Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
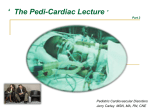
Q Fever Endocarditis in Queensland H. G. WILSON, M.D., F.R.A.C.P., G. H. NEILSON, M.D., F.R.A.C.P., E. G. GALEA, M.D., G. STAFFORD, M.D., F.R.A.C.S., AND M. F. O'BRIEN, M.D., F.R.A.CS. F.R.A.C.P., Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 SUMMARY Thirteen patients with proven Q fever endocarditis and three additional patients with probable endocarditis are reviewed. The most helpful diagnostic test is the demonstration of a high complement fixing antibody titre to Phase I antigen of Coxiella burneti. The macroscopic pathology of the aortic valve is described and includes aneurysmal pockets in the aortic wall and valve annulus which are demonstrable angiographically. Evidence is presented that the infection may be controlled by prolonged tetracycline therapy and that this is accompanied by a falling antibody titre to Phase 1 antigen. Valve replacement is undertaken only for symptomatic and hemodynamic indications. The combined tetracycline therapy and valve replacement have produced a fall in titres with eradication of infection and palliation of the cardiac disability in all patients followed for long periods. Q FEVER was originally described by Derrick in 1937.1 The diagnosis is made by an increasing complement fixing antibody titre to the antigens of Coxiella burneti (C. burneti). These antibody titres are measured against Phase I and Phase 2 antigens. During the acute infection the rising antibody titre is to the Phase 2 antigen, whereas elevated antibody titre to Phase 1 antigen suggests past persistent infection;2 high titres are found in chronic infections, including Q fever endocarditis.3 The ultimate diagnosis of Q fever endocarditis is based on identification of the organism in the affected valve tissue removed at autopsy or operation. Laboratory animals inoculated with such tissue demonstrate a rising antibody titre and C. burneti is present in their tissues. Cases of Q fever must be reported to the Health Department in Queensland. All diagnostic blood tests are performed in the State Health Laboratory so that it is possible to follow all proven cases. This communication surveys Q fever endocarditis in Queensland from 1959 to 1974. fever, rigors, malaise, splenomegaly, painful emboli in hands and feet, and heart failure one year earlier. Three months before admission he had a transient left hemiparesis. Although a meat worker for 14 years, he had no definite history of Q fever. On examination he had aortic stenosis and incompetence (AS, Al) and a mycotic aneurysm of the right posterior tibial artery (fig. 1). His hemoglobin was 11.4 g/100 ml, C. reactive protein positive, serum protein 8.1 g/100 ml with 3.27 g/100 ml gamma globulin and complement fixing antibody titres greater than 1:512 to Phase 1 antigen. He was given a prolonged course of tetracycline. On March 4, 1969 the aortic valve was removed and a calf heterograft valve was inserted. The fused bicuspid valve was disrupted around the whole of the attachment of the noncoronary leaflet and the adjacent anterior commissure, the valve tissue being like a bowstring across the aortic orifice. Some necrotic tissue was present with a large anterior commissure aneurysm (3.5 X 2.5 cm) projecting into the ventricular septum. C. burneti was not found in the smears, but grew in inoculated mice. Repeat angiogram ten days postoperatively showed the posterior tibial aneurysm had disappeared (fig. 2). The heterograft valve later developed moderate incompetence and was replaced by a ring-supported fascia lata autograft in 1971. At reoperation no macroscopic or microscopic evidence of persisting Q fever infection was present. Incompetence was due to a tear in one of the heterograft valve cusps. The aneurysm had completely healed. The patient is now asymptomatic and the valve remains competent. It is considered that this man has been cured of Q fever endocarditis. Figure 3 shows the changing C.F. antibody titre to Phase I antigen. Clinical History Twenty-one patients with Q fever and cardiac murmurs were reviewed. Thirteen patients had proven Q fever endocarditis, the organism being identified in the laboratory. Three additional patients had probable endocarditis with symptoms and signs of infective endocarditis, negative blood