Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Spectrum disorder wikipedia , lookup
Child psychopathology wikipedia , lookup
Asperger syndrome wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
History of mental disorders wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Alcohol withdrawal syndrome wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
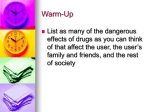
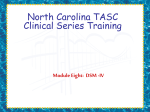
RESEARCH REPORT doi:10.1111/j.1360-0443.2010.02951.x Continuous, categorical and mixture models of DSM-IV alcohol and cannabis use disorders in the Australian community add_2951 1246..1253 Andrew J. Baillie1 & Maree Teesson2 Psychology Department, Macquarie University, Sydney, NSW, Australia1 and National Drug and Alcohol Research Centre, University of New South Wales, Sydney, NSW, Australia2 ABSTRACT Aims To apply item response mixture modelling (IRMM) to investigate the viability of the dimensional and categorical approaches to conceptualizing alcohol and cannabis use disorders. Design A cross-sectional survey assessing substance use and DSM-IV substance use disorders. Setting and participants A household survey of a nationally representative sample of 10 641 Australia adults (aged 18 years or older). Measurements Trained survey interviewers administered a structured interview based on the Composite International Diagnostic Interview (CIDI). Findings Of the 10 641 Australian adults interviewed, 7746 had drunk alcohol in the past 12 months and 722 had used cannabis. There was no improvement in fit for categorical latent class nor mixture models combining continuous and categorical parameters compared to continuous factor analysis models. The results indicated that both alcohol and cannabis problems can be considered as dimensional, with those with the disorder arrayed along a dimension of severity. Conclusions A single factor accounts for more variance in the DSM-IV alcohol and cannabis use criteria than latent class or mixture models, so the disorders can be explained most effectively by a dimensional score. Keywords Alcohol, cannabis, diagnosis, DSM-IV. Correspondence to: Andrew Baillie, Macquarie University, Sydney, NSW 2109, Australia. E-mail: [email protected] Submitted 2 June 2009; initial review completed 13 July 2009; final version accepted 6 January 2010 INTRODUCTION Alcohol is the most widely used licit drug and cannabis is the most widely used illicit drug in developed countries [1,2], and each has a significant impact on health in the general population [3–5]. Both alcohol and cannabis users in the general population frequently endorse criteria for the most common drug phenotypes, abuse and dependence [3–10]. Risks associated with alcohol use have long been known and the risks of cannabis use are being recognized increasingly. The most common description of the phenotype of these consequences is DSM-IV alcohol and cannabis use disorders, yet it is becoming increasing clear that the validity and utility of the abuse and dependence syndrome (and its implementation in widely used diagnostic schemes) requires attention [11]. The dependence syndrome was first formulated by Edwards & Gross [12] and Edwards et al. [13], as a number of psychological and physiological factors asso- ciated with diminished control over alcohol use. In a later publication Edwards [14] referred to the ‘bi-axial concept’, where dependence as described above constitutes one axis of the syndrome and alcohol-related problems forms the other. While the bi-axial concept has clinical appeal, evidence from large population and clinical samples has called into question this distinction and the use of categorical descriptions generally providing evidence for the conceptualization of problems along a dimension or continuum of severity. In the current paper we apply item response mixture modelling (IRMM) to investigate the viability of the dimensional and categorical approaches to conceptualizing alcohol and cannabis problems. The aims of this paper are to compare continuous, categorical and mixture models for the structure of the DSM-IV [15] criteria in a large population survey using item response mixture modelling. This is conducted on the most commonly used licit and illicit drugs, alcohol © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 Mixture models and cannabis. Item response mixture modelling is a new hybrid latent variable model which combines the features of categorical and dimensional analyses used in the conventional techniques of latent class and factor analysis. It has been argued that hybrid models are more suitable for understanding substance use dependence and fit the data better than conventional models of factor analysis and latent class analysis (LCA) [16]. Muthén et al. [16–18] have demonstrated its superiority in nicotine dependence and alcohol use disorders, but it is untested as yet in the most commonly used illicit drugs. If superior, these hybrid models may be useful in improving our conceptualization of alcohol and cannabis problems. The focus of this paper is therefore to explore whether categorical or latent class models, dimensional or factor analysis/item response theory models or the new hybrid models are superior in describing problems associated with alcohol and cannabis use. Both the relationship between the abuse and dependence criteria and the appropriateness of the criteria to alcohol and cannabis use disorders are examined with each measurement model. The DSM-IV specifies 11 criteria for substance use disorders, equally applicable to all classes of psychoactive substances including alcohol, cocaine, opiates, cannabis, sedatives, stimulants and hallucinogens. Dependence is measured by seven criteria, at least three of which must be endorsed for a diagnosis to be reached. Abuse is measured by four additional criteria, and a diagnosis is made if at least one criterion is endorsed (and a diagnosis of dependence is absent). Criteria for each diagnostic outcome are assumed to have equal weighting. The application of statistical modelling to substance use criteria is increasing. Most investigations of this type have focused upon clinical populations (with associated range restriction) and employed a range of factor analytical techniques, yielding inconsistent results. In the alcohol literature some studies have found evidence for two separate, although related factors [19,20], while others have identified single dimensions [21]. The two studies to assess the current DSM-IV criteria in population-based samples supported a one-factor solution [22,23]. The position of the items along this latent dimension differed considerably, with abuse indicating severity in the Australian analysis [22] and abuse items being spread more widely across the continuum in the US analysis [23] In terms of cannabis, some studies have found evidence for the coherence of cannabis dependence [10,24–27], while others have identified multiple dimensions [28] For example, Kosten et al. [28] suggested a three-factor model for disorders of cannabis use, based on profiles of endorsement of DSM-III-R criteria for substance use disorders in a clinical population. 1247 The majority of these studies have restricted their examination to the structure of the cannabis dependence criteria only. Teesson et al. [3], Lynskey et al. [4] and Compton et al. [5] examined the structure of both DSM-IV cannabis abuse and dependence in population samples and found that the one-factor solution was the most parsimonious. Langenbucher et al. [29] found similar results in a mixed clinical and general population sample. The WHO cross-national study by Nelson et al. [27] tested the seven DSM-IV dependence and four abuse criteria for alcohol and cannabis using confirmatory factor analysis (CFA) using community and treatment centre samples. With this sample they found a two-factor solution no better than the one-factor solution; but when they ‘trimmed’ the data of extreme respondents (those who responded ‘no’ to all criteria or ‘yes’ to 10 or 11 criteria) they found the two-factor solution to be superior. This result implies that symptoms behave differently at different levels of severity and supports the exploration of hybrid models with both dimensional and categorical conceptualizations. The dimensionality of the substance use criteria is not entirely clear. Our work to date has supported unidimensionality; however, it is recognized that categories are useful in the clinical response to disorders [19]. In 2006, Muthén [17] raised the possibility that both dimensional and continuous models may fit diagnostic criteria. He proposed the application of new hybrid latent variable models for phenotypical analyses. He tested these models on tobacco dependence criteria and alcohol use disorder criteria in males and found that the hybrid latent models fitted the data more effectively than conventional models of factor analysis (IRT) and LCA. The current paper extends our existing work with Australian general population data [3,22] to examine these hybrid models. Based on previous work [16–18] we plan to compare the fit of one- and two-factor models which assess substance use disorders as a single dimension or as separate dependence and abuse dimensions, as two, three, four, five or six latent classes in which individuals are conceptualized as forming separate classes or categories, and hybrid models with both categorical and dimensional entities. Following on from Nelson et al. [27], who removed