Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
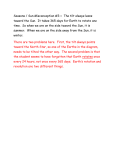
C The Author 2009. Published by Oxford University Press [on behalf of the British Geriatrics Society]. Age and Ageing 2009; 38: 718–723 doi: 10.1093/ageing/afp167 All rights reserved. For Permissions, please email: [email protected] Published electronically 12 September 2009 Impedance cardiography: a role in vasovagal syncope diagnosis? STEVE W. PARRY1 , MICHAEL NORTON2 , JESSIE PAIRMAN2 , MARY BAPTIST2 , KATHARINE WILTON2 , PAM REEVE2 , KATY SUTCLIFFE2 , JULIA L. NEWTON1,3 1 Institute for Ageing and Health, Newcastle University, Newcastle upon Tyne, NE4 5PL, UK Falls and Syncope Service, Royal Victoria Infirmary, Newcastle Hospitals NHS Trust, Newcastle upon Tyne, NE1 4LP, UK 3 Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, NE2 4HH, UK 2 Address correspondence to: J. Newton. Tel: +44 (0)191 2824128. Fax: +44 (0)191 2825338. Email: [email protected] Abstract Background: vasovagal syncope is the most common cause of syncope in all age groups, with diagnosis usually based on history, examination and basic investigations to exclude alternative causes of syncope. Where doubt exists, the head-up tilt (HUT) test is used for diagnosis but is time consuming and lacks a gold standard to accurately assess sensitivity and specificity. Alternative methods of diagnosing vasovagal syncope would thus be useful. Objective: to investigate the potential for impedance cardiography (ICG)-derived haemodynamic measures to predict HUT test outcome in unexplained syncope. Design: prospective controlled study. Subjects: eighty-six patients with unexplained syncope and 43 non-syncopal controls. Methods: all subjects underwent continuous heart rate, blood pressure and ICG measurements during 10 min supine rest and during HUT. Vasovagal syncope was diagnosed when patients experienced symptom reproduction with concomitant haemodynamic derangements. Results: during rest prior to HUT, the syncopal group had higher mean heart rate (P = 0.0008) and lower baroreceptor effectiveness index (P < 0.0001) compared to non-syncopal controls. On comparing patients who presented with unexplained syncope who subsequently had a positive HUT (therefore a diagnosis of vasovagal syncope 55 [64%]; mean age 47 years, range 17–85) to those having a negative tilt test (n = 31; mean age 47 years, range 17–88), there were no significant differences found in cardiovascular or autonomic parameters prior to HUT. A predictive ROC curve model at a 85% threshold allowed using cardiac index (CI), end-diastolic index (EDI) and left ventricular work index (LVWI) would identify those who would have a positive HUT from baseline cardiovascular measurements (CI >3.5, EDI > 77, LVWI >4.7) with 93% sensitivity and 17% specificity. Conclusion: supine haemodynamic measures derived from transthoracic ICG can simply, non-invasively and sensitively differentiate HUT-positive patients from those with negative tilt tests. Further work is needed, particularly in older patients, before this technique can be used in clinical practice. Keywords: syncope, impedance cardiography, autonomic, tilt table test, elderly Introduction Vasovagal syncope is themost common cause of syncope in the general population and is the most frequently diagnosed cause of syncope in both specialist and non-specialist practice [1, 2]. The syndrome is usually diagnosed through a combination of careful history, clinical examination and surface electrocardiogram to exclude both non-cardiac and cardiac causes of syncope [1, 2]. Where the diagnosis is uncertain, for example in older patients with cognitive impairment or unheralded syncope [3], or where syncope is associated 718 with injury or a driving or occupational imperative for formal diagnosis, prolonged head-up tilt (HUT) table testing with or without pharmacological or mechanical provocation is the standard investigation [1–5]. The test has reasonable specificity, sensitivity and reproducibility [1–4], but has been criticised for the absence of a gold standard (with the inherent difficulties in assessing sensitivity and specificity [6]), its reliance on symptom reproduction as surrogate for positivity, prolonged