Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
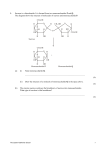
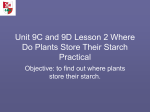
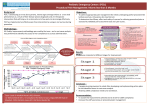
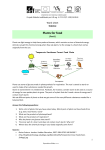
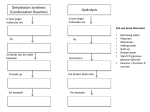
4/8/2017 Idaho Academy of Nutrition & Dietetics Annual Meeting – Boise, Idaho What Every Dietitian Needs to Know about Genetic SucraseIsomaltase Deficiency (GSID) Disclosures Employed by QOL Medical, LLC — QOL Medical is the manufacturer of a treatment to relieve the Anne Boney, MEd, RD, LDN Clinical Science Liaison QOL Medical, LLC symptoms of Genetic Sucrase-Isomaltase Deficiency (GSID) 2 Genetic Sucrase-Isomaltase Deficiency (GSID) Outline Introduction (Don’t Worry-This Is Not A Test) How many have heard of Genetic Sucrase-Isomaltase Deficiency (GSID)? #1 Quick carbohydrate overview – as it relates to Genetic Sucrase-Isomaltase Deficiency (GSID) #2 Why should I test for GSID? It’s so rare. Prevalence #3 Wh Who should h ld b be screened d ffor GSID? Identifying the Patient #4 What kind of diagnostic testing is available? Diagnostic Tools #5 How do I treat GSID? Treatment Options How many are familiar with foods high in sucrose? What about foods that are high in starch? GSID is not something we learned about in school. GSID is not something most physicians are familiar with. But, there are patients suffering with GSID. And, I believe dietitians are in the perfect place to help identify these patients, recommend further diagnostic testing, and provide nutrition education to those with GSID. 3 4 1 4/8/2017 Genetic Sucrase-Isomaltase Deficiency (GSID) Activities Classification of Carbohydrates GSID comprises two activities1: — SUCRASE Sucrose = fructose + glucose Hydrolyzes α-1,2- and α-1,4- glucosidic bonds Digests g sucrose, maltose, and maltotriose — ISOMALTASE Maltose = glucose + glucose Hydrolyzes α-1,6 linkages Digests isomaltose, maltose, maltotriose, and limit dextrins GSID and maltase-glucoamylase (MGAM) are intricately involved in sucrose and starch digestion2,3 5 5 1. Nichols BL, Adams B, Roach CM, Ma CX, Baker SS. Frequency of Sucrase Deficiency in Mucosal Biopsies. J Pediatr Gastroenterol Nutr. 2012b;55:S28-S30. 2. Lin AH, et al. Direct Starch Digestion by Sucrase-Isomaltase and Maltase-Glucoamylase. J Pediatr Gastroenterol Nutr. 2012;55:S43-S45. 3. Lee B, et al. Inhibition of Maltase-Glucoamylase Activity to Hydrolyze α-1,4 Linkages by the Presence of Undigested Sucrose. J Pediatr Gastroenterol Nutr. 2012;55: S45-S47. Sucrose Digestion and Possible Clinical Implications Carbohydrate Digestion1 Starch Glycogen α-Dextrins Glucoamylase (Maltase) Isomaltase (Palatinase) Maltotriose Maltose α-1,6 α-1,4 5 60 25 25 20 25 25 20 50 50 Sucrase Membrane digestion TIME Sucrose Amylase Luminal digestion 95 Lactose Sucrose Pulls in excess water Numbers in circles indicate percentage of substrate hydrolyzed by brush border enzyme 100 Glucose Glucose Glucose Glucose Glucose Galactose Glucose Fructose LOW ENERGY LOW BLOOD SUGAR DIARRHEA Glucose 1. Wahbeh GT, Christie DL. Basic aspects of digestion and absorption. In: Wyllie R, Hyams J, Kay M, eds. Pediatric Gastrointestinal and Liver Disease. 4th ed. Philadelphia, PA: Elsevier; 2011:11. 7 SUCRASE Fermentation 100 100 Lactase Product H2O COLON Trehalase Glucose + Fructose H2O Trehalose 8 Please see Sucraid® (sacrosidase) Oral Solution Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 2 4/8/2017 Starch Digestion and Possible Clinical Implications #1 Why Should I Test for GSID? It’s So Rare TIME Starch dextrins Maltose Glucose + Glucose amylase – alpha glucoamylase – amylase -- isomaltase Prevalence MALTASE COLON +/- LOW ENERGY Fermentation Pulls in excess water +/- LOW BLOOD SUGAR GAS, DISTENTION BLOATING, +/- DIARRHEA 9 10 Let’s Talk Briefly about Prevalence… Genetic