Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
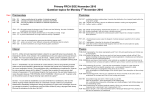
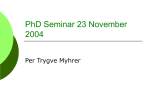
(CANCER RESEARCH 36, 132-137,January1976) Critical Evaluation of Lymphocyte Functions in Urological Cancer Patients1 Mostafa M. Elhllali,2 Sven BillIon, Stanley Brosman, and John L. Fahey Departments of Surgery/Urology, Microbiology, and Immunology, University of California, Los Angeles 90024 (M.M.E., Sv.B., St.B., J.L.F.J and Department of Surgery/Urology,HarborGeneralHospital, Torrance,California90609[St.B.J SUMMARY One hundred three patients with varying stages of urobogical cancer (bladder, prostate, kidney) were investigated with regard to the following lymphocyte functions. T-cells were assessed numerically (E rosettes), their blastogenic response to phytohemagglutinin (PHA) was determined, and their cytotoxic potential against heterobogous target cells in short-term presence of PHA (i.e., PHA-dependent cellular cytotoxicity) was evaluated. Similarly, B cells were numerically assessed (EA rosettes), and their function was evaluated by antibody-dependent cellular cytotoxicity against antibody-coated heterobogous target cells. The data on cancer patients, divided on the basis of extent of disease and prior radiation therapy, were compared to those of normal young and age-matched controls. Our investigations emphasize the importance of the fol lowing factors: (a) comparison of data with age-matched controls, since several lymphocyte functions appear to change with age; (b) use of multiple controls to compensate for the inherent variability found in certain tests; (c) mini mized contamination by nonlymphoid cells in the purified cell preparation; and (d) the influence of certain treatment regimens (radiation, chemotherapy, etc.) on the results. Radiotherapy significantly depressed T-cell number with a depression of PHA blastogenic responses as well as PHA dependent cellular cytotoxicity. When all of these conditions were taken into account, the urobogical cancer patients as a group were found to have a lower proportional value of E rosettes (T-cells) and a re duced PHA blastogenic responsiveness. Certain cancer pa tients displayed an elevated PHA-dependent cellular cyto toxicity as compared to age-matched controls, which may indicate the presence of activated cells in the presence of tumors. With this identification of a group of cancer pa tients with markedly depressed E rosette values and PHA responsiveness, it will now be possible to follow them clini cally in comparison with a group of cancer patients with normal T-ceII functions. INTRODUCTION Immunocompetence persensitivity I These as reflected by normal delayed hy skin test reactions investigations were supported tends to correlate by National Bladder Cancer with the Project Grant CA 16880. a To whom requests for reprints should be addressed, at Department Urology, Sherbrooke University, Sherbrooke, Quebec, Canada. Received June 18, 1975; accepted 132 October 2, 1975. of stage, clinical course, and prognosis of cancer (4, 6). Skin tests of this type, however, involve immunological and in flammatory components. Assessment of individual compo nents of the immune response in relation to tumor burden and modes of therapy is needed. Also, such information is needed to assess changes in the immune system of bladder cancer patients receiving nonspecific adjuvant immunother apy. No comparable study using the battery of investiga tions reported in this work in patients with cancer of the genitourinary tract has been reported. A broad assessment of lymphocyte functions, measured by in vitro assays, was undertaken as a part of immunologi cal and immunotherapy investigations in bladder cancer. The influence of tumor burden and radiation therapy was compared by dividing the patients into appropriate groups. Also, salient pitfalls encountered in this type of investiga tion are noted. MATERIAL AND METHODS Peripheral venous blood samples (50 ml heparinized blood) were obtained from 3 different populations. These included 41 young controls (113 specimens), 47 age matched controls (52 specimens), and 103 patients with documented cancer of the bladder, kidney, or prostate (139 specimens) (Table 1). The mean age of the young controls was 26.7 years, that of the age matched controls was 58.7, and that of the cancer patients was 65.3 years. The distribu tion of the specimens obtained from the 3 cancer groups included 77 specimens obtained from 56 bladder cancer patients, 45 specimens from 32 prostatic cancer patients, and 17 specimens from 15 renal carcinoma patients. Blood Separation. The blood samples were kept at room temperature and were separated as soon as possible by the Ficoll-Hypaque technique described by Boyum (2). Analysis of Surface Markers. Separated lymphocytes were analyzed for T- and B-cell markers by 2 rosetting assays. The ability of peripheral resting T-cells to produce rosettes (E rosettes) with sheep ABC was used as a marker for T-cells. The non-T-celbs were assessed by their ability to rosette with sheep ABC coated with a 1/200 dilution of rabbit anti-sheep immunoglobubin (EA rosettes). The tech nique described by Jondab et al. (11) was followed for both the E and EA rosette assays. The lymphocytes and sheep ABC suspension were incubated as a pellet overnight at 4°. The E rosettes were then suspended very gently, whereas the EA suspension was Vigorously agitated in a Van-whirl mixer before being counted. CANCERRESEARCHVOL. 36 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research. Lymphocyte Functions in Uro!ogica! Cancer Patients Table 1 % released by IRS (on PHA) Number and age distribution of urological cancer patients Age (yr)Na. mensYoung of subjectsNo. % specific lysis = of speci — % released in NRS (or MEM) NRS (or MEM) % released by Triton — % released in The percentage released by Triton represents the total lysable counts (80% average). The IRS was obtained by giving a rabbit a weekly i.v. injection of 10@D6 mouse tumor cells for 3 weeks. Three days after the last injection the animal was bled, and this serum was used at a 1/5@ dilution which had maximal cytotoxic activity with normal lympho cancers65.3 ±11.0103139a cytes in the ADCC assay. Both the IRS and NRS were heat inactivated at 56° for 60 mm. In the absence of effector cells, Mean ±S.D.. neither of the sera caused any increased lysis of the target PHA3-proliferative Assay. Purified lymphocyteswere cub cells over that obtained with cells cultivated in MEM alone tured in microplates (microtest-2 Falcon) (Van Water and (<10%). PHA was diluted in MEM and added at a 1/@@ Rogers, Los Angeles, Calif.) at a concentration of 10@ dilution (10 /Lg) in 0.1 ml. cells/mb in MEM plus 10% AB serum. Three concentrations Statistical Analysis. Student's t test was used in the of PHA (Burroughs Wellcome and Co. , Research Triangle analysis of all test results. One-sided x2analysis was used to Park, N. C.) were added at the start of the culture (0.5, 1, evaluate the frequency of certain observations. The results and 5 pg). Two days later 2 @Ci [3H]thymidine (New England were considered significant when p < 0.01. Nuclear, Boston, Mass.) in 30 pi were added, and the cells were incubated for a further 18 hr. The cells were harvested RESULTS on Whatman Grade 934 AH glass filters (Reeve Angel, Clif ton, N. J.) in a manifold collector (MASH), and uptake of the The results obtained in the cancer patient population [3H]thymidine was determined in a f3 counter after the filters were evaluated and will be presented as a function of the were washed 5 times in distilled water. PHA proliferation tumor load present at the time of testing. The patients were index was calculated according to the formula: controls26.7 ±4.1@41113Age-matched contrals58.7 ±10.14752Localizedwithcancer62.9 ±12.92732Localized without evi ±10.94153dent 67.9 cancerMetastatic ±9.53554Allcancer64.4 separated into2 groups relatedto the stage of the disease, i.e., localized to the organ of origin, or metastatic. The PHA index = cpm in presence of PHA cpm in absence of PHA Cytotoxic Assays. A gross virus-induced mouse lym phoma (D6) of thymic origin from C3H mice (courtesy of Dr. H. Weben, Department of