Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
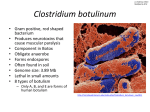
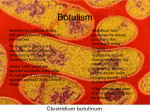
Silent Murder associated with home-canned-preserved bamboo shoots. Yotsawee Chotechuang , M. D. Teeraya Puavilai , M.D. Pornthep Worawongprapa , M.D. Department of Internal Medicine, Lampang hospital. ABSTRACT Seven patients from the same residential area came to Lampang hospital with the same clinical presentation of progressive dysphagia, dysarthria, paralysis and bilateral ptosis preceded by abdominal cramps, nausea, vomiting, and diarrhea after all of them had eaten home-canned-preserved bamboo shoots bought from the weekend central-village market. Although botulism was rare but potentially fatal illness. Prompt recognition of clinical syndrome plays an important role in decreasing morbidity and mortality rates. This report provided a clinical overview, progression and management in one of seven patients who was suffered from botulism and brief review literature about thi.s disease. We hope that this report will be advantage for physicians and healthcare workers to prevent misdiagnosis and delay treatment in the patients with these clinical syndrome. Key words: Foodborne Botulism, Home-canned-preserved bamboo shoots. INTRODUCTION Preserved bamboo shoots (cooked and uncooked) was a kind of cultural favorite foods of Thai Northern people. One day on November 2003, seven patients from the same Tambon, District and Province, came to hospital with the same clinical presentation of progressive dysphagia, dysarthria, paralysis and bilateral ptosis preceded by abdominal cramps, nausea, vomiting, diarrhea after all of them had eaten home-canned-preserved bamboo shoots which bought from the weekend central-village market. What's happen to them? PRESENTATION OF CASE A 36-year-old woman, couple, agriculture, in Sobprap District, Lampang Province was admitted to Lampang hospital on 26 November 2003 because of having diarrhea followed by multiple cranial-nerve palsies. Three days prior to admission, she had watery diarrhea, nausea, vomiting, abdominal pain, weakness and fatigue around six hours after ingestion home-canned-preserved bamboo shoots which she bought from the weekend central-village market. She had no fever (No medications had been taken). The next day, she began to have difficulty in drinking water and swallowing both liquid and soft food. Blurred vision was noted. She could walk well at that time. She was taken to a private hospital where computer tomographic (CT) scan was performed, and unremarkable result. She was admitted to the hospital and got nasogastric tube for feeding, supportive and symptomatic treatment while observing her neurological sign. Approximately 24 hours after admission, she complained perioral numbsness and worsening dysphagia. Her speech became severe slurred. Bilateral ptosis was seen but she could move her eyes in all directions. She was unable to stand, walk, and write complete coherent sentences. She complained that her legs was more severe weakness than her arms. Then she was transferred to Lampang hospital. The patient had no history of underlying diseases, exposure to pets or ticks, recent foreign travel, use of alcohol or drugs, previous neurologic problems, and loss of vision. Physical examination revealed that the temperature was 3 6 . 5 ' ~ ,the pulse rate was 82 Imin, the respiratory rate was 20 Imin and the blood pressure was 120180 mmHg. General physical examination showed no abnormalities. On neurological examination, the patient was drowsy, bilateral ptosis and countable fingers. She gave appropriate positive or negative response by turning either thumb up or down. Both pupils were 3 mm. in diameter and equally reacted to light. Extraocular movement was normal. Facial sensation and hearing were intact. Uvula was in midline position. She could not protrude her tongue. Sternocleidomastoid strength was 315 bilaterally. Decreased in gag reflex was noted. Proximal muscle strength was 315 in both arms and legs. Vibratory, pinprick, light touch, joint position, and temperature sensations were intact. All deep tendon reflexes were l+.Plantar responses were flexion. Stiffness of neck was absent. The patient could not cooperate during tests of coordination. Four hours after admission, her consciousness was down to stuporous. She used