Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
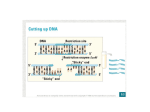
116 ANATOMIC PATHOLOGY Single Case Report 30. 31. 32. 33. carcinoid tumor and Crohn's disease. J Surg Oncol 1983; 24:310314. Janin Y, Schwartz D, Becker JM, Valderama E. Crohn's disease and carcinoid tumor of the appendix in a child. Z Kinderchir 1981;4:376-379. Kanter M, Lechago J. Multiple malignant rectal carcinoid tumors with immunocytochemical demonstration of multiple hormone substances. Cancer 1987;60:1782-1786. Maruyama M, Fukayama M, Koike M. A case of multiple carcinoid tumors of the rectum with extraglandular endocrine cell proliferation. Cancer 1988;61:131-136. Rode J, Dhillon AP, Papadaki L, et al. Neurosecretory cells of the lamina propria of the appendix and their possible relationship to carcinoid. Histopathology 1982;6:67-79. 34. Bloom SR, Polak JM. The hormonal pattern of intestinal absorption. In: Polak JM, Bloom SR, Wright NA, Daly MJ, eds. Basic Science in Gastroenterology, Structure of the Gut. London: Glaxo Group Research Ltd., 1982, pp 409-419. 35. Wilander E, Portela-Gomes G, Grimelius L, Westermark P. Argentaffin and argyrophil reactions of human gastrointestinal carcinoids. Gastroenterology 1977;73:733-736. 36. O'Briain DS, Dayal Y, DeLellis RA, et al. Rectal carcinoids as tumors of the hindgut endocrine cells: A morphological and immunohistochemical analysis. Am J Surg Pathol 1982;6:131-142. 37. Azumi N, Traweek ST, Battifora H. Prostatic acid phosphatase in carcinoid tumors: Immunohistochemical and immunoblot studies. Am J Surg Pathol 1991; 15:785-790. Positive Immunoglobulin Gene Rearrangement Study by the Polymerase Chain Reaction in a Colonic Adenocarcinoma FRANKLIN C. LING, M.B.B.S., COLLEEN E. CLARKE, R.T., AND DAVID LILLICRAP, M.D., F.R.C.P.C. The detection of clonal rearrangements of the immunoglobulin heavy chain gene by the polymerase chain reaction provides a rapid method to differentiate monoclonal from polyclonal Blymphocyte proliferations. It has been shown to be highly specific and so far, no false-positive results have been described. A case of a poorly differentiated colonic adenocarcinoma that showed a "false positive" clonal immunoglobulin heavy chain gene rearrangement by the polymerase chain reaction technique is reported. DNA contamination was unlikely because of the strict adherence to the laboratory polymerase chain reaction protocol and also the repeated demonstration of the same amplified band in a separate experiment using DNA extracted from another piece of tumor tissue. The apparent monoclonal immunoglobulin heavy chain gene rearrangement in the first polymerase chain reaction may be related to a combination of the paucity of lymphoid cells in the tissue sample and the presence within this small number of lymphocytes of a clonal reactive cell population. It is, therefore, important to correlate the routine microscopic and immunohistochemical findings in the interpretation of polymerase chain reaction results, especially when working with nonlymphoid tumors and lymphocyte-poor lesions. (Key words: Immunoglobulin heavy chain gene rearrangement; Polymerase chain reaction; Adenocarcinoma; Clonal proliferation) Am J Clin Pathol 1992; 98:116-119 The recent development of the polymerase chain reaction From the Department of Pathology. Queen's University and Kingston (PCR) to detect clonal rearrangements of the immunoGeneral Hospital, Kingston, Ontario, Canada. Supported by the Clare Nelson Bequest Research Fund from the Kingston General Hospital. Dr. Lillicrap was supported by an Ontario Ministry of Health Career Scientist Award. Received August 28, 1991; received revised manuscript and accepted for publication November 11, 1991. Address reprint requests to Dr. Lillicrap: Department of Pathology, Kingston General Hospital, Kingston, Ontario, Canada, K7L 2V7. globulin heavy chain (IgH) gene has provided a rapid and practical method to distinguish monoclonal from polyclonal B-cell proliferations.1,2 This method shows great promise in routine diagnostic surgical pathology because of its simplicity and short turnaround time, and because it is relatively inexpensive compared to previous studies using Southern blot analysis. A.J.C.P.