Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
605
Relation of Mitochondrial and Cytosolic Free
Calcium to Cardiac Myocyte Recovery
After Exposure to Anoxia
Haruo Miyata, Edward G. Lakatta, Michael D. Stern, and Howard S. Silverman
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
Mitochondrial calcium overload has been suggested as a marker for irreversible injury in the ischemic
heart. A new technique is used to measure dynamic changes in mitochondrial free calcium concentration
([Ca2+]m) in electrically stimulated (0.2 Hz) adult rat cardiac myocytes during exposure to anoxia and
reoxygenation. Cells were incubated with indo-1 AM, which distributes in both the cytosol and
mitochondria. After Mn2+ quenching of the cytosolic signal, cells were exposed to anoxia, and the residual
fluorescence was monitored. [Ca2+]. averaged 94±3 nM (n=16) at baseline, less than the baseline
diastolic cytosolic free calcium concentration ([Ca 2+] 124±4 nM, n=12), which was measured in cells
loaded with the pentapotassium salt of indo-1. [Ca2+]m and [Ca 2+1c rose steadily only after the onset of
ATP-depletion rigor contracture. At reoxygenation 35 minutes later, [Ca2+1k fell rapidly to preanoxic
levels and then often showed a transient further rise. In contrast, [Ca2+]m showed only a slight transient
fall and a secondary rise at reoxygenation. At reoxygenation, cells immediately either recovered,
demonstrating partial relengthening and retaining their rectangular shape and response to stimulation,
or they hypercontracted to rounded dysfunctional forms. Recovery occurred only in cells in which [Ca'2+LI
or [Ca2+1k remained below 250 nM before reoxygenation. Early during reoxygenation, [Ca21]m remained
higher in cells that hypercontracted (305±36 nM) than in cells that recovered (138±9 nM, p<0.05),
whereas [Ca211k did not differ between the two groups (156+ 10 versus 128+ 10 nM, respectively; p=NS).
The role of the sarcoplasmic reticulum in Ca2+ regulation was evaluated in cells (n=16) pretreated with
thapsigargin, an inhibitor of the sarcoplasmic reticulum Ca2+-ATPase. During anoxia [Ca21]c and
[Ca2+1L rose as they did without thapsigargin pretreatment. At reoxygenation, the rapid fall in [Ca2%]c
was blunted, and [Ca2+1m showed an immediate increase in these cells, demonstrating the importance of
the sarcoplasmic reticulum in postanoxic Ca21 regulation. In summary, cellular hypercontracture is not
associated with a sudden and massive rise in [Ca2+]1 immediately after reoxygenation. The basis for the
relation between [Ca21]m and cellular recovery as well as the mechanisms underlying the observed
changes in [Ca2+]m remain to be defined. (Circulation Research 1992;71:605-613)
KEY WoRDs * mitochondrial [Ca2+] * cytosolic [Ca21] * indo-1 * anoxia * reoxygenation myocytes
,
D uring the past two decades, attention has focused on the role of calcium in ischemic
myocardial injury. Only recently has it been
possible to measure intracellular ionized calcium in
cardiac tissue. Although numerous studies suggest that
calcium loading leads to myocyte death,1-6 it remains
unclear how calcium mediates cell injury. Although a
number of investigators have found a correlation between cytosolic calcium levels and cell hypercontracture
after hypoxia, a recent report5 demonstrated that cytosolic free calcium concentration ([Cac2+]) actually falls
From the Laboratory of Cardiovascular Science (H.M., E.G.L.,
M.D.S., H.S.S.), Gerontology Research Center, National Institute
on Aging, and the Department of Medicine (E.G.L., M.D.S.,
H.S.S.), Division of Cardiology, Johns Hopkins Medical Institutions, Baltimore, Md.
Supported in part by National Heart, Lung, and Blood Institute
grants RO1 HL-42050 and K08 HL-02539. H.S.S. was supported
in part by a Lilly Clinician Scientist Award.
Address for correspondence: Howard S. Silverman, MD, Division of Cardiology, Johns Hopkins Hospital, 600 N. Wolfe Street,
Baltimore, MD 21205.
Received November 13, 1991; accepted May 4, 1992.
early in reoxygenation despite cell hypercontracture.
Although [Ca2]c fell, cell calcium uptake (measured
with 45Ca) increased, compatible with calcium uptake by
intracellular organelles, namely the sarcoplasmic reticulum and mitochondria. In this study we use a new
technique to examine mitochondrial calcium regulation
and its relation to myocyte recovery after glucose-free
anoxia. Exchange of calcium between the cytosol and
mitochondria in cardiac muscle plays an important role
in energy balance, through the Ca2` sensitivity of the
activities of the pyruvate dehydrogenase complex,
NAD-isocitrate dehydrogenase, and a-ketoglutarate
dehydrogenase.7-9 Although modest increases in mitochondrial free calcium concentration ([Ca`+]m) enhance
enzymatic activity and subsequent ATP synthesis, massive mitochondrial calcium loading may disable ATP
synthetic pathways.10"'1 Mitochondria store small
amounts of exchangeable calcium under normal conditions but have a large capacity to accumulate and buffer
calcium under states of high cellular calcium loading."
Mitochondrial Ca`+ deposits have been considered to
be an ultrastructural hallmark of irreversible ischemic
606
Circulation Research Vol 71, No 3 September 1992
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
cell injury in the heart1 and have been documented in
isolated cardiac myocytes exposed to prolonged
anoxia.'2
Despite its importance, [Ca2+]m has not been measurable in living cells. Studies have used electron probe
microanalysis, a technique that provides single measures of mitochondrial total matrix calcium,13 or isolated mitochondrial suspensions loaded with calciumsensitive fluorescent indicators.14 A recent report from
this laboratory15 introduced a technique that allows the
continuous measurement of [Ca`+]m in single cardiac
myocytes. The calcium-sensitive fluorescent probe
indo-1 is loaded into myocytes by incubation with the
membrane-permeant AM form. By using this loading
technique, roughly half of the indo-1 partitions into the
mitochondria. This signal can be monitored continuously once the cytosolic component is quenched by
superfusing the cells with manganese chloride. The
present study examines the relation between [Ca 2+]m,
[Ca2+]c, and cell recovery in cardiac myocytes exposed
to glucose-free anoxia and reoxygenation. The role of
the sarcoplasmic reticulum in regulating [Ca2+] is examined. These studies demonstrate reversible rises in both
[Ca2+]m and [Ca]2+] during anoxia and suggest that
cytosolic calcium overload per se does not fully account
for cellular injury. After reoxygenation, persistent elevation in [Ca2+]m, but not [Ca2+'], is correlated with cell
hypercontracture.