Microbiology and Immunology, UCLA) was used as a target serum. Immediately before testing,the D6 cellswere Ia beled with 51Crfollowing the technique of Wigzell (17). We used 0.4 p.Ci sodium chnomate (l.C.N. Corporation, Irvine, Calif.), which was added to 10@tumor cells in 1 ml MEM supplemented with 10% fetal calf serum. After incubation at 37°for 90 mm the labeled cells were washed 4 times and were added to the effecton lymphocytes at the ratio of 1:20 (target:effector). The tumor cell number was always kept constant at 10@ cells/tube yielding3000 to 5000 cpm. PHA, IRS prepared against the target cells, NAS was then added at a volume of 0.1 ml. The mixture was centrifuged at 185 x g for 5 mm at room temperature and the pellet was incu bated for 2 to 3 hr at 37°.The reaction was stopped by the addition of 1 ml cold MEM, and the mixture was centrifuged in the cold for 8 mm at 185 x g. The supemnatant was decanted for determination of radioactivity in a y counter (Nuclear Chicago, Chicago, Ill.). Percentage of specific lysis was calculated according to the formula: abbreviations used are: PHA, phytohemagglutinin; MEM, minimal essential medium; IRS, immune rabbit serum; NRS, normal rabbit serum; ADCC, antibody-dependent cellular cytotaxicity; PDCC, PHA-dependent cal lular cytotoxicity; PMN, polymarphonuclear leukocyte; DNCB, 2,4-dinitro chlorobenzene. JANUARY 1976 Lymphocyte Subpopulation cell in these assays. It was grown in suspension in Tissue Culture Medium MJLA (Re heis, Los Angeles, Calif.) supplemented with 10% fetal calf 3 The group with localized cancer was divided into 2 categories, namely, with or without clinically evident cancer at the time of testing, i.e., pre- and postoperatively. T-dependent Lymphocytes (E Rosettes). The sponta neous sheep RBC-rosetting test was used to obtain the percentage of T-dependent lymphocytes in separated blood (Table 2). There was no significant difference between the percentage of E rosettes in the young controls (68.39) and that in the age-matched controls (67.20). On the other hand, the difference between the age-matched controls and the mean score of patients with localized cancer (62.98), meta static cancer (58.24), or all combined (61.37) was statisti cabbysignificant. Non-T-dependent Lymphocytes (Fc Rosettes). Using an tibody-coated sheep ABC in the rosette assays, the percent age of non-T-dependent lymphocytes in separated blood was obtained (Table 2). There was no significant difference between the percentage of EA rosettes in the young con trols (19.45) and that in age-matched controls (19.34). However, the difference between the age-matched controls and the mean score of patients with localized cancer (22.92), metastatic cancer (25.01), or both combined (23.36) was significant. PHA Proliferative Assay The blastogenic response to PHA in the 3 populations is presented in Table 2 as PHA index. The PHA index of cancer 133 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research. M. M. E!hi!ali et a!. Table2 Comparisonof in vitro lymphocytestudies between controls and cancer patients lysis)Young E rosettes (%)Fc controls68.39 (32)Age-matched controls67.20 (38)Localized with cancer64.20 (9)Localized withoutevident cancer62.98 ±0.92a (100)C19.45 ±1.40 (49)19.34 ±2.02 (31)21.12 ±1•77b ±0.64 (100)275.83 ±0.74 (49)151 ±1.58 (31)159.68 ±1 00b (53)22.92 (53)67.65 (19)Metastatic cancer58.24 ±1,83b (54)25.01 (22)All cancers61.37 ±1,1ob (138)23.36 a Mean b p < C Numbers (% (% lysis)PDCC ±1.14 ±2,79 (32)6.39 ±2.49 (38)7.00 ±2.94 (9)11.46 ±42.82 (50)24.91 .82 ±27.59 (41)32.88 ±57.01 (15)27.83 ±1612b ±1.01 ±2.71 ±1.91 ±3.43 (19)7.97 (19)34.13 ±1 29D (54)86.30 ±0,74b (138)99.63 ±1.03 .89 ±2.42 ±22.95 (22)31 (22)3.78 ±18@83b ±1.76 (56)31.94 (50)6.75 ±1.04 (50) ± S.E. 0.01 when in compared parentheses, to results obtained in age-matched controls by Student's t test. n. patients as a group (99.63) was significantly depressed corn pared to that of young controls (275.83) and age-matched controls (151.82). The difference between the group of local ized cancer patients without evident disease and the age matched controls