Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
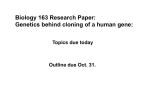
Genome-Wide Scan for Pulse Pressure in the National Heart, Lung and Blood Institute’s Framingham Heart Study Anita L. DeStefano, Martin G. Larson, Gary F. Mitchell, Emelia J. Benjamin, Ramachandran S. Vasan, Jiang Li, Diane Corey, Daniel Levy Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 Abstract—The objective of this study was to assess heritability and identify chromosomal regions showing evidence of linkage to pulse pressure (PP), a simple indicator of proximal conduit vessel stiffness. Blood pressure data were analyzed for 8478 members of the National Heart, Lung and Blood Institute’s (NHLBI) Framingham Heart Study. Long-term PP was defined using 2-stage analysis. First, the difference between systolic and diastolic blood pressure was averaged over all qualifying clinic examinations. In the second stage, mean PP was adjusted for mean age, time period of examination, and body mass index by regression analysis. PP values were available for 6421 individuals in 1593 families for heritability estimation and for 2492 individuals in 330 families for linkage analysis. Microsatellite markers covering the genome at 10 cM intervals were typed by the NHLBI Mammalian Genotyping Service; genome scan data were available on 1585 individuals with PP data. Heritability estimates of long-term PP accounting for hypertension treatment and for ignoring treatment were 0.52 and 0.51, respectively. Variance component linkage analysis identified several locations with suggestive evidence of linkage: chromosome 15 at 122 cM (logarithm of odds [LOD]⫽2.94), chromosome 7 at 71 cM (LOD⫽2.42), chromosome 5 at 53 cM (LOD⫽2.03), and chromosome 10 at 81 cM (LOD⫽1.83) for PP accounting for treatment. LOD scores were slightly lower when ignoring treatment, with the exception of a peak on chromosome 10 at 81 cM (LOD⫽2.58). In conclusion, we have demonstrated a substantial genetic component to PP and have identified 4 chromosomal regions that may harbor genes influencing vascular stiffness. (Hypertension. 2004; 44:152-155.) Key Words: genetics 䡲 blood pressure 䡲 human P Subjects ulse pressure (PP), which is the difference between systolic blood pressure (SBP) and diastolic blood pressure (DBP), provides an indirect measure of pulsatile hemodynamic load and vascular stiffness. PP is associated with left ventricular hypertrophy,1 carotid intimal-medial thickness,2,3 and artherosclerotic burden.4 Of the 3 BP components, PP has also been found to be the best predictor of risk for cardiovascular disease5 and heart failure in older people.6 An understanding of the genetic determinants of PP, therefore, is important. Prior genetic studies in Nigerian,7 Mexican American,8 and Utah cohorts9 have found modest heritability for PP, ranging from 0.12 to 0.25. In these 3 studies, PP was measured at a single point in time. In this study, we estimated heritability of PP and performed a genome-wide linkage analysis based on repeated measures obtained during up to 50 years of follow-up of Framingham Heart Study participants. Subjects were participants in the Framingham Heart Study, a longitudinal study established in 1948 with the enrollment of 5209 individuals residing in Framingham, Mass.10 Beginning in 1971, 5124 offspring of the original participants and their spouses were recruited.11 At each clinic visit, the physician measured the seated BP with a mercury column sphygmomanometer. The systolic and diastolic pressures were determined by the first and fifth Korotkoff sounds, respectively. Two BP measurements were averaged to derive the systolic and diastolic pressures for that examination, except for the first offspring examination at which only 1 BP measurement was obtained. All subjects gave informed consent, and the study protocol was approved by the Institutional Review Board at Boston Medical Center (Mass). PP Phenotype Long-term PP was defined as the mean difference between SBP and DBP obtained at each qualifying examination. The method used to compute long-term blood pressure and to impute SBP and DBP in the setting of antihypertensive treatment has been described previously.12 Long-term BP data were analyzed for 8478 subjects who met criteria using a 2-stage procedure: (1) within-subject mean SBP and DBP were calculated and (2) sample-wide regressions were used to adjust mean PP (defined as mean SBP⫺mean DBP) for age, time Methods An expanded Methods section is available in the online supplement at http://www.hypertensionaha.org. Received March 17, 2004; first decision April 5, 2004; revision accepted May 28, 2004. From the Department of Biostatistics (A.L.D., J.L.), Boston