abdominal muscle to respiration. the respiratory rates was 32 to 35 /min and secretion sound was heard on both lungs. She was intubated endotracheal tube and transferred to intensive care unit. The results of laboratory tests throughout the course of the patient's illness was showed in Tables 1 to 3. A chest radiograph showed alveolar infiltration in right lower lung field, findings consistent with the presence of suspected aspiration pneumonia. A cranial CT scan showed unremarkable study. Hemoculture, sputum examination and sputum culture were done. Empirical antibiotics were Ceftriaxone 2 gm. intravenous once daily and .Metronidazole 500 mg, intravenous every eight hours per day. Specimens of stool and urine were obtained. for culture and toxin studies. Botulinum antitoxin was not administered due to it was not available in Thailand. TABLE 1. Hematologic Laboratory values on admission in Lampang Hospital. VARIABLE ON ADMISSION DAY 6 12.9 11.8 24,800 26,400 Neutrophils 90 85 Lymphocytes 6 7 Platelet count (per mm3) 229,000 271,000 Red cell morphology NCNC* NCNC* Hemoglobin (g %) Hematocrit (%) MCV (pm3) White-cell count (per mm3) Differential count (%) Monocytes Bands - * Normocytic Nornlochrornic. TABLE 2. Blood Chemical values. VARIABLE ON ADMISSION Glucose, (mgldl) BUN (mgldl) DAY 6 160 6 Creatinine (mgldl) 0.6 Sodium (mEq1L) 132 Potassium (mEq/L) 3.6 Chloride (mEq/L) 105 Carbon dioxide (mEq/L) 26 Albumin (gmldl) 3.3 Calcium (mgldl) 8.9 Phosphorus (mgldl) 3.5 Magnesium (mgldl) 2.9 TABLE 3. Results of Lumbar puncture. VARIABLE Appearance of fluid FINDING Clear, colorless Cells (per mm3) No cell Glucose (mg%) 97 ( log* ) Protien (mg%) 38 Stained smear No microorganism * Plasma glucose. On the second hospital day, the temperature was 3 7 . 5 ' ~to 3 8 . 2 ' ~ ,the blood pressure was 110170 mmHg. Drowsiness and complete external ophthalmoplegia were presented. Bilateral pupils were 3 mm. in diameter and sluggish react to light. Bilateral ptosis persisted. Both arms and legs were flaccid. Bilateral muscle strength was 115 in proximal and 415 in distal of upper extremities. Both her legs; muscle strength was 015 in proximal and 315 in distal. Deep tendon reflexes of her arms remained l+. Knee and ankle jerks were areflexia. Plantar responses were flexion. Pyridostigmine Bromide (360 mg daily) were administered. On the fifth day, she was stuporous. The temperature was 3 6 . 7 ' ~ .The pulse rate was 120 Imin The blood pressure was 90160 mmHg. Bilateral ptosis persisted. The cranial-nerve deficits and bilateral abnormal pupils were unchanged. Generalized flaccid and hyporeflexia was noted. The hemoculture was no growth in two days. Motor conduction studies was not performed due to unstable hemodynamics of this patient. On the sixth day, her neurological signs were unchanged. Her vital signs was unstable. Inotropic agents were administered. She had sudden cardiac arrest and the cardiopulmonary resuscitation was performed. Postmortem study was not performed. DISCUSSION This patient had acute, afebrile, and bilateral cranial-nerve paralysis that worsened over the period of hours. In patients with muscle weakness could be explained by a lesion at one of four sites: ea the central motor neurons and their descending tracts, the nerves, the neuromuscular junctions, or the muscles themselves"'. Primary muscle disease can result in oropharyngeal weakness, and ptosis can occur in cases of primary muscle disease, but it would be exceptional for myopathy to evolve over a period of two or three days. Furthermore, oculomotor paralysis is not typical feature of muscle disease, except in cases of progressive external ophthalmoplegia (a type of mitochondria1 myopathy), thyroid ophthalmopathy, and oculopharyngeal dystrophy, all of which are ingravescent processes. Muscle disease is therefore unlikely because of the rapid in progression, distribution, and severity of the weakness in this case. Polymyositis is usually insidious and only rarely fulminant. Proximal-limb weakness and facial weakness are common manifestations, and dysphagia occurs in more than 25 percent of cased2'. Although muscle tenderness and cramping are common, the absence of pain is not unusual. The deterioration in this patient, however would be exceptional even for fulminant polymyositis. Ptosis is rare in polymyositis. Periodic paralysis, which includes a group