is significant. Because the PHA index does not take into consideration the daily experimental Variation, the PHA index of the test @ indexADCC rosettes (%)PHA 60 50 x 40 (I) z w @1\@ x@x Cancer Pct,ents( @——-—. Controls(n@83) subject was divided by the average of the PHA index of the (.) controls studied the same day. We calculated the percent age of specimens that gave a PHA index less than 50% of the control value for that day for each group. In the localized cancer group with evident disease, the percentage of pa tientS having less than 50% PHA index was 60%; whereas in the group without evident cancer, this was 63%. In meta static cancer this was 72% and in the overall cancer group it was 63%. The PHA index was obtained on 3 or more occasions in 8 young controls. In 3 subjects the multiple determinations were quite similar. In 2 subjects the difference between any 2 determinations was less than 1 S.D. , while in the other 3 ‘I, (youngandage-matched). Thefrequency(%)in eachpopulationis plotted againstthePHAindex.A biphasiccurveis notedforthecontrolpopulation. subjects the difference The incidence of high response was greatly reduced in cancer patients. was more pronounced .. These varia tions, we believe, are inherent in the test itself. The changes in results obtained on different days can be minimized by comparing the result of the test subject to 2 or more con trols tested under the same conditions on the same day. When the results of the PHA index were plotted in cancer patients and controls, the values for young controls were noted to cluster into 2 distinct groups, one being less than 150 and the other group being above 350. The young con trols tended to have a greater distribution in the high group, whereas the age-matched controls had more values on the bower side with few high values. In cancer patients this distribution was even more pronounced, with most of the values occurring on the lower side and only an occasional high responder. When the number of specimens in cancer patients and controls (percentage of the total) was plotted against the PHA index in increments of 50 (Chart 1), the difference in distribution was readily apparent. The PHA index results in all groups were arbitrarily di vided into 2 subgroups with a PHA index value more or less than 50. The 1st group (>50) was considered to be the high responders, and the 2nd group (<50) were the low respond 134 30 U. 0 ‘p 20 I0 x____.___@@,__. 0L50 ! _S,. @, 00-ISO ‘ 200-250 PHA Chart 1. PHA proliferative 300-350 >350 INDEX response in cancer patients and controls ers (Table 3). The differences between the number of sub jects in the low and high responder groups of the cancer, age-matched, and young control populations were highly significant (x2@ P < 0.005). The incidence of low response was higher in the cancer patients as compared to the con trois. When the PHA index/control data were analyzed, the index was less than 0.5 in 35 cancer patients (mean 0.14 ± 0.01), whereas this value was higher than 0.5 in 21 cancer patients (mean 1.79 ±0.31). Cytotoxiclty Results ADCC. As shown in Table 2, the difference between me suIts obtained with young controls (24.91) and those for age-matched controls (32.88) is significant. The differences between age-matched controls and cancer patients are not statistically significant. PDCC. No significant differences were found between the different cancer groups and the control groups (Table 2). CANCERRESEARCHVOL. 36 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research. Lymphocyte Functions in Urological Cancer Patients Influence of Blood Separation Purity on Results The incidence of PMN contamination of more than 15% in separated blood was compared in young controls, age matched controls, and cancer patients. In young controls the incidence of contamination was 1% as compared to 43% in age-matched controls and 40% in cancer patients. These differences are highly significant. The influence of this con tamination on the assay results in age-matched controls and cancer patients was studied. In age-matched controls no significant effect was demon