University School of Public Health, Mass; the Departments of Neurology (A.L.D.) and Epidemiology and Preventive Medicine (M.G.L., E.J.B., R.S.V., D.L.), Cardiology Section (E.J.B., R.S.V., D.L.), Boston University School of Medicine, Mass; the National Heart, Lung, and Blood Institute’s Framingham Heart Study (M.G.L., E.J.B., R.S.V., D.C., D.L.), Framingham, Mass; and Cardiovascular Engineering, Inc. (G.F.M.), Holliston, Mass. Correspondence to Anita L. DeStefano, Boston University School of Public Health, 715 Albany Street, T418E, Boston, MA 02118. E-mail [email protected] © 2004 American Heart Association, Inc. Hypertension is available at http://www.hypertensionaha.org DOI: 10.1161/01.HYP.0000135248.62303.81 152 DeStefano et al period of examination, and body mass index, yielding a residual for each subject. Residuals were computed separately for each sex and cohort. For subjects receiving hypertension treatment, the recorded BP is less than what the untreated value would be. We addressed treated observations by using a nonparametric algorithm to adjust BPs for treatment effect as previously described.12 These adjusted BP values were used in place of the measured BP values when obtaining the difference between SBP and DBP. Analyses were also conducted on long-term average PP ignoring treatment. Genome-Wide Scan for Pulse Pressure 153 Variance Component Multipoint LOD Scores >1.5 for Long-Term Pulse Pressure Obtained From Genehunter Adjusted for Treatment Chromosome cM Ignoring Treatment LOD cM LOD 1.51 5 53 2.03 56 7 71 2.42 70 2.36 7 152 1.54 154 1.55 Genotyping 8 140 1.56 140 1.22 DNA was extracted using a standard protocol. A 10 cM density genome scan was performed (marker set 8A, average heterozygosity 0.77) on 1702 individuals with DNA available from the 330 largest families by the National Heart, Lung and Blood Institute Mammalian Genotyping Service laboratory at the Marshfield Clinic (Marshfield, Wis). Genotype data were cleaned as previously described.12 10 81 1.83 80 2.58 15 122 2.94 122 2.86 22 36 1.75 36 1.02 Results by-descent estimation at this location may not be as accurate as if there were additional flanking markers typed. However, such genotype data are currently not available in these subjects. LOD scores ⬎2.0 for PP accounting for treatment were also observed on chromosome 5 at 53 cM (LOD⫽2.03) and chromosome 7 at 71 cM (LOD⫽2.42). Minor peaks (LOD between 1.5 and 2.0) were observed on chromosomes 7, 8, 10, and 22. LOD scores tended to decrease slightly when treatment was ignored. An exception to this pattern was the chromosome 10 linkage peak at 80 cM, which yielded a LOD score of 2.58 when treatment was ignored. A permutation approach that maintains the trait heritability17 was implemented to assess the significance of the largest observed LOD score (2.94). The heritability of the permuted phenotypes averaged over 1000 replicates was 0.51, indicating that, on average, the permutated data sets maintained the additive genetic variance. The genome-wide empirical P value associated with LOD⫽2.94 is 0.067. For heritability estimation, long-term average PP was available for 6421 subjects in 1593 families. Linkage analysis was based on the long-term average PP values of 2492 subjects from the 330 families in which the genome scan was performed. There were 1584 individuals with genotype and PP data available. Among the 1584 individuals with both genotype information and phenotypic measures, mean PP was 47.33⫾10.77 mm Hg when accounting for treatment effect and 47.09⫾9.56 mm Hg when ignoring treatment. Descriptive statistics for other characteristics in these subjects have been previously published.12 Estimated heritability for mean PP accounting for treatment effect was 0.52⫾0.03. Heritability ignoring antihypertensive treatment was nearly identical at 0.51⫾0.03. Thus, we have demonstrated a considerable genetic influence for PP. Genome scan results are summarized in the Table and Figure. The highest multipoint LOD score for PP accounting for treatment was 2.94 observed on chromosome 15 (122 cM). This value is just below the threshold for significant linkage on a genome-wide level and must be considered strong suggestive evidence of linkage to this chromosome. There was minimal change in the LOD score at this location when treatment was ignored (LOD⫽2.86). This peak does occur for the last marker on the chromosome, and identity- We found highly suggestive evidence of linkage for PP on chromosome 15 (LOD score 2.94 at 122 cM). This is the same region where linkage to low DBP (LOD⫽3.77) was previously reported in a Chinese population.18 This overlap is particularly intriguing because a low diastolic pressure