from analysis those individuals who endorsed no criteria or all criteria from some analyses, we examine one- and two-factor models in conjuction with a zero class accounting for those who endorsed no criteria. By comparing the extent to which these models explain the observed data on the same fit indices, this paper provides an empirical test of the whether the DSM-IV criteria behave as one or more dimensions, categories or a mixture of the two. © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 1248 Andrew J. Baillie & Maree Teesson We use data from the Australian National Survey of Mental Health and Wellbeing (NSMHWB) [30], a study of a large and representative sample of the general population. A detailed description of this study is provided elsewhere [30]. METHODS The NSMHWB was a multi-stage sample of private dwellings across Australia. Dwellings were selected using random stratified multi-stage area sampling, so that each person had a known chance of participation. One person aged at least 18 years was selected randomly (next birthday) from each dwelling and asked to participate. Approximately 13 600 private dwellings were approached, with a final sample size of 10 641 people giving a response rate of 78%. Mental disorders were assessed by a modified version of the CIDI [30], which yielded diagnoses of both ICD-10 and DSM-IV disorders. The CIDI has been used in a range of epidemiological studies, and has been shown to be a reliable and valid survey instrument; details of this have been provided elsewhere [30] based upon studies using an earlier version of the CIDI. The substance use disorders section has changed very little between this version and that used in the NSMHWB. Interviews were conducted face to face with trained interviewers and questioning was restricted to symptoms in the last 12 months. Alcohol abuse and dependence were assessed in all people who had consumed at least 12 alcoholic drinks in the past 12 months (n = 7746). Cannabis abuse and dependence criteria were assessed in all people who had used cannabis more than five times in the past 12 months (n = 722). Statistical methods Although the NSMHWB data have been obtained by complex sampling procedures, the factor analysis methods used in this paper assumed simple random sampling. Muthén et al. [19] argue that this simplified method is acceptable because multivariate methods are generally less sensitive than univariate methods to complex sampling features. All analyses in this paper were carried out using maximum-likelihood estimation in the Mplus program [31,32]. Three models are tested on the data; one and two CFA, two to six LCA and the new hybrid item response or factor mixture model. Muthén & Asparouhov [16] provide a description of the three models. Maximum likelihood estimation was used to allow comparison of the fit of different models by comparison of the –2log-likelihood estimates. RESULTS Alcohol use disorders Indices of the fit of the different models proposed to underlie DSM-IV alcohol use disorders are shown in Table 1. CFA/item response theory models using maximum likelihood estimation are reported first. Two separate abuse and dependence factors gave a significantly better fit (deviance c2 = 5.35, df = 1, P < 0.05) than a single substance use factor. The correlation between these two latent factors was very high (0.954). Latent class models were examined next. As can be seen in Table 1, the best-fitting LCA employed three latent classes [log-likelihood = 11 834.084, parameters = 35, Bayesian information criteria (BIC) = 23 981.611] but higher log-likelihood and BIC indicate a worse fit while using a greater number of parameters than the CFA models. Figure 1 shows the profile of criteria for each of the three latent classes in the best-fitting LCA model. The estimated proportion falling into each of these three classes were class 1, 10.64% (n = 824); class 2, 2.07% (n = 160); and class 3, 87.29% (n = 6762). In comparison, the existing DSM-IV algorithm would assign a diagnosis of alcohol dependence to 5.6% of drinkers and alcohol abuse to 2.6% of drinkers [19]. Class 1 can be taken to represent dependent drinkers with a lower threshold for diagnosis than expressed in DSM-IV and class 2 reflects a small proportion of drinkers who are likely to experience criteria LARGER and CUTDOWN and TOLERANCE to a lesser extent, but not other criteria. Class 3 represents a zero class. The lines representing the profiles for classes 1 and 2 might be interpreted as parallel or indicating that these two profiles may differ on severity alone. Notably, absent is a latent class with high probability of endorsement for the abuse criteria. Consistent with our earlier modelling using item response theory [21], criteria