strated on E or Fc rosettes or on PDCC. The PHA index with PMN less than 15% was 236.82 ±57.43 (mean ±S.E.) as compared to 137.01 ±26.91 when PMN was more than 15%. This difference was not statistically significant. The ADCC results were 29.12 ±3.41 with PMN less than 15% and 39.17 ±4 .06 with PMN more than 1 5% . This difference was statisti to nonradiotherapy group. There were no significant differ ences in the ADCC results. The PHA index results were analyzed in the nonradiated group after elimination of data from patients with a higher than 15% polymorphonuclear contamination. The group of patients with localized but evident cancer (170.95 ±71.64) and the group with metastatic cancer (144.71 ±60.00) were not significantly lower than the age-matched controls (236.82 ±57.43). The differences between the group of patients with localized but no evident cancer (51.37 ± 14.29) and the age-matched controls were significant. Simi larly, the PHA index results in the overall cancer group (120.17 ±31.85) were significantly different from those obtained in age-matched controls. Correlation of Laboratory Results and Delayed Hypersen sitivity cabbysignificant. In the group of cancer patients only the PDCC assay was significantly elevated when the PMN contamination was less than 15% (10.48 ±2.21) as compared to a higher than 15% contamination (4.25 ±0.95). Reactions The cancer patients studied were concomitantly skin tested as part of the investigative protocol. The results of 97 patients sensitized to DNCB were divided into positive and negative responders and were compared to the laboratory data. Radiotherapy Effect A group of patients who had received radiotherapy (39 patients) was divided into 3 subgroups. The 1st group had completed radiation within 3 months of testing, the 2nd group within 6 months to 1 year, and the 3rd group more than 1 year prior to testing. The radiation was confined to the pelvis in all but 2 patients, who received therapy to the spine or breasts. The dose of radiotherapy ranged between 1600 and 7000 rads. Most patients received Levels of E or Fc rosettes, ADCC, or PDCC were not found to correlate with the presence or absence of positive DNCB response. There was a significant reduction in the PHA index, however, in the DNCB nonresponders (34.70 ±9.28) as compared to the DNCB-positive group of patients (169.76 ± 43.86). A more complete account of other skin testing results and their correlation to laboratory tests and other variables will be published separately. 1600 rads, which was administered prior to cystectomy. There was a significant reduction in E rosettes in the group of patientswhose radiationwas completed more than 1 year prior to testing as compared to either the age matched controls or the group with no radiation (Table 4). In the same group, the Fc rosettes were significantly higher than in age-matched controls on the group without radia tion. The PHA index shows a tendency to decrease after the onset of radiation which is even more depressed at the 6month to 1-year period but recovers slightly 1 year after radiation. The results of PDCC showed a pattern similar to that of the PHA index, with significant reduction within 3 months and 6 months to 1 year postradiation as compared DISCUSSION The studies undertaken included a broad assessment of the lymphocyte functions in a population of patients with different stages of unobogical cancer. The influence of tu momload and the effect of radiation therapy were studied. The choice of tests has been partly empirical and partly influenced by our own experience with certain assays. The T- and B-cell surface markers are accepted as a means of numerical evaluation of peripheral T- and B-cells. The PHA proliferation assay has also been widely used as a measure of T-cell function. Although the cells were exposed to var ious doses of PHA, the data reported were obtained with the Table 3 Distribution of blastogenic response in high and low responders (56)Young (41)High controls responders>50<50>50<50>50<50PHA respondersLow index 315.79±47.06a (43)b. a Mean b Numbers @ r < r30.25 ContraIs (91)Cancer patients (50)Age-matchedcontrols respondersHigh ±4.95 ([email protected] respondersLow ±33.59 (28)C18.76 respondersHigh ±3.17 (13)―179.30 respondersLow ±29.50 (29)C14.50 ±2.34 (27)@ ± SE. in parentheses, by 1-sided n. x2 analysis for the frequency of law and high response in each group. JANUARY1976 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research. 