Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
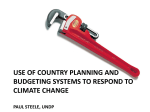
Journal of Pakistan Association of Dermatologists 2010; 20: 246-248. Case Report A case report of chronic sclerosing panniculitis Hadiuzzaman*, M. Hasibur Rahman*, Nazma Parvin Ansari**, Aminul Islam† *Department of Dermatology, Community Based Medical College, Bangladesh, Mymensingh, Bangladesh. **Department of Pathology, Community Based Medical College, Bangladesh, Mymensingh, Bangladesh †Department of Medicine, Community Based Medical College, Bangladesh, Mymensingh, Bangladesh Abstract Sclerosing panniculitis is a fibrotic process that usually occurs on the legs, commonly in women older than 40. The principal features are indurated woody plaques with erythema, edema, telangiectasia, and hyperpigmentation. Although the exact pathogenesis is uncertain, it is thought to occur as a result of ischemic changes. We present a 28-year-old married female who had a 10year history of painful sclerotic plaques, repeated ulceration and healing with fibrosis of the both lower legs and abdomen. Venogram and Doppler investigations were normal. Skin biopsy from the edge of the ulcer demonstrated the feature of chronic sclerosing panniculitis. Satisfactory improvement was found with methotrexate 7.5mg weekly for 4 months. No recurrence was noted within 1 year follow up. Key words Sclerosing panniculitis, lipodermatosclerosis. Case report A 28-year-old married female presented to dermatology outpatient, Community Based Medical College, Bangladesh, with a 10-year history of painful repeated ulceration and healing with fibrosis of the both lower legs and abdomen. This patient frequently visited different doctors for his lesions; sometimes healing was noted with conventional antibiotics and other supportive medicine but no permanent cure. The patient had been hospitalized repeatedly for episodes of increased pain, redness, oozing and swelling surrounding the ulcers. Address for correspondence Dr. M. Hasibur Rahman, Associate Professor of Dermatology, Community Based Medical College, Bangladesh, Mymensingh, Bangladesh. E mai l: [email protected] Mild swelling of the legs worse at the end of the day was also reported. Tenderness of the ulcer was worse with dependency. There was no history of previous trauma to the area, joint complaint, pancreatic disease, or other tender nodular lesions or ulcerations. There was no significant history of fever and night sweating. All the members of family were fine. She took different types of oral and injectable antibiotics and even a therapeutic trial of antituberculous therapy but improvement was not satisfactory. Some improvement was found with corticosteroid therapy but was followed by recurrences. On examination, there were multiple, mildly tender, sclerotic/fibrotic plaques with scaling, asymmetrically distributed over both lower legs (Figure 1) and abdomen. Some oozing ulcerated areas were noted over the plaques. There was no regional lymphadenopathy. No associated itching, hypoesthesia or loss of peripheral 246 Journal of Pakistan Association of Dermatologists 2010; 20: 246-248. Discussion Sclerosing panniculitis also known as ‘lipodermatosclerosis’, ‘hypodermitis sclerodermiformis’, and ‘stasis panniculitis’1 is a skin and connective tissue disease. It is a form of lower extremity panniculitis,2 an inflammation of the subcutaneous fat. Figure 1 A sclerotic plaque on left shin.. pulses was recorded. On laboratory investigation, CBC, liver functions, renal functions, and blood glucose were within normal limit. Mantoux test showed 15mm induration after 72 hours. Skin biopsy from the edge of the ulcer demonstrated a thinned epidermis; the superficial dermis showed sclerosis with angioplasia, patchy, chronic inflammation, and pigment deposition. Fibroadipose tissue with broad bands of sclerosis and fibrosis and prominent lipomembranous change with shrunken fat lobules was present beneath the dermis. In addition, other areas showed a