Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Infant mortality wikipedia , lookup
Women's medicine in antiquity wikipedia , lookup
Dental emergency wikipedia , lookup
Seven Countries Study wikipedia , lookup
List of medical mnemonics wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Hypothermia therapy for neonatal encephalopathy wikipedia , lookup
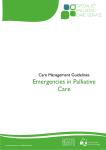
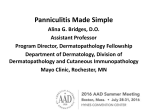
Australasian Journal of Dermatology (2001) 42, 207–210 CAS E REPORT Subcutaneous fat necrosis of the newborn following hypothermia and complicated by pain and hypercalcaemia Todd P Wiadrowski and Gillian Marshman Flinders Medical Centre, Bedford Park, South Australia, Australia SUMMARY A female infant was delivered at term with complications of severe meconium aspiration and birth asphyxia. Surface cooling was performed in the first 24 hours as part of the management of her birth asphyxia. Woody erythema was noted at 24 hours, followed by the formation of red–purple nodules on the 6th day. Clinical findings in the first 24 hours were suggestive of cold panniculitis. However, clinical and histological findings progressed to be in keeping with the diagnosis of subcutaneous fat necrosis of the newborn (SCFN). Furthermore, the immediate postnatal period was complicated by pain resistant to treatment with opiates. Asymptomatic hypercalcaemia was noted on periodic testing at 7 weeks and treated by rehydration, diuretics, prednisolone, etidronate and a low-calcium and -vitamin D diet. A review of the clinical and histological findings of the relevant panniculitides occurring in the postnatal period is presented, as well as a review of the treatment of hypercalcaemia in SCFN. Key words: cold panniculitis, corticosteroids, etidronate, infants, opiates, panniculitis. INTRODUCTION Subcutaneous fat necrosis of the newborn (SCFN) is a transient panniculitis of neonates typically presenting within the first 6 weeks of life. Most reported cases involve infants at full term or post-dates and of normal size for dates, but often with a history of birth asphyxia, meconium aspiration, cyanosis, seizures and hypothermia. An association with maternal diabetes and pre-eclampsia has been reported.1 The natural Correspondence: Dr G Marshman, Dermatology Unit, Department of Internal Medicine, Flinders Medical Centre, Flinders Drive, Bedford Park, SA 5042, Australia. Todd P Wiadrowski, BM, BS. Gillian Marshman, FACD. Submitted 12 September 2000; accepted 6 February 2001. history of the condition is for resolution without scarring. The most common complication of SCFN is hypercalcaemia, which has been associated with neonatal death.2 We describe a child with an overlapping clinical presentation following medically induced hypothermia to treat birth asphyxia. In this case, the initial clinical features of cold panniculitis progressed to those of SCFN, both clinically and histologically. This patient’s case was further complicated by pain and hypercalcaemia. CASE REPORT A female infant was born at term weighing 4350 g. Standard maternal prenatal screens revealed no significant abnormalities (haemoglobin, group and screen, glucose tolerance test, rubella serology, syphilis serology, hepatitis B surface antigen, hepatitis C serology, HIV serology and midstream urine specimen). The mother was noted to have mild hypertension with associated oedema and albuminuria in the third trimester. No medications were taken during the pregnancy. Table 1 details the significant events after delivery and over the ensuing months. During the first 24 hours, the child was noted to be hypotensive with cardiogenic shock requiring dopamine, had a pneumothorax, acute renal failure and a mild disseminated intravascular coagulation. Within the first hours of life, a decision was made for paralysis and sedation, with her core temperature kept between 32 and 33°C to treat her birth asphyxia. Hypothermia was achieved with the use of ice packs applied to the skin and turning off the overhead heating lamps. Her temperature was monitored via a rectal probe. This temperature was held for 24 hours, then raised to 35°C and then 37°C over a 3 day period. Approximately 24 hours post-delivery, a pink woody oedematous change was noted on the infant’s thighs and back, as well as petechiae on the right ankle. This progressively worsened over the ensuing 4 days and the buttocks were noted to be exquisitely tender to touch with grimacing and shrill cry. Plaques and nodules formed within these background changes at 6 days of age. A clinical diagnosis of SCFN was made (Fig. 1). Histology revealed an acute panniculitis with frank fat necrosis and needle-like clefts (Fig. 2), which confirmed the clinical diagnosis of SCFN. 208 TP Wiadrowski and G Marshman Figure 1 Purple nodules formed on erythematous and oedematous buttock skin at seven days