Materials and Methods
Single cardiac myocytes were isolated from rats according to a previously described technique.1617 After
isolation, cells were loaded with indo-1 by exposure to
the acetoxymethyl ester (indo-1 AM) at a concentration
of 25 ,uM for 10 minutes, then washed, and incubated at
23°C for more than 1 hour. A small portion of the
suspension of indo-1-loaded cells was placed in an
experimental chamber, which was mounted on the stage
of an inverted microscope. The majority of cells were
studied in a solution containing (mM) NaCl 144, KCl 5,
MgSO4 1.2, and HEPES 20 (pH 7.4) plus Ca2+ 1, with
0.5 mM octanoate as respiratory substrate. A few cells
were studied in a solution containing (mM) NaCl 116,
KCl 5, MgSO4 1.2, NaH2PO4 1.2, NaHCO3 26, CaCl2 1,
and octanoate 0.5 (pH 7.4). The myocyte to be studied
was illuminated with a red light, and its image was
visualized with a solid-state TV camera. Cell length was
monitored by projecting the cell image onto a photodiode array. Epifluorescence of indo-1 was excited by
light from a pulsed xenon arc. Exciting light at 350 nm
was selected by a 5-nm bandwidth filter; emitted light
was monitored in the wavelength ranges of 391-434 nm
("410" channel) and 477-507 nm ("490" channel),
corresponding to the peak emission of the Ca2+-bound
and Ca2+-free forms of the indicator, respectively, by a
pair of photomultiplier tubes (EMI 989313/350). Full
details of the instrumentation are given in a previous
communication. 18
To obtain values of [Ca 2+i, the ratio of emission
intensity in the 410-nm and 490-nm channels obtained
after subtracting cell autofluorescence at each wavelength was compared with ratios obtained using a
solution of indo-1 pen.apotassium salt (2.5 ,M) in
physiological saline and containing Ca 2+ EGTA buffers
of known Ca 2+ concentration. The results of the indo-1
salt calibration were similar to those obtained when
AM-loaded myocytes were treated with respiratory inhibitors and ionophores to equilibrate membrane potential, pH, and Ca 2+ across the cell membranes by
using a wide range of Ca' EGTA buffers. Full details
are given in an earlier publication.'8 [Ca'2]m was measured by superfusing the AM-loaded cells with 100 ,uM
MnCl2 for 30 minutes to quench the companion cytosolic signal. This process did not alter cell contraction
but did eliminate the cytosolic contribution to the
fluorescence signal. The validation of this technique is
described in a previous report.15
To measure [Ca2+]c, cardiac myocytes were loaded
directly with indo-1 salt during isolation.19 After perfusion with collagenase and protease, the left ventricle
was excised and mechanically dissociated in 2 ml
HEPES-buffered preparation medium containing 1 mM
indo-1 (pentapotassium salt) and 250 ,M CaCl2. After
10-15 minutes of gentle agitation, cells were resuspended in HEPES-buffered medium, and the Ca 2+
concentration was gradually increased to 1 mM, and
indo-1 was washed away. Systolic and diastolic values of
[Ca2+]c determined by this method were consistent with
those found by loading indo-1 into the cytosol with a
micropipette. All studies were conducted at 23°C to
minimize loss of the fluorescent indicator, a particular
problem in the free-acid-loaded cells.
It is established that the calcium sensitivity of indo-1
is affected by pH.20 Specifically, as pH decreases the Kd
for the indo-1/Ca' complex increases, which, if not
considered, would lead to a false underestimate of true
[Ca2+]. Significant effects on the Kd for calcium binding
occur only when pH falls below 6.8. In preliminary
experiments using cells studied in a bicarbonate-based
buffer and loaded with the pH-sensitive fluorescent
probe carboxyseminaphthorhodofluor, we have found
that cytosolic pH shifts from a control level of 7.33 +0.03
to 7.15±+0.04 during ATP-depletion contracture (n=7
cells). Mitochondrial pH, which is normally maintained
alkaline relative to the cytosol, would not be expected to
fall much below cytosolic levels. Since these shifts in pH
would not be expected to significantly affect the Kd of
indo-1, no effort to correct the data for pH changes was
made. In addition, in previous experiments with isolated
mitochondria, the Kd of the mitochondrial indo-1/Ca2
complex was not found to differ significantly from the
values obtained in solution.14
Cells were also studied in the continued presence of
200 nM thapsigargin, a specific inhibitor of the sarcoplasmic reticulum ATP-dependent Ca2+ pump,21 to
assess the role of sarcoplasmic reticulum in the regulation of [Ca2+] during and after anoxia.
Exposure to Anoxia
Experiments were performed on the stage of an
inverted microscope in a specially developed chamber
fully detailed in a prior publication.17 Briefly, individual
myocytes were made anoxic using the laminar counterflow barrier well, an open chamber in which oxygen is
excluded by a laminar flow of ultrahigh-purity argon.
HEPES-based buffer was equilibrated with 20% 0280% argon (normoxia) or 99.9995% pure argon (anoxia). Bicarbonate-based buffer was equilibrated with 5%
C02-20% 02-75% argon (normoxia) or 5% C02-95%
argon (anoxia). Cells exposed to anoxia remained mor-
Miyata et al Mitochondrial [Ca2+] in Anoxic Myocytes
607
W
zE
14w P.