of disorders that cause rapid and profound weakness, frequently with loss of reflexes, tends to occur in the first few decades of life. Involvement of cranial nerves is infrequent, and involvement of ocular muscles is very rare. Disorders of the neuromuscular junction could explain this patient's illness, because they preferentially involve ocular and cranial muscles - the ones with the lowerest threshold for synaptic failure. The most common neuromuscular disorder, Myasthenia gravis, may progress rapidly, causing ptosis and oropharyngeal, oculomotor, proximal-limb weakness and respiratory failure. Until the reflex and sensory loss became evident later in course of the disease, myasthenia gravis was a defensible diagnosis. However, the pupils are not overtly affected in patients with myasthenia gravis, and total ophthalmoplegia is uncommon with this disorder. Another disease of neuromuscular junction which generally begins with a nasal voice, dysarthria, that warrants consideration is ~otulism'~', dysphagia and ptosis. In this case, the evolution of neurologic signs over a period of hours, and then days, after a gastrointestinal illness is also suggestive of botulism, caused by a toxin synthesized by Clostridium botulinum. Ophthalmoparesis, facial weakness, and bulbar palsy are the most common initial symptoms of the disease. Despite pharyngeal weakness, a gag reflex is often preserved, as in this case. Dilatation of the pupils is common but may be absent, in one series, less than half the patients had dilated pupils'4'. Limb weakness and respiratory compromise may follow, although respiratory weakness can occur without severe limb weakness. Reflexes may be depressed or absent. Sensation and cognition are almost always preserved. Evidences which strongly support the diagnosis of botulism in this patient: First, history of ingestion of home-canned-preserved bamboo shoots which prone to contaminate with botulinum toxin and had evidence of outbreak of foodborne (home-canned-preserved bamboo shoots) botulism in Northern of Thailand in 1998'~'. Second, the neighborhood and her friends from the same village had clinically signs and symptoms of illness like her, by all of the neurologic signs changed over a period of hours, the interval less than 24 hours, after the gastrointestinal illness, and every patients had an important history of ingestion home-cannedpreserved bamboo shoots which they bought from the same sources and on the same day like her that preferably thought to botulism first, because botulism may occur in the clusters of people ingesting the same tainted food, but sporadic cases are not unusual. Third, she was afebrile, eventhough there is no mention of prominent dryness of the mouth and throat, which typical of the early stage of botulism, botulism could not be ruled out in this patient. The diagnosis of botulism can be made by injecting a sample of the patient's serum or a preparation of tainted food into mice intraperitoneally. The test is positive if the mouse becomes paralyzed and dies"'. But this procedure is not widely available. Another weakness due to neuromuscular junction dysfunction is seen in the Lambert-Eaton syndrome"', but it was progressed slowly, and cranial-nerve involvement was usually not as conspicuous as in this case, and respiratory failure is rare. Hypermagnesemia and the administration to an Aminoglycoside or Polymixin can cause neuromuscular in this case. but neither was a factor Any acute weakness of cranial musculature demands a consideration of disease of the cranial-nerve nuclei in brain stem, especially the common problem of infarction of pons and midbrain from occlusion of the basilar artery. It was also difficult to conceive of a process that affects the widely dispersed brain-stem nuclei innervating the ocular, facial, and oropharyngeal muscles but spare the adjacent corticospinal tracts. Involvement of the corticospinal tracts is almost essential for the diagnosis of occlusion of the midbasilar artery. Exception to these rule include Wernicke's disease that involves the brain-stem nuclei and causes ophthalmoplegia and syringobulbia, with may affect several cranial-nerve nuclei, but neither disease explains the other features of this patient's illness. Bulbar poliomyelitis could account for the pattern of destruction of brain-stem motor neurons in this patient, but