Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
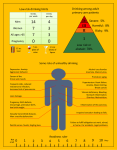
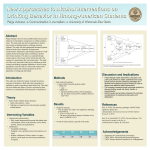
Overview of the SBIRT Process David P. Miller, MD, MS, FACP Associate Professor Internal Medicine and Public Health Sciences 5 Basic Components of an SBIRT System Prescreening (1-2 question screen) Screening (AUDIT / DAST; CRAFFT) Clinician Intervention for all screen-positive clients Referral as appropriate for clients with higher levels of risk or possibly dependent Follow-up assessment/reinforcement at future visits 2 STEP 1: Prescreen is routinely performed every 6-12 months Tools: Single alcohol screening question (SASQ - NIAAA) single drug screening question (NIDA) 3 Prescreening Questions “Single Alcohol Screening Question” (NIAAA) 1. Do you sometimes drink beer, wine, or liquor? 2. How many times in the past year have you had more than (3 or 4) drinks in a day? “Single-Item Drug Use” (NIDA) 1. How many times in the past year have you used an illegal drug or used a prescription medication for nonmedical reasons? 4 STEP 2: Administer screening IF prescreen is positive Tools: AUDIT (for alcohol) DAST-10 (for drugs) 5 AUDIT (for + alcohol prescreen) Healthy Lifestyles Screen (AUDIT) PATIENT: Because alcohol use can affect your health and can interfere with certain medications and treatments, it is important that we ask some more questions about your use of alcohol. If we find that you are drinking more than you or we feel is good for you, we have some services right here that can help you take better care of yourself. Your answers will remain confidential so please be honest. Place an X in one box that best describes your answer to each question. QUESTIONS 1. How often do you have a drink containing alcohol? 2. 3. 4. 5. 6. 7. 8. 9. How many drinks containing alcohol do you have on a typical day you are drinking? How often do you have four or more drinks on one occasion? How often during the last year have you found that you were not able to stop drinking once you had started? How often during the past year have you failed to do what was expected of you because of drinking? How often during the past year have you needed a drink first thing in the morning to get yourself going after a heavy drinking session? How often during the past year have you had a feeling of guilt or remorse after drinking? How often during the past year have you been unable to remember what happened the night before because of your drinking? Have you or someone else been injured because of your drinking? 10. Has a relative, friend, doctor, or other health care worker been concerned about your drinking and suggested you cut down? 6 0 Never 1 Monthly or less 2 2-4 times a month 3 2-3 times a week 4 4 or more times a week 1 or 2 3 or 4 5 or 6 7 to 9 10 or more Monthly Weekly Monthly Weekly Monthly Weekly Daily or almost daily Monthly Weekly Daily or almost daily Never Never Never Never Less than monthly Less than monthly Less than monthly Less than monthly Daily or almost daily Daily or almost daily Never Less than monthly Monthly Weekly Daily or almost daily Never Less than monthly Monthly Weekly Daily or almost daily No No Yes, but not in the past year Yes, but not in the past year Yes, during the past year Yes, during the past year Adapted from World Health Organization 3 quantity & frequency questions (1-3) 3 questions probing signs of dependency (4-6) 4 questions about alcohol-related problems (7-10) Score Range: 0 - 40 DRUG USE QUESTIONNAIRE (DAST -10) These questions refer to the past 12 months only: 1. Have you used drugs other than those required for medical reasons? 2. Do you abuse more than one drug at a time? 3. Have you had medical problems as a result of your drug use (e.g., memory loss, hepatitis, convulsions, bleeding, etc.)? 4. Have you had “blackouts” or “flashbacks” as a result of drug use? 5. Do you ever feel bad or guilty about your drug use? 6. Does your spouse (or parent) ever complain about your involvement with drugs? 7. Have you neglected your family because of your use of drugs? 8. Have you engaged in illegal activities in order to obtain drugs? 9. Have you ever experienced withdrawal symptoms (felt sick) when you stopped taking drugs? 10. Are you always able to stop using drugs when you want to? Circle Response Yes No Yes No Yes No Yes Yes Yes No No No Yes Yes Yes No No No No Yes DAST-10 score (add circled responses in left column) www.sbirtonline.org Southeastern Consortium for Substance Abuse Training © 2013 DAST-10 Advantages Short, self-administered 8 www.sbirtonline.org Disadvantages Is not drug-specific Validation data is limited Does not distinguish between active and inactive illicit drug use Focuses on dependence Southeastern Consortium for Substance Abuse Training © 2012 Risk Zones AUDIT Score: ≥ 14 DAST Score: 3-10 1-2 1-13 (No drug use) Sensitivity & specificity in the discrimination of drug use disorders with psych populations are optimized with a score of ≥3 (Maisto et al., 2000) 9 www.sbirtonline.org Southeastern Consortium for Substance Abuse Training © 2012 Prescreening/Screening for Adolescents: CRAFFT During the past 12 months, did you: Drink any alcohol (more than a few sips)? Smoke any marijuana or hashish? Use anything else to get high? 10 Prescreening/Screening for Adolescents: CRAFFT 11 Ask everyone Risk Zones CRAFFT 12 >2 High Risk 0 or 1 (use alcohol or drugs) At Risk 0 Low/No Risk www.sbirtonline.org Southeastern Consortium for Substance Abuse Training © 2012 STEP 3: Administer Brief Intevention 13 Components of a Brief Intervention Ask permission Provide feedback Enhance motivation Provide advice Discuss next steps Close on good terms 14 Intervention Guide Zone I: At Risk AUDIT 1-13 (≥ 1 binge); DAST 1-2 Ask Permission Provide Feedback Enhance Motivation & Elicit Change Talk 15 Zone II: High Risk, Possibly Dependent AUDIT ≥ 14; DAST 3-10 “I appreciate your answering our health questionnaire. Could we take a minute to discuss your results?” Refer to pyramid & provide patient’s AUDIT/DAST score & risk level(s). [As your physician] “Drinking/using at this level can be harmful to your health and possibly responsible for the health problem for which you came in today. What do you make of that?” “What are the good things/not so good things about your alcohol/drug use?” (Decisional balance) “On a scale of 0-10, how important is it that you cut back or quit your alcohol/drug use?” If >0, “Why that number and not a lower one?” [Use rulers to also ask about confidence, readiness] “Have you ever considered cutting back or quitting?” If so, “Why?” If not, “What would have to happen for you to consider cutting back/quitting?” Provide Advice Refer to chart on front of card in providing advice to quit or cut down as per NIH guidelines (or offer advice to quit or cut back drug use). Discuss Next Steps “If you were to make a change, what would be your first step?” Close on Good Terms Summarize, emphasize patient strengths, highlight change talk and decisions made. Arrange for follow-up as appropriate. Zone II Additional Steps: Ask: “If you go a day or 2 without drinking/using do you ever get sick, shaky, have tremors/seizures/cramps, or see/hear things that are not there?” Offer menu of options for more help: ► Medication (naltrexone, acamprosate, disulfiram, methadone, Suboxone) ► Referral •Counseling/Brief treatment •Support group (e.g., AA, NA, Celebrate Recovery) •Treatment or substance abuse program www.sbirtonline.org Funded by: Rev. Mar 2012 Intervention card adapted from Oregon Health & Sciences University SBIRT Primary Care Residency Initiative STEP 4: Refer to Treatment (if indicated) 16 Local Treatment Resources Detox Inpatient Outpatient Faith-based Long-term residential 17 STEP 5: Follow-up Reassess Reinforce 18 19