Sucrase-Isomaltase Deficiency (GSID) Historical data (1960 – 1970) for Genetic Sucrase-Isomaltase Deficiency (a genetically inherited autosomal recessive disorder)1 GSID originally thought to cause symptoms in autosomal recessive (homozygous) inheritance only Recent studies have demonstrated carriers may also present with symptoms1 — 5 – 10% in Greenland Eskimos — 3 – 7% in Canadian native peoples — 3% in Alaskans of native ancestry — <0.2% in non-Hispanic whites But, look at what we have learned since then… 1.Nichols BL, Adams B, Roach CM, Ma C, Baker S. Frequency of sucrase deficiency in mucosal biopsies. J Pediatr Gastroenterol Nutr. 2012;55(Suppl 2):S28-S30. 1.Treem, WR. Clinical aspects and treatment of congenital sucrase-isomaltase deficiency. J Pediatr Gastroenterol Nutr. 2012;55(Suppl 2):S7-S13. 11 12 3 4/8/2017 GSID Genetic Prevalence Study Genetic Results by Primary Symptom Potential Etiologies of Sucrase Deficiency Genetic Sucrase-Isomaltase Deficiency (GSID) Genotypes Congenital SucraseIsomaltase Deficiency (CSID) (Compound Heterozygotes) GSID Symptomatic Carriers (Simple Heterozygotes) Secondary Sucrase Deficiency Abdominal Pain Total n= 375 n= 375 N= 750 15 8 23 Celiac Disease Primary Variants (H t (Heterozygotes) t ) 0 2 2 Bacterial Overgrowth Secondary Variants (Heterozygotes) Compound Heterozygotes 1 0 1 Crohn’s Disease Other (e.g., blunted villi) 13 Diarrhea Please see Sucraid® (sacrosidase) Oral Solution Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. Total 16 10 26 Rate 4.3% 2.7% 3.5% 14 Frequency of Sucrase Deficiency in Mucosal Biopsies Review of Disaccharidase Analyses1 N=27,875 Prospective Disaccharidase Testing in Children with Recurrent Abdominal Pain1 Pilot Study N=28 9.3% [VALUE] Total Sucrase Deficiency (1.2 SD< Norm) # of subjects % of total Low Lactase 15 53.6 L Low S Sucrase 4 14 3 14.3 Low Maltase 5 17.9 Low Glucoamylase 4 14.3 Pan-Disccharidase Deficiency (all 4 low) 3 10.7 All Other Results 1.Nichols BL, Adams B, Roach CM, Ma C, Baker S. Frequency of Sucrase Deficiency in Mucosal Biopsies. J Pediatr Gastroenterol Nutr. 2012; 55 (Suppl 2):S28-S30. 15 1. Chumpitazi BP, et al. Yield of Prospective Disaccharidase Testing in Children with Recurrent Abdominal Pain. Gastroenterology. 2013;144(5 Suppl 1):S401-402. 16 4 4/8/2017 Retrospective Study of 963 Symptomatic Children Undergoing Upper Endoscopy and Disaccharidase Testing1 #2 Who Should Be Screened for GSID? Identifying y g the Patient 1. Cohen SA. The clinical consequences of sucrase-isomaltase deficiency. Molecular and Cellular Pediatrics. 2016;3;5. 17 18 Checklist for Considering GSID Reported Symptoms: Possible Diagnosis: - Chronic diarrhea - Viral/bacterial gastroenteritis - Abdominal pain - Parasitic diarrhea - Abdominal distension - Lactose intolerance - Excess gas - Celiac Disease - Excoriated buttocks - Inflammatory Bowel Disease - Vomiting - Crohn’s Disease - Failure to thrive - Ulcerative Colitis - Weight loss - Cystic Fibrosis - Constipation - Irritable Bowel Syndrome - Acid reflux - Genetic Sucrase-Isomaltase - Burping Initial Presentation of GSID in Infancy1 May not present until ~ 6 months - 1 year — Breast milk and standard infant formula (CHO source is lactose) are tolerated — First illness; antibiotic (high in sucrose) — Introduction of sucrose and/or starch — Formula, cereals, fruits, vegetables, and/or juice Often misdiagnosed as allergy or intolerance to cow’s milk or soy protein — Changing baby formula may actually worsen symptoms and delay diagnosis Deficiency 1. Treem WR. Congenital sucrase-isomaltase deficiency. J Pediatr Gastroenterol Nutr. 1995;21:1-14. 