it rarely causes ophthalmoplegia and was unlikely because of the absence of fever during early phase of the neurologic illness and the normal cerebrospinal fluid findings. The syndrome of acutely advancing ocular, facial, and oropharyngeal weakness coupled with limb weakness is acute inflammatory demyelinating polyneuropathy (Guillain-Bank syndrome). Predominant weakness of the ocular and oropharyngeal muscles characterized one of several variants of the Guillain-BmC syndrome in which weakness was purely or predominantly regional. All these variants are linked to the typical form of the Guillain-BmC syndrome by the presence of generalized areflexia weakness; shared electromyographic features, which may abnormal only in weakened regions; and elevated cerebrospinal fluid protien level in some cases. The differential between botulism and Guillain-BmC syndrome and its variants was showed in Table 4. Other causes of cranial polyneuropathy do not satisfactorily explain an acute symmetric paralysis involving cranial nerves I11 through XII. Neoplastic meningeal infiltration evolves more gradually, affects the nerves unilaterally or asymmetrically, and results in abnormalities in the cerebrospinal fluid. Infectious disease and noninfectious granulomatous diseases, such as tuberculosis, fungal infections, syphillis, Lyme disease, sarcoidosis, Wegener's granulomatosis, and idiopathic granulomatous disease, can cause cranial polyneuropathy, but not as acute and severe as in this case. Diptheria may associated with the cranial neuropathy but rare and exudative pharyngeal membrane was not detect in this patient. From many reasons above, the differential diagnosis of this patient were Botulism, Guillain-BmC syndrome and its variants, Myasthenia gravis, respectively. All of them can be distinguished by their electromyographic studies, but limit in this case due to complications from aspiration pneumonia with respiratory failure. Guillain-BmC syndrome, the result was initially be normal or almost normal. Myasthenia gravis, by demonstrating the absence of a decrement in muscle contraction with repetitive nerve stimulation. Botulism, by demonstrating the absence of an increment in muscle contraction. Seven patients who were suffered from botulism in Larnpang hospital, between November to December 2003, the median age was 40 years (range from 29 to 59 years), and six patients were female. They had symptoms include diarrhea ( l o o % ) , nausea ( l o o % ) , vomiting ( l o o % ) , dysphagia(lOO%), dysphonia (loo%), dysarthria (loo%), symmetrical paralysis (loo%), bilateral ptosis(100%), perioral numbness (14%).0ne patient had associated with positive Tensilon test. Four patients required mechanical ventilation (57%). The onset of neurologic symptoms in these patients was three days after ingestion contaminated foods (range from 2 to 5 days). The sequence of signs and symptoms of foodborne botulism in order of onset as showed in Table 5. Two patients died from aspiration pneumonia and respiratory failure. Length of hospitalization was' 20 days (range from 9 to 40 days). All patients came from the same Tambon in Soprap District, Lampang. They had the same history of home-canned-preserved bamboo shoots ingestion bought from the same village market. TABLE 4. Differentiating Botulism from the Guillain-BarrC Syndrome. Variable Fever Guillain-Bw 6 Variant of Syndrome Guillain-Bmt5 Absent May be present May be present Dilated Normal Normal Botulism Motor Pupils or umeactive (50%) Ophthalmoplegia Present early Present late Present late Paralysis Descending Ascending Ascending DTRs Preseentlabsent Absent Absent Ataxia Absent Present Present Paresthesia Absent Present Present CSF protien Normal Elevated Elevated Adapted from Reference number 6. Abbreviations: DTRs, Deep tendon reflexes; CSF, cerebrospinal fluid. TABLE 5. Sequence of symptoms and signs of seven patients in order of onset after ingestion home-canned preserved bamboo shoots. T i e after ingestion signs and symptoms 6 - 24 hours Nausea, Vomiting, Diarrhea, Diz7.iness. 