find it striking that the average price of formal
treatment went down in each of the three study regions, even
in Say where the policy change was to increase prices at the
public facilities. We note that even the new fees charged in
Say (200 FCFA per episode for adults, 100 FCFA for children) were well below the average reported payments in Say
and Boboye even before the policy intervention. One probable explanation is that substantial payments were being
made for medicines and consultations by formal providers
10 Chawla (jl/d)
11/2/00 3:15 pm
80
Page 80
Mukesh Chawla and Randall P Ellis
Table 3. Nested logit results for the treatment-seeking process (t-statistics in parenthesis)
Household size
Old age
Adult
Sex: male
Married
Secondary school
Non-Zarma
Household income
Say district
Boboye district
Price/1000
Drug availability
Travel time
Price*Income
Travel time*Income
Drug availability*Income
Say district*Post dummy
Boboye district*Post dummy
Illela district*Post dummy
Inclusive value
Log-likelihood
Sample size
a
Reporting illness
Seeking treatment
–0.0366a
(10.398)
0.106
(1.659)
–0.399a
(7.996)
–0.888a
(3.878)
0.300a
(5.964)
–0.0291
(0.212)
–0.0360
(0.747)
0.000315
(0.069)
–0.547a
(8.837)
0.244a
(3.019)
0.0160
(1.250)
–0.136a
(3.192)
0.000287
(0.875)
0.00197a
(2.532)
0.0000233b
(1.879)
0.0469a
(2.443)
0.473a
(7.910)
–0.250a
(4.537)
0.119b
(1.854)
–0.140
(0.897)
–13 607.54
–27 357
–0.00483
(0.699)
0.330a
(2.797)
–0.0304
(0.284)
–0.0241
(0.080)
–0.0873
(0.839)
0.367
(1.008)
–0.338a
(3.678)
–0.0236a
(2.423)
–0.0456
(0.404)
0.818a
(6.597)
–0.0724a
(2.722)
0.0300
(0.365)
0.000464
(0.648)
0.00496a
(2.571)
0.0000363
(1.190)
0.0133a
(3.086)
0.122
(1.099)
0.120
(1.008)
0.292a
(2.781)
–1.542a
(3.789)
–3 348.64
15 618
Formal versus informal
0.00972
(1.058)
–0.284a
(1.587)
–0.0298
(0.187)
0.438
(1.299)
0.131
(0.829)
0.314
(1.079)
–0.0942
(0.798)
0.00782
(0.828)
0.0584
(0.307)
–0.290b
(1.576)
–0.0141
(0.348)
–0.298a
(2.569)
–0.0123a
(11.714)
0.00131
(0.686)
0.00000790
(0.193)
–0.00168
(0.406)
0.0607
(0.343)
0.556a
(3.834)
–0.605a
(3.103)
–1 593.70
–3 722
Significant (t > 2); b weakly significant (2 > t > 1.5).
before the introduction of user fees and insurance systems,
even though the public system was in principle free. With the
improvements in drug availability pursuant to the quality
improvements, the fall in average price may well be picking
up a saving in expenditure on drugs. Thus, average prices fell
markedly in Boboye, the district that recorded the highest
improvement in drug availability. We cannot, however,
explain the big fall in prices in Illela.
Results from a logit model of the decision process
The preceding analysis has identified major patterns of treatment and change using univariate comparisons of means. In
this section we report the results of estimating a discrete
choice (logit) model of the decision process underlying treatment decision.
Results from the three-stage nested logit model are presented
in Table 3. The decision to report an illness is modelled in the
first stage of the decision tree, where the choice is ‘reporting
an illness’.iii Individuals belonging to large families are less
likely to report an illness, as indicated by the negative and significant coefficient on household size. Married people and
females are more likely to report an illness. Ethnic group is
not a significant predictor of illness. The coefficients on
income, price, drug availability and travel time cannot be
used to infer their effect on the probability of reporting an
illness because the model also includes interactions between
income and the price, drug availability and travel time variables. We note that the coefficient on drug availability alone,
and price interacted with income, are each significant, suggesting that there is a relationship between these three variables and reporting an illness. Even after controlling for
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 81
Impact of cost-recovery on health care demand
demographics and observed prices and drug availability, the
two district dummies for Say and Boboye are statistically significant. The probability of illness being reported is negative
and significant in the district of Say, while the reverse holds
for Boboye. These coefficients changed significantly after the
new payment system was introduced in Say and Boboye,
perhaps picking up the impact of unobserved changes in facility quality not captured in our drug availability measure. Consistent with the absence of any changes in the structure of
delivery in Illela, there was no change in the probability of
reporting illness in the control region of Illela. The coefficient
on the inclusive value is statistically insignificant, suggesting
that the decision to report an illness is independent of
whether the individual seeks treatment for this illness.