135 M. M. Elhi!ali et a!. Table4 Effect of radiation therapy on various lymphocytestudies lysis)Age-matched E rosettes (%)Fc controls67.20 (38)No radiation63.10 (26)Radiation within 3 mo.63.66 (8)Radiation 6 mo.—1 yr .82 ±27.59 (41)7.00 ±29.63 ±1.55 (32)9.41 (74)21.04 (74)134.40 ±1.52 ±16.92 ±2.17 (11)2.00 (25)24.98 (25)60.47 ±26.21 ±2.55 ±2.89 (7) (14) (14) 52.37 ±2@62@@,d 29.79 ±1,72@@d71.78±48.82 (6)4.69 (24)38.71 (24)21.92 Radiation >1 yr62.14 a Mean < 0.01 d p < 0.01 ±0.74 (49)151 ±0.86 ±1 @4Q (49)b19.34 in parentheses, (% lysis)ADCC (% .63 ±2.69 ±1.01 (38)31 ±1.65 ±4.40 (26)30.45 ±2.92 ±2.38e (8)31.34 ±1.32'@ ±5.64 (9) (10) 5.04 ±0.73 32.88 ±2.49 (7) (6)32.20 n. when compared to when compared to results results obtained in obtained in age-matched “No radiation― lowest dose (1 i@g)found to give a consistent positive prolif eration index in normal controls. The 2 cytotoxic assays (ADCC and PDCC) were chosen because of previous work in this laboratory (1, 18). The ADCC measures a non-T-ceIb function (cytotoxicity) against antibody-coated target cells (16). The PDCC measures cyto toxic potential of lymphocytes in the presence of PHA. In the short-term assay as we use it , 2 hr), PHA is unlikely to induce a cytotoxic potential in ‘ virgin―lymphocytes as previously suggested (10). Instead, it is more likely to meas ure a cytotoxic potential of in vivo activated effector cells, probably of T-cell origin (B. Bonavida and A. Robins, per sonal communication). A significant reduction was found in the number of circu bating T-cells (E rosettes) in cancer patients as compared to the control groups. This was associated with a concomitant reduction in PHA proliferative response as compared to the control population. This depression of blastogenic re sponse cannot be totally explained by the decrease in the percentage of T-cebls. Such a conclusion is substantiated in the age-matched controls where there was a discrepancy between a normal T-celI number but a depressed PHA probif erative response compared to the young controls. This would lead us to assume that subclasses of E-rosetting T cells exist and that those capable of proliferative responsive ness to PHA are primarily affected in old age. The variability in PHA response in the same subject tested sequentially necessitates the use of multiple control speci mens for these assays. To learn more about the reproducibil ity of the PHA response, the data from the young control population were plotted against variables such as PMN contamination, percentage of lymphocytes, and age. The responses spread across a wide range. This wide range accounts for the large S.D. seen in this assay. The majority of the young controls were high responders. The older controls (58.7 ±10.1 years) had a greater percentage of low responders than did the young controls. In the cancer popu lation there was a wide distribution of responses, but the increase in the number of bow responders was significantly accentuated in the cancer group. The various assays were evaluated to determine whether they were affected by PMN contamination. The results were 136 indexPDCC ± S.E. b Numbers Cp rosettes (%)PHA group controls by Student's by Student's t test. t test. arbitrarily divided into 2 groups with more or less than 15% contamination. In the age-matched controls there is an indication that the PHA index may be depressed when the PMN count is high; however, too few patients were studied to provide statistical significance. The major difference in the control group was seen in the ADCC assay. The en hanced ADCC response may be explained by the participa tion of PMN in this reaction. In the cancer group the P0CC assay was the only test significantly affected. The lowered response seen with