48 - 72 hours Mucus throat, Difficult swallowing food, Slurred speech, Bilateral ptosis 72 - 96 hours Progressive dysphagia Unsteady gait, Extreme weakness, Respiratory failure CLINICAL DIAGNOSIS Botulism LITERATURE REVIEW Botulism is a paralyzing disease caused by the potent neurotoxin of bacterium Clostridium botulinum. The name botulism is derived from the Latin word botulus, meaning sausage'"'. In the early part of the nineteenth century, Justinus Kerner of Germany reported cases of botulism from ingestion of improperly smoked sausage and found ingestion of an extract from the sausage reproduced clinical botulism. Kerner hypothesized that the toxic substance found in the sausages was "fatty acid"lll'12). Not until 1895, Professor Emile van Ermengen of Ghent identified a bacterial toxin to be the cause of botulism. Professor van Ermengen isolated an aerobic bacterium from the ham and reproduced the disease in laboratory animals by injection of a toxin produced by the bacteria. Clostridium botulinum is a spore-forming, obligate anaerobe whose natural habitat is soil, from which it can be isolated without undue difficulty. Botulinum toxin exists in 7 distinct antigenic types that have been assigned the letters A through G. The toxin types are defined by their absence of cross-neutralization (eg, anti-A antitoxin does not neutralize toxin type B-G). Human botulism is primarily caused by strains of C. botulinum that produce toxin types A,B,and E. Neurotoxigenic strains of C. baratii (which produce type F toxin) and C. butyricum (which produce type E toxin) also have been implicated in human botulism. Strains of C. botulinum that produce type C or D toxin for the most part cause botulism only in nonhuman species. Botulinum toxin is a simple dichain polypeptide that consists of 100-kd "heavy" chain joined by a single disulfide bond to a 50-kd "light" chain. The toxin's light chain is a zn2' containing endopeptidase that blocks acetylcholine-containing vesicles from fusing with the terminal membrane of the motor neuron, resulting in flaccid muscle paralysis'13' The lethal dose of botulinum toxin for humans is not known but can be estimated from primate studies. By extrapolation, the lethal amounts of crystalline type A toxin for 70-kg human would be approximately 0.09-0.15 p g intravenously or intramuscularly, 0.70-0.90 p g inhalationally, and 70 p g orally"3'. Four clinical forms of botulism occur in human: foodborne botulism; wound botulism; infant botulism (infant intestinal colonization); and rarely, adult infectious botulism (adult intestinal colonization). Clostridium botulinum. organisms cause food poisoning because the heat-resistant spores survive food preservation methods that kill nonsporulating organisms; the bacterial spore are resistant to heat and may survive the home-canning process at the temperatures below 120 o ~ ' 1 4 They '. subsequently produce a potent neurotoxin under anaerobic, low acid (pH > 4.6), and low solute conditions. Recently identified vehicles for foodborne botulism are showed in Table 6. The classic picture of botulism is that of a patient in whom acute, bilateral cranial neuropathies develop in association with symmetric descending weakness. The CDC suggests attention to the following cardinal features: (1) fever is absent (unless a complicating infection occurs), (2) the neurologic manifestations are symmetric, (3) the patient remains responsive, (4) the heart rate is normal or slow in the absence of hypotension, and (5). Sensory deficits do not occur (except for blurred ~ision)."~' Disease manifestations are similar regardless of botulinum toxin type. Some patients may be mildly affected, while others may be so paralyzed that they appear comatose and required months of ventilatory ~ u ~ ~ o r t ' ' ~ ' . Foodborne botulism usually develops between 12 and 36 hours after toxin ingestion. The patient initially complains of nausea and a dry mouth, and diarrhea may occur at this stage. Evidence of cranial nerve dysfunction most commonly starts with the eyes; parasympathetic involvemerit causes blurred vision from pupillary dilatation, or nerves 111, IV or VI may be involved. Pupillary reactions may remain abnormal for months after motor recovery. Nystagmus is occasionally noted, usually in type A disease. Lower cranial nerve dysfunction is manifested as dysphagia, dysarthria, and hypoglossal weakness. Weakness then spreads to upper extremities, the trunk, and the lower extremities. Respiratory dysfunction may result from either airway obstruction or diaphragmatic weakness. Patients who requiring mechanical ventilation, mean periods of 58 days (type A) and 26 days (type B) for