The decision to seek treatment conditional on reporting an
illness is modelled in the second level of the decision tree,
where the choice variable is ‘seeking treatment’ versus ‘not
seeking treatment’. Consistent with the results found in Ellis
and Mwabu,14 few of the demographic variables are statistically significant. Older people are more likely to seek treatment when ill than adults or children, and non-Zarma ethnic
groups are less likely to seek treatment. The coefficient on
price is negative and statistically significant, and the interaction term between income and price is positive and significant. Together these two parameters indicate that individuals
from families with high incomes are less responsive to prices
than individuals from families with low incomes. The income
variable, not interacted with any others, is significant and
negative, but cannot be easily interpreted in the presence of
the interaction terms. We defer a discussion of income until
the next section where we use simulations to identify
meaningful patterns. The coefficient on the inclusive value is
negative and significant. This implies that individuals that are
more likely to use formal treatment are less likely to seek any
treatment, which is contrary to expectations but not implausible.
The third level of choice modelled is between formal and
informal treatment, with the choice variable being ‘formal
81
treatment’. Perhaps in part because the sample size is smaller
than in the previous stages, none of the individual demographic variables are significant. The price term is negative,
and the price–income interaction term is positive, both as
theory would predict, but the coefficients are statistically
insignificant. Drug availability is negative, and the coefficient
on the interaction term between drug availability and income
is also negative but insignificant. In Boboye, where an indirect
payment system (tax) was introduced, the region–period
interaction variable has a significant positive coefficient, indicating a shift toward formal treatment. The Illela district
dummy interacted with the post-period dummy is negative
and significant, suggesting a shift away from formal treatment
in the region even after controlling for prices and drug availability. Together the three regional–time period interaction
dummy coefficients suggest that the cost recovery/quality
enhancements in Say and Boboye had modest negative and
positive effects on seeking formal treatment, while the
control region experienced a sharp decline in rates of formal
treatment.
Simulation results
As highlighted in the previous section, the income, price, drug
availability and travel time results from nested logit models
are not readily interpreted in terms of their policy significance. Therefore, we used the estimated parameters from our
three-stage nested logit model to simulate the probabilities of
each of the three decision stages. Results from our simulations are shown in Tables 4, 5 and 6. These simulations are
based on a hypothetical individual with average characteristics for all variables except for the variables being simulated
in each part of the table. The indirect effects of the variables
through the inclusive values are taken into account in the
simulations. Comparisons of the probabilities can be used to
assess the magnitude of the policy impacts and how individuals of different incomes were affected. For each simulation, we used the 10th, 50th and 90th percentiles of the
variable of interest. Hence, as shown in Table 4, we simulated
probabilities for income levels of 2300, 7800, and 28 800
Table 4. Simulated probabilities of seeking formal treatment conditional on seeking any treatment: income level and price
Income percentile
Level
Income (’000 FCFA)
10th
2.3
Median
7.8
90th
28.8
Probability of seeking treatment conditional on reporting illness
Income (’000 FCFA)
10th
2.3
Median
7.8
90th
28.8
Probability of reporting illness
Income (’000 FCFA)
10th
2.3
Median
7.8
90th
28.8
Price
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
10th percentile
50th percentile
90th percentile
2
11.1%
11.3%
12.4%
317
11.0%
11.3%
12.5%
2568
10.8%
11.2%
13.1%
2
52.3%
53.9%
59.9%
317
51.9%
53.7%
60.4%
2568
48.5%
51.8%
64.1%
2
23.4%
23.8%
25.5%
317
23.5%
24.0%
26.0%
2568
24.3%
25.3%
29.3%
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 82
82
Mukesh Chawla and Randall P Ellis
Table 5. Simulated probabilities of seeking formal treatment conditional on seeking any treatment: income level and drug availability
Income percentile
Level
Income (’000 FCFA)
10th
2.3
Median
7.8
90th
28.8
Probability of seeking treatment conditional on reporting illness
Income (’000 FCFA)
10th
2.3
Median
7.8
90th
28.8
Probability of reporting illness
Income (’000 FCFA)
10th
2.3
Median
7.8
90th
28.8
Drug availability
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
10th percentile
50th percentile
90th percentile
1.63
13.0%
13.5%
15.3%
2.29
10.9%
11.3%
12.6%
3.0
9.0%
9.2%
10.1%
1.63
50.0%
51.0%
54.8%
2.29
51.0%
53.2%
61.5%
3.0
52.1%
55.6%
68.2%
1.63
25.3%
25.9%
28.4%
2.29
23.7%
24.3%
26.7%
3.0
22.0%
22.6%
25.0%
Table 6. Simulated probabilities of seeking formal treatment conditional on seeking any treatment, pre- and post-policy change, by income
Income percentile
Level
Say
–––––––––––––––––––––––––
pre (%)
post (%)
10th
2.3
11.3
11.1
Median
7.8
11.6
11.4
90th
28.8
13.1
12.6
Probability of seeking treatment conditional on reporting illness
10th
2.3
53.5
51.3
Median
7.8
55.6
53.8
90th
28.8
63.3
62.4
Probability of reporting illness
10th
2.3
22.8
31.2
Median
7.8
23.4
31.8
90th
28.8
26.0
34.5
FCFA, and prices of 2317 and 2568 FCFA. In Table 5 we simulated the probabilities for income percentiles and for percentiles of average drug availability by grappe: 1.6, 2.3 and
3.0. Table 6 shows how the gross impact of the policy changes
affected each income level in each of the three districts,
taking into account changes in average prices, drug availability and the post-policy-period dummy variables.
