Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
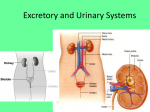
H E M AT U R I A Introduction The word hematuria is derived from the Greek equivalent <hemat> meaning blood and the New Latin equivalent <uria> meaning urine; hence hematuria translates into blood in the urine. Hematuria is one of the most common conditions, that urologists are called upon to investigate or diagnose and often treat. This pamphlet is designed to help the patient better understand the nature and possible significance of this condition as well as explain the various tests and procedures required during this investigation. The Urinary System The human urinary system is a complicated grouping of several important structures (See Figure 1) including the paired kidneys and ureters as well as the single urinary bladder and urethra. The primary function of this system is to rid the body and blood stream of a number of “poisons” or toxic materials produced during normal body functioning. The cleansing process begins in the kidneys, which each receive approximately 25 gallons of blood per day. This blood flows into the kidneys via arteries, is processed or filtered, and the cleansed blood flow out of the kidneys via veins. During this filtration process the body’s poisons, including chemicals such as urea and uric acid, as well as excess body water are deposited as urine into a variety of collection chambers, which ultimately lead to the ureters. The Figure 1 ureters act simply as conduits and carry the urine into the urinary reservoir or bladder. The bladder stores urine until such time as it is convenient and socially acceptable for the individual to urinate. At this time, the urine is expelled to the outside through the last part of the urinary system, the urethra. It is important to realize that all aspects of the urinary system, except the urethra, are essentially the same in both females and males. In females, the urethra consists of a relatively uncomplicated, short (1 – 2 inch), straight tube. In males, the urethra is not only considerably longer and more tortuous, but it is also surrounded by the prostate gland, all of which makes it a more complicated, and hence more disease- prone structure than its female counterpart. Hematuria is frequently described as gross or microscopic. The term gross hematuria implies that the blood in the urine is actually visible to the naked eye. Often the patient describes the passage of bright or dark red or rusty or brownish colored urine, with or without the simultaneous passage of dark reddish solid blood clots. This type of hematuria is understandably very alarming to the patient. Microscopic hematuria, on the other hand, describes the condition in which the urine has a normal yellowish appearance, but nevertheless blood can be demonstrated when a urine specimen is examined under the microscope or tested chemically with a dip-stick. A wide variety of abnormal conditions anywhere along the course of the urinary system can result in the presence of blood within the urine. Some of these conditions such as low grade infections or small ruptured blood vessels frequently heal themselves and are of little consequence, while others, such as inflammations of the kidneys, stones, blockages (obstructions) or malignancies require specific medical or surgical treatment and can be life-threatening. It is the job of the urologist to determine the location and nature of any such condition as well as to prescribe any required treatment. The following steps are characteristic of an evaluation of hematuria. Medical History: A detailed history of the patient’s experience with the hematuria (i.e.: gross versus microscopic bleeding, presence or absence of associated kidney pain, etc.) as well as any other current or prior urologic or general medial experiences (i.e.: prior history of kidney stones or treatment with blood thinners such as Coumadin, etc.) is obviously important. Physical Examination: A general medical examination with emphasis on the urinary system could indicate a mass (growth) in one of the kidneys or abrasions or ulcerations on the penis or vagina near the urethral opening such that blood from these areas could accidentally mix with the voided urine. Urinalysis: The patient’s urine would obviously be examined for blood but also for infection cells (simple kidney or bladder infections frequently are associated with hematuria), protein (kidney inflammationsglomerulonephritis usually produce blood and protein in the urine), and sugar. Urine Culture: Formal evaluation of urine for infection usually requires a urine culture, which is a study designed to determine whether or not bacteria can be grown from the patient’s urine. Urine Cytology: Many malignancies of the urinary system shed cancerous appearing cells into the urine. Utilizing techniques similar to the female Pap smear, these cells can be identified. Blood Tests: Blood tests (BUN and Creatinine) to evaluate overall kidney functions are often helpful. Kidney Ultrasound: This study utilizes