19 20 5 4/8/2017 Think about the Toddler with Chronic Diarrhea… Think about the Toddler with Chronic Diarrhea… Started with diarrhea around 6 months of age Reports no sweets and no nuggets or fries from McDonald’s Hospitalized with vomiting and diarrhea Typical intake at 3 y/o B: ham, egg Sn: potato chips or corn chips L: eats meat off sandwich D: mac and cheese Drinks: Peptamen Junior® Susceptible to infection, URIs Allergy testing all negative Tried Alimentum®, EleCare®, Neocate® Splash, Splash Peptamen Junior® Endoscopy with small bowel biopsies for disaccharidase assay — Low-sucrase — Low-glucoamylase (maltase) — Normal lactase — Normal mucosa 21 22 Think about Your Older Patients Diagnosed with IBS – Could It Be GSID? #3 What Kind of Diagnostic Testing Is Available? You’ve tried medications and various diets Patient finds some relief with Low FODMAPs* diet — But still has lingering symptoms: diarrhea, abdominal pain, gas, and bloating Diagnostic g Tools — And you believe they are compliant with the diet Consider testing for GSID (see #4 for diagnostic options) Sucraid® (sacrosidase) Consider a trial of Oral Solution therapy and diet modification (see #5 for treatment options) Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 23 24 6 4/8/2017 “Gold Standard” Diagnostic Test: Disaccharidase Activity Assay #3 Diagnostic Options for GSID Diagnostic Tests: — Upper Endoscopy – Small Bowel Biopsy - Dissacharidase Assay “Gold Standard” Normal Range — Trial Prescription of Sucraid® (sacrosidase) Oral Solution (µmol glucose/min/g protein) Prescription/order forms on Sucraid.net website Tests That Aid in Diagnosis — Sucrose Hydrogen Methane Breath Test (SHMBT) QOL Medical offers this test free of charge through Commonwealth Labs — Genetic Testing (buccal swab or saliva) Genetic Test Kits can be ordered free of charge from Sucraid.net Deficient (µmol glucose/min/g protein) Sucrase 29 0 – 79.8 29.0 79 8 <25 Maltase 98.0 – 223.6 <100 Palatinase 4.6 – 17.6 <5 Lactase 16.5 – 32.5 <15 Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 25 26 Pan-Disaccharidase Deficiency Sucraid® (sacrosidase) Oral Solution Therapy Do not discredit a Disaccharidase Assay where all 4 enzymes are deficient (pan-disaccharidase deficiency) If other more common GI disorders have been ruled out, it may be warranted to prescribe Sucraid® as a one to two week trial to see if the patient responds. In general, as people age, they are more likely to have a lactase deficiency: — Congenital lactase deficiency (in infants) is rare Order/prescription forms are available at www.sucraid.net — Approximately 65 percent of the human population has a reduced ability to digest lactose after infancy1 — It makes sense that an older child and certainly an adult could have both a lactase deficiency and Genetic Sucrase-Isomaltase Deficiency — QOL Observational Study of 49 Sucraid® patients; 25% also had a lactose intolerance Please see Sucraid® Important Safety Information and details on accessing the Full Prescribing Information in slides 37-39 Treat for both GSID and lactose intolerance 1. NIH – US National Library of Medicine Website. https://ghr.nlm.nih.gov/condition/lactose-intolerance#sourcesforpage. Accessed March 20, 2017 27 Please see Sucraid® (sacrosidase) Oral Solution Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 28 7 4/8/2017 Sucrose Hydrogen Methane Breath Test (SHMBT) Sucrose Hydrogen Methane Breath Test (SHMBT) A noninvasive, functional test to aid in identifying and diagnosing patients suffering with Genetic Sucrase-Isomaltase Deficiency (GSID) Prior to the SHMBT, patients are instructed to discontinue certain medications (probiotics, antibiotics) and follow a lowcarbohydrate diet one day before the test After a 12-hour overnight fast, the patient starts with a baseline breath sample sample, drinks a sucrose solution solution, and completes a series of breath samples (test is ~3 hours in all) SHMBT kits are available to healthcare professionals, including dietitians, for