The simulations in Table 4 summarize the interactions
between price and income on the three decisions: reporting
illness, seeking treatment and seeking formal treatment. The
first part of the table indicates that neither price nor income
seem to have much of an impact on the decision to seek
formal treatment conditional on seeking any treatment. Probabilities range from 10.85 for a high price, low income probability to 12.4% on the low price, high income simulation. The
second part of Table 4 indicates that the probability of
seeking any treatment is more responsive to prices and
income levels. The simulations suggest an approximate 7.5%
increase in the probability of seeking any treatment as income
Boboye
–––––––––––––––––––––––––
pre (%)
post (%)
Illela
–––––––––––––––––––––––––
pre (%)
post (%)
10.4
10.7
12.2
15.7
16.1
17.8
12.3
12.7
13.0
6.6
6.8
6.9
50.4
52.5
60.3
54.5
56.7
65.2
49.9
51.9
59.8
58.2
60.4
68.4
24.9
25.6
28.3
19.8
20.3
22.3
23.8
24.4
27.1
25.1
25.7
28.1
varies, and an approximate 4% increase as the price is
increased. Changes in price responsiveness are striking: for
low income levels, the probability of seeking any treatment
declines as prices are increased, while for high income levels,
the probability is predicted to increase with prices. Although
contrary to usual economic theory, this is consistent with
inadequately controlling for facility quality variation, which
may be correlated with prices and highly desired by highincome individuals.
The bottom half of Table 4 presents simulations for the
probability of reporting treatment. Consistent with expectations, this probability is virtually unaffected by prices, but
increases modestly with income.
Table 5 presents a similar set of simulations for various levels
of drug availability, each considered for three income levels.
The probability of seeking formal treatment is negatively
related to the average drug availability, and does not show a
meaningful difference in responsiveness across income levels.
10 Chawla (jl/d)
11/2/00 3:15 pm
Page 83
Impact of cost-recovery on health care demand
Drug availability has a large effect on the decision to seek
formal treatment, and causes nearly a 14% increase in the
probability of seeking any treatment for the highest income
level, versus only a 2.1% difference for the low income level.
Income and drug availability predict a difference of more
than 18% in the probability of seeking any treatment. The
final section of Table 5 indicates that higher drug availability
appears to reduce the rate of reported illness, with an
approximate 3% reduction in the probability of reporting
illness at a 90th versus 10th percentile level of drug availability.
Table 6 summarizes the total impact of the policy change,
including changes in prices, drug availability and unobserved
variables captured by the district-level dummies interacted
with the post-period dummy. This table provides the best
picture of the overall impact of the policy changes on individuals with different household incomes, holding constant
all other observed characteristics. The first part of Table 6
indicates that the probability of seeking formal care conditional on seeking any care was virtually unchanged for all
income levels in Say, increased approximately 5% in Boboye,
and decreased approximately 6% in Illela. In each district the
reduction in use of formal treatment when any treatment is
sought is relatively independent of income levels.