cultures, and high or rising titres to Phase 1 antigen. Of these, one patient was considered to have been cured prior to his death from uremia (case 10) and one died but no autopsy was done (case 5). The third (case 6) had five years of tetracycline therapy with apparent clinical cure prior to operation for residual valve damage. Only the sixteen patients with Q fever endocarditis are reported in this paper. The clinical features of these sixteen patients are summarized in table 1, while the important laboratory data are shown in table 2. Brief accounts of the operative findings and the clinical course of these patients are presented in table 3. Two illustrative case histories follow in more detail. Case 10 W.K., 64 years old, originally a butcher in Scotland, was first seen in 1963. He was admitted because of pain and swelling of the right calf and was found to have finger clubbing, anemia and Al. The hemoglobin was 8.7 g/100 ml, erythrocyte sedimentation rate (ESR) 82 mm/hr, urine showed occasional red cells and gamma globulin was increased. The C.F. antibody titre to Phase 1 antigen was 1:1024. He was treated with pyrrolidino-methyl-tetracycline (Reverin) 275 mg b.d. and steroids for 52 days and improved. By 1965 the C.F. antibody titre to Phase 1 antigen Case 3 a J.D., 44 years old, a meat worker, presented in 1969 with five year history of a heart murmur. He had developed From the Cardiac Unit, The Prince Charles Hospital and Princess Alexandra Hospital, Brisbane, Australia. Address for reprints: G. H. Neilson, M.D., The Prince Charles Hospital, Rode Road, Chermside, 4032, Brisbane, Australia. Received June 5, 1975; revision accepted for publication November 18, 1975. 680 Q FEVER ENDOCARDITIS/Wilson et al. 681 TABLE 1. Stn marcp of Clnical J)ata No Occopation 1. Meat worker Age af, rese rii a t 1l(1 .31 Valve lesICion AS) AI 5. Farmier A-leat woikeri Flar han( Farmier' 70 AS, Al AS. Al Al AS, Al 6. Stdes mnaiager 27 Al. Ml 2. 3. 4. 59 44 t) Undferrling etiology Important cliniea! feat J)iration of Q fcevi to ires crldocarditis Cotgellit al bicitspid valve Fever,, aniginia, (dy spia, Uiikitowit Il-hennaltic Congeiital Iliennmatic RLhIenIrnatic Fever', angina, dy(spnlea FeveI, spleinomegaly Fatigue, dysplea Arrh-llythmia, dyspaet, Uniknlowin 2 yr 1 yr 11heuLmniatic Palpitatiolns,ldtyspea IUtikniowii. Bacterial finiger clul)bing 14 yr enidoc arditsisresumed AS MS Conigeniital lRheumatie Ilemiparesis, dy,sIpnea Fever, tiredness, Salesmani 8 Al UIiknownt lIt (her 64 Al ? Conigenital dyspiea Fever, tiredness, hepatosplenomegaly Veniotis thrombosis leg, Mltxtte Meat inlspecto-r} 9. 10. pr'eVioLnly years ;) 50 40 7. S. 8 yr 7 vy 11 yr Unknown finiger clubbinig Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 l. Gardenier Rheumatic Stable hand 58 20 AS, Al 12. Al 1Rheumatic 13. R ailway porter 47 Al Congenital 14. Farmer 15. 16. Farmer (hriazier 49 49 48 AS Al Al AI Congenital Congenital C(ongenital 1)yspnea Unkrnown Uinknown Clubbing, subungual hemorrhages, dyspiiea l)yspnea, clubbing 1)yspnea, hemiparesis Acutte polmonary edemiia, 15 yr Dyspnea, increasinig cardiormegaly Uniknowni Uniknowrwn 2(0 yr splenoomegaly had fallen to 1:64 and to 1:32 by 1966 (see fig. 3). In 1965 he developed heart failure and in 1966 died from uremia. At autopsy he was found to have venous thrombi in the legs and thromboembolism and infarction in the lungs. The aortic valve cusps showed thickening of the free edges and the right coronary and noncoronary cusps were roughened and fused for about 5 mm. There was an aneurysm running behind this fused area with a blind passage about 20 mm deep. A full thickness posterior myocardial infarction was also present. No C. burneti was found at autopsy or grown in mice. A clinical diagnosis of healed Q fever endocarditis was made, based on the change in the C.F. antibody titre during therapy and the autopsy macroscopic appearance. Death was caused by renal and cardiac failure with pulmonary thromboembolism. It seems that the initial Q fever endocarditis may be regarded as having been sterilized. Discussion We have now investigated 21 patients who have had Q fever associated with an organic cardiac murmur. Of the total, 16 have developed Q fever endocarditis. It is apparent that such patients should be followed carefully for a long time. T ABLiE 2. Important Laboratory Data ESR No 1. 