-oU-
S0
ZDFE
00
_iiA
-ct
77.4J
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
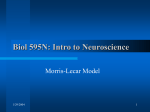
FIGURE 1. Recordings showing mitochondrial and cytosolic [Ca 2+] in cells recovering from anoxia and reoxygenation. Left
panel: Simultaneous recording of Mn2'-quenched indo-1 fluorescence ratio (top tracing), calculated mitochondrial [Ca 2+
(middle tracing), and cell length (bottom tracing) from a typical cell. Small arrow indicates onset of anoxia; large arrow indicates
point of reoxygenation. Cell contracture is displayed by the sudden marked cell shortening that occurs during anoxia. Right panel:
Recording from another cell displaying indo-1 fluorescence ratio (top tracing), cytosolic [Ca 2+] (middle tracing), and cell length
(bottom tracing).
phologically normal (i.e., rectangular) for a variable
period of time and then rapidly shrank longitudinally,
over approximately 1 minute, to become "square" or
"brick-shaped" rigor forms, which were morphologically
inert as long as the cells remained anoxic. Myocytes
were reoxygenated 35 minutes after they underwent
rigor contracture. At reoxygenation, cells immediately
experienced one of two distinct outcomes: they either
partially relengthened, retaining their rectangular
shape, sarcomere pattern, and response to electrical
stimulation (recovery), or rapidly crushed into rounded
blebbed forms with absent sarcomere pattern and disordered myofibrils (hypercontracture). Though recovery was accompanied by relengthening of only a few
microns, cellular structure and contractile function were
preserved, distinguishing these cells clearly from those
that hypercontracted. These changes were consistent
with those reported in our prior studies.6'22
Statistical Analysis
Means±SEM were obtained for each group. Intercomparisons were made using Student's t test or
analysis of variance where appropriate. Categorical data
were compared using X2 analysis. Analysis of covariance
(SYSTAT software package, SYSTAT Inc., Evanston, Ill.)
was used to test differences in Ca21 uptake rates.
Statistical significance was identified as the 95% confidence level.
group
Results
[Ca2+Im was measured in 16 individual indo-1 AMloaded myocytes by monitoring fluorescence after superfusion of the cells with Mn21 to quench the cytosolic
component of the fluorescent signal. Cell length was
monitored simultaneously. During exposure to anoxia,
the electrically stimulated twitch contraction was preserved for a variable time period (27±+2 minutes). This
was followed by the abrupt onset of contractile failure.
Three to 5 minutes later, cells suddenly shortened to
assume a square, morphologically inert rigor form associated with profound intracellular ATP depletion.23
This state was maintained until oxygen was readmitted
35 minutes later. The left panel of Figure 1 shows a
recording from a typical cell. The bottom tracing displays cell length. The marked rapid shortening of the
cell indicates the onset of rigor contracture. The
changes in cell morphology and contraction were identical to those observed in our prior studies using myocytes that were not loaded with fluorescent indicators.22'24 At reoxygenation (large arrow), this cell
recovered, demonstrating partial relengthening, and
once again responded to electrical stimulation. Of the
16 cells studied, seven recovered at reoxygenation,
whereas nine showed further shortening (hypercontracture) and developed into dysfunctional rounded forms.
The mitochondrial indo-1 fluorescence signal for this
same cell is displayed in the top tracing. Changes in the
fluorescence ratio are used to monitor [Ca 2+Im. During
anoxia, the fluorescence ratio remained unchanged until the onset of contracture. The signal then showed a
brief abrupt rise followed by a more gradual steady rise
as anoxia was continued. At reoxygenation, the ratio fell
and then showed a transient overshoot followed by a
gradual recovery toward control values. The calculated
[Ca2+]m is displayed in the middle tracing. This value is
derived using the calibration values obtained from indoloaded cells exposed to ionophores and metabolic inhibitors in the presence of buffers with varying calcium
concentration. The final calculated values account for
average changes in cellular autofluorescence that are
due to changes in the redox state of NAD, which are
induced by exposure to anoxia and then by subsequent
reoxygenation. Autofluorescence, measured in a separate set of non-dye-loaded cells, abruptly increased by
36±4% and 45+5% in the 410- and 490-nm channels,
respectively (n= 10 cells), during anoxia and rapidly
decreased to 90±4% of control values in both channels
at reoxygenation.
The right panel of Figure 1 demonstrates the typical
changes that occur in [Ca 2+] during exposure to anoxia.
It is a recording from one of 12 cells studied that were
loaded directly with indo-1 free acid. The top and
bottom tracings show the indo-1 fluorescence signal and
cell length, respectively. The middle tracing represents
608
Circulation Research Vol 71, No 3 September 1992
0.6
W-J
_i
0
:E
.+
0
JE
k
_J
.,
.
0 _j
::
0
0.064
I-
130. _
-_Z---k9 E
WZ 5.
UW-
~JF
-J
-J
5min
69.9
5 min
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
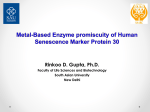
FIGURE 2. Recordings showing mitochondrial and cytosolic [Ca 2+] in cells that hypercontracted at reoxygenation. Left panel:
Simultaneous recording of calculated mitochondrial [Ca 2+] (top tracing) and cell length (bottom tracing) from a typical cell.
Small arrow indicates onset of anoxia; large arrow indicates point of reoxygenation. The further cell shortening at reoxygenation
is associated with an irreversible loss of sarcomere structure. Right panel: Recording of cytosolic [Ca 2+ (top tracing) and
simultaneous cell length (bottom tracing) from another cell.
the calculated [Ca'2+]. These values were derived using
calibration methods identical to those for [Ca'2+]m. Exposure to anoxia caused a modest decrease in the
amplitude of cell contraction as well as a decrease in the
amplitude of the intracellular calcium transient. After a
lag period, the contraction and calcium transient were
abruptly abolished. The cell then underwent contracture followed by a gradual rise in [Ca2+]c. At reoxygenation, the cell recovered, displaying partial relengthening as [Ca2+], fell within 1 minute to preanoxic levels.