is often a key component of an elevated PP. A genome-wide linkage analysis of PP in a populationbased sample of Mexican Americans (San Antonio Family Heart Study) revealed suggestive evidence of linkage (LODs between 2.78 and 1.95) for 4 markers: D7S1799 (113.9 cM), D8S1100 (154 cm), D18S844 (116.4 cM), and D21S1440 (36.7 cM).8 The chromosome 8 location identified in that study (LOD⫽0.59 at D8S1179 at 135 cM and LOD⫽1.98 at D8S1100 at 154 cM) overlaps with the region on chromosome 8 that yielded a LOD score of 1.56 (at 140 cM) in our Framingham sample. As noted by Atwood et al,8 this region on chromosome 8 contains the aldosterone synthase gene (CYP11B2) and the adjacent 11 -hydroxylase gene, which are causative for glucocorticoid-remediable aldosteronism, a rare Mendelian form of hypertension.19 Linkage analysis of PP in extended Utah pedigrees ascertained on the basis of early coronary disease deaths or strokes or early-onset hypertension yielded suggestive evidence of Statistical Analysis Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 Heritability was estimated by a variance component model using the program SOLAR.13 Multipoint linkage analysis was conducted using the variance component approach as implemented in the program Genehunter.14,15 Although 14 families were split because of computational constraints when using Genehunter, the algorithm implemented in Genehunter has been shown to provide more exact multipoint identity-by-descent estimates.16 The splitting of families resulted in linkage analysis being performed on 345 pedigrees compared with the 330 originally defined. Variance components methods have been shown to be sensitive to departures from normality. Although extreme departures from normality were not observed for these data (skewness⫽0.76, kurtosis⫽1.70 for residual PP adjusted for treatment), a constrained permutation test, which maintains the additive genetic variance of the phenotype,17 was used to obtain a genome-wide empirical P value for the largest logarithm of odds (LOD) score observed. Simulation, permutation, and linkage analysis was repeated 1000 times. Discussion 154 Hypertension August 2004 Genome-wide linkage analysis results for long-term pulse pressure. Multipoint LOD score is on the vertical axis, and centiMorgan distance from the p-terminus of the chromosome is on the horizontal axis. Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 linkage (LOD ⬎1.5) for 11 chromosomal regions. A LOD score of 1.53 was observed at 8q at 164 cM.9 This linkage peak overlaps with the 8q peak observed in Mexican Americans and is approximately 24 cM from the chromosome 8 linkage peak observed in the Framingham Heart Study sample. The Framingham Heart Study and the Utah pedigrees also had concordance for linkage on chromosome 7. The Utah study observed linkage at 70 cM (LOD⫽1.59), which overlaps with the peak at 71 cM (LOD⫽2.42) in the current study. No other linkage peaks were common between the Framingham Heart Study and either the San Antonio Family Heart Study or the Utah study. This is not surprising given the ethnic differences between the populations and the differences in study design (cross sectional for San Antonio and Utah and longitudinal for Framingham). Additionally, distinct linkage analysis methods were applied in each study: a multipoint variance component approach in the current genome scan, a 2-point parametric model in the San Antonio analysis, and a multipoint parametric model accounting for heterogeneity in the Utah sample. The parametric model applied in the San Antonio study assumed a genetic model with sex-specific genotypic means and sex-specific and genotype-specific means for age, age squared, and BMI. This type of modeling is computationally intensive for large pedigrees, and computational restraints limited the San Antonio study to 2-point analysis (ie, examining linkage between PP and a single genetic marker at a time).8 The variance component method used in our study enabled multipoint analysis in which information from all markers along a chromosome are used simultaneously to evaluate linkage. Analysis of the Utah pedigrees was also based on multipoint inheritance probabilities and required estimation of additional parameters to specify the trait distribution for the parametric analysis.9 Linkage analysis to SBP and DBP has been previously reported in the Framingham Heart Study.12 Minimal overlap was observed in linkage peaks for SBP (or DBP) and PP. The peak on chromosome 5 observed for PP (LOD⫽2.03) coincides with a 2-point LOD score of 2.0 we previously observed for SBP. The peak regions for SBP (LOD⫽4.70 at 67 cM on chromosome 17) and DBP (LOD⫽2.1 at 7 cM on chromosome 