duration and limited usefulness in those with typical symptoms [7]. To circumvent some of these issues, several attempts have been made to predict tilt test outcome Impedance cardiography in VVS using tilt-derived haemodynamic and autonomic function data including baroreflex gain [8], total peripheral vascular resistance [9] and asymptomatic systolic blood pressure reductions [10] but none have found acceptance in clinical practice [1–4]. Impedance cardiography (ICG) was initially developed by NASA in the 1960s to remotely monitor cardiac output in its astronauts [11], but in the last decade has attracted much interest in clinical settings as diverse as heart failure management [12], critical care [13] and haemodialysis monitoring [14]. ICG non-invasively measures changes in thoracic impedance generated by fluctuating blood volumes during the cardiac cycle, allowing calculation of stroke volume, cardiac output and other derived parameters [13]. In recent years, ICG accuracy has been greatly facilitated by the advent of beat-to-beat blood pressure monitoring, with results obtained equivalent to conventional invasive methods [13–15] with an electrode cost of ∼£10 per test. Recent reports have explored the usefulness of ICG in the HUT-related investigation of vasovagal syncope [16–20], though current guidelines [1, 2, 7] make no mention of the technique in the investigation of unexplained syncope. We therefore set out to investigate whether ICG-derived haemodynamic data and autonomic function measures could accurately predict HUT outcome (and hence vasovagal syncope diagnosis) in consecutive patients undergoing tilt testing as part of their diagnostic work-up for unexplained syncope. Methods This study was performed in two parts. In part 1, baseline haemodynamic characteristics were compared between syncopal subjects and controls. In part 2, we compared haemodynamic, autonomic and cardiovascular parameters obtained during HUT in those who subsequently had a positive HUT with those who had a negative test. The syncopal patient group Consecutive patients with unexplained syncope attending our tertiary referral falls and syncope service were included. All subjects were routinely undergoing HUT table testing following detailed investigation per national [2] and international guidelines [1, 7]. All had normal surface electrocardiograms and no evidence of structural heart disease per clinical examination and/or echocardiograph. Control population A series of controls were recruited through notices in the university and hospital. Controls were excluded if they had experienced previous syncopal or pre-syncopal episodes. Controls underwent the same protocol as the patients. Head-up tilt protocol Patients and controls underwent HUT using the Italian protocol [21], with all cardiovascular assessments carried out with continuous heart rate and beat-to-beat blood pressure and ICG [11, 13–15] measurement, (TaskForce:CNSystems, Graz, Austria) supine for 10 min, during 20 min passive tilt and 15 min of 400 mcg provoked tilt. Vasovagal syncope was diagnosed using recognised diagnostic criteria, namely symptom reproduction with concomitant characteristic haemodynamic derangements [2]. Subjects who completed all phases of the HUT without symptoms were considered to be in the negative group. HUT was terminated if syncopal or presyncopal symptoms were reproduced, or at the patient’s request or if systolic blood pressure was <80 mmHg for longer than 3 min. Reproduction of symptoms in association with hypotension and/or bradycardia per evidence-based guidelines [2] was considered to be a positive test. Those subjects who had symptoms during the HUT with no change in heart rate or blood pressure were considered to have had a false-positive HUT and were excluded from further analysis. Assessment of autonomic parameters The integrity of the autonomic nervous system was assessed during HUT using baroreflex sensitivity (BRS) and baroreceptor effectiveness index (BEI; quantifies the number of times the baroreflex is effective in driving the sinus node) calculated by the Taskforce using the ‘sequence method’ [22] and heart rate variability (HRV), using spectral analysis [23]. Impedance cardiography