The electrically stimulated calcium transient was restored within 3 minutes. In this cell, recovery of the
electrically stimulated contraction was minimal. This
was occasionally the case when cells were reoxygenated
after long periods of energy depletion.
The changes in both [Ca2.]m and [Ca2"]c seen in cells
recovering from hypoxic exposure were smaller than
those seen in cells that hypercontracted on readmission
of oxygen. Nine of 16 cells in which [Ca 2+]m was
monitored and eight of 12 cells in which [Ca2+Jc was
monitored hypercontracted at reoxygenation after 35
minutes of exposure to anoxia. Data from two of these
cells are shown in Figure 2. [Ca2.]m is displayed in the
left panel of Figure 2, and [Ca 2+]C is displayed in the
right panel. The time course of changes in [Ca 2+] in
both the mitochondrial and cytosolic compartments
qualitatively resembled those seen in cells recovering at
reoxygenation, although the absolute levels achieved
during anoxia were greater in this group. Importantly,
[Ca 2+]C showed a rapid transient fall to preanoxic levels
at reoxygenation despite the fact that these cells were
morphologically irreversibly damaged at this time. In
contrast, [Ca 2+]m showed a modest fall and a secondary
rise at reoxygenation.
Table 1 summarizes the mean [Ca 2+] data for all cells
studied and contrasts values from cells that recovered
with those that hypercontracted. Several important observations emerge. For the group as a whole, baseline
levels of diastolic [Ca 2+] exceeded those of [Ca 2+]m. The
levels of [Ca 2+]m and [Ca 2+]c achieved just before reoxygenation were markedly greater in those cells that
hypercontracted compared with those cells that recovered at reoxygenation (p<0.05). [Ca2+]c fell to baseline
levels in the first minute after reoxygenation in cells that
recovered as well as in cells that hypercontracted
(p=NS versus baseline in both groups at 1 minute after
reoxygenation). In contrast, [Ca2+]m at reoxygenation
remained significantly above baseline in both groups
(p<0.05). Levels of [Ca2']m were persistently higher in
cells that hypercontracted than in cells that recovered at
both 1 and 5 minutes after reoxygenation. The corresponding values for cell length for all cells are displayed
in Table 2.
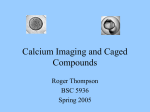
[Ca2+]m and diastolic [Cac2+] at control, just before
reoxygenation, and at 1 and 5 minutes after reoxygenation are plotted for each of the studied cells in Figure
3. The data are divided into two groups based on the
morphological outcome of cells at reoxygenation. A
threshold value of [Ca 2+] is observed in both the
mitochondrial and cytosolic compartments; cells uniformly recovered if these values were below 250 nM just
before reoxygenation. Values exceeding this limit were
uniformly associated with cell destruction.
Sixteen additional cells were exposed to anoxia and
reoxygenation in the presence of thapsigargin to disable
TABLE 1. Mean Mitochondrial and Cytosolic [Ca2+] in Recovered and Hypercontracted Cells
Recovered
Hypercontracted
p
Mitochondrial [Ca 2+] (nM)
Control
92-+-4
94-+-2
NS
End anoxia
157+18
404+39
<0.05
Reox 1 min
138+9
305+36
<0.05
Reox 5 min
210+15
383+44
<0.05
n
7
9
...
Diastolic cytosolic [Ca 2+] (nM)
Control
119+3
126+9
NS
End anoxia
197+23
430+35
<0.05
Reox 1 min
128+10
156+10
NS
Reox 5 min
142+8
212+26
<0.05
n
4
8
...
Control, values obtained before anoxia; end anoxia, 35 minutes
after ATP-depletion contracture; Reox 1 min and Reox 5 min, 1
minute and 5 minutes after reoxygenation, respectively; n, number
of cells. [Ca 2+] values are mean+SEM.
Miyata et al Mitochondrial [Ca2"] in Anoxic Myocytes
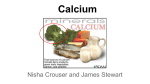
the sarcoplasmic reticulum. Five (31%) of 16 cells
recovered after reoxygenation. The fraction of cells
showing recovery was no different from that seen in
cells studied in the absence of thapsigargin (i.e., 11
[39%] of 28 cells,p=NS). [Ca2+]m and [Ca2"]J rose after
the onset of rigor contracture. [Ca2]1]m rose to 409+43
nM just before reoxygenation in five cells that hypercontracted after reoxygenation. [Ca 2+] rose similarly
during anoxia to 421±46 nM in six cells that hypercontracted after reoxygenation. These values do not differ
from those obtained in cells studied in the absence of
thapsigargin (p=NS). Raw data from two cells studied
in the continued presence of 200 nM thapsigargin are
shown in Figure 4 ([Ca 2+Ini and cell length in the left
panel and [Ca21]. and cell length in the right panel).
Figure 5 displays representative raw data tracings from
four separate cells and shows the changes that occur in
[Ca21] immediately after reoxygenation on an expanded
time base. [Ca 2+]m is displayed in panels A and B, and
TABLE 2. Cell Length in Recovered and Hypercontracted Cells
Cell length (gm)
p
Hypercontracted
Recovered
Manganese-quenched indo-1 AM-loaded cells
NS
127.0+13.0
131.5±11.5
Control
NS
80.1±12.9
87.5±9.1
Rigor
<0.05
56.7±18.0
89.8±8.0
Reox
...
9
7
n
Indo-1 salt-loaded cells
NS
120.3±4.6
137.3±5.3
Control
NS
71.9±3.9
84.6±4.5
Rigor
<0.05
52.6±6.6
90.5±5.5
Reox
...
8
4
n
Control, values obtained before anoxia; Reox, values after
reoxygenation; n, number of cells. Length values are mean±SEM.
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
HYPERCONTRACTED
RECOVERED
600,
600
:
609
400l
X
h-
11
400
1-1
+
Ct
to
U 200
0.