postnatally. Figure 2 Skin biopsy from sacral nodule demonstrating radially arranged needle shaped clefts at seven days postnatally (H&E). Pain was poorly controlled by morphine. Due to continued difficulties with analgesia and the formation of new plaques and nodules, prednisolone was added at a dose of 1 mg/kg per day on day 34. This led to a definite improvement in pain control and subjective improvement in the intensity of the erythema. Weekly measurements of serum calcium detected hypercalcaemia at a corrected level of 3.74 mmol/L (normal range 2.20–2.75 mmol/L) 49 days after delivery. The infant’s weight at this time was 4910 g. Intravenous access was particularly difficult to attain in this infant and, therefore, initial treatment was with oral fluids, frusemide (8 mg, orally b.d.) and spironolactone (5 mg, orally b.d.). Prednisolone was being administered at a dose of 5 mg on alternate days when hypercalcaemia was detected and this was then increased to 5 mg, daily. After 4 days treatment, as described above, calcium levels were stable, but without significant decline. Etidronate was started at an oral dose of 25 mg, twice daily. Due to the irritant nature of etidronate and the patient’s underlying gastro-oesophageal reflux (GOR), the infant was nursed in an upright position for 30 min following administration. It was also suggested that etidronate should not be given within 2 hours of milk feeds because calcium–drug binding may occur and reduce absorption. Cisapride (1 mg, orally t.d.s.) had already been commenced for the treatment of the infant’s GOR and this was continued while etidronate was being administered. Calcium, parathyroid hormone and 1,25(OH)2-vitamin D3 levels were 3.49 mmol/L, 0.4 pmol/L (normal range 1.1–6.9 pmol/L) and 55 pmol/L (normal range 50–160 pmol/L), respectively. These levels were taken at the same time as the etidronate was started and it should be noted that the infant had been taking prednisolone for 19 days prior to this. A low-calcium and -vitamin D formula (Locasol) was commenced on day 54 and frusemide and spironolactone were ceased. Etidronate was continued for a total of 8 days treatment. At this time, calcium levels had normalized. Prednisolone was weaned over the ensuing 21 days because the infant’s pain had settled. Locasol was continued for 7 months and, when the child was weaned onto solids, a diet low in calcium was used initially. This diet consisted of fruit, vegetables, meat, cereals, such as rolled oats and semolina, and avoidance of dairy products. It was noted that some cereals, in particular Table 1 Time-course of presented case Delivery 2 min 5 min 10 min First hour’s 24 h Day 4 Day 5 Day 6 Day 7 Day 26 Day 34 Day 49 Day 53 Day 54 Day 61 Day 82 6 months Mid-cavity forceps delivery at term, thin meconium, cord pH 6.97 Apgar score 2 Apgar score 4 Apgar score 5, first spontaneous gasp followed this Endotracheal oxygen, adrenaline, hypothermia-induced paralysis and sedation Woody pink oedematous change on thighs and back, petechiae of right ankle Buttocks noted to be tender to touch Morphine added Nodules arise within previously erythematous and oedematous areas Biopsy taken; histology shows needle-shaped clefts in lipocytes and fat necrosis Cisapride started Prednisolone added at 1 mg/kg per day with subsequent improvement in pain relief Hypercalcaemia 3.74 mmol/L corrected, treatment commenced with oral rehydration, frusemide and spironolactone, prednisolone dose increased back to 1 mg/kg per day Hypercalcaemia 3.49 mmol/L corrected, etidronate 25 mg twice daily; normal vitamin D level Locasol added, frusemide and spironolactone ceased Etidronate ceased Prednisolone ceased Resolution of most nodules Subcutaneous fat necrosis of the newborn baby rice cereals, are fortified with calcium and should be avoided. A diet free of restrictions was commenced after 7 months. The infant continued to display nodules, predominantly on the proximal extremities and back, with slow resolution of most of these lesions by 6 months. At 9 months, the firm nodules that were present at her previous visit had altered little. Magnetic resonance imaging (MRI) was performed. Calcification was not present. The MRI appearances were of septate lesions composed of soft tissue and lipid. The nodules are stable and asymptomatic and further biopsy has not been performed. DISCUSSION Subcutaneous fat necrosis of the newborn is an uncommon transient panniculitis seen in term to post-term neonates that usually resolves without scarring. Lesions often develop on skin that initially appears oedematous prior to the formation of red–purple nodules and plaques.1,3 The nodular lesions of SCFN may present during the first 6 weeks, with one study reporting 45% of lesions arising in the first week of life.4 A differential diagnosis would include sclerema neonatorum (SN) and cold panniculitis, as outlined