Standard and accepted ICG parameters were evaluated. Myocardial contractility was measured as IC, ACI and ejection fraction. Afterload was measured as total peripheral resistance (TPRI) and preload as end-diastolic index (EDI). Other ICG variables were normalised for body surface area to provide cardiac index (CI; cardiac output normalized for body surface area), stroke index (SI) and left ventricular ejection time (LVET; time interval from the opening to the closing of the aortic valve (mechanical systole)) [15]. Statistics Where variables were parametric, data were presented as mean and standard deviation and comparisons were drawn between groups using Student’s t-test. Where variables were non-parametric, data were presented as median and range and comparisons drawn using Mann–Whitney tests. Correlation analyses and logistic regressions were obtained using ‘PrismGraphpad’ (http://www.graphpad.com/prism/Prism.htm). Receiver operating characteristic (ROC) analysis was used to determine the parameters that discriminated between predictors of a positive test and then used to determine sensitivity and specificity of a range of diagnostic models. ROC analysis provides a means to assess the diagnostic accuracy of a test and to compare the performance of more than one test for the same outcome. ROC curves are a plot of the sensitivity against false-positivity (sensitivity vs. (1 − specificity)) over all values available (rather than the single point calculations used in other means of assessing diagnostic accuracy) and hence allow the evaluation of the balance between sensitivity and specificity of a diagnostic test over a variety 719 S. W. Parry et al. Table 1. Demographics of the syncopal patient group Negative Positive P-value ................................................................. N 55 31 Age (years) 47 (21) 47 (20) ns Mean (SD) (range) [17–85] [17–88] Males Number (%) 13 (24%) 10 (32%) ns Culprit medications Number of patients taking (%) 7(13%) 6(19%) ns Co-morbidity Number affected (%) 7(13%) 7(23%) ns The negative group patients were those who underwent head-up tilt (HUT) and experienced no symptoms or haemodynamic change, whilst the positive group patients were those who experienced reproduction of syncopal symptoms in association with hypotension and/or bradycardia during HUT. of cutpoints. ROC curves were generated using ‘Analyse-it’ (http://www.analyse-it.com/). A P-value <0.05 was considered a statistically significant result. Ethical permission Ethical permission was obtained for the study of control subjects from the Newcastle and North Tyneside Local Research Ethics Committee. For the patient group, written permission was obtained for the use of data obtained during clinical management and this documentation was also reviewed and approved by our institution. Results Ninety unselected, consecutive syncopal patients who attended for 20:15 HUT over a 6 month period were included. Four had a false positive test and were excluded from further analysis. Therefore, the remaining 86 patients with unexplained syncope were matched group wise to 43 age- and sex-matched non-syncopal controls [mean (SD) age 47 (20) vs. 51 (7); ns]. Comparing syncopal versus non-syncopal subjects during the rest period During 10 min rest, the syncopal patient group had significantly higher mean heart rate [73 (12) vs. 66 (9); P = 0.0008] and significantly lower baroreceptor effectiveness index [55 (21) vs. 70 (16); P < 0.0001] compared to the non-syncopal control group. There were no significant differences between those who had a positive HUT compared to negative HUT in age, sex, the proportion taking culprit medications and the presence of co-morbidity (Table 1). Differences in haemodynamics between syncopal subjects who have a positive compared to those who have a negative 20:15 HUT Fifty-five (64%) of the 86 syncopal subjects had a negative HUT, and 31 subsequently had a positive test. There were no significant differences between those who had a positive 720 Table 2. Differences in baseline haemodynamic and cardiovascular parameters between the negative group (those who underwent head-up tilt (HUT) and experienced no symptoms or haemodynamic change) and the positive group (those