200
oa
0
Cont Rigor Reox 1
Reox 5
Cont Rigor Reox 1
HYPERCONTRACTED
RECOVERED
600
Reox 5
64
A
DO
v
W
x 400
X
illV
4C
0
0
CV
0
2
v
Nd
CV)U
200
20
(A~~~~~~
0
Cont Rigor Reox 1
Reox 5
Cont Rigor Reox 1
Reox 5
FIGURE 3. Plots showing mitochondrial [Ca 2+] ([Ca 2+]m) and diastolic cytosolic [Ca 2+] ([Ca 2+]) as a function of cell
Top panels: [Ca2+]m (n=16) is displayed for each cell at baseline (Cont), end anoxia (Rigor), 1 minute
after reoxygenation (Reox 1), and 5 minutes after reoxygenation (Reox 5). Data from cells that recovered are displayed on the left,
and data from cells that hypercontracted are displayed on the right side of the figures. Bottom panels: [Ca 2+] (n=12) is
displayed. The time points are as above.
outcome at reoxygenation.
610
Circulation Research Vol 71, No 3 September 1992
-J
4
:E<
_i
0
n-
o*o
0M
I-4i
:k
00
0
124
st E-:.
wz
_iZ
L
33...
5min
5mm
FIGURE 4. Recordings showing mitochondrial and cytosolic [Ca 2+] in cells pretreated with thapsigargin. Left panel:
Simultaneous recording of mitochondrial [Ca 2+ (top tracing) and cell length (bottom tracing) from a typical cell. Small arrow
indicates onset of anoxia; large arrow indicates point of reoxygenation. These cells hypercontracted at reoxygenation. Right panel:
Cytosolic [Ca 2+] (top tracing) and cell length (bottom tracing).
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
[Ca2+], is displayed in panels C and D. The tracings in
panels B and D are from cells that were pretreated with
thapsigargin. Inhibition of the sarcoplasmic reticulum
Ca2'-ATPase resulted in an immediate increase in
[Ca2.]m with reoxygenation (to an average of 542±68
nM at 1 minute after reoxygenation). The rapid fall in
[Ca 2+]1 typically observed at reoxygenation was attenuated or blocked with the sarcoplasmic reticulum disabled. In addition, in these same cells, no spontaneous
cytosolic Ca 2+ oscillations or electrically stimulated
Ca2' transients were seen in the immediate postreoxygenation period. Rather than falling rapidly to baseline
levels immediately after reoxygenation, [Ca 2+], remained at 399±42 nM at 1 minute after reoxygenation
in cells treated with thapsigargin. Figure 6 demonstrates
the relation between the [Ca 2+] just before reoxygenation and the instantaneous rate of change in [Ca 2+] in
both the cytosolic and mitochondrial compartments at
the moment of reoxygenation for all cells studied. The
A.
rate of fall of [Ca2+], at reoxygenation markedly exceeds
that of [Ca2`]m (p<0.0001), and both of these are
reduced in the presence of thapsigargin (p<0.0001).
Discussion
In our present study, we demonstrate that during
anoxia free calcium levels rise in both the cytosolic and
mitochondrial compartments only after the onset of
energy-depletion rigor contracture. The levels of calcium achieved during anoxia, in both the cytosolic and
mitochondrial compartments, predict cell outcome at
reoxygenation. With the readmission of oxygen, [Ca2+],
falls rapidly to control levels even in cells that hypercontract, but [Ca2+]m declines more slowly, such that
control levels are only reached 15-20 minutes after
reoxygenation. Mitochondrial free calcium levels remain predictive of cell outcome early during reoxygenation. We have also shown that reversible rises in
B.
1.v
v
_J
z
C)
00-9
o.o
C.
D.
L)
0
v
0on-
0-.CZ3
>U
0)
o.o0J
o.o J
FIGURE 5. Recordings of mitochondrial [Ca 2+] (panels A and B) and cytosolic [Ca 2+] (panels C and D) in cells at
reoxygenation showing the effects of thapsigargin. Changes that occur in [Ca 2+] at reoxygenation (arrowhead) in four individual
cells are shown on an expanded time base. The cells in panels B and D were pretreated with thapsigargin; the cells in panels A
and C were not pretreated. The time bar indicates 10 seconds.
Miyata et al Mitochondrial [Ca2"] in Anoxic Myocytes
100
vj
0
0
l
a)
Ud)
-100
az
_.
(L)
-200
:i
-300
v
-400
0
200
400
600
[Ca"]
800
1000
1200
(nM)
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
FIGURE 6. Plot showing relation of instantaneous rate of
[Ca 2+] change at reoxygenation to peak anoxic [Ca 2+] level
for cells. Triangles represent cytosolic values; circles represent
mitochondrial values. Open symbols are from data obtained
in the absence of thapsigargin; closed symbols are from data
obtained in the presence of thapsigargin.
[Ca2+Im
may occur
during
oxygen
deprivation and do
not necessarily lead to irreversible cellular injury.
Mitochondria possess well-described influx and efflux
pathways for Ca2+.25 The major route for Ca2' entry in
heart mitochondria is via a Ca21 uniporter. This transport process uses the mitochondrion's electrochemical
proton gradient to facilitate diffusion of Ca'+ into the
matrix. The primary driving force for Ca2' entry is the
mitochondrial membrane potential, which is ordinarily
maintained electronegative to the cytosol by as much as
180 mV in fully energized cells. The major efflux pathway for Ca2 is Na+ dependent. Finally, there exists a
latent transport process,25 referred to as the "mitochondrial transition" and now thought to represent a large
channel or pore, that can suddenly render the mitochondrial membrane permeable to a number of ions
including Ca2+. The mechanisms underlying the rise in
[Ca2+1m seen during and often after anoxia are not
established. Proton-motive force approaches zero in
mitochondria that are fully deenergized, as would occur
during anoxia after the onset of ATP-depletion rigor
contracture. However, a membrane potential may still
be generated under these conditions. Investigators have
demonstrated that nonrespiring mitochondria maintain
a potential of -30 mV26 relative to their exterior. This
results, in large part, from negative charges on impermeant macromolecules in the mitochondrial matrix.