-July 1992 LING, CLARKE, AND LILLICRAP 117 IgH Gene Rearrangement Study i' PCR in Colonic Adenocarcinoma The primary problem with the method is that monoclonality is only detected in about 80% of B-cell lymphoproliferative disorders.1,2 In a recent study performed at our institution, only 19 of the 34 cases of B-cell nonHodgkin's lymphomas showed monoclonal rearrangements by the PCR technique (sensitivity rate, 56%). (Ling F, Lillicrop D, unpublished observations). Possible reasons for the failure of amplification in some cases include suboptimal priming by available consensus primers, mutation or translocation involving the IgH gene, and the presence of PCR inhibitors in the tissue. The PCR technique is very specific for clonal B-cell lymphoproliferative lesions and no false-positive reactions have been reported. We describe a case of a poorly differentiated adenocarcinoma that showed a monoclonal rearrangement of the IgH gene by PCR. The possible causes for false-positive results and practical implications of this result are discussed. CASE REPORT A 71-year-old man came to the Kingston General Hospital with a right lower quadrant mass and weight loss. Computed tomographic scan showed a large tumor in the cecum and the ascending colon with metastatic deposits in the liver. A palliative right hemicolectomy with ileotransverse anastomosis was performed. The entire surgical specimen was immediately submitted to the laboratory. In addition to routine histologic examination, fresh tissue also was taken from the tumor for PCR and Southern blot analysis of IgH gene rearrangement as part of an ongoing study of the sensitivity and specificity of these methods to detect clonal B-cell proliferations. MATERIALS AND METHODS DNA Extraction DNA was extracted from fresh tumor tissue by treatment with sodium dodecyl sulfate and Proteinase K followed by phenol chloroform extraction, as previously described.3 The extracted DNA was precipitated with ethanol and redissolved in TRIS-EDTA buffer. Southern Blot Analysis The extracted DNA was digested with the restriction endonucleases EcoRl, Hindlll, and BamHl, size fractionated by agarose gel electrophoresis, and transferred to a nylon membrane (Gene Screen Plus, Dupont Canada Inc, Lachine, Quebec) by the Southern blotting method.4 The membrane was hybridized with an alpha - 32 P-dCTP-labeled probe from the J region of the IgH gene.5 After washing to a stringency of 0.1 X standard saline citrate, 0.1% sodium dodecyl sulfate at 65 °C for 30 minutes, the blot was subjected to autoradiography for 1 to 7 days. Polymerase Chain Reaction The PCR was performed according to the method of Wan and colleagues6 with some modifications. The prim- ers used were as follows. For the third framework portion of the V region: 5' ACACGGC(QT) (G/ QTGTATTACTGT 3' (Fr3A); for the J region: 5' TGAG GAGACGGTGACC 3' (LJH); or 5' GTGACCAGGGTNCCTTGGCCCCAG 3' (VLJH). A nested PCR procedure was performed in a Perkin-Elmer Cetus Thermal Cycler using Thermus aquaticus (Taq) polymerase (Perkin-Elmer Cetus, Norwalk, CT). The PCR reaction mixture (100 JUL) contained 0.2 jtmol/L of each primer, 5 units of Taq polymerase, 0.8 mmol/L of a dNTP mix, 3 mmol/L magnesium sulphate, 16.6 mmol/L ammonium sulphate, 10 mmol/L beta-mercaptoethanol, and 67 mmol/L TRIS-HCl (pH 8.0). A first round of 25 PCR cycles was performed using primers Fr3A and LJH. In the second round of 20 PCR cycles, Fr3A and the internal nested primer VLJH were used. Each PCR cycle consisted of denaturation at 94 °C for 2 minutes, annealing at 60 °C for 2 minutes, and extension at 72 °C for 2 minutes. The final amplified product was electrophoresed and visualized under ultraviolet light after staining with ethidium bromide. Special precautions were taken to avoid DNA crosscontamination and PCR carryover. Stringent laboratory guidelines were followed during the entire DNA extraction and PCR procedures, as suggested by Kwok and associates.7 These included extraction of DNA in a class II biological containment cabinet separate from our PCR area, dedicated sets of supplies and positive-displacement pipetting devices for PCR, use of disposable gloves, and inclusion of "no DNA template" tubes as negative controls in every run. RESULTS Histologic sections of the tumor showed a poorly differentiated adenocarcinoma extending through the muscularis propria into the serosal fat. There was only a mild host inflammatory response that was present primarily at the margins of the tumor and consisted predominently of small lymphocytes. The tumor cells showed strong positive staining for low-molecular-weight keratin and negative staining for leukocyte common antigen. Southern blot analysis showed a normal germline band with no evidence of clonal IgH gene rearrangement. The PCR, however, yielded a discrete amplified band (Fig. 1, T l ) suggesting a clonal B-cell proliferation. Because the PCR finding was completely unexpected for what had now been identified morphologically as an adenocarcinoma, DNA was extracted from a separate piece of fresh frozen tumor tissue and processed for a second PCR. The result of the second PCR is also shown in Figure 1 (T2). The amplified products from the second piece of tumor tissue formed a diffuse band on the gel, but in addition the same amplified band seen in the first PCR was Vol. 98 • No. 1 118 ANATOMIC PATHOLOGY Single Case Report