patient distribution at no charge (through QOL Medical, LLC) — Patients with GSID may experience GI symptoms due to the consumption of the sucrose solution and may prefer to take the test at home — Both hydrogen and methane gas production are measured Mal-digested sucrose results in an increase of these gases, due to bacterial fermentation Test results will be sent to the physician’s office within 48 hours of receiving the completed test kit 29 30 #4 How Do I Treat GSID? Genetic Testing Genetic Testing – no charge for the cost of the kit or testing Order genetic test kit from www.sucraid.net Treatment Options p Buccal B ccal sswab ab Test kit sent out to LabCorp Detects 37 known mutations Can help rule GSID in, but may not necessarily rule it out 31 Please see Sucraid® (sacrosidase) Oral Solution Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 32 8 4/8/2017 Patient Identified! What Are the Treatment Options? Infant Diet Guidelines for Patients Diagnosed with GSID Diet alone (low-sucrose and low-starch) Sucraid® (sacrosidase) Oral Solution - enzyme replacement therapy for the treatment of the genetically determined sucrase deficiency which is part of congenital sucraseisomaltase deficiency (CSID) Available on: CSIDcares org CSIDcares.org — Although Sucraid® provides replacement therapy for the deficient Sucraidassist.com sucrase, it does not provide specific replacement therapy for the deficient isomaltase Sucraid.net Combined diet and Sucraid® therapy Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 33 Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 34 Infant Diet Guidelines for Patients Diagnosed with GSID Infant Diet Guidelines for Patients Diagnosed with GSID Formula Starting Solids — Breast milk — Start solids as soon as age appropriate; don’t delay — Standard infant formula (lactose-based) — Abbott Nutrition RCF® no added carbohydrate — Start Sucraid® (sacrosidase) Oral Solution therapy when soy-based soy based formula starting solids Add dextrose or fructose Add water Provide mixing instructions Sucraid® has been tested in clinical trials with children 5 months of age and older — Start with low-sucrose, low-starch, pureed vegetables, fruits, and then meats; do not start with cereals 35 Please see Sucraid® (sacrosidase) Oral Solution Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 36 9 4/8/2017 Sucraid® (sacrosidase) Oral Solution Indication/Safety Information Sucraid® (sacrosidase) Oral Solution Indication/Safety Information INDICATION: IMPORTANT SAFETY INFORMATION (cont’d.): Sucraid® (sacrosidase) Oral Solution is an enzyme replacement Sucraid® may cause a serious allergic reaction. Patients should stop taking Sucraid® and get emergency help immediately if any of the following side effects occur: difficulty breathing, wheezing, or swelling of the face. Care should be taken when administering initial doses of Sucraid® to observe any signs of acute hypersensitivity reaction. reaction therapy for the treatment of the genetically determined sucrase deficiency, which is part of congenital sucrase-isomaltase deficiency (CSID). IMPORTANT SAFETY INFORMATION: Although Sucraid® provides replacement therapy for the deficient Adverse reactions as a result of taking Sucraid® may include worse Do not use Sucraid® (sacrosidase) Oral Solution with patients known to Before prescribing Sucraid® to diabetic patients, the physician should abdominal pain, vomiting, nausea, diarrhea, constipation, difficulty sleeping, headache, nervousness, and dehydration. sucrase, it does not provide specific replacement therapy for the deficient isomaltase. consider that Sucraid® will enable sucrose hydrolysis and the absorption of those hydrolysis products, glucose and fructose. be hypersensitive to yeast, yeast products, papain, or glycerin (glycerol). 