who experienced reproduction of syncopal symptoms in association with hypotension and/or bradycardia during HUT) Negative Positive P-value ................................................................. HR 72 (13) 74 (10) 0.5 SBP 129 (24) 131 (14) 0.9 DBP 86 (15) 87 (10) 1.0 MAP 106 (16) 100 (11) 0.5 SI 39 (9) 43 (9) 0.1 CI 2.8 (0.6) 3.2 (0.8) 0.03 TPRI 2890 (872) 2685 (885) 0.6 EDI 64 (13) 70 (14) 0.05 IC 42 (15) 48 (16) 0.1 ACI 62 (23) 70 (27) 0.1 LVWI 4 (1) 4 (1) 0.02 LVET 310 (19) 295 (57) 0.08 Statistically significant differences are shown in bold. and those who had a negative HUT test in cardiovascular or autonomic parameters measured during 10 min of rest in supine position prior to tilting to 70◦ . There were, however, differences in central haemodynamic parameters as assessed by ICG, with those having a positive test having higher cardiac index, end-diastolic index and left ventricular work index (Table 2). These three significantly different variables were entered into a ROC curve model at a variety of thresholds. The most reliable model proved to be when the three variables were considered in the model at a threshold of 85% sensitivity (Figure 1). This allowed development of a predictive model that would identify those who would have a positive HUT from baseline cardiovascular measurements (CI >3.5, EDI >77, LVWI >4.7) with 93% sensitivity and 17% specificity. Discussion Our data show that supine, resting haemodynamic parameters derived from transthoracic ICG can simply, noninvasively and sensitively differentiate HUT-positive patients from those with negative tilt tests. This, the first prospective study involving asymptomatic controls to assess the role of ICG in vasovagal syncope diagnosis, showed that cardiac index, left ventricular work index and end diastolic index fitted to a ROC curve model at specific thresholds allowed the development of a predictive model that would identify syncopal patients with a positive HUT with 93% sensitivity and 17% specificity. In the absence of a gold-standard diagnostic test, the HUT is currently the only test available to aid clinicians for the diagnosis of vasovagal syncope, where history, clinical examination and surface ECG to exclude alternative causes are unhelpful [1–8]. The test takes a minimum of 30 min Impedance cardiography in VVS (a) 1 Sensitivity (true positives) 0.9 0.8 0.7 No discrimination 0.6 CI1 0.5 EDI 1 0.4 LVWI 1 0.3 0.2 0.1 0 0 0.2 0.4 0.6 0.8 1 - Specificity (false positives) 1 (b) 1 Sensitivity (true positives) 0.9 0.8 0.7 0.6 No discrimination 0.5 all 3 0.4 0.3 0.2 0.1 0 0 0.2 0.4 0.6 0.8 1 - Specificity (false positives) 1 Figure 1. Receiver operator curves of (a) the three variables Left Ventricular Work Index (LVWI), Cardiac Index (CI) and End-Diastolic Index (EDI), and (b) modelling including LVWI, EDI and CI at 85% threshold. even with the shortest nitrate-provoked protocols [6], while reliance on symptom reproduction (usually syncope) during appropriate haemodynamic changes is unpleasant for patients. These issues prompted several attempts to find an alternative to HUT testing in the diagnosis of vasovagal syncope particularly in groups where standing for long periods of time might be difficult, including older patients with mechanical difficulties. Early invasive studies using heterogeneous groups with unexplained syncope demonstrated that haemodynamic changes may predict syncope [24–26] with a small study estimating that the time delay between systolic and diastolic peaks of the finger arterial pressure wave form and large artery stiffness index predicted tilt positivity with 81% sensitivity and 96% specificity [27]. However, the importance placed upon a factor (arterial stiffness) unlikely to play a significant part in vasovagal syncope pathophysiology is questionable [27]. Several studies have shown that heart rate variability (HRV) increases before syncope, though there has been no definitive study specifically to guide clinical practice [1, 28, 29]. Others have shown that systemic vascular resistance reduces in those with a positive HUT at the time of syncope compared to those who have a negative HUT [30, 31]. None of these techniques have gained acceptance in the search for an