the PMN-contaminated specimens (more than 15%) could be explained by the presence of fewer available lymphocytes, which are required for this assay. In studies of this nature it is important to consider the influence of various therapeutic modalities. In the group of patients receiving radiotherapy, we detected a significant reduction in the percentage of E rosettes 1 year after com pletion of treatment. The PHA blastogenic response was found to be reduced to a greater extent in patients studied within 3 months of radiation therapy, although the percent age of E rosettes was not significantly reduced. Stratton et al. (15) studied the effects of radiation therapy delivered to the thymus on the numbers and functional capacities of certain subpopulations of circulating bympho cytes. They compared these results with pelvic radiation. Using rosette formation , membrane immunofluorescence, and blastogenic response to mitogens, they found that both T- and B-cells undergo rapid depletion during radiotherapy, whether or not the thymus is included in the treatment field. The T-cells disappeared more rapidly and their eventual drop is somewhat greater than that of B-cells. On the other hand, Stjernsward et a!. (14) felt that radiation of the thymus per se is the primary cause of the alterations in circulating lymphocyte populations. Stratton et a!. (15) also demon strated that the decrease in the ability to synthesize DNA in response to mitogen stimulation is much greater than the decrease in number of lymphocytes during radiotherapy, a finding in line with our observation. The recovery of this depression was biphasic, showing an improvement in 1 to 3 months followed by a depression in 4 to 6 months and partial recovery by 7 to 12 months. This correlates well with the trend we noticed in the progression of PHA inhibition in our results in a different patient population. CANCERRESEARCHVOL. 36 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research. Lymphocyte Chee et a!. (5) concluded that the reduction in PHA response following radiation was primarily due to the de creased numbers of a subpopulation of circulating lympho cytes normally responsive to PHA. The rapidly dividing bym phocytes are probably the cells most vulnerable to radia tion. When the results of the cytotoxic assays were analyzed, we noticed a normal number of cytotoxic effector cells against antibody-coated target cells in cancer patients. This finding is in contrast to what has been reported in patients with hematobogical tumors (9). We do not have an explana tion for this difference but the normal values for ADCC in cancer patients corresponded well with the higher than normal numbers of cells with Fc receptors (EA rosettes) which seem to represent the effector cells in this cytotoxic reaction (12). When the samples with more than 15% contami nation of PMN were eliminated, the cancer patients as a group displayed an increased cytotoxicity against heterobo gous target cells in the presence of PHA. This kind of cytotoxicity (PDCC) could be a function of activated cyto toxic cells in vivo that will express the cytotoxicity if brought in contact with target cells by means of PHA. The effector cells appearto be an activated thymus-denived cell (8). Such cells have been found in the spleen of sarcoma-beaning mice (16). An attractive possibility is that these effector cells have specificity for the tumor target cell in vivo, and we intend to compare the P0CC data in these patients with the results of tests for specific cytotoxicity against human blad dem cancer cells in Vitro. The presence of cell-mediated cytotoxicity associated with bladder and kidney cancer seems to correlate with the stage and course of the disease (3, 7, 13). The value of studying immunocompetency in cancer pa tients has been shown by correlations between the immune state and stage of cancer (4). Additional value may be gained by monitoring therapeutic modalities known to de press the immune system. The possible value of these tests in objectively assessing immunotherapy and designing opti mal treatment regimens is still to