This passive Donnan equilibrium potential can support
the existence of a mitochondrial:cytosolic Ca21 gradient
without expenditure of energy. This potential could
provide the driving force for continued Ca2' entry via
the uniporter during anoxia as [Ca2]c rises. The mitochondrial Ca2' efflux pathway may also be inhibited
during anoxia. [Mg2+]i is known to rise during myocardial ischemia27 and hypoxia28 and would be expected to
inhibit the Na+-dependent Ca2' efflux pathway.25 Finally, it is possible that the mitochondrial transition
occurs during anoxia and allows Ca21 from the cell
cytosol to readily enter the matrix. At reoxygenation,
when mitochondrial respiration recovers, the electrochemical proton gradient would rapidly be restored,
favoring enhanced Ca2' entry via the uniporter.
611
Several studies have demonstrated that ruthenium
red, an inhibitor of the mitochondrial Ca2` uniporter,
reduces ischemic and hypoxic injury in the heart.29,30 It
also improves posthypoxic recovery of intracellular
ATP.30 In isolated cardiac myocytes exposed to hypoxia
and reoxygenation, it reduces the reoxygenation-induced increase in total cellular Ca2+.31 Despite the fact
that ruthenium red is a rather nonspecific inhibitor of
mitochondrial Ca2+ transport that has significant effects
on sarcoplasmic reticulum Ca2+ release, it may be that it
exerts its protective effects on the heart by reducing
mitochondrial Ca2+ loading and subsequent injury during and after hypoxia. If this is the case, it is conceivable
that, in the absence of ruthenium red, the uniporter
continues to load mitochondria with Ca2' both during
and after hypoxia.
Based on our results, it is possible to establish a
tentative sequence of calcium movements occurring in
the single-myocyte anoxia/reoxygenation model. Before
the onset of ATP-depletion contracture, neither cytosolic nor mitochondrial free calcium concentrations rise.
During the rigor period, both [Ca2+] and [Ca2+]m rise
steadily. Because of the very large buffering capacity of
the mitochondrial matrix for calcium," the bulk of the
total cell calcium increase may be in the mitochondria.
The source of this calcium could, in principle, be either
external to the cell or from calcium stored in the
sarcoplasmic reticulum. The studies with thapsigargin
demonstrate that the rise in [Ca2+]c and [Ca2+Im occurs
even when the sarcoplasmic reticulum is depleted of
Ca2+ before anoxia. Studies conducted with caffeine2
have shown similar results. In contrast, the rise in
[Ca2+]c is markedly blunted when external sodium is
fully replaced by choline.32 Therefore, it seems most
reasonable to assume that calcium enters the cell primarily via Na+ /Ca 2+ exchange, probably in exchange for
sodium, which accumulates in the cytosol during rigor
by an unknown mechanism.33-36
At the time of reoxygenation, [Ca 2+] falls within a
minute to levels that are not significantly different from
the control diastolic level, both in cells that recover and
in those that hypercontract. This initial fall is probably
due to uptake of calcium by the sarcoplasmic reticulum,
since it was nearly abolished in our experiments by
thapsigargin, an agent that inhibits the sarcoplasmic
reticulum calcium pump,21 and in other studies in which
caffeine was used to release sarcoplasmic reticulum
calcium.2 In the absence of thapsigargin, [Ca2+]m also
falls at this time but more slowly than [Ca 2+]c.
The qualitative sequence of reversible calcium
changes in both the cytosol and mitochondria is the
same in cells that hypercontract as in cells that recover;
however, the absolute magnitude of the calcium rise is
strongly predictive of recovery. The absolute level of the
threshold for hypercontracture (250 nM) is lower than
that found in previous studies using aequorin (2-3
gM)2 or fura-2 (1 ,uM).5 Li et a13 reported a threshold of
500 nM for hypercontracture of cells on washout of
carboxyl cyanide m-chlorophenyl-hydrazone and
amytal. The differences in threshold values may be due
to species differences or to the fact that these studies
were performed at 37°C rather than 23°C as we have
done. The reason for the correlation of [Ca 2+] and
[Ca2']m with cellular recovery is unclear. Unlike the
situation in intact tissue, hypercontracted isolated myo-
612
Circulation Research Vol 71, No 3 September 1992
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
cytes do not initially lose membrane integrity,37 and the
increase of free calcium in both compartments was at
least partially reversible. Cellular hypercontracture was
not due to a sudden and massive rise in [Ca"2], immediately after reoxygenation. The leading explanations
for hypercontracture are either that excessive myofilament activation occurred immediately at reoxygenation
as soon as some ATP was available to the myofilaments
even though [Ca2"]c soon fell or that the increase of
[Ca2+]m impaired the ability of the mitochondria to
resynthesize ATP. In relation to the first possibility, low
levels of ATP (micromolar) are known to sensitize the
myofilaments to activation by Ca2+38 and may even
induce Ca2'-independent crossbridge cycling.39 Thus,
the rise in [Ca2+]m seen during anoxia may merely reflect
more important changes in [Ca"2] occurring in the
cytosol. [Ca2.]m probably follows [Ca2"]c once ATPdepletion contracture has occurred. At reoxygenation,
the recovery of [Ca2']m occurs more slowly than the
recovery of [Ca2]c, reflecting the relatively slow kinetics of the mitochondrial Ca2+ efflux pathways that we
have demonstrated previously.15 In relation to the latter
hypothesis, mitochondrial ATP generation is severely
limited when there is a marked rise in intramitochondrial matrix calcium.10 Impaired intracellular ATP restoration could certainly lead to irreversible cell injury,
as has been suggested by prior studies.37,39,40 A problem
with this hypothesis is that the threshold value of
[Ca2']m associated with hypercontracture (250 nM) is
less than the level that produces half-maximal activation
of pyruvate dehydrogenase in isolated, normally respiring mitochondria.14 Although these levels of free calcium would not be expected to be damaging to normally
respiring mitochondria, it is possible that prolonged
exposure to this calcium level during ATP depletion
might be injurious to the mitochondria. In fact, Murphy
et a141 found that cellular damage (indexed by lactate
dehydrogenase release) was greater in chick heart cells
depleted of ATP by metabolic inhibitors than it was in
cells intoxicated with ouabain, despite a smaller [Ca 2+]i,
increase in the ATP-depleted cells. This may reflect an
increased sensitivity of the cardiac myocyte to the
damaging effects of excess Ca2+ when mitochondrial
function is impaired. More recently, the concept that
nonischemic cells (as opposed to ATP-depleted cells)
defend themselves remarkably well against elevated
levels of [Ca 2ji has been reinforced.42
Although the present study defines the changes in
mitochondrial free calcium that occur during and after
anoxia, it is limited in certain regards. First, despite the
fact that these are the first measurements of [Ca 2+]m in
living cells, [Ca 2+]m cannot be monitored simultaneously
with [Ca 2+]c in the same cell. We have performed
parallel experiments in cells in which [Ca 2+]c is monitored. The morphological and functional changes in
these two groups were similar, permitting comparison of
the two groups. The present experiments were conducted at 23°C rather than 37°C to minimize loss of
fluorescent probes during long protocols. Even at 23°C,
calcium levels were no longer quantifiable at 20-30
minutes after reoxygenation in cells that hypercontracted. [Ca 2+]m was monitored in a few cells studied at
37°C. The results were qualitatively similar to those
obtained at room temperature, although several cells
that were irreversibly injured at reoxygenation showed
rises in [Ca2+]m as high as 1 AM. Finally, [Ca21]m could
only be measured after exposure of the cell to Mn2+.