T1 T2 L 126—• : " 1 ^ s*4 FIG. 1. Polymerase chain reaction analysis of IgH gene rearrangement. Amplified DNA from the first and second PCR of the colonic tumour are in tracks Tl and T2, respectively. Track P is marker DNA with relevant size markers labelled in base pairs along the left hand side. Track L is amplified DNA from a B-cell lymphoma. The track between P and Tl is a negative control in which no DNA template was included in the reaction. still identifiable, although it was less intense than in the initial PCR. DISCUSSION Immunoglobulin gene rearrangement analysis by the PCR is very specific for B-cell lymphoproliferative disorders. Previous studies have shown no false-positive reactions. The case reported here showed a positive PCR for IgH gene rearrangement although the morphologic and immunohistochemical stains were diagnostic of adenocarcinoma. Furthermore, IgH gene rearrangement study was negative on Southern blot analysis. One of the primary problems with the PCR is contamination by DNA from extraneous sources. Because of the exquisite sensitivity of this technique, even very low levels of DNA contamination can result in erroneous test data. The effect is especially problematic if contamination involves products of a completed PCR that provides high concentrations of a specific DNA template. DNA contamination is unlikely to have been the cause of false-positive results in this case because of meticulous specimen handling and strict adherence to laboratory PCR protocol. In addition, there were no unexpected findings in other PCR analyses at the time of this study. Furthermore, the finding of the same amplified band in a second independent PCR using DNA extracted from another piece of tumor tissue essentially precludes contamination as the cause of false-positive results. Nevertheless, there were significant differences between the results of the first and the second PCR. Although the same amplified band could still be recognized in the second PCR, it was much less distinct and was present with a diffuse smear in the background. The difference in appearance of the amplified products in the first and second PCR implies some important differences in the cellular composition between the two tissue samples despite the fact that they were both taken from the same tumor. Unfortunately, morphologic confirmation of this theory was not possible in this case. Understanding the underlying principle of PCR analysis of IgH gene rearrangement helps to explain the observed differences and may suggest a possible cause for the false-positive reaction in this case. In contrast to the use of the PCR to amplify a segment of DNA unique to the neoplastic clone, such as t(14;18) chromosome breakpoints in follicular lymphomas, 8 the amplification of rearranged IgH genes is not specific for the neoplastic population. The detection of monoclonality by PCR is, in essence, a quantitative comparison of all rearranged IgH gene segments to identify a predominant rearrangement that will appear as a distinct band on electrophoresis. It follows that the specificity of the PCR in predicting monoclonality will rely on the presence of a sizeable and representative population of lymphoid cells. If very few lymphoid cells are sampled and amplified, a distinct "monoclonal" band may be produced, regardless of whether the lymphocytic infiltrate is neoplastic or reactive. This "sampling artefact" will be more evident in PCR than Southern blot analysis because of the inherent sensitivity of the former procedure. Adequate sampling of lymphoid cells is not a problem in lesions rich in lymphocytes. However, it could be a factor in lymphocyte-poor lesions, as in this colonic adenocarcinoma. It is possible that the first PCR reaction was performed on tissue that contained sheets of carcinoma cells with very few lymphocytes and thus resulted in a false-positive monoclonal reaction. The production of a less distinct band against a stronger polyclonal background in the second PCR could be due to sampling of more lymphoid cells in the second specimen, thereby ameliorating the effects of the sampling artefact. Another possible explanation for the false-positive PCR was the presence of a clonal lymphocytic proliferation in response to specific antigens on the carcinoma cells. Clonal lymphoid rearrangements have been detected in a variety of nonmalignant lymphoproliferative disorders.9 Although this might have been a contributing factor in this case, it alone cannot explain the observed differences between the two PCR reactions and the negative Southern blot result. Immunoglobulin heavy gene rearrangement study by the PCR technique is a new and powerful method to detect clonal B-lymphocyte proliferations. Although it is highly specific, false-positive reactions can still occur, as