be determined. ACKNOWLEDGMENTS The authors wish to express their thanks to Laurie Buckley, Ulla Claeson, Candace Vescera, Pam Cohn, Wanda Hale, Neal Groch, Pablo Villanueva, Functions in Uro!ogical Cancer Patients and Joe Rosenblatt for their expert technical assistance. We are grateful to Dr. B. Bonavida for his assistance in the establishment of the PDCC assay. Dr. Virginia Clark, professor of biostatistics (UCLA, School of Public Health), assisted in the statistical analysis of the data. REFERENCES 1. Bonavida, B. Studies on the Induction and Expression of T Cell-mediated Immunity. IV. Non-specific Cytotoxicity of Sensitized Murine Lympho cytes by PHA and ConA. Transplantation, in press. 2. Boyum, A. Isolation of Leukocytes from Human Blood and Bone Marrow. Scand. J. Clin. Lab. Invest., 21(Suppl. 97): 9—109, 1968. 3. Bubenik, J., Perlmann, P., Helinstein, K. , and Moberger, G. Cellular and Humoral Immune Response to Human Urinary Bladder Carcinomas. In tern. J. Cancer, 5: 310—319, 1970. 4. Catal6na, W. J., Chretien, P. B., and Trahan, E. E. Abnormalities of Cell mediated Immunocompetence in Genitourinary Cancer. J. Urol., 111: 229—232,1974. 5. Chee, C. A., Ilbery, P. L. T., and Rickinson, A. B. Depression of Lympho cytes Replicating Ability in Radiotherapy Patients. Brit. J. Radiol., 47: 37—43,1974. 6. Eilber, F. A., and Morton, D. L. Impaired Immunologic Reactivity and Recurrence following Cancer Surgery. Cancer, 25: 362—367,1970. 7. ElhilaIi, M. M., and Nayak, S. K. Immunologic Evaluation of Human Bladder Cancer: In Vitro Studies. Cancer, 35: 419—431 , 1975. 8. Forman, J., and Moller, G. Generation of Cytotoxic Cells in the Mixed Lymphocyte Culture Reaction. I. Specificity ofthe Effector Cells. J. Exptl. Med., 138: 672—685, 1973. 9. Gale, R. P., Zighelboim, J., Ossorio, R. C., and Fahey, J. L. A Compari son of Human Lymphoid Cells in Antibody-dependent Cellular Cytotoxic ity (ADCC). Clin. Immunol. Immunopathol., 3: 377—384.1975. 10. HoIm, G., and Perlmann, P. The Cytotoxic Potential of Stimulated Human Lymphocytes. J. Exptl. Med., 125: 721—732, 1967. 11. Jondal, M., HoIm, G., and Wigzell, H. Surface Markers on Human B and T Cells. I. A Larger Population of Cells Forming Non-immune Rosettes with Sheep Red Blood Cells. J. Exptl. Med., 136: 207—215, 1972. 12. McLennan, I. C. Competition for Receptors on Cytotoxic Lymphocytes. Clin. Exptl. Immunol., 10: 275—283,1972. 13. O'Toole, C., Perlmann, P., Unsgaard, B., Moberger, G., and Edsmyr, F. Cellular Immunity to Human Urinary Bladder Carcinoma. I. Correlation to Clinical Stage and Radiotherapy. Intern. J. Cancer, 10: 77—91 , 1972. 14. Stjernsward, J., Jondal, M., Vanky, F., Wigzell, H., and Sealy, A. Lympho penia and Change in Distribution of Human B and T Lymphocytes in Peripheral Blood Induced by Irradiation for Mammary Carcinoma. Lan cat, 1: 1352—1356, 1972. 15. Stratton, J. A., Byfield, P. E., Byfield, J. E., Small, R. C., Benfield, J., and Pilch, Y. A Comparisan of the Acute Effects of Radiation Therapy, Includ ing or Excluding the Thymus, on the Lymphocyte Subpopulations of Cancer Patients. J. Clin. Invest. , in press. 16. Takiguchi, T., Adler, W. H., and Smith, R. T. Cellular Recognition In Vitro by Mouse Lymphocytes: Effects of Neonatal Thymectomy and Thymus Graft Restoration of Alloantigen and PHA Stimulation of Whole and Gradient-Separated Subpopulations of Spleen Cells. J. Exptl. Med., 133: 63—80.1971. 17. Wigzell, H. Quantitative Titrations of Mouse H-2 Antibodies Using sCr Labeled Target Cells. Transplantation. 3: 423—429,1965. 18. Zighelboim, J., Bonavida, B., and Fahey, J. L. Evidence for Several Cell PopulationsActive in Antibody Dependent CellularCytotoxicity. J. Immu nol., 111: 1737—1742, 1973. JANUARY1976 Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research. 137 Critical Evaluation of Lymphocyte Functions in Urological Cancer Patients Mostafa M. Elhilali, Sven Britton, Stanley Brosman, et al. Cancer Res 1976;36:132-137. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/36/1/132 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1976 American Association for Cancer Research.