harmless, high frequency sound waves to create an image or picture of the kidneys. A small-lubricated probe is gently rubbed over the upper abdomen as the picture is observed on a television screen. Kidney tumors, stones, and/or blockages can be easily noted. Intravenous Pyelogram: The Intravenous Pyelogram or IVP represents another method of viewing the kidneys and ureters. A liquid “dye” or contrast material is injected into the patient’s blood stream and a few minutes later, as the material is excreted into the urinary system, a series of X-rays clearly demonstrate these important structures. An IVP can uncover a wide variety of causes of hematuria including stones, tumors, and blockages. Computerized Tomography: At times, preliminary studies such as a kidney ultrasound or an IVP will suggest, but not be specific enough, to diagnose an abnormality. Under these circumstances, a computerized tomogram or CAT scan may be performed. Like an IVP, contract material is injected and then a series of cross sectional X-rays are performed yielding detailed images of the patient’s internal anatomy. Cystoscopy: The primary aspects of the urinary system visualized by X-rays such as sonograms, IVP’s and/or CAT scans are the kidneys and ureters. On the other hand, the urinary bladder and urethra are optimally examined by direct visualization with the cystoscope. This small, lubricated instrument is gently passed down the anesthetized urethra into the bladder. Common abnormalities such as scarring or strictures of the urethra, prostatic enlargement (in the male), bladder tumors, or bladder stones can be easily located. Contrary to popular misconception, cystoscopy can be safely and comfortably performed as an office procedure and rarely requires the risks of general anesthesia. Retrograde Pyelogram: On occasion, the ureters or the interior of the kidneys are not well delineated on standard X-rays such as sonograms or IVP’s. Under these circumstances, the cystoscopic examination of the bladder can be extended to include a retrograde pyelogram. In the study, the X-ray “dye” or contrast material is directly injected into the ureters and hence into the kidneys as both structures are viewed on a television-type screen. The most significant causes of hematuria diagnosed or excluded during this study include ureteral or kidney stones, tumors, or blockages. Most patients with hematuria do not require all of these tests. The patient’s urologist will select those tests most appropriate for the given situation. Remember, the overall aim of the evaluation is to very thoroughly evaluate the urinary system in the safest, most efficient, and least costly manner. What Could Be The Cause Of The Hematuria And What Treatment Would Be Required? Depending upon the patient’s type of hematuria, his or her age and sex, and the presence of associated symptoms and/or physical findings, a number of possible causes for hematuria must be considered. In approximate order of increasing frequency, these would include the following: Inflammations (not infections) of the kidneys Tumors of the Ureters Tumors of the Kidneys Kidney Stones Tumors of the Urinary Bladder Blockages of the Ureters Bladder Stones Prostatic Enlargement Urinary Infections Inflammations of the Bladder Necessary treatment would obviously depend upon the type of condition diagnosed. At times, simple patient observation (i.e.: with prostatic enlargement) might be appropriate, while in other circumstances (i.e.: with urinary infection) medications such as antibiotics might be prescribed. Tumors (malignancies) and/or blockages frequently require surgery. not require treatment and almost never leads to any long-term health problems. What If The Cause Cannot Be Determined? It is quite common, especially with microscopic hematuria, that the tests will all prove to be normal and no specific cause for the hematuria can be detected. This situation is often quite unsettling for the patient. In reality, however, not finding a tumor, stone, or blockage is actually “good news”. In these cases, the urinary bleeding is often referred to as “benign hematuria,” meaning that the hematuria is not being produced by a significant abnormality. It is assumed in benign hematuria that there is possibly a microscopic “leak” in the kidney filtration process, resulting in small amounts of blood seeping into the urine. This situation is of no consequence since it does What About the Future? Assuming the evaluation has uncovered no major problems, most urologists would simply observe the patient’s course. A repeat medical history, physical examination, and most likely, another urinalyses would be appropriate in 4 to 6 months. Repeating any of the other studies would probably not be necessary. Benign, microscopic hematuria is very frequently persistent and long lasting. Thus, patients should be cautioned not to become alarmed if future urinalysis again demonstrates blood. On the other hand, should a patient again experience gross (visible) urinary bleeding, the urologist should be immediately notified.