2. 3. 4. ,. 6. 7. 8. 9. 10. 11. FIGURE 1. Angiogram of case 3, showing the posterior libial artery. a sacular aneurysm of 12. 13. 14. 15. 16. (mm/hr) 2 40-60 2 3-23 10 3-75 7-16 29 13 82 47 18 57 23 4 110 Abbreviation: ESR Urine (RBC) No No No No No No No Occas. Yes Occas. No No Occas. Yes No No Gamma globulin 3.0 gr 3.27 gb 2.0g 'Ye 3.3 g %I 1.2 5gc - Increased 2.01 g %c 1 .9 g 670 Pliase I titre (reciprocal) 128 512 512 512 256 512+ 512 512 512 1024 512+ 512+ 512± 512+ 1.32 g %7o erythrocy te sedimentation rate. 128 128 682 CIRCULATION VOL. 53, No. 4, APRIL 1976 TABLE 3. Follow-up Data Follow-up Operation Autopsy Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 1. Died of myocardial infarction 2. Aortic valve replacement (heterograft), valve annulus aneurysms extending into septum 3. Aortic valve replacement (heterograft), annular aneurysm exteniding into septum 4. Aortic valve replacement (heterograft), no aneurysm 5.6. Aortic valve replacement (disc valve), no aneurysms 7. Aortic valve replacement (fascia lata), annular aneurysm and thrombus 8. Developed mitral valve incompetence, valve competent and well until 412 years postop, died from myocardial infarctioni Two years postop AI required reoperation (fascia lata), no evidence of Q endocarditis, valve still competent at 4 yr Not performed Valve competent, then died 2 years postop from dislocated neck after heavy drinking Not performed Sudden death in cardiac failure Well, no symptoms, competent valve Bicuspid aortic valve, friable red vegetations Not performed 3 years postop, asymptomatic, valve Died after three months in cardiac failure 9. Died of heart failure and uremia 10. 11. Aortic valve replacement, 3 years postop, valve competent, calcified necrotic leaflets, no cardiac problems C. burineti on mouse inoculation C. burneti on mouse inoculation C. burneti On mouse inoculation C. burneti microscopy Guinea pig developed positive titre competent Followed for 7 years, suicide by shotgun Bacteriological data Severe mitral valve stenosis, Vegetations with irregular- vegetations over C. burneti on mitral valve microscopy Destroyed anterior leaflet of Microscopic aortic valve, vegetations examination of and aneurysms of annulus valve showed C. burneti posteriorly Aortic valve congenitally No C. burneti bicuspid and fused, annular 2 cm deep aneurysm anteriorly, large posterior myocardial infarction Positive mouse inoculation endothelial lined healed annular aneurysm 12. Aortic valve replacement No evidence of Q endocarditis at reoperations which were due to (fascia lata), reoperated tissue valve failure, died after 4 yr twice with mounted homograft & finally from pneumonia & heart failure prosthetic valve 13. Aortic valve replacement 1 year postop, asymptomatic, trivial AI, diastolic murmur (homograft), calcified valve, healed aneurysm 14. 15. Aortic valve replacement Autopsy permission refused Positive evidence of C. burneti on microscopy Mouse inoculated, Coccoid organisms consistent with C. burneti Calcified aortic valve stenosis, C. burneti on Bitten by pig, 2 weeks later cardiac thrombus & subannular failure, died of Klebsiella microscopy septicemia from infected intravenous aneurysm, tricuspid valve thrombus showed C. site burneti organisms 1 year, asymptomatic, valve Positive mouse competent inoculation (ball valve), thrombi and annular aneurysm 16. Aortic valve replacement 1 year, asymptomatic, valve (disc), calcified, bicuspid, competent perforated valve with annular aneurysm The longest "proven" interval between the original attack of Q fever and the clinical onset of Q fever endocarditis was seven years. This patient lived for a further eight years (and died by suicide) and his cardiac signs were not worsening at the time of his death (case 8). It is probable that others had their initial Q fever 20 years (case 16), 14 years (case 2), 15 years (case 13), and 11 years (case 9) prior to their clinical presentation with Q fever C. burneti grown endocarditis, but these times are based only on histories given by the patients. Several of the other patients gave brief histories, but in some the initial history of "Q fever" was clearly the symptomatic onset of their Q fever endocarditis. However, both the initial attack of Q fever and the onset of Q fever endocarditis evidently may occur many years before clinically serious valve damage from the endocarditis occurs; hence, it Q FEVER ENDOCARDITIS/Wilson et al. '.. 