alternative to HUT testing. The advent of ICG has meant that central haemodynamics could be accurately monitored non-invasively [16, 17]. An elegant series of studies from one laboratory examined the role of ICG in more detail [18–20]. In the initial retrospective study, Bellard et al. examined the central haemodynamic records of 68 patients during the supine rest and subsequent HUT [18]. They found that a model incorporating changes in baseline slow ejection time (representing late systole) and heart rate, systolic and diastolic blood pressure and pulse pressure during tilt provided 50% sensitivity and 97% specificity for subsequent positive tilt, though slow ejection time did not change around the time of syncope in positive patients [18]. A later study by this group found that neural network modelling of ICG-derived LVET and the slopes calculated from maximum and minimum impedance during tilt along with age and sex allowed 88% sensitivity and 64% specificity in predicting a positive tilt outcome [19]. The authors acknowledge the major limitation of this study, namely the technical difficulties of measuring LVET using ICG. Our results are both consonant with, and an advance on, Schang et al.’s findings. We have shown that supine prediction of tilt positivity is achievable in a falls and syncope clinic with current user-friendly technology albeit with specificity reminiscent of provocative tilt studies. The haemodynamic variables predicting tilt positivity not only made statistical but potentially pathophysiological sense. EDI (in essence the amount of blood remaining in the ventricle at the end of diastole adjusted for body surface area) is a powerful predictor of preload status, and while there is only a small venous pressure gradient between peripheral vasculature and the heart, the higher EDI in tiltpositive patients may reflect chronic alterations in venous capacitance (and hence venous pooling) that predispose the individual to vasovagal events. CI and LVWI (cardiac output and left ventricular work adjusted for body surface area) were also significantly higher in tilt-positive patients. Both of these impedance parameters strongly parallel myocardial oxygen consumption, while LVWI is a powerful indicator of the amount of work the left ventricle must perform to pump blood each minute and rises and falls with changes in arterial blood pressure and volume.The ROC curve model with the highest sensitivity incorporated these variables at the higher end of the normal ranges in these individuals, raising the possibility that the lower arterial compliance noted by others [18, 25] during supine rest in vasovagal patients may reflect further chronic capacitance vessel pooling. Relative compensatory increases in CI and LVWI are therefore necessary to combat the tendency to faint. Our findings provide evidence for chronic capacitance vessel pooling rather than the conventionally accepted acute venous pooling as the major physiological abnormality and predisposing factor to faints in patients with vasovagal syncope. To our knowledge, this is a novel hypothesis and is strongly supported by our findings. It is interesting to note the absence of any difference in HRV, BRS or BEI between any of the groups. Others have noted differences between tilt positive and negative, and vasovagal and control subjects in these parameters which suggest baroreflex deactivation in vasovagal subjects [28, 29, 32]. We found no such differences, though syncopal subjects 721 S. W. Parry et al. as a whole had significantly higher heart rates and lower BEI at rest than asymptomatic controls. If these finding were to apply only to tilt positive vasovagal subjects, one could speculate that this relatively enhanced tachycardic response was an appropriate response to relative baroreceptor deactivation, as previously noted by Pitzakis et al. [32]. It may be that the more heterogeneous syncope group had more patients with a vasovagal predisposition than was uncovered by a single tilt test, making a type II error a strong possibility. While our data are suggestive of a possible role for ICG in supplanting HUT in the diagnosis of VVS, the more work is needed before the latter cheap, safe and more readily