ventilatory weaning. Recovery may not begin for up to 100 days. Botulinum toxin inhibition of acetylcholine release affects the parasympathetic and sympathetic systems, as well as the neuromuscular junction. TABLE 6. Vehicles Associated with foodborne Botulism. Home-canned or home-processed low-acid (pH > 4.6) foods. Vegetables Whale or seal products Fermented or salted fish products Meats Fish Relish Salsa Bamboo shoots Chili pepper Baked potatoes in .aluminum foil Garlic in oil Yogurt Sauteed onions kept under butter sauce Commercial cheese sauce Adapted from Reference number 16. Autonomic problems may include gastrointestinal dysfunction, alterations in resting heart rate, loss of responsiveness to hypotension or postural change, hypothermia, or urinary retention. Common signs and symptoms are showed in Table 7. The rapidity of onset and severity of botulism depend on the rate and amount of toxin absorption. Symptoms of foodborne botulism may begin as early as 2 hours or as long as 8 days after ingestion of toxin'13'. Typically, cases present 12 to 72 hours after the implicated'meal. In severe cases, extensive respiratory muscle paralysis leads to ventilatory failure have required ventilatory support for up to 7 month before return of muscular function, but ventilatory support is most commonly needed for 2 to 8 weeks. The toxin is readily inactivated by heat ( 2 8 5 ' ~for 5 ~ninutes)'~~'. Thus, foodborne botulism is always transmitted by foods that are not heated. Specific tests that helpful in diagnosing botulism are summarized in Table 8. Edrophonium (or ~ensilon)'~' test, occasionally used to differentiate myasthenia gravis from suspected botulism but in rare cases, early course of botulism, there is a limited improvement in strength, which is farless dramatic than occurs in myasthenia gravis'17'. Electromyographic pattern in botulism characterized by brief, small, abundant motor unit action potentials (BSAPs). Repetitive nerve stimulation at high rates (20 Hz or greater, as compared with the 4-Hz rate in the diagnosis of myasthenia gravis). Sample of serum, stool, vomitus, gastric contents and suspected foods should be sent for anaerobic culture (C. botulinum) and toxin assay. Respiratory compromise is the usual cause of death from botulism. To prevent or treat this complication, hospital admission of the patient and of all individuals exposed to a possible source is mandatory. Close monitoring of respiratory status by using parameters such as vital capacity, peak expiratory flow rate (PEFR), negative inspiratory force (NIF), pulse oximetry, and the presence or absence of gag reflex is essential to determine the need for intubation or tracheostomy as the patient begins to manifest signs of bulbar paralysis. Gastric decontamination should be initiated only for an asymptomatic person who has very recently ingested a known contaminated foods. Sorbitol is preferable to magnesium salts, which may potentially depress neuromuscular transmi~sion'~'. In human, the efficacy of the type specific antitoxin to type B strain toxin is unknown whereas the type-specific antitoxins to A and E q e probably beneficial. Antitoxin can prevent paralysis but does not affect already paralyzed muscles. The benefits must always weighed against the high incidence of anaphylaxis and serum sickness from the equine antitoxin. Botulinum antitoxins types A, B, AB (bivalent), E, ABE (trivalent), F are available. Although specific foods tend to correlate relatively well with botulinum type, trivalent antitoxin (7500 U type A, 5500 U type B, and 8500 U type E) should be administered. Guanidine which used to enhance acetylcholine release is no longer recommended to and intravenous immune globulin'22' have been given treat botulism6. steroid1', plasmapheresis,'19~20'21' to a small numbers of patients with ambiguous benefit. Further treatment strategies are being developed to include a F(ab)2 despeciated heptavalent immune globulin, human botulism immune globulin. SUGGESTION Botulism remains one of the rarest poisonings, while its etiologies have become increasing diverse. The most important aspect of foodborne botulism is prevention. One of many questions should be answer. Is the Thailand's health care system better for every Thai and foreign people? The best of medical center in the Southeast Asia will be only dream project or it