GIVE-UP and TIME SPENT discriminated between classes 1 and 2, as did WITHDRAWAL, CONTINUE and, to a lesser extent, the abuse criteria. The first item response or factor mixture model (model 8 in Table 1) examines a single factor with a zero class. This model proposes that (i) there are people who drink alcohol but report none of the 11 criteria (the zero class) and (ii) that the patterns of criteria reported by the remainder of drinkers are accounted for by a single dimension. Model 9 (see Table 1) estimates a zero class and two related but separable dependence and abuse factors. This model follows from Nelson et al. [27], who concluded that there were separate abuse and dependence dimensions when they removed those who endorsed all or none of the 11 criteria. Higher –2log-likelihood and BIC indicate a worse fit than the two-factor CFA/IRT model and worse than the three-class LCA. © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 4855.682 4875.443 23 26 The procedure for fitting models to the 11 DSM-IV cannabis use disorder criteria was the same as above. As can be seen in Table 1, a single dimension underlying all 11 DSM-IV cannabis use disorder criteria was not a significantly worse fit to the data based on comparison of –2log-likelihoods (deviance c2 = 0.010, d f = 1, P = ns) and showed lower BIC than separate abuse and dependence factors. Of the latent class models fitted, model 3 with two latent classes had the lowest BIC. However, this model showed a poorer fit to the data than the best CFA model a single factor. Figure 2 shows the probability of endorsing each of the criteria for the two latent classes in the best-fitting latent class model. The second class, which accounted for 547 (75.76%) of the 722 cannabis users, approximates a zero class with an approximately 20% chance of endorsing the CUTDOWN criteria. In contrast, the first latent class containing 175 (24.24%) of the 722 cannabis users shows much greater endorsement of the TOLERANCE, WITHDRAWAL, LARGER and CUTDOWN criteria. Application of the DSM-IV algorithm gives a prevalence of cannabis dependence as 20.9% [standard error (SE) = 2.2], so this class can be thought of as reflecting a dependence-like syndrome with a lower threshold. Adding a zero class to a single dimension underlying the 11 criteria (model 8) showed no significant improvement in –2log-likelihood [deviance c2 = 1.07, df = 1, P = not significant (NS)] and an increase in the BIC, indicating a worsening of fit to the data compared to the single-factor CFA model. As with drinkers above, there was no improvement in fit for a two-factor model with a zero class. -2352.148 -2352.155 DISCUSSION BIC: Bayesian information criteria. 23 26 -11 814.226 -12 088.402 1249 Cannabis use disorders 23 834.416 24 409.631 4910.052 4923.976 4978.043 5018.716 5086.560 23 35 47 59 71 -2379.333 -2346.802 -2334.334 -2315.188 -2309.618 23 35 47 59 71 -12 200.049 -11 834.094 -11 817.335 -11 799.682 -11 760.249 24 606.062 23 981.611 24 055.551 24 127.705 24 156.297 4851.244 4857.807 22 23 -2353.220 -2353.210 23 835.681 23 833.936 22 23 -11 819.336 -11 813.986 Continuous confirmatory factor analysis/item response theory models 1. One substance use disorder factor 2. Two separate abuse and dependence factors Categorical latent class models 3. Two latent classes 4. Three latent classes 5. Four latent classes 6. Five latent classes 7. Six latent classes Item response or factor mixture models 8. One factor with a zero class 9. Two factors with a zero class Log-likelihood Log-likelihood Model Table 1 Model fit results. Alcohol (n = 7746) No. of free parameters BIC Cannabis (n = 722) No. of free parameters BIC Mixture models The purpose of these analyses was to compare explicitly categorical, continuous and new mixture models of DSM-IV alcohol and cannabis criteria in a large representative epidemiological sample. Single- or two-factor (highly correlated) models were found to be the bestfitting models for both alcohol and cannabis use disorders. While two-factor models showed a better fit, the correlation between the two factors was so high that a single-factor model is the most parsimonious solution. Hybrid item response mixture models incorporating both dimensional and categorical conceptions of substance use disorders do not provide substantial gains in fit over straight categorical or straight dimensional conceptions of alcohol and cannabis problems. The current results are somewhat inconsistent with previous analyses undertaken on tobacco and alcohol use disorders [16–18], which report that these item response © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 1250 Andrew J. Baillie & Maree Teesson Criterion Profiles from Latent Class Models of Drinkers 1.2 Criterion Probability 1 0.8 