in Table 2. Our patient was noted to have pink woody oedematous skin on the thighs and back 24 hours after delivery. The distribution of these areas corresponded to the areas of application of the ice packs used to lower the child’s core temperature. Therefore, these features could be in keeping with cold panniculitis. However, at 6 days post-delivery, nodules were noted that steadily increased in size. These nodules were biopsied and demonstrated features in keeping with SCFN. Therefore, while we have clinical and histological evidence of SCFN, the lack of a biopsy specimen of the earliest lesion allows us only to speculate that, on clinical grounds, the infant either had an atypical presentation of SCFN or that this is a case of cold panniculitis progressing to SCFN. Painful lesions that proved to be difficult to control with opiate analgesia complicated the course of our case. An infant with painful SCFN requiring the use of morphine has been reported following the maternal use of amlodipine.10 Painful lesions in cases of SCFN without the maternal use of a calcium Table 2 209 channel blocker have not been highlighted. In our case, the infant’s lesions were noted to be painful as nodules began to arise. Cold panniculitis has been described as having tender nodules in adults6 and it is not unreasonable to expect these lesions may be tender in infants. Morphine, at doses of 1–2 mg four times a day, was administered without complete pain control. It was decided to add prednisolone at a dose of 1 mg/kg per day. This had a synergistic effect with morphine, giving complete pain control with doses of morphine that were previously insufficient. There was also some subjective improvement in the erythema overlying the nodules as well as a decrease in nodule size. We believe that the use of prednisolone should be strongly considered over the short-term in cases complicated by painful lesions. Evidence is lacking as to whether this changes the overall disease course or progression. Hypercalcaemia complicating SCFN is well recognized, but the pathogenesis is yet to be fully determined. Hypercalcaemia occurs between 2 and 16 weeks, most commonly at 6–7 weeks.7 Clinically, the most common feature is failure to thrive (90%), followed by fever, vomiting, feeding difficulties, irritability and listlessness. Mortality from hypercalcaemia complicating SCFN has been estimated at 15%.2 Because the child may have been discharged by the time these features arise, education of the parents to recognize these symptoms and report this to the managing physician is essential. To the best of our knowledge there are no specific guidelines for routine monitoring of serum calcium levels in these cases. For our patient, it was decided to perform weekly investigations of serum calcium and albumin levels until 16 weeks of age. Once a diagnosis of hypercalcaemia has been made, treatment options considered are outlined in Table 3.11 It is necessary to stress the importance of adequate hydration in the treatment of hypercalcaemia. Rehydration with a resultant increase in intravascular volume will increase glomerular filtration rate and increase renal calcium clearance.12 Loop diuretics are used to achieve increased calcium excretion by inhibiting calcium reabsorption and preventing volume overload secondary to the rehydration. Thiazide diuretics should not be used because they increase distal tubular reabsorption of calcium and, therefore, may aggravate the process. Differential diagnosis of subcutaneous fat necrosis of the newborn1,3,5–9 Subcutaneous fat necrosis Delivery Full term/post-dates Predisposing factors Maternal diabetes, hypertension Birth asphyxia, meconium aspiration, cyanosis, seizures, hypothermia Onset First 6 weeks Signs Red, blue nodules on trunk, buttock, arms, face, eyes Cold panniculitis Sclerema neonatorum Nil specific No maternal factors Cold stress Preterm neonate No maternal factors Uneventful delivery Within 72 hours of exposure Red, blue induration plaques Within the first week Diffuse yellow–white nodules, sparing the genitalia, palms and soles Needle-shaped clefts in lipocytes, nil to mild inflammatory infiltrate or fat necrosis, septa widened by oedema Poor, 75% mortality Histology Fat necrosis, foreign body giant cells, lymphocytic infiltrate, radially arranged needle-shaped clefts in lipocytes Lobular panniculitis, mixed infiltrate, no needle-shaped clefts Prognosis Generally very good; hypercalcaemia carries a 15% Excellent mortality rate 210 Table 3 TP Wiadrowski and G Marshman Management of an infant with subcutaneous fat necrosis of the newborn11–14 Panniculitis Hypercalcaemia Pain Education of parents regarding disease and symptoms and signs of hypercalcaemia (failure to thrive, fever, vomiting, feeding difficulties, irritability and listlessness); protect areas of panniculitis from trauma plus dressings