can be reality. A valuable lesson from outbreak of foodborne botulism may be only one piece of jigsaws for the direction in sustainable development of Thai health care system in the future. TABLE 7. Commonly Reported Clinical Symptoms and Physical Findings in Botulism . Symptoms Gastrointestinal: Nausea Diarrhea (early) constipation (late) Abdominal cramps Vomiting Neurologic : Blurred vision Dysphagia Dry mouth Diplopia Dysarthria Arm weakness leg weakness Dyspnea Miscellaneous: Fatigue Sore throat Dizziness Physical findings Ptosis Tongue weakness Extraocular muscle weakness Hypoactive gag reflex. Pupils fixed or dilated Extremity weakness - Symmetric, Proximal to distal, Descending pattern Nystagmus Hypoactive deep-tendon reflexes Adapted from Reference number 9. TABLE 8. Tests that are useful in the diagnosis Botulism. Test ResuIt Consistent with botulism Initial test Brain imaging Normal Lumbar puncture Normal Electromyography Decreased amplitude of action in involved muscle group potential Rapid repetitive pattern Facilitation (increasing electromyography of action potential amplitude , 20-50 Hz) Confirmatory test Mouse inoculation test for toxin (serum, stool , food) Positive Stool culture for Clostridium botulinum. Positive Adapted from Reference number 9. REFERENCES 1. Ropper AH, Cros DP. Case records of Massachusetts General Hospital, case 39-1999. N Eng J Med 1999; 341: 1996-2003. 2. Devere R, Bradley WG. Polymyositis: its presentation, morbidity and mortality. Brain 1975; 98: 637-66. 3. Hayes MT, Soto 0 , Ruoff KL. Case records of Massachusetts General Hospital, case 22-1997. N Eng J Med 1997; 337: 184-190. 4. Teeraova W, Palumbo JN,Berman JG. Ocular findings in botulism type B. JAMA 1979; 241: 475-7. 5. Wongwatcharapaiboon P, Thaikruea L, Ungchusak K, et al. Foodborne Botulism Associated With home-canned bamboo shoots-Thailand, 1998. MMW'R Morb Mortal Wkly Rep 1998; 48 : 437-439. 6. Goldfrank LR, Flomenbuam. Botulism. In: Goldfrank LR. Goldfrank's Toxicologic Emergencies. New York Mc-Graw Hill; 2002: 1100-1111. 7. Newson-DavisJ. Lambert-Eaton myasthenic syndrome. Springer sernin Irnrnumopathol 1985; 8: 129-40. 8. Mordes JP, Waker WEC. Excess magnesium. Pharmacol Rev 1978; 29: 273-300. 9. Argov Z, Mastaglia FL.Disorders of neuromuscular transmission caused by drugs. N Eng J Med 1979; 301: 409-13. 10. Chutkow JG. Magnesium ions. In: Boulton AA, Baker GB, Walz W, eds. Neuromethods. Vol 9. The neuronal microenvironment. Clifton, N.J. Humana Press; 1988. 691-7 15. 11.Kessler KR,Benecke R. Botulinum toxin: from poison to remedy. Neurotoxicity 1997; 18: 761-770. 12. Erbguth FJ. Botulinum toxin, a historical note. Lancet 1998; 351: 1820. 13. Arnon SS, Schechter R, Inglesby TV, et al: Botulinum toxin as a Biological Weapon: Medical and Public Health Management. JAMA 2001; 285: 1059-1070. 14. Cherington M. Botulism: ten year experience. Arch Neurol 1974; 30: 432-437. 15. McCroskey LM, Hateway CL, Woodruff BA, et al. Type F botulism due to neurotoxigenic Clostridium baratii from an unknown source in an adult. J Clin Microbiol.1991; 29: 2618-2620. 16. Shapiro RL, Hatheway C, Swerdlow DL. Botulism in the United states: a clinical and epidemiologic review. Ann Intern Med 1998;129:221-228. 17. Cherington M. The clinical spectrum of botulism. Muscle Nerve 1998; 21: 701-707. 18. Cherington M, Schultz D. Effect of guanidine, germine, and steroids in a case of botulism. Clin Toxic 1977; 11: 19-25. 19. Paterson DL, King MA, Boyle RS, et al. Severe botulism after eating home-preserved asparagus. Med J Aust 1992; 157: 269-270. 20. Shapiro BE, Soto 0, Shafqat S,Blumenfeld H. Adult botulism. Muscle Nerve1997; 20: 100-102. 21. Rapoport S, Watkins PB. Descending paralysis resulting from occult wound botulism. Ann Neurol 1984; 16: 359-361. 22. Schmidt RD, Schmidt TW. Infant botulism: a case series and review literature. J Emerg Med 1992; 10: 713-718. 23. Hallett M. One man's poison: clinical applications of botulinum toxin. N Eng J Med 1999; 341: 118-120. 24. Edell TA, Sullivan CP Jr, Osborn KM, et al. Wound botulism associated with a positive tensilon test. West J Med 1983; 139: 218-219. 25. Cherington M. Botulism. In: Bashar Ratriji. et al. Neuromusclar disorders in clinical practice. New York: Butterworth-Heinemann Publication 2002 :942-952. 26. Critchley EMR. Botulism and Gulf War syndrome. Lancet 1996; 347: 1561.