18) yielded LOD scores of 1.47 and 0.0, respectively for PP. This suggests that genes contributing to variation in PP, and by inference, to vascular stiffness, may be distinct from those contributing specifically to SBP or DBP. Many genes located in the regions for which linkage peaks were observed can be postulated as candidate genes. We highlight the most promising in the 4 regions that yielded suggestive evidence of linkage. Located at the distal end of the long arm of chromosome 15 are genes for the insulin-like growth factor-1 receptor (IGF1R); myocyte-specific enhancer factor 2A (MEF2A), a transcription factor involved in angiotensin II-mediated activation of vascular smooth muscle cells20; chondroitin synthase (CHSY1), an enzyme involved in synthesis of proteoglycans that are an integral component of the extracellular matrix21; and a secretory proprotein convertase (PACE4). The genes for 2 major binding proteins of IGF1, IGFBP1 and IGFBP3, are both located in the proximal linkage peak on chromosome 7. Growth hormone (GH), acting at the GH receptor located under the chromosome 5 linkage peak, increases levels of IGF1. Clearly, the GH/IGF axis has DeStefano et al Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 important effects on vascular growth and tone, and several elements of this axis (eg, IGFR, IGFBP1, IGFBP3, GHR) have shown up under our linkage peaks, making detailed analysis of the members of this pathway a high priority for future studies. There were no obvious candidate genes in our linkage peak on chromosome 10. A strategy for moving to gene identification from linkage analysis results is using a bioinformatics approach to identify likely candidate genes, such as those described above in the linkage regions. Selection of candidate genes may be followed by SNP typing within the candidate genes, including the 3⬘ untranslated region that may be critical for gene regulation. Family-based association analysis, using the linkage subjects, or association analysis in a subset of unrelated individuals can then be used to determine whether variants in the candidate genes influence PP. Given that linkage peaks tend to be broad and there are numerous genes, which may have unknown function, it may be necessary to type additional genes or densely cover the entire region with SNP genotyping. Definitive proof of any positive association would require functional studies of the specific variant implicated as well as replication in another population. Despite the large sample size, extended pedigrees, and detailed phenotyping in the Framingham Heart Study, the largest LOD score observed in this analysis was 2.94, which highlights the challenges of genetic localization and identification for complex traits. Researchers must question whether the best use of limited resources is to allocate them for follow-up of a modest linkage peak by either examining candidate genes within the region or undertaking large-scale sequencing or typing of single nucleotide polymorphisms across the region for association studies. Although differences in populations, ascertainment, and analytic methods make comparison among multiple linkage analyses difficult, regions such as 8q, which yield suggestive peaks in multiple studies, may be important regions worthy of such follow-up. These results also suggest that even larger family-based studies may be needed. Perspectives In summary, we have demonstrated a substantial genetic component for PP. Although we did not meet the Lander and Kruglyak criterion for genome-wide significance (LOD score ⬎3.2),22 we did observe several suggestive regions of linkage, most notably LOD⫽2.94 at 122 cM on chromosome 15. A region on 8q also appears to be of particular interest for PP because this location yielded suggestive evidence of linkage in 3 independent studies. There are several interesting candidate genes in the regions of suggestive linkage, and future work will include association studies of these genes. The third generation of Framingham Heart Study families are currently being recruited, and extension of these pedigrees by an additional generation will result in a substantial increase in power for detecting genes influencing a complex trait such as PP. Acknowledgments The Framingham Heart Study is funded by National Institutes of Health (NIH) contract NO1-HC-25195. This study was also supported by the Donald W. Reynolds Foundation. We thank Ming-Huei Chen for computing assistance in obtaining the empirical probability values. Genome-Wide Scan for Pulse Pressure 155 References 1. Kobayashi S, Yano M, Kohno M, Obayashi M, Hisamatsu Y, Ryoke T, Ohkusa T, Yamakawa K, Matsuzaki M. Influence of aortic impedance on the development of pressure-overload left ventricular hypertrophy in rats. Circulation. 