illustrated by this case. We have examined 19 other control cases, including T-cell lymphomas (two), Hodgkin's disease (three), reactive lymphadenopathy (five), reactive marrow lymphocytosis (seven), and metastatic carcinoma (two), and none of them have shown a monoclonal rear- A.J.C.P. • July 1992 SCHOFIELD, AGOSTINI, AND YUNIS 119 Microvillus Inclusion Disease rangement on PCR (Ling F, Lillicrop D, unpublished observations). The case reported here is the only case of false-positive reaction we have encountered and this is also the only primary colonic carcinoma included in our study. The authors believe that the most probable explanation for the positive PCR in this instance is related to the paucity of lymphoid cells in the tissue samples. This report reemphasizes the importance of correlating the tumor morphologic and immunohistochemical findings in the interpretation of PCR results. 3. 4. 5. 6. 7. 8. REFERENCES 1. Trainor KJ, Brisco MJ, Story CJ, Morley AA. Monoclonality in Blymphoproliferative disorders detected at the DNA level. Blood 1990;75:2220-2222. 2. McCarthy KP, Sloane JP, Wiedemann LM. Rapid method for dis- 9. tinguishing clonal from polyclonal B cell populations in surgical biopsy specimens. J Clin Pathol 1990;43:429-432. Maniatis T, Fritsch EF, Sambrook J. Molecular Cloning: A Laboratory Manual. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory, 1982. Southern EM. Detection of specific sequences among DNA fragments separated by gel electrophoresis. J Mol Biol 1975;98:503-517. Arnold A, Cossman J, Bakhshi A, Jaffe ES, et al. Immunoglobulin gene rearrangements as unique clonal markers in human lymphoid neoplasms. N Engl J Med 1983;309:1593-1599. Wan JH, Trainor KJ, Brisco MJ, Morley AA. Monclonality in B cell lymphoma detected in paraffin wax embedded sections using the polymerase chain reaction. J Clin Pathol 1990;43:888-890. Kwok S, Higuchi R. Avoiding false positives with PCR. Nature 1989;339:237-238. Crescenzi M, Seto M, Herzig GP, Weiss PD, et al. Thermostable DNA polymerase chain amplification of t( 14; 18) chromosome breakpoints and detection of minimal residual disease. Proc Natl Acad Sci USA 1988;85:4869-4873. William CL, Griffith BB, Whittaker M. Molecular genetic approaches for the diagnosis of clonality in lymphoid neoplasms. Clin Lab Med 1990;10:119-149. Gastrointestinal Microvillus Inclusion Disease DEBORAH E. SCHOFIELD, M.D., ROCCO M . AGOSTINI, J R . , B.S., AND EDUARDO J. YUNIS, M.D. A 3-year-old girl of Navajo heritage had intractable diarrhea beginning at 4 days of age and resulting in long-term hyperalimentation. Investigation before multivisceral transplantation included biopsies of the rectum, stomach, duodenum, and liver. The diagnosis of microvillus inclusion disease was established by documentation of microvillus inclusions in duodenal epithelial cells. A trial of somatostatin therapy was ineffective in controlling the diarrhea. Subsequently, a multivisceral organ transplant provided a unique opportunity to establish the gastrointestinal extent of involvement of this disease. Ultrastructural microvillus inclusions were identified in the duodenum, jejunum, ileum, and colon, but not in the gallbladder. A few inclusions also were documented in gastric antral epithelial cells. Alkaline phosphatase stains performed on paraffin-embedded material showed a few inclusions in the antrum of the stomach and many inclusions throughout the small intestine, primarily in surface epithelial cells but also in upper crypt cells. (Key words: Villus atrophy; Microvillus inclusion; Chronic intractable diarrhea of infancy; Familial enteropathy; Intestinal alkaline phosphatase) Am J Clin Pathol 1992; 98:119-124 Microvillus inclusion disease was first characterized in 1978,' although cases probably had been included in earlier reports of protracted diarrhea occurring in infancy.2'3 Intractable diarrhea typically begins early in infancy and the prognosis is poor. Diagnosis is based on demonstration of mucosal atrophy with loss of villi accompanied by ultrastructural demonstration of internalized inclusions of From the Department of Pathology, Children's Hospital of Pittsburghmicrovilli within enterocyte cytoplasm. Familial cases and the University of Pittsburgh, Pittsburgh, Pennsylvania. have been reported and occur in a pattern consistent with autosomal recessive inheritance. We are unaware of reReceived August 20, 1991; received revised manuscript and accepted for publication November 11, 1991. ports of ultrastructural findings in organs other than the Address reprint requests to Dr. Schofield: Department of Pathology, small intestine, colon, rectum, and kidney. When a 3The Children's Hospital, 300 Longwood Avenue, Boston, Massachusetts year-old girl afflicted with this unrelenting disease under02115. Vol. 98 • No. I