Latent Class 1 Latent Class 2 Latent Class 3 0.6 0.4 0.2 Social 5 Legal TImeSp 4 Hazard Cutdown 3 Major Role Larger 2 Coninue Withdrawal 1 Give up Tolerance 0 6 7 8 9 10 11 DSM-IV Criteria Figure 1 Criterion profiles for a three latent class model of drinkers Criterion Profiles from Latent Class Models of Cannabis Users 0.9 0.8 Criterion Probability 0.7 0.6 0.5 LC(1) LC(2) 0.4 0.3 0.2 0.1 L SO C IA _ AL G AZ H LE AR D LE M AJ R U TN N C IV G E EU P P ES TI M N W TD C U G ER R LA D TH W TL R R W N C L E 0 DSM-IV Criteria Figure 2 Criterion profile for a two latent class model of cannabis users mixture models give a richer account of obtained data for tobacco dependence and alcohol use disorders. Their results suggest that these new methods, which allow joint testing of categorical and continuous models of the underlying disorder, are a closer match to the theoretical descriptions of substance dependence. They argue that the hybrid models may provide a richer description of the disorders. The current study did not find any substantial gains in fit over straight dimensional conceptualizations. The analyses reported here are consistent with previous analyses we have reported on this data set [22]. In this analysis of the 11 DSM-IV alcohol use disorder criteria we found that a two-factor model gave the best fit to the data. The differences between the one- and two-factor © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 Mixture models models were small in both analyses and the correlation between the two factors in a two-factor model were very high (0.95). Thus, the one-factor model represents the most parsimonious solution. A model containing two highly correlated factors might seem to support the notion that substance abuse represents the social and role impairment that develops before symptoms of neuroadaptation and dependence. However, in previous analyses we have shown that the abuse criteria generally are markers of a more severe state of substance use disorder. We would argue that the finding that abuse criteria indicate a more severe state, and that there is only a relatively small number of people who meet criteria for abuse and not dependence, means that the abuse diagnosis is a residual [33]. These results are contrary to findings reported by Langenbucher & Chung [34], who argue that the abuse criteria reflect an early stage in the development of substance use disorders in a clinical sample; however, it may be that there is something about the abuse criteria that brings people into contact with treatment services, so that clinical samples give different results. Thus it is critical to examine the substance use disorder construct in population samples to reduce such potentially confounding effects. The original formulation of the dependence syndrome [12,13] was as a number of psychological and physiological factors associated with diminished control over alcohol use. Later, this was conceptualized further as ‘bi-axial’ [14], where dependence as described above constitutes one axis of the syndrome and alcohol-related problems formed the other, and this has influenced conceptualizations in DSM-IV. While these concepts have clinical and intuitive appeal, their examination using IRMM does not support such categorical conceptualizations in the current paper. The implications of this paper for DSM-V is that substance use disorders, as experienced in the general community, are better conceptualized as unidimensional, with criteria indicating severity. Importantly, our findings are consistent across both alcohol and cannabis use disorders. A single factor performs best in accounting for variance in the DSM-IV alcohol and cannabis use criteria. This may mean that a single dimension is sufficient to describe the most common presentations with these disorders in the community. An alternative is that the DSM-IV criteria do not encompass all the essential features of substance use disorders. The DSM-IV criteria might represent a premature narrowing of the construct. Some work on the latent structure of alcohol problems by Chick [35] found support for more than one factor in a set of 21 symptoms based on the Edwards & Gross [12] dependence syndrome assessed in a clinical sample of men attending an alcoholism treatment unit. It may be that more than one factor emerges from clinical samples, 1251 because most criteria are met leading to ceiling effects and a restriction in the covariation of symptoms. Future research should examine the possibility that multiple-factor models of substance use disorders might be accommodated under a single higher-order factor. Having demonstrated superior fit and parsimony for a single latent variable to account for DSM-IV alcohol and cannabis use disorders, further