83
residents of Boboye in terms of a moderate fee-for-service
and an indirect tax specifically earmarked for financing health
care. This result could have been brought about by one or
both of the following reasons. First, the policy changes also
included significant quality enhancements which, in the case
of Boboye, began three years before the changes in health
care financing were implemented. The quality-improvement
initiatives included increased drug availability as well as
improved management, supervision and training. The probability of visiting formal providers is likely to have been positively affected by these quality enhancements. Secondly, after
incurring an ex-ante fixed cost in terms of the indirect tax, the
marginal cost of 50 FCFA per visit to a formal provider is low,
and demand is likely to increase irrespective of any other
changes that might have taken place. In absence of complete
data on the quality variables and on out-of-pocket expenditures before the policy changes, we are unable to unequivocally attribute the higher utilization rates to either the quality
effect or to the moral hazard effect; both of these could potentially have brought about the observed increases in visits to
formal providers. In any case, the observed changes in rates
of visits were not due to changes in reported illness, which
actually declined in Boboye.
The second part of Table 6 indicates that the policy changes
also had a large impact on the probability of seeking any
treatment when ill. There is a small decrease (2%) in this
probability in Say, roughly a 4% increase in Boboye, and a
4% increase in Illela. These changes are similar across different income levels.
The probability of visiting a formal provider did not change
significantly in Say, where a fee of 200 FCFA was introduced.
Unlike Boboye, quality changes in Say were introduced more
or less simultaneously with the financing changes. In contrast,
the probability of treatment by a formal provider when ill
decreased significantly in the control region of Illela, where
there were no cost-recovery or quality-improvement initiatives.
The third section of Table 6 indicates the probability of
reporting illness in each of the three districts, before and after
the policy change, for each income level. The simulations
indicate large increases in Say (9%), reductions in Boboye
(5%), and a small increase in Illela (1%). With only three
regions and two time periods, we cannot detect whether these
large changes in rates of reported illness are related to the
policy changes or due to exogenous influences, such as epidemics.
The introduction of cost recovery and improvements in
quality of care in Boboye and Say changed the probabilities
of seeking treatment by informal providers in the desirable
direction. Individuals reporting an illness in the two experimental regions were more likely to visit formal providers and
less likely to be treated only at home or by healers and other
informal providers. In contrast, in the control region of Illela,
individuals were more likely to report treatment at home or
by informal providers after the policy change.
Several findings from the simulations are worth contrasting
with previous literature. Price effects are significant, but relatively small, noticeably smaller than the income effects on the
impact of seeking formal treatment and seeking any treatment. Households with the lowest incomes have roughly a
2% lower probability of seeking formal treatment, when
seeking any treatment, than households in the highest income
level, a difference that is small in comparison to other studies
of other regions.14,16 On the other hand, income is more
strongly related to the probability of seeking any treatment,
with roughly a 10% change between low and high income
levels.
As far as reported illness is concerned, both the univariate
analysis and logit model indicate that rates of reported illness
increased substantially in Say, decreased in Boboye and were
virtually unchanged in Illela. Because of the short time
elapsed since changes in cost recovery and quality improvements, together with the fact that rates of visits were increasing or unchanged in the two experimental regions, it seems
implausible that these changes can be attributed to the policy
changes. They do suggest the need for further monitoring of
this important trend, however.
5. Discussion
The probability of a patient visiting a formal provider
increased in Boboye following the policy changes, even
though these changes meant a greater financial outlay for the
Overall, the results give a reasonably favourable impression
of the policy changes. In neither case is there evidence of
serious reduction in access or increase in cost. Particularly
notable is the fact that in Say, with moderate cost sharing, the
observed decline in rates of visits is statistically insignificant.
The observed increase in the probability of formal visits in
Boboye is also striking. Both contrast with the control region
10 Chawla (jl/d)
11/2/00 3:15 pm
84
Page 84
Mukesh Chawla and Randall P Ellis
of Illela, where visit rates fell substantially even when there
was no change in price.
An important caveat in using the above results to guide widespread health sector reforms is that while many of the
observed changes lend positive support to the qualityenhancement and cost-recovery initiatives in Niger, the
absolute magnitudes are rather low. Moreover, in the absence
of any data on the informal provision sectors during this
period of changes, it is difficult to examine any interactions
between formal and informal care. This remains an important
area for future research.