One concern is that Mn2' would affect the contractile
properties of the cell. We previously demonstrated that
this was not the case.15 It is well known that Mn21 can
competitively inhibit the uptake of Ca2' by the mitochondrial Ca2' uniporter25 and can inhibit the Na+dependent mitochondrial Ca>2 efflux pathway as well.
In our prior studies, we demonstrated that 10-20 ,M
Mn2 had very little effect on Ca>2 transport by isolated
mitochondria15 when they were studied in the presence
of physiological concentrations of magnesium and spermine. It is extremely unlikely that free Mn>2 concentration reaches 20 ,M in the cytosol of cells in these
studies, since it takes roughly 30 minutes of Mn>2
superfusion to titrate the indo-1 in the cytosol, estimated at 30 AM, and indo-1 binds Mn>2 more tightly
than Ca>2 (Kd for the Mn2+-indo-1 chelate, :10 nM).15
Further evidence that Mn2+ concentrations in the cell
likely remain below a level that would have major effects
on mitochondrial Ca>2 regulation is offered in a prior
publication.15
Although mitochondrial calcium loading is strongly
predictive of "irreversible" hypercontracture, our results make it clear that it is not itself an irreversible
marker of loss of sarcolemmal membrane integrity and
ion homeostasis. The mechanism underlying the association of mitochondrial calcium with cellular hypercontracture requires further investigation.
References
1. Shen AC, Jennings RB: Myocardial calcium and magnesium in
acute ischemic injury. Am J Pathol 1972;67:417-421
2. Allshire A, Piper HM, Cuthbertson KSR, Cobbold PH: Cytosolic
free Ca 2+ in single rat heart cells during anoxia and reoxygenation.
Biochem J 1988;244:381-385
3. Li QA, Altschuld RA, Stokes BT: Myocyte deenergization and
intracellular free calcium dynamics. Am J Physiol 1988;255:
C162-C168
4. Murphy JG, Marsh JD, Smith TW: The role of calcium in ischemic
myocardial injury. Circulation 1987;75(suppl V):V-15-V-24
5. Quaife RA, Kohmoto 0, Barry WH: Mechanisms of reoxygenation
injury in cultured ventricular myocytes. Circulation 1991;83:
566-577
6. Hano 0, Silverman HS, Blank PS, Mellits ED, Baumgardner R,
Lakatta EG, Stern MD: Nicardipine prevents calcium loading and
"oxygen paradox" in anoxic single rat myocytes by a mechanism
independent of calcium channel blockade. Circ Res 1991;69:
1500-1505
7. Denton RM, McCormack JG: Ca 2+ transport by mammalian mitochondria and its role in hormone action. Am J Physiol 1985;249:
E543-E554
8. McCormack JG, Halestrap AP, Denton RM: Role of calcium ions
in regulation of mammalian intramitochondrial metabolism. Physiol Rev 1990;70:391-425
9. Hansford RG: Relation between mitochondrial calcium transport
and control of energy metabolism. Rev Physiol Biochem Pharmacol
1985; 102:1-72
10. Lehninger AL: Mitochondria and calcium ion transport. Biochem J
1970;1 19:129-138
11. Carafoli E: The homeostasis of calcium in heart cells. J Mol Cell
Cardiol 1985;17:203-212
12. Borgers M, Piper HM: Calcium shifts in anoxic cardiac myocytes:
A cytochemical study. J Mol Cell Cardiol 1986;18:439-448
13. Wendt-Gallitelli MF, Isenberg G: Total and free myoplasmic calcium during a contraction cycle: X-ray microanalysis in guinea-pig
ventricular myocytes. J Physiol (Lond) 1991;435:349-372
14. Hansford RG: Dehydrogenase activation by Ca2+ in cells and
tissues. J Bioenerg Biomembr 1991;23:823-854
15. Miyata H, Silverman HS, Sollott SJ, Lakatta EG, Stern MD, Hansford RG: Measurement of mitochondrial free Ca 2+ concentration
Miyata et al Mitochondrial
16.
17.
18.
19.
20.
21.
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
22.
23.
24.
25.
26.