research could examine the incremental validity [36] of assessments in addition to a severity score based on the current criteria. That is, other constructs associated with additional clinical information over and above those are accounted for by a severity score based on the DSM-IV criteria. It may also be instructive to examine diagnostic orphans, those whose patterns of symptoms are at odds with the prevailing single-factor model. This paper relies upon a structured diagnostic interview to derive symptoms and diagnoses. Although this is common practice in psychiatric epidemiology, it is likely that such methods do not capture the breadth of each concept under study. For example, the DSM conveys the notion that for the diagnosis to be given there must be significant clinical impairment or distress. This may not be captured well in structured diagnostic interviews. However, the current findings are consistent with previous studies examining the performance of DSM criteria in clinical samples [27,29,37]. The hybrid item-response/factor-mixture models used in the present study following the recommendations of Muthén [16,17] allow for the comparison of continuous, categorical and combined or ‘mixture’ models of substance use disorders and psychopathology more generally [38]. In this paper these new models do not provide a better account of the symptoms of substance use disorders in the community than earlier continuous models. However, it is important to continue to refine further the diagnostic criteria and models of these criteria to define phenotypes more tightly for genetic analyses and to examine treatment responses more closely. Declarations of interest None. Acknowledgement The NSMHWB was designed, developed and conducted with funding from the Mental Health Branch of the Australian Commonwealth Department of Health and Family Services. Development and testing of the computerized survey instrument was undertaken by Gavin Andrews, Lorna Peters and other staff at the Clinical Research Unit for Anxiety Disorders, and the WHO Collaborating Centre in Mental Health at St Vincent’s Hospital, Sydney. The design of the survey was overseen and © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 1252 Andrew J. Baillie & Maree Teesson approved by the Technical Advisory Group comprising: Professors A. Scott Henderson (Chair), Gavin Andrews, Wayne Hall, Helen Herman, Assen Jablensky and Bob Kosky. Survey fieldwork and implementation and the enumeration, compilation and initial analyses of the data were undertaken by the Australian Bureau of Statistics. References 1. World Health Organisation (WHO). Global Status Report on Alcohol 2004, 2nd edn. Geneva, Switzerland: WHO; 2005. 2. Hall W., Johnston L., Donnelly N. Epidemiology of cannabis use and its consequences. In: Kalant H., Corrigall W. A., Hall W., Smart R., editors. The Health Effects of Cannabis, Toronto, ON: Centre for Addiction and Mental Health; 1999, p. 69–125. 3. Teesson M., Lynskey M., Manor B., Baillie A. The structure of DSM-IV cannabis use disorders in the community. Drug Alcohol Depend 2002; 68: 255–62. 4. Lynskey M. T., Agrawal A. Psychometric properties of DSM assessments of illicit drug abuse and dependence: results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Psychol Med 2007; 9: 1345– 55. 5. Compton W. M., Saha T. D., Conway K. P., Grant B. F. The role of cannabis use within a dimensional approach to cannabis use disorders. Drug Alcohol Depend 2009; 100: 221–7. 6. Anthony J. C., Warner L. A., Kessler R. C. Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: basic findings from the National Comorbidity Survey. Exp Clin Psychopharmacol 1994; 2: 244–68. 7. Compton W. M., Grant B. F., Colliver J. D., Glantz M. D., Stinson F. S. Prevalence of marijuana use disorders in the United States: 1991–1992 and 2001–2002. JAMA 2004; 291: 2114–21. 8. Stinson F. S., Grant B. F., Dawson D. A., Ruan W. J., Huang B., Saha T. Comorbidity between DSM-IV alcohol and specific drug use disorders in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend 2005; 80: 105–16. 9. Warner L. A., Kessler R. C., Hughes M., Anthony J. C., Nelson C. B. Prevalence and correlates of drug use and dependence in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1995; 52: 219– 29. 10. Swift W., Hall W., Teesson M. Characteristics of DSM-IV and ICD-10 cannabis dependence among Australian adults: results from the National Survey of Mental Health and Wellbeing. Drug Alcohol Depend 2001; 63: 147–53. 11. Hasin D. S., Liu X., Alderson D., Grant B. F. DSM-IV alcohol dependence: a categorical or dimensional phenotype? Psychol Med 2006; 36: 1695–705. 12. Edwards G., Gross M. Alcohol dependence: provisional description of a clinical syndrome. BMJ 1976; 1: 1058–61. 