accessible test is abandoned. Tilt testing can be performed with relatively little in the way of specialist equipment. While beatto-beat blood pressure monitoring is desirable, tilt testing can be performed with less exact blood pressure measures, while current ICG measures require sophisticated hardware and software for data recording and analysis. The modest cost of the specialised electrodes (£10.00) needs to be balanced against this added set-up cost when considering the costs and benefits of ICG testing in the future. Limitations While the TaskForce Monitor’s ICG system is highly sensitive and validated in a variety of settings and patient groups [13–15], stroke volume and cardiac output may be slightly inaccurate in those with significant valvular disease, reduced aortic compliance and with significant thoracic fluid accumulation [15]. Our patients were relatively young, and underwent detailed clinical examination to exclude these problems, but occult arteriosclerotic disease may still have been present in a small proportion. These factors must be accounted for in future studies incorporating older individuals. In conclusion, supine haemodynamic measures derived from transthoracic ICG can simply, non-invasively and sensitively differentiate HUT-positive patients from those with negative tilt tests. Our data suggest that the pattern of the central haemodynamic indices of most use in differentiating tilt positive patients may reflect a tendency to chronic capacitance vessel pooling in vasovagal patients. This is a novel finding that requires further investigation. Future studies are needed to explore the technique and our predictive model further, with the eventual aim of replacing the tilt test with these simple measures. Key points r Impedance cardiography is a powerful tool in assessing central haemodynamics and can now be measured noninvasively. r Comparing HUT testing in tilt-positive patients and controls. r ICG was sensitive but less specific in VVS diagnosis. r ICG may have a role in complementing or replacing tilt testing in VVS diagnosis. 722 Acknowledgements This work was supported by the UK NIHR Biomedical Research Centre for Ageing and Age-Related Disease award to the Newcastle upon Tyne Foundation Hospitals NHS Trust. Conflicts of interest No conflicts of interest declared. References 1. Brignole M, Alboni P, Benditt DG et al. Guidelines on management (diagnosis and treatment) of syncope—update 2004. Europace 2004; 6: 467–537. 2. Parry SW, Reeve P, Lawson J et al. The Newcastle Protocols 2008: an update on head-up tilt table testing and the management of vasovagal syncope and related disorders. Heart 2009; 95: 416–20. 3. Tan MP, Parry SW. Vasovagal syncope in the elderly. J Am Coll Cardiol 2008; 51: 599–306. 4. Parry SW, Kenny RA. Diagnosis and differential diagnosis of syncope using the head-up tilt table test. Q J Med 1999; 92: 623–9. 5. Gieroba ZJ, Newton JL, Parry SW, Norton M, Lawson J, Kenny RA. Unprovoked and glyceryl trinitrate provoked head-up tilt table test is safe in older people: a review of 10 years experience. J Am Geriatr Soc 2004; 52: 1913. 6. Parry SW, Gray JC, Baptist M, O’Shea D, Newton JL, Kenny RA. ‘Front-loaded’ glyceryl trinitrate-head-up tilt table testing: validation of a rapid first line tilt protocol for the diagnosis of vasovagal syncope. Age Ageing 2008; 37: 411–5. 7. Strickberger SA, Benson DW, Biaggioni I et al. AHA/ACCF scientific statement on the evaluation of syncope. Circulation 2006; 113: 316–27. 8. Freitas J, Pereira S, Lago P, Costa O, Carvalho MJ, Falcao de Freitas A. Impaired arterial baroreceptor sensitivity before tilt-induced syncope. Europace 1999; 1: 258–65. 9. Gierelak G, Guzik P, Makowski K, Kowal J, Chowela M. Haemodynamic indices of the early phase of the tilt test: does measurement predict outcome. Kardiol Pol 2005; 63: 244–51. 10. Pitzalis M, Massari F, Guida P et al. Shortened head-up tilting guided by systolic pressure reductions in neurocardiogenic syncope. Circulation 2003; 105: 146–8. 11. Kubicek WG, Karnegis JN, Patterson RP, Witsoe DA, Mattson RH. Development and evaluation of an impedance cardiac output system. Aerosp Med 1966; 37: 1208–12. 