27.
in living single rat cardiac myocytes. Am J Physiol 1991;261:
H1123-H1134
Silver LH, Hemwall EL, Marino TA, Houser SR: Isolation and
morphology of calcium-tolerant feline ventricular myocytes. Am J
Physiol 1983;245:H891-H896
Stern MD, Silverman HS, Houser SG, Josephson RA, Capogrossi
MC, Nichols CG, Lederer WJ, Lakatta EG: Anoxic contractile
failure in rat heart myocytes is caused by failure of intracellular
calcium release due to alteration of the action potential. Proc Natl
Acad Sci U SA 1988;85:6954-6958
Spurgeon HA, Stern MD, Baartz G, Raffaeli S, Hansford RG, Talo
A, Lakatta EG, Capogrossi MC: Simultaneous measurements of
the cytosolic Ca2+ transient, contraction and membrane potential
or current in single adult cardiac myocytes. Am J Physiol 1990;27:
H574-H586
Sollott SJ, Ziman BD, Lakatta EG: A novel technique to load
indo-1 "free acid" into single adult cardiac myocytes, to assess
cytosolic calcium. Am J Physiol (in press)
Lattanzio FA: The effects of pH and temperature on fluorescent
calcium indicators as determined with chelex-100 and EDTA
buffer systems. Biochem Biophys Res Commun 1990;171:102-108
Lytton J, Westlin M, Hanley MR: Thapsigargin inhibits the sarcoplasmic or endoplasmic reticulum Ca-ATPase family of calcium
pumps. J Biol Chem 1991;266:17067-17071
Stern MD, Chien AS, Capogrossi MC, Pelto DG, Lakatta EG:
Direct observation of the "oxygen paradox" in individual rat ventricular myocytes. Circ Res 1985;56:889-903
Haworth RA, Nicolaus A, Goknur AB, Berkoff HA: Synchronous
depletion of ATP in isolated adult rat heart cells. JMol Cell Cardiol
1988;20:837-846
Silverman HS, Ninomiya M, Blank PS, Hano 0, Miyata H, Spurgeon HA, Lakatta EG, Stern MD: A cellular mechanism for
impaired posthypoxic relaxation in isolated cardiac myocytes:
Altered myofilament relaxation kinetics at reoxygenation. Circ Res
1991;69:196-208
Gunter TE, Pfeiffer DR: Mechanisms by which mitochondria
transport calcium. Am J Physiol 1990;258:C755-C786
Jung DW, Davis MH, Brierley GP: Estimation of the pH gradient
and Donnan potential in de-energized heart mitochondria. Arch
Biochem Biophys 1988;263:19-28
Kirkels JH, van Echteld CJA, Ruigrok TJC: Intracellular magnesium during myocardial ischemia and reperfusion: Possible consequences for postischemic recovery. J Mol Cell Cardiol 1989;21:
1209-1218
[Ca2"]
in Anoxic Myocytes
613
28. Headrick JP, Willis RJ: Cytosolic free magnesium in stimulated,
hypoxic, and underperfused rat heart. J Mol Cell Cardiol 1991;23:
991-999
29. Ferrari R, Di Lisa F, Raddino R, Visioli 0: The effects of ruthenium red on mitochondrial function during post-ischaemic reperfusion. J. Mol Cell Cardiol 1982;14:737-740
30. Park Y, Bowles DK, Kehrer JP: Protection against hypoxic injury
in isolated-perfused rat heart by ruthenium red. J Pharmacol Exp
Ther 1990;253:628-635
31. Stone D, Darley-Usmar V, Smith DR, O'Leary V: Hypoxiareoxygenation induced increase in cellular Ca 2+ in myocytes and
perfused hearts: The role of the mitochondria. J Mol Cell Cardiol
1989;21:963-973
32. Haigney MCP, Miyata H, Lakatta EG, Stern MD, Silverman HS:
Sodium-linked Ca 2+ overload and cell death in reoxygenated rat
cardiac myocytes. (abstract) Circulation 1991;84(suppl II):II-664
33. Guarneiri T: Intracellular sodium-calcium dissociation in early
contractile failure in hypoxic ferret papillary muscles. J Physiol
(Lond) 1987;388:449-465
34. MacLeod KT: Effects of hypoxia and metabolic inhibition on the
intracellular sodium activity of mammalian ventricular muscle.
J Physiol (Lond) 1989;416:455-468
35. van Ecteld CJA, Kirkels JH, Eijgelshoven MHJ, van der Meer P,
Ruigrok TJC: Intracellular sodium during ischemia and calciumfree perfusion: A 23Na NMR study. J Mol Cell Cardiol 1991;23:
297-307
36. Haigney MCP, Miyata H, Lakatta EG, Stern MD, Silverman HS:
Intracellular [Na+] changes in rat cardiac myocytes exposed to
hypoxia and reoxygenation. J Mol Cell Cardiol 1991;23:S.83
37. Hohl C, Ansel A, Altschuld RA, Brierley GP: Contracture of
isolated rat heart cells on anaerobic to aerobic transition. Am J
Physiol 1982;242:H1022-H1030
38. Bremel RD, Weber A: Cooperation within actin filament in vertebrate skeletal muscle. Nature 1972;238:97-101
39. Nichols CG, Lederer WJ: The role of ATP in energy deprivation
contractures in unloaded rat ventricular myocytes. Can J Physiol
Pharmacol 1990;68:183-194
40. Altschuld RA, Wenger WC, Brierley GP: Ionic movements and
irreversible anoxic damage. Basic Res Cardiol 1985;80:151-154
41. Murphy E, Jacob R, Lieberman M: Cytosolic free calcium in chick
heart cells, its role in cell injury. J Mol Cell Cardiol 1985;17:221-231
42. Marsh JD, Smith TS: Calcium overload and ischemic myocardial
injury. Circulation 1991;83:709-711
Relation of mitochondrial and cytosolic free calcium to cardiac myocyte recovery after
exposure to anoxia.
H Miyata, E G Lakatta, M D Stern and H S Silverman
Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017
Circ Res. 1992;71:605-613
doi: 10.1161/01.RES.71.3.605
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1992 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/71/3/605
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/