683 .--.:!C 2 56 4 i K> R~~~~~~~~~~~e-ol, v '.0 Died Cdase 10 '~~~~ *< \ ~~~~~d years of lollow ,Ip FiGURE 3. Diagram showing the changing titres of complement fixing antibody to Phase 1 antigen in cases 3 and 10. Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 FIGURE 2. Angiogram from the same patient as in figure I ten days after valve replacement and the commencement of tetracycline therapy. is of the most indolent forms of infective endocarditis. Diagnostic features often quoted for Q fever endocarditis include: male patients with aortic valve disease4 usually with anemia and a raised ESR5 and typically with a rise in the gamma globulin level. Grist5 also states that the white cell one count may be low or normal and that albuminuria may often be present without red cells in the urine. Robson and Shimmin6 state that there may be no anemia, leukocytosis, embolic phenomena, or red cells in the urine. In our own 16 patients, 15 had some form of aortic valve disease, two had associated aortic and mitral lesions and only one had isolated mitral stenosis. One patient (case 14) had tricuspid as well as aortic valve involvement. All were males, and 11 were meat industry workers or farmers. Ten had a raised ESR at some time in their illness, but contrary to Grist's findings, only one ever had hemoglobin less than 11 g/100 ml and this patient died of uremia and pulmonary thromboembolism. Gamma globulin was increased in eight of the nine patients in whom it was measured. The white cell count in the blood was over 10,000/mm3 in only two patients. Fever was rarely present and only three of our patients had emboli from their valves. The patient who developed a mycotic aneurysm (shown radiographically and disappearing after treatment) had the first such lesion to be described in Q fever endocarditis (case 3). In this series, as in that of Robson and Shimmin,6 anemia, leukocytosis, hematuria and emboli were uncommon. The most useful laboratory finding would appear to be increased gamma globulin, present in most cases tested for it in our experience. Other tests were of little diagnostic value except for the C.F. antibody titre. Elevated C.F. antibody titre for the Phase 1 antigen of Q fever suggests a past persistent infection. It is the usual laboratory clue that confirms the suspicion of Q fever endocarditis. In our laboratory all but one patient who have ever shown a Phase I titre of 1:256 or greater have eventually been shown to have Q fever endocarditis. The one exception is still being followed. In the symptomatic stage only four patients with Q fever endocarditis had a Phase I antibody titre of less than 1:512 (one was 1:256 and three were 1:128). In our laboratory, therefore, Phase I antibody titres of 1: 128 and above suggest the diagnosis. All patients with these levels are followed up carefully. Readings of 1:512 or greater are virtually diagnostic of the presence of Q fever endocarditis. At least one of our patients had a known valvular lesion before his initial attack of Q fever and, in three others, the valvular lesion was known to be present long before the overt symptoms of Q fever endocarditis appeared. In seven patients the aortic valve was bicuspid, indicating a congenitally abnormal valve prior to the onset of the Q fever endocarditis. Four patients gave a history of recurrent rheumatic fever and in two others valve thickening, cusp fusion and valve calcification were compatible with rheumatic valve damage prior to the onset of Q fever endocarditis. While in some patients it was impossible to ascertain whether the valve was normal or abnormal prior to the onset of rickettsial endocarditis, in most patients it would appear that the infections occurred on a valve already damaged by rheumatic fever or on one which was congenitally abnormal. In our experience, the appearance of the affected valve is typical. The valves are often calcified with small areas of necrotic, thrombotic vegetations. Ten of the 14 aortic valves with endocarditis, either operated on or seen at autopsy, showed aneurysms of the aortic wall at the base of the leaflet. Such aneurysms were particularly striking in case 9 and in the patient whose infection we considered to have been cured by therapy (case 