lobular panniculitis with foamy macrophages and scattered lymphocytes and plasma cells. The biopsy was consistent with sclerosing panniculitis/lipodermatosclerosis. The patient was given methotrexate 7.5 mg weekly for 4 months with periodic monitoring of liver function tests, renal function tests and CBC. The patient subsequently had steady, gradual healing over 4 months without complications. Pain may be the first noticed symptom.2 People with lipodermatosclerosis have tapering of their legs above the ankles, forming a constricting band resembling an inverted coke bottle.2,4 In addition, there may be brownish-red 4 pigmentation and induration. The exact cause of lipodermatosclerosis is unknown.2,5 Venous disease, such as venous incompetence, venous hypertension, and body mass (obesity) may be relevant to the underlying pathogenesis.2 Increased blood pressure in the veins (venous hypertension) can cause diffusion of substances, including fibrin, out of capillaries. Fibrotic tissue may predispose the tissue to ulceration. Recurrent ulceration and fat necrosis is associated with lipodermatosclerosis. In advanced cases, the proximal leg swells from chronic venous obstruction and the lower leg shrinks from chronic ulceration and fat necrosis resulting in the inverted coke bottle appearance of the lower leg.6 Lipodermatosclerosis is most commonly diagnosed in middle-aged women.2 It is usually diagnosed clinically, and skin biopsy is not done routinely. Dermatopathological changes mainly affect the fat and depend on the stage of the disease. Early lesions show an infiltrate of lymphocytes and areas of tissue necrosis in the subcutis septa; in intermediate lesions there is a mixed infiltrate of white cells and new fibrous 247 Journal of Pakistan Association of Dermatologists 2010; 20: 246-248. tissue in the septa. Fibrous zones are present in the fat. Late lesions show marked fibrosis in the fat with diminished or absent inflammatory cells. Changes in the dermis include a mixed inflammatory cell infiltrate, increased fibrous cells, atrophy, or both, and tortuous thick-walled veins. Fibrin cuffs are seen around the capillaries by direct immunofluorescence. The histology stages correlate well with the two stages seen clinically. • • • • Fibrinolytic agents such as stanozolol, fibrinolytic agents use an enzymatic action to help dissolve blood clots.2,3,4,7 Pentoxyfylline to increase blood flow Clobetasol propionate (ultrapotent topical steroid) or intralesional triamcinolone injections to reduce inflammation Capsaicin to reduce pain References Blood tests are not usually required in lipodermatosclerosis but coagulation may be tested. Ultrasound scans and magnetic resonance imaging may be used to define the extent of the disease and to determine whether there is a role for vascular surgery. The most important part of management is compression therapy to correct venous stasis. Management may also include: • • • • • Vein surgery, endovenous laser ablation or sclerotherapy for varicose veins. Leg elevation, Elastic compression stockings, and bed rest Weight reduction Ultrasound therapy 1. 2. 3. 4. 5. 6. 7. James WD, Berger TG, Elston DM, eds. Andrews' Diseases of the Skin: Clinical Dermatology. Philadelphia: Saunders/ Elsevier; 2006. Bruce AJ, Bennett DD, Lohse CM et al. Lipodermatosclerosis: Review of cases evaluated at Mayo Clinic. J Am Acad Dermatol 2002; 46: 187-92. Ginsburg PM, Ehrenpreis ED, eds. NORD Guide to Rare Disorders. Philadelphia PA: Lippincott Williams & Wilkins; 2003. Phelps RG, Shoji T. Update on panniculitis. Mt Sinai J Med 2001; 68: 262-7. Fischer DR, Matthews JB, eds. Sleisenger & Fordtran’s Gastrointestinal and Liver Disease, 7th edn. Philadelphia PA: Saunders Elsevier.; 2002. Habif TP. Habif: Clinical Dermatology, 4th edn. New York: Mosby; 2004 Luis Requena L, Yus ES, Kutzner H. Panniculitis. In: Wolff K, Goldsmith LA, Katz SI et al., editors. Fitzpatrick’s Dermatology in General Medicine, 7th edn. New York: McGraw-Hill; 2003. P. 569-85. 248