Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
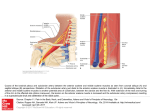
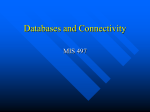
British Journal of Anaesthesia 111 (5): 840–9 (2013) CORRESPONDENCE Dorsal scapular nerve injury: a complication of ultrasound-guided interscalene block Editor—In-plane ultrasound guidance is often used for interscalene block. This approach shifts the traditional needle insertion point of the Winnie’s approach, that is, in the groove between the anterior and the middle scalene muscles,1 to a more distal (either medial or lateral and caudal) puncture site.2 The increased risk of both vascular and phrenic nerve lesions, carried by the medial to lateral approach,3 often makes anaesthetists to choose a lateral to medial needle direction to reach the brachial plexus in the interscalene groove through the middle scalene muscle. However, this approach increases the theoretical risk of damage to other branches of brachial plexus, namely the long thoracic and the dorsal scapular nerves (DSN), which run inside or in close proximity to the middle scalene muscle.4 DSN originates from the fifth cervical nerve root, with a possible contribution of C6 and after its origin runs in close proximity of the upper trunk of the brachial plexus, before piercing the middle scalene muscle and passing posteriorly, beneath the levator scapula muscle. It is responsible for the motor innervation of the levator scapula muscle itself, which elevates the scapula, and of both the rhomboid major and minor muscles, which pull the scapula medially.5 DSN injuries can be the origin of a well-defined chronic pain syndrome, often referred to as DSN syndrome. DSN syndrome is often characterized by a dull ache along the medial border of the scapula, eventually radiating to the lateral surface of the arm and forearm. Patients usually complain of a not well-defined shoulder pain and dysfunction, with different degrees of functional impairment. Weakness and hypotrophy of the rhomboid, the levator scapulae muscles, or both can be present as well. The long thoracic nerve (LTN) runs within or next to the middle scalene muscle, often in close proximity of the DSN and thus can be injured by the same mechanisms during performance of an in-plane ultrasound-guided interscalene block. A lesion of the LTN often results in a chronic pain syndrome of the shoulder, with associated different degree of serratus anterior muscle palsy, determining impairment of shoulder elevation and a characteristic scapular winging with medial translation and rotation of the inferior angle towards the midline.6 Both DSN syndrome and LTN syndrome symptoms are not specific and the often poorly defined pain characteristics and GE Le C5 AS 1 MS C6 LTN C7 2 Fig 1 Ultrasound image of DSN (arrow) located within the middle scalene muscle. AS, anterior scalene muscle; MS, middle scalene muscle; C5, C6, C7, fifth, sixth, seventh cervical roots; LTN, long thoracic nerve. & The Author [2013]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: [email protected] BJA Correspondence extension are the cause of frequent misdiagnoses, being confused with other shoulder chronic pain syndromes. DSN lesions have been described in the context of trauma to the brachial plexus or entrapment syndromes, in which they are a relatively common cause of shoulder dysfunction.7 8 However, may be because of difficulty in diagnosing if not specifically searched for, DSN injuries have never been described as a direct complication of an ultrasound-guided interscalene block. In this context, a lesion, likely due either to direct needle trauma or to intraneural injection, seems to be not only possible, but also likely relatively frequent (even if not reported), if DSN and LTN are not preliminary systematically identified, in order to choose the safest needle trajectory. Hanson and Auyong4 demonstrated that DSN and LTN can be identified by ultrasound in the majority of patients (Fig. 1). We encourage this practice in all patients undergoing an ultrasound-guided interscalene block. Declaration of interest None declared. A. Saporito Bellinzona, Switzerland E-mail: [email protected] 1 Winnie AP. Interscalene brachial plexus block. Anesth Analg 1970; 49: 455– 66 2 Mariano ER, Loland VJ, Ilfeld BM. Interscalene perineural catheter placement using an ultrasound-guided posterior approach. Reg Anesth Pain Med 2009; 34: 60–3 3 Kessler J, Schafhalter-Zoppoth I, Gray AT. An ultrasound study of the phrenic nerve in the posterior cervical triangle: implications for the interscalene brachial plexus block. Reg Anesth Pain Med 2008; 33: 545–50 4 Hanson NA, Auyong DB. Systematic ultrasound identification of the dorsal scapular and long thoracic nerves during interscalene block. Reg Anesth Pain Med 2013; 38: 54–7 5 Tubbs RS, Tyler-Kabara EC, Aikens AC, et al. Surgical anatomy of the dorsal scapular nerve. J Nerurosurg 2005; 102: 910–1 6 Wiater JM, Flatow EL. Long thoracic nerve injury. Clin Orthop Relat Res 1999; 368: 17 –27 7 Sultan HE, Younis El-Tantawi GA. Role of dorsal scapular nerve entrapment in unilateral interscapular pain. Arch Phys Med Rehabil 2013; 94: 1118–25 8 Jerosch J, Castro WH, Geske B. Damage of the long thoracic and dorsal scapular nerve after traumatic shoulder dislocation: case report and review of the literature. Acta Orthop Belg 1990; 56: 625– 7 only recently, navigation systems received a CE mark in Europe. So far the interventional nurses and physicians, in the field of vascular access in Europe, have been using the ECG method, fluoroscopy, and/or anthropometric methods in order to locate the position of the tip in the cavo-atrial junction. This point is considered to have a certain advantage when it comes to intravascular therapy.3 We present, for the first time ever in Europe, two instances where a new navigation system was used for advancing a peripherally inserted central catheter (PICC) (VasoNova, Arrow International, Reading, PA, USA). The device uses real-time internal physiological parameters that are unaffected by the patient’s cardio-pathophysiological condition as it is designed to achieve optimal placement of the catheter in the lower third of the superior vena cava and specifically at the cavo-atrial junction. In both cases, the basilic vein was punctured under ultrasound guidance. With further advancement of the catheter for about 20 cm, a red signal came up as the catheter entered the internal jugular vein which was neither compressed nor observed using the ultrasound device for identification. After confirming that the PICC had advanced in the internal jugular, the catheter was pulled back and re-advanced. In total, the PICC was advanced 46 cm from the entrance point (48 cm had been estimated using anthropometric methods). As the PICC reached the optimum point, the maximal P showed up on the navigation device and the bull’s eye appeared on the screen (Fig. 1). The procedure in the second patient (an 84-yr-old woman suffering from osteomyelitis who needed to receive i.v. antibiotics and fluid administration for more than 2 months) was performed by a trainee. The whole procedure lasted about 15 min and the advancement of the catheter lasted 3.5 min. At first glance, this navigation system appears to have the feel of a computer game. There is no need for simultaneous ultrasonography of the internal jugular vein. In the unlikely doi:10.1093/bja/aet358 Navigation-assisted peripherally inserted central catheter’s insertion performed by university degree nurses: technical report of two cases Editor—Although central catheters inserted peripherally under ultrasound guidance is a common procedure used worldwide,1 2 Fig 1 Bull’s eye appearance, indicating that the tip of the catheter is at the cavo-atrial junction. 841