1996;94:3362–3368. 2. Saba PS, Roman MJ, Pini R, Spitzer M, Ganau A, Devereux RB. Relation of arterial pressure waveform to left ventricular and carotid anatomy in normotensive subjects. J Am Coll Cardiol. 1993;22:1873–1880. 3. Franklin SS, Sutton-Tyrrell K, Belle SH, Weber MA, Kuller LH. The importance of pulsatile components of hypertension in predicting carotid stenosis in older adults. J Hypertens. 1997;15:1143–1150. 4. Lee TM, Lin YJ, Su SF, Chien KL, Chen MF, Liau CS, Lee YT. Relation of systemic arterial pulse pressure to coronary atherosclerosis in patients with mitral stenosis. Am J Cardiol. 1997;80:1035–1039. 5. Franklin SS, Khan SA, Wong ND, Larson MG, Levy D. Is pulse pressure more important than systolic blood pressure in predicting coronary heart disease events? The Framingham Heart Study. Circulation. 1999;100: 354 –360. 6. Haider AW, Larson MG, Franklin SS, Levy D. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study. Ann Intern Med. 2003;138:10 –16. 7. Adeyemo AA, Omotade OO, Rotimi CN, Luke AH, Tayo BO, Cooper RS. Heritability of blood pressure in Nigerian families. J Hypertens. 2002;20:859 – 863. 8. Atwood LD, Samollow PB, Hixson JE, Stern MP, MacCluer JW. Genome-wide linkage analysis of pulse pressure in Mexican Americans. Hypertension. 2001;37(2 Part 2):425– 428. 9. Camp NJ, Hopkins PN, Hasstedt SJ, Coon H, Malhotra A, Cawthon RM, Hunt SC. Genome-wide multipoint parametric linkage analysis of pulse pressure in large, extended Utah pedigrees. Hypertension. 2003;42: 322–328. 10. Dawber TR, Meadors GF, Moore FEJ. Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health. 1951;41: 279 –286. 11. Kannel WB, Feinbleib M, McNamara PM, Garrison RJ, Castelli WP. An investigation of coronary heart disease in families: the Framingham Offspring Study. Am J Epidemiol. 1979;110:281–290. 12. Levy D, DeStefano AL, Larson MG, O’Donnell CJ, Lifton RP, Gavras H, Cupples LA, Myers RH. Evidence for a gene influencing blood pressure on chromosome 17q12–21: genome scan linkage results for longitudinal blood pressure phenotypes in subjects from the Framingham Heart Study. Hypertension. 2000;36:477– 483. 13. Almasy L, Blangero J. Multipoint quantitative trait linkage analysis in general pedigrees. Am J Hum Genet. 1998;62:1198 –1211. 14. Kruglyak L, Daly MJ, Reeve-Daly MP, Lander ES. Parametric and nonparametric linkage analysis: a unified multipoint approach. Am J Hum Genet. 1996;58:1347–1363. 15. Pratt SC, Daly MJ, Kruglyak L. Exact multipoint quantitative-trait linkage analysis in pedigrees by variance components. Am J Hum Genet. 2000;66:1153–1157. 16. Sobel E, Sengul H, Weeks DE. Multipoint estimation of identity-bydescent probabilities at arbitrary positions among marker loci on general pedigrees. Hum Hered. 2001;52:121–131. 17. Iturria SJ, Williams JT, Almasy L, Dyer TD, Blangero J. An empirical test of the significance of an observed quantitative trait locus effect that preserves additive genetic variation. Genet Epidemiol. 1999;17: S169 –S173. 18. Xu X, Yang J, Rogus J, Chen C, Schork N, Xu X. Mapping of a blood pressure quantitative trait locus to chromosome 15q in a Chinese population. Hum Mol Genet. 1999;8:2551–2555. 19. Sutherland DJ, Ruse JL, Laidlaw JC. Hypertension, increased aldosterone secretion and low plasma renin activity relieved by dexamethasone. Canad Med Assoc J. 1966;95:1109 –1119. 20. Suzuki E, Nishimatsu H, Satonaka H, Walsh K, Goto A, Omata M, Fujita T, Nagai R, Hirata Y. Angiotensin II induces myocyte enhancer factor 2and calcineurin/nuclear factor of activated T cell-dependent transcriptional activation in vascular myocytes. Circ Res. 2002;90:1004 –1011. 21. Kitagawa H, Uyama T, Sugahara K. Molecular cloning and expression of a human chondroitin synthase. J Biol Chem. 2001;276:38721–38726. 22. Lander ES, Kruglyak L. Genetic dissection of complex traits: guidelines for interpreting and reporting results. Nat Genet. 11:241–245. Genome-Wide Scan for Pulse Pressure in the National Heart, Lung and Blood Institute's Framingham Heart Study Anita L. DeStefano, Martin G. Larson, Gary F. Mitchell, Emelia J. Benjamin, Ramachandran S. Vasan, Jiang Li, Diane Corey and Daniel Levy Downloaded from http://hyper.ahajournals.org/ by guest on June 18, 2017 Hypertension. 2004;44:152-155; originally published online June 21, 2004; doi: 10.1161/01.HYP.0000135248.62303.81 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2004 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/44/2/152 Data Supplement (unedited) at: http://hyper.ahajournals.org/content/suppl/2004/07/29/44.2.152.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/