37 38 Sucraid® (sacrosidase) Oral Solution Dosing and Administration Sucraid® (sacrosidase) Oral Solution Indication/Safety Information IMPORTANT SAFETY INFORMATION (cont’d.): Sucraid® must be kept refrigerated The effects of Sucraid® have not been evaluated in patients with Dosing: secondary (acquired) disaccharidase deficiency. — 1 mL (28 drops) if ≤ 15 kg (≤ 33 lbs) — 2 mL (56 drops) if > 15 kg (> 33 lbs) DO NOT HEAT SOLUTIONS CONTAINING SUCRAID®. Do not put Sucraid® Sucraid® in warm or hot fluids. Do not reconstitute or consume with fruit juice since the acidity of the juice may reduce the enzyme activity of Sucraid®. Half of the reconstituted Sucraid® should be taken at the beginning of the meal or snack and the other half during the meal or snack. Mixing: — Mix Sucraid® in 2 – 4 ounces of milk, water, or sucrose-free, starch- free formula Do not mix in hot beverages; do not heat after mixing Administer Sucraid® with every meal or snack Sucraid® should be refrigerated at 36°F-46°F (2°C-8°C) and should be — Take ½ at beginning of meal/snack and other ½ during meal/snack protected from heat and light. FULL PRESCRIBING INFORMATION was provided at the beginning of this presentation and can be accessed online at sucraid.net/pi.pdf. Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 39 40 10 4/8/2017 Treatment Plan for Previously Discussed Toddler (GSID Confirmed by Biopsy) Formula Options for Our Toddler… Start Sucraid® (sacrosidase) Oral Solution therapy FORMULA Modified diet/elimination (sucrose and starch) Consider changing formula to RCF® (Abbott) or KetoCal® (Nutricia) PROTEIN SOURCE CARB SOURCE FAT SOURCE Portagen® (Mead Johnson) Sodium caseinate Corn syrup solids, sugar MCT, corn oil % of Kcals RCF® (Abbott) 14% Soy protein isolate 46% None 40% Safflower oil, soy oil, coconut oil % of Kcals KetoCal® 4:1 (Nutricia) % of Kcals 14% Milk protein (casein, whey) 8.2% 0 Corn syrup solids 86% Vegetable oil 3.1% 88.7% Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 41 42 A Comparison of Other Elemental Formulas Often Trialed, But Failed… FORMULA CARB SOURCE FAT SOURCE casein Similac hydrolysate Alimentum® (Abbott) EleCare® (Abbott) amino acids sugar, modified tapioca starch safflower oil, MCT, soy oil corn syrup solids amino acids corn syrup solids amino acids maltodextrin, sugar safflower oil, MCT, soy oil vegetable oil, canola oil, safflower oil coconut oil, canola oil, sunflower oil MCT, soybean oil, canola oil Neocate (Nutricia) Jr® Splash® (Nutricia) Peptamen, Jr® (Nestle) PROTEIN SOURCE hydrolyzed whey protein maltodextrin, sugar, cornstarch Child or Adult Diet Guidelines for Patients Diagnosed with GSID Begin Sucraid® (sacrosidase) Oral Solution therapy Elimination Diet (2 weeks) – eliminate the culprits — Sucrose — Starch, maltose — Others Symptom improvement is generally seen within these first two weeks Induction Diet – establish tolerance to sucrose and starch — Sucrose (Sucraid® may allow for a nearly “normal” intake of sucrose) — Starch tolerance will vary significantly (Sucraid® does not replace isomaltase) Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 43 44 11 4/8/2017 Child and Adult Diet Guides Menu Guide Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 45 Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 46 Why Do Patients with GSID Need to See a Registered Dietitian? Why Do Patients with SI Deficiency Need to See a Registered Dietitian? Sucrose and starch modifications are difficult to understand, making the diet hard to follow for newly diagnosed patients: Continued… — Many patients may have other diagnoses and diet restrictions to contend with: — Food labels do not provide sucrose and starch content — Most nutrient databases do not have complete sucrose and starch data — People do not think in terms of sucrose and starch; they are