for ulceration Weekly serum calcium and albumin levels to 16 weeks of age; rehydration, dietary vitamin D and calcium restriction, frusemide and prednisolone; consider etidronate if other measures fail Opiates, prednisolone Prednisolone is used in the treatment of hypercalcaemia, particularly in cases associated with haematogenous malignancy or cases of 1,25(OH)2-vitamin D3 excess, such as sarcoidosis. It has been suggested that the pathogenesis of hypercalcaemia in SCFN may be similar to that of sarcoidosis and, therefore, prednisolone would have a role in its treatment. In our case, prednisolone was administered for 15 days prior to the onset of hypercalcaemia. This may suggest that either the dose was inadequate, that prednisolone alone is unable to treat hypercalcaemia associated with SCFN or that the pathogenesis is unrelated or only partially related to the production of 1,25(OH)2-vitamin D3. We can only comment that, in our case, hypercalcaemia occurred despite the use of prednisolone and that vitamin D3 levels, when taken, were normal. Etidronate is a member of the bisphosphonate group of drugs that are known to decrease bone resorption. Etidronate has been reported to be successful in the management hypercalcaemia associated with SCFN13 and, due to the resistant nature of the hypercalcaemia to first-line treatments described above, this was embarked upon. The dose used was 5 mg/kg, which was in keeping with the previous report. The use of bisphosphonates, while effective in our case, should not be embarked on lightly because their effect on bone production, growth plates and mineralization is yet to be clarified.14 However, once etidronate was started, calcium levels fell to normal, at which time etidronate was ceased. A low-calcium and -vitamin D3 formula should also be added at the earliest possible stage and would optimally have been best used in association with the initial treatments as described above if it had been readily available at our institution. In conclusion, we present a case with early clinical features in keeping with cold panniculitis, but an overall clinical and histological picture of SCFN. This case was unusual in that it was complicated by significant pain in the infant only partially controlled with opiate anaesthesia. Oral prednisolone appeared to act synergistically with morphine to control this infant’s pain and should be considered for use in similar cases. In this case, etidronate was used with success over an 8 day course to control hypercalcaemia when first-line treatment failed. Normal serum calcium levels were subsequently maintained with dietary measures. REFERENCES 1. Fretzin DF, Arias AM. Sclerema neonatorum and subcutaneous fat necrosis of the newborn. Pediatr. Dermatol. 1987; 4: 112–22. 2. Norwood Galloway A, Lebwohl M, Phelps RG, Raucher H. Subcutaneous fat necrosis of the newborn with hypercalcemia. J. Am. Acad. Dermatol. 1987; 16: 435–9. 3. Atherton DJ. The neonate. In: Champion RH, Burton JL, Burns DA, Breathnach SM (eds). Textbook of Dermatology, Vol. 1, 6th edn. Oxford: Blackwell Science, 1998; 449–518. 4. Burden AD, Krafchik BR. Subcutaneous fat necrosis of the newborn: A review of 11 cases. Pediatr. Dermatol. 1999; 16: 384–7. 5. Black MM, Cunliffe WJ. Subcutaneous fat. In: Champion RH, Burton JL, Burns DA, Breathnach SM (eds). Textbook of Dermatology, Vol. 3, 6th edn. Oxford: Blackwell Science, 1998; 2403–35. 6. Bondi EE, Margolis DJ, Lazarus GS. Panniculitis. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, Fitzpatrick TB (eds). Fitzpatrick’s Dermatology in General Medicine, Vol. 1, 5th edn. New York: McGraw-Hill, 1999; 1275–89. 7. Hicks MJ, Levy ML, Alexander J, Flaitz CM. Subcutaneous fat necrosis of the newborn and hypercalcemia: Case report and review of the literature. Pediatr. Dermatol. 1993; 10: 271–6. 8. Lewis A, Cowen P, Rodda C, Dyall Smith D. Subcutaneous fat necrosis of the newborn complicated by hypercalcaemia and thrombocytopenia. Australas. J. Dermatol. 1992; 33: 141–4. 9. Weedon D. Panniculitis. In: Skin Pathology. Edinburgh: Churchill Livingstone, 1997; 441–56. 10. Rosbotham JL, Johnson A, Haque KN, Holden CA. Painful subcutaneous fat necrosis of the newborn associated with intrapartum use of a calcium channel blocker. Clin. Exp. Dermatol. 1998; 23: 19–21. 11. Ghirri P, Bottone U, Coccoli L, Bernardini M, Vuerich M, Cuttano A, Riparbelli C, Pellegrinetti G, Boldrini A. Symptomatic hypercalcemia in the first months of life: Calcium-regulating hormones and treatment. J. Endocrinol. Invest. 1999; 22: 349–53. 12. Wood AJJ. Management of acute hypercalcaemia. N. Engl. J. Med. 1992; 326: 1196–203. 13. Rice AM, Rivkees SA. Etidronate therapy for hypercalcemia in subcutaneous fat necrosis of the newborn. J. Pediatr. 1999; 134: 349–51. 14. Shoemaker LR. Expanding role of bisphosphonate therapy in children. J. Pediatr. 1999; 134: 264–7.