12. Packer M, Abraham WT, Mehra MR et al. Prospective Evaluation and Identification of Cardiac Decompensation by ICG Test (PREDICT) Study Investigators and Coordinators. Utility of impedance cardiography for the identification of short-term risk of clinical decompensation in stable patients with chronic heart failure. J Am Coll Cardiol 2006; 47: 2245–52. 13. Mathews L, Singh KRK. Cardiac output monitoring. Ann Card Anaesth 2008; 11: 56–67. 14. Kitzler TM, Sergeyeva O, Morris A, Skrabal F, Kotanko P, Levin NW. Noninvasive measurement of cardiac output in hemodialysis patients by task force monitor: a comparison with the Transonic System. Asaio J 2007; 53: 561–5. Impedance cardiography in VVS 15. Fortin J, Habenbacher W, Heller A et al. Non-invasive beatto-beat cardiac output monitoring by an improved method of transthoracic bioimpedance measurement. Comput Biol Med 2006; 36: 1185–203. 16. Shen WK, Low PA, Lohse CM, Hodge DO, Hammill SC. Distinct hemodynamic profiles in patients with vasovagal syncope: a heterogeneous population. J Am Coll Cardiol 2000; 35: 1470–7. 17. Nowak L, Nowak FG, Janko S, Dorwarth U, Hoffmann E, Botzenhardt F. Investigation of various types of neurocardiogenic response to head-up tilting by extended hemodynamic and neurohumoral monitoring. Pacing Clin Electrophysiol 2007; 30: 623–30. 18. Bellard E, Fortrat JO, Schang D, Dupuis JM, Victor J, Leftheriotis G. Changes in the transthoracic impedance signal predict the outcome of a 70 degree head-up tilt test. Clin Sci (Lond) 2003; 104: 119–26. 19. Schang D, Bellard E, Plantier G, Dupuis JM, Victor J, Leftheriotis G. Comparison of computational algorithms applied on transthoracic impedance waveforms to predict headup tilt table testing outcome. Comput Biol Med 2006; 36: 225– 40. 20. Schang D, Feuilloy M, Plantier G, Fortrat JO, Nicolas P. Early prediction of unexplained syncope by support vector machines. Physiol Meas 2007; 28: 185–97. 21. Bartoletti A, Alboni P, Ammirati F et al. ‘The Italian protocol’: a simplified head-up tilt testing potentiated with oral nitroglycerin to assess patients with unexplained syncope. Europace 2000; 2: 339–42. 22. Bertinieri G, di-Rienzo M, Cavallazzi A, Ferrari A, Pedotti A, Mancia G. A new approach to analysis of the arterial baroreflex. J Hypertension Supp 1985; 3: S79–81. 23. Anonymous. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American 24. 25. 26. 27. 28. 29. 30. 31. 32. Society of Pacing and Electrophysiology. Circulation 1996; 93: 1043–65. Epstein SE, Stampfer M, Beiser GD. Role of the capacitance and resistance vessels in vasovagal syncope. Circulation 1968; 37: 524–33. Chen CH, Hu HH, Lin YP, Chem CM, Hsu TL, Ding PY. Increased arterial wave reflection may predispose syncope attacks. Clin Cardiol 2000; 23: 825–33. Pitzalis M, Massari F, Guida P et al. Shortened head up tilting test guided by systolic pressure reductions in neurocardiogenic syncope. Circulation 2002; 105: 146–8. Simek J, Wichterle D, Melenovsky V, Malik J, Svobodova J, Svacina S. Pulse wave analysis during supine rest may identify subjects with recurrent vasovagal syncope. Clin Sci 2005; 109: 165–70. Kochiadakis GE, Orfanakis A, Chryssostomakis SI, Manios EG, Kounali DK, Vardas PE. Autonomic nervous system activity during tilt testing in syncopal patients, estimated by power spectral analysis of heart rate variability. Pacing Clin Electrophysiol 1997; 20: 1332–41. Kochiadakis GE, Kanoupakis EM, Rombola AT, Igoumenidis NE, Chlouverakis GI, Vardas PE. Reproducibility of tilt table testing in patients with vasovagal syncope and its relation to variations in autonomic nervous system activity. Pacing Clin Electrophysiol 1998; 21: 1069–76. Mitro P, Hijova E. Myocardial contractility and cardiac filling measured by impedance cardiography in patients with nitroglycerine-induced vasovagal syncope. Pacing Clin Electrophysiol 2006; 29: 1–8. Gielerak G, Guzik P, Makowski K, Kowal J, Cholewa M. Haemodynamic indices of the early phase of the tilt test: does measurement predict outcome? Kardiol Pol 2005; 63: 244–51. Pitzalis M, Gianfranco P, Massari F et al. Enhanced reflex response to baroreceptor deactivation in subjects with tiltinduced syncope. J Am Coll Cardiol 2003; 41: 1167–73. Received 1 February 2009; accepted in revised form 29 July 2009 723