more Lactose intolerance Wh t or gluten Wheat l t sensitivity, iti it Celiac C li Di Disease, or food f d allergies ll i IBS/low FODMAPs diet Milk protein intolerance — They may be given a list of what NOT to eat, but do not likely to think in terms of sugars and carbohydrates, but even those terms are not always familiar to the general population know what they CAN eat! Improper diet modifications and restrictions increase risk of nutrient deficiencies 47 48 12 4/8/2017 Nutrition Topics to Cover with Patients What is sucrose? What is starch? What are acceptable alternatives to cow’s milk? How much sucrose/starch is too much? How much sucrose/starch is not enough? How to read a food label? Grams of Sucrose per Meal/per Day? Compliance with a sucrose-free diet is very difficult What artificial sweeteners are acceptable? Is gluten-free low in starch? Following an elimination diet, sucrose can be increased by ~0.5 g/day or more What about 100% fruit juice? Add back sucrose via fruits and healthier “sugar” g foods first What about FODMAPS, SCD? Sucraid® (sacrosidase) Oral Solution will cover a significant amount of sucrose in the diet, but tolerance is variable and depends on the individual How do I meet calorie needs? Where do I buy fructose and dextrose? What about lactose, fructose? Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 49 50 Grams of Starch per Meal/per Day? Nutrient Data for Sucrose and Starch Although Sucraid® (sacrosidase) Oral Solution provides replacement therapy for the deficient sucrase, it does not provide specific replacement therapy for the deficient isomaltase; starch tolerance is highly variable Sucrose and starch information are not found on food labels “Cracker Cracker Test”; Test ; adding 1 Saltine cracker/day (2 g starch per day) University y of Minnesota Nutrition Data System y for Research (NDSR) has complete sucrose and starch data Ann McMeans, RD suggests 120 grams/day may be tolerated1 Total carbohydrates, total sugars, and fiber are on Nutrition Facts Label Sucrose and starch data are not a part of most nutrient databases; USDA has limited information, but adding to it The type of starch may allow more grams per day Total CHOs – total sugars – fiber = starch Chewing food well – exposing to amylase longer Type(s) of sugar and starch sources are listed on the ingredient label, but patients must learn to be ingredient detectives Some take over-the-counter “starch enzymes” 1. McMeans AR. Congenital Sucrase-Isomaltase Deficiency: Diet Assessment and Education Guidelines. J Pediatr Gastroenterol Nutr. 2012;55(2):S3739. Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 51 52 13 4/8/2017 QOL Observational Study1 QOL Observational Study1 49 subjects on Sucraid® (sacrosidase) Oral Solution % of Total CHOs — >3 months on therapy AVG for All Subjects (%) Typical American Diet (%) 12 – 39 49 Maltose 1–2 N/A Sucrose 11 – 14 N/A — Age ranged 1 – 45 years 24-hour dietary recalls; three consecutive days % of Total Kcals Starch AVG for All Subjects (%) DRI (%) CHO 42 45-65 FAT 39 25-40 PRO 18 5-35 1. Boney A, Elser H, Silver HJ. Relationships Between Dietary Intakes and Persistent Gastrointestinal Symptoms in Patients on Enzyme Treatment for Genetic Sucrase-Isomaltase Deficiency. In: World Congress of Pediatric Gastroenterology, Hepatology and Nutrition; October 5-8, 2016; Montreal, Canada. 1. Boney A, Elser H, Silver HJ. Relationships Between Dietary Intakes and Persistent Gastrointestinal Symptoms in Patients on Enzyme Treatment for Genetic Sucrase-Isomaltase Deficiency. In: World Congress of Pediatric Gastroenterology, Hepatology and Nutrition; October 5-8, 2016; Montreal, Canada. Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 53 54 QOL Observational Study1 Tolerance to Sweeteners Sweeteners “tolerated by most” Top Five Sucrose Sources: — Dextrose and Fructose — cake/pie, donut, ice cream, frozen desserts, espresso/chocolate — High Fructose Corn Syrup milk — Aspartame (NutraSweet®) Top Five Starch Sources: Sweeteners “tolerated by y some” — pizza, pasta, potato, brown rice, bread — Acesulfame K (Sweet One®) — Agave nectar (primarily glucose and fructose) — Equal® (aspartame based) Top Five Maltose Sources: — Honey (primarily glucose and fructose) — breakfast cereal, chips, pancake syrup, tortilla, CLIF Bar — Saccharin (Sweet’N Low®) — Increased maltose associated with increased GI symptoms — Stevia® — Sucralose (Splenda®) — Sugar alcohols 1. Boney A, Elser H, Silver HJ. Relationships Between Dietary Intakes and Persistent Gastrointestinal Symptoms in Patients on Enzyme Treatment for Genetic Sucrase-Isomaltase Deficiency. In: World Congress of Pediatric Gastroenterology, Hepatology and Nutrition; October 5-8, 2016; Montreal, Canada. 55 56 14 4/8/2017 Tolerance to Sweeteners Starch Ingredients That May Not Be Tolerated Sweeteners to “Avoid”; Sucrose: Limit dextrins — Beet sugar Maltodextrin — Brown sugar — Cane juice, cane sugar Modified tapioca starch — Caramel Glucose polymers — Coconut sugar — Confectioner’s sugar Maltose — Date sugar — Maple syrup — Brown rice syrup — Molasses — Corn syrup solids — Raw sugar — Sucrose — Malt — Sugar 57 58 Fruit Juice Differences Between Elimination Diets Low FODMAPs JUICE (4 fluid ounces) 59 SUCROSE STARCH GLYCEMIC INDEX FRUCTOSE GLUCOSE MALTOSE LACTOSE Dairy No (some cheese) Low Sucrose, Low Starch Yes JJ APPLE 1.6 6 0 39 7.1 7 3.3 3 3 0 0 Fat Yes Yes JJ GRAPE 0.8 0 50 8.2 5.9 0 0 Protein (meats) Yes Yes LIBBY’S PEAR 0.3 0 64 10.7 7.3 0 0 Starch/grains Yes (selected) No ORANGE JC, fresh 5.0 0 46 2.8 2.6 0 0 Fruits Yes (low fructose) Yes (low sucrose) PINEAPPLE JC 1.9 0 46 4.8 5.8 0 0 Vegetables Yes (selected) Yes (low starch) PRUNE JC 0.3 0 29 10.1 7.0 0 0 “Sugars” APPLE-GRAPE DRINK 7.4 0 67 3.3 3.7 0 0 No fructose; No sucrose; Yes (sugar, syrup, jelly) Yes (fructose, dextrose) TOMATO JUICE 0.3 0 33 1.9 1.6 0 0 60 15 4/8/2017 Case Study – RD Intervention 4-year-old female presented to RD with IBS for education on low FODMAPs diet Patient showed some improvement on diet, but still with GI symptoms — FODMAPs does not restrict sucrose and starch RD recalled our conversation about SI deficiency and Sucraid® (sacrosidase) Oral Solution therapy RD probed and thought perhaps this could be “one of those patients” RD recommended the MD order a trial of Sucraid® After 10 days on Sucraid®, BMs normalized and all other symptoms improved — This child’s symptoms began around 1 year of age — She was 4 years old before GI symptoms resolved — Genetic testing was negative Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 61 62 Allowed or Not Allowed on Elimination Phase of A Low-Sucrose, Low-Starch Diet Apple Olives Cracker QOL Medical, LLC Offers a Variety of Services to Healthcare Providers and Their Patients One Patient Services – SucraidASSIST™ Nurse Case Manager Banana Tomato Eggs g cheese Cottage Nuts Blueberries Gluten-Free Insurance Specialist Dietitian Di titi Peer Coach Grapes p Butter Green beans Websites: Black-eyed peas SucraidAssist.com CSIDcares.org Sucraid.net Yogurt 63 not tolerated by most tolerated by most Point of contact for all needs (patients and clinicians) Prescriptions, forms, paperwork, tracking All questions 1-800-705-1962 Please see Sucraid® Important Safety Information on slides 37-39 and Full Prescribing Information passed out at the beginning of this presentation. Sucraid® may cause a serious allergic reaction. 64 16 4/8/2017 Thank You! Questions? Anne Boney, MEd, RD, LDN 1-800-705-1962, ext. 1001 1-919-832-0404 [email protected] Thank you for the opportunity to share this presentation with you today! SUC17.1019b 04/2017 65 66 17