13. Edwards G., Arif A., Hodgson R. Nomenclature and classification of drug and alcohol related problems: a WHO memorandum. Bull World Health Organ 1981; 50: 225–42. 14. Edwards G. The alcohol dependence syndrome: a concept as stimulus to enquiry. Br J Addict 1986; 81: 171–83. 15. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders DSM-IV, 4th edn. Washington, DC: APA; 1994. 16. Muthén B., Asparouhov T. Item response mixture modeling: application to tobacco dependence criteria. Addict Behav 2006; 31: 1050–66. 17. Muthén B. Should substance use disorders be considered as categorical or dimensional? Addiction 2006; 101: 6–16. 18. Kuo P. H., Aggen S. H., Prescott C. A., Kendler K. S., Neale M. C. Using a factor mixture modeling approach in alcohol dependence in a general population sample. Drug Alcohol Depend 2008; 98: 105–14. 19. Muthén B. O., Grant B. F., Hasin D. The dimensionality of alcohol abuse and dependence: factor analysis of DSM-III-R and proposed DSM-IV criteria in the 1988 National Health Interview Survey. Addiction 1993; 88: 1079–90. 20. Harford T. C., Muthén B. O. The dimensionality of alcohol abuse and dependence: a multivariate analysis of DSM-IV symptom items in the National Longitudinal Survey of Youth. J Stud Alcohol 2001; 62: 150–7. 21. Hasin D. S., Muthén B., Wisnicki K. S., Grant B. Validity of the bi-axial dependence concept: a test in the US general population. Addiction 1994; 89: 573–9. 22. Proudfoot H., Baillie A. J., Teesson M. The structure of alcohol dependence in the community. Drug Alcohol Depend 2006; 81: 21–6. 23. Saha T., Chou S. P., Grant B. F. Toward an alcohol use disorder continuum using item response theory: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychol Med 2006; 36: 931–41. 24. Hasin D. S., Grant B. F., Harford T. C., Endicott J. The drug dependence syndrome and related disabilities. Br J Addict 1998; 83: 45–55. 25. Morgenstern J., Langenbucher J. W., Labouvie E. W. The generalizability of the dependence syndrome across substances: an examination of some properties of the proposed DSM-IV dependence criteria. Addiction 1994; 89: 1105–13. 26. Feingold A., Rounsaville B. J. Construct validity of the dependence syndrome as measure by DSM-IV for different psychoactive substances. Addiction 1995; 90: 1661–9. 27. Nelson C. B., Rehm J., Ustin T. B., Grant B., Chatterji S. Factor structures for DSM-IV substance disorder criteria endorsed by alcohol, cannabis, cocaine and opiate users: results from the WHO reliability and validity study. Addiction 1999; 94: 843–55. 28. Kosten T. R., Rounsaville B. J., Babor T. F., Spitzer R. L., Williams J. B. Substance-use disorders in DSM-III-R. Evidence for the dependence syndrome across different psychoactive substances. Br J Psychiatry 1987; 151: 834–43. 29. Langenbucher J., Martin C. S., Labouvie E., Sanjuan P. M., Bavly L., Pollock N. K. Toward the DSM-V: the withdrawalgate model versus the DSM-IV in the diagnosis of alcohol abuse and dependence. J Consult Clin Psychol 2000; 68: 799–809. 30. Teesson M., Hall W., Lynskey M., Degenhardt L. Alcoholand drug-use disorders in Australia: implications of the National Survey of Mental Health and Wellbeing. Aust NZ J Psychiatry 2000; 3: 206–13. 31. Muthén B. O., Muthén L. K. Mplus: Statistical Analysis with Latent Variables. User’s Guide (V2.01). Los Angeles, CA: Muthén & Muthén; 2001. 32. Muthén B., Muthén L. MPlus. Available at http://www. statmodel.com (accessed 11 March 2010). Archived at http://www.webcitation.org.5o9LJhpBS (11 March 2010). 33. Hasin D. Classification of alcohol use disorders. Alcohol Res Health 2003; 27: 5–17. © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 Mixture models 34. Langenbucher J. W., Chung T. Onset and staging of DSM-IV alcohol dependence using mean age and survival-hazard methods. J Abnorm Psychol 1995; 104: 346–54. 35. Chick J. Is there a unidimensional alcohol dependence syndrome? Br J Addict 1980; 75: 265–80. 36. Garb H. N. Incremental validity and the assessment of psychopathology in adults. Psychol Assess 2003; 15: 508–20. 37. Wu L. T., Pan J. J., Blazer D., Tai B., Stitzer M. L., Brooner 1253 R. K. et al. An item response theory modeling of alcohol and marijuana dependence: a national drug abuse treatment clinical trials network study. J Stud Alcohol Drugs 2009; 70: 414–42. 38. Krueger R. F., Markon K. E. Reinterpreting comorbidity: a model-based approach to understanding and classifying psychopathology. Annu Rev Clin Psychol 2006; 2: 111– 33. © 2010 The Authors. Journal compilation © 2010 Society for the Study of Addiction Addiction, 105, 1246–1253 This document is a scanned copy of a printed document. No warranty is given about the accuracy of the copy. Users should refer to the original published version of the material.