10). These aneurysms are demonstrable angiographically and are helpful in establishing the diagnosis of Q fever endocarditis (fig. 4). The most useful drug in the treatment of Q fever endocarditis is tetracycline,7 and we have used 500 mg four times daily for some months, then 250 mg four times daily for a year or more. If oral therapy should cause side effects, parenteral pyrrolidino-methyl-tetracycline should be used, as in case 10. It seems probable that this patient's Q fever endocarditis was sterilized by tetracycline therapy. Clinical features for the diagnosis were present. Following therapy 684 CI RCU LATION VOL. 53, No. 4, APRIL 1976 FIGURE 5. Photomicrograph X 1000 of aortic valve tissue from patient 13, showing the presence of numerous coccoid organisms, the appearance of which is consistent with Coxiella burneti. Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 FIGURE 4. Aortogram showing aneurysm of the aortic valve incompetence outlining the left ventricular cavity. root and the antibody titres to Phase 1 antigen fell (fig. 3), and when he died three years later an aneurysm similar to those often seen with Q fever endocarditis was found but no C. burneti was isolated. Trimethroprim with sulphamethoxazole has been suggested as an alternative treatment8 but we have no personal experience with its use. An index of the success in controlling the Q fever infection is the behavior of the C.F. antibody to Phase I antigen. The falling titre following surgery and tetracycline therapy is illustrated by case 3 (fig. 3) at the time when macroscopic and microscopic examination for Q fever infection was negative at the second operation. Valve replacement is undertaken when, despite medical treatment, increasing symptoms and worsening hemodynamics occur. Ten such patients were submitted to surgery. In case 2, clinical mitral incompetence and increasing heart size were noted one year after the aortic valve replacement. The aortic valve replacement remained competent throughout. Whether the mitral valve lesion was related to Q fever endocarditis, or to dilatation of the left ventricle associated with coronary artery disease is not clear. Falling antibody titres to both Phase I and Phase 2 antigen suggests that the Q fever infection was controlled. In case 12 the aortic valve was replaced but the presence of Q fever endocarditis was not recognized at first. Aortic incompetence developed due to technical factors, but after a course of tetracycline, at reoperation three months later no macroscopic or microscopic evidence of continuing Q fever infection was present. As in this case, in our experience, no prosthetic valve replacing a Q fever infected valve has been damaged by continuing Q fever infection, all patients of course being treated postoperatively with tetracycline. Acknowledgment The authors wish to acknowledge the assistance given by the Laboratory of Microbiology and Pathology, Queensland Health Department and the Queensland Institute of Medical Research. References I. Derrick EH: Q fever, a new fever entity: Clinical features, diagnosis and laboratory investigation. Med J Aust 2: 281, 1937 2. Powell OW, Stallman ND: The incidence and significance of phase I complement-fixing antibody in Q fever. J Hyg Camb 60: 359, 1962 3. Marmion BP, Higgins FE, Bridges JB, Edwards AT: A case of subacute rickettsial endocarditis with a survey of cardiac patients for this infection. Br Med J 2: 1264, 1960 4. Kristinsson A, Bentall HH: Medical and surgical treatment of Q fever endocarditis. Lancet 2: 693, 1967 5. Grist NR: Annotation. Am Heart J 75: 846, 1968 6. Robson AO, Shimmin CDGL: Chronic Q fever: Clinical aspects of a patient with endocarditis. Br Med J 2: 980, 1959 7. Powell OW, Kennedy KP, Mc Iver M, Silverstone H: Tetracycline in the treatment of Q fever. Australasian Ann Med 11: 184, 1962 8. Freeman R, Hodson ME: Q fever endocarditis treated with Trimethoprim and Sulphamethoxazole. Br Med J 1: 419, 1972 Q fever endocarditis in Queensland. H G Wilson, G H Neilson, E G Galea, G Stafford and M F O'Brien Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017 Circulation. 1976;53:680-684 doi: 10.1161/01.CIR.53.4.680 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1976 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/53/4/680 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/