5
6
7
8
9
Endnotes
i More formally, let S be the set of alternatives from which the
ij
consumer chooses at stage i given that he is currently at node j, and
let Xij be the vector of explanatory variables used at stage i node j of
the decision tree to predict choice of alternative j, and let fli be the
vector of utility weights assigned to this vector Xij. The probability
that the consumer will choose alternative j e Sij can be written as
Pr(j = j*) = exp(Xij* bi + ri Iij*)/ [Sexp(Xi,k bi + ri Iik)}.
k e Si,j
Note that in addition to the Xij variables, the selection of alternative
j at stage i depends on the ‘inclusive value’, Iij, weighted by the utility
weight ri. The inclusive value is defined recursively as
Iij = ln{[Sexp(Xi+1,k bi+1 + ri+1 Ii+1,k)}.
k e Si+1,j
The inclusive value for node j of the model is the denominator of the
logit expression used to make choices at node j. Under the assumption that the errors follow the generalized extreme value distribution, this expression is equal to the expected utility derived from
making the subsequent choices. Note that if there are no further
choices to be made, then the inclusive value is zero. For a good discussion of logit models, see Train.15
ii We are grateful to an anonymous referee for drawing our
attention to this.
iii The variable ‘reporting an illness’ captures incidence of illness
as reported by the individuals interrogated by the survey team.
References
1
2
3
4
Bitrán R. HFS Project: Major applied research in Niger under the
cost recovery pilot tests: research goals, objectives, and methods.
Health Financing and Sustainability Project paper, 1993.
Diop FP. Long term technical assistance pilot tests on cost recovery in the non-hospital sector: quarterly report, technical and
financial activities. Reports for the period Oct–Dec 1992,
Aug–Oct 1993 and Nov 1993-Jan 1994, submitted to USAID,
1993–94.
Wouters A, Kouzis A. Quality of health care and its role in cost
recovery with a focus on empirical findings about willingness to
pay for quality improvements. Major Applied Research Paper
No. 8, Health Financing and Sustainability Project. Report submitted to USAID, 1994.
Diop FP, Yazbeck A, Bitrán R. The impact of alternative cost
10
11
12
13
14
15
16
recovery schemes on access and equity in Niger. Health Policy
and Planning 1995, 10(3): 223–41.
Heller P. A model for the demand for medical and health services
in peninsular Malaysia. Social Science and Medicine 1982, 16:
267–84.
Akin J, Griffin C, Guilkey D, Popkin B. The demand for primary
health care services in the Bicol Region of the Philippines. Economic Development and Cultural Change 1984, 34(4): 755–82.
Gertler P, van der Gaag J. The willingness to pay for medical care:
evidence from two developing countries. Baltimore: John
Hopkins University Press, 1990.
Ii M. The demand for medical care: evidence from urban areas in
Bolivia. LSMS Working Paper No. 123. Washington DC: World
Bank, 1996.
de Béthune X, Alfani S and Lahaye JP. The influence of an abrupt
price increase on health service utilization: evidence from
Zaire. Health Policy and Planning 1989, 4(1): 76–81.
Waddington CJ, Enyimayew KA. A price to pay: the impact of
user charges in Ashanti-Akim District, Ghana. International
Journal of Health Planning and Management 1989, 4: 17–47.
Mwabu G, Wang’ombe JK, Kimani VN. Health service pricing
reforms and health care demand in Kenya. Paper presented at
the 4th Annual Meeting of the IHPP in Nyon, Switzerland, 1991.
Huber J. Ensuring access to health care with the introduction of
user fees: a Kenyan example. Social Science and Medicine 1993,
36: 485–94.
Litvack J, Bodart C. User fees plus quality equals improved access
to health care: results of a field experiment in Cameroon. Social
Science and Medicine 1993, 37(3): 369–83.
Ellis RP, Mwabu G. The demand for outpatient medical care in
rural Kenya. Unpublished Working Paper, Economics Department, Boston University, 1993.
Train K. Qualitative Choice Analysis. Massachusetts: The MIT
Press, 1986.
Ellis RP, McInnes DK, Stephenson EH. Inpatient and outpatient
health care demand in Cairo, Egypt. Health Economics 1994, 3:
183–200.
Acknowledgements
Research support for paper is gratefully acknowledged from USAID
as part of the Health Financing and Sustainability project conducted
by Abt Associates, Inc. We are grateful to Abdo Yazbeck, Ricardo
Bitran, Francois Diop and two anonymous referees for helpful comments on the paper. Any errors remain our own.
Biographies
Mukesh Chawla is the Senior Health Economist with the International Health Systems Group at the Harvard School of Public
Health. His research interests include health care financing, health
systems reform, policy analysis, and project design and evaluation in
health.
Randall Ellis is a Professor in the Economics Department at Boston
University specializing in modelling the interaction between supply
and demand side incentives on health markets. His research interests
span both US and international health topics.
Correspondence: Mukesh Chawla, Department of Population and
International Health, Harvard School of Public Health, Boston,
MA 02115, USA.