Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
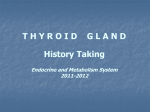
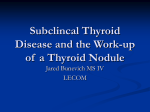
Subclinical Thyroid Disease and the Incidence of Hypertension in Pregnancy Karen L. Wilson, MD, Brian M. Casey, and F. Gary Cunningham, MD MD, Donald D. McIntire, OBJECTIVE: To estimate the possibility of long-term effects of subclinical thyroid dysfunction on hypertension and other cardiovascular-related conditions during pregnancy. METHODS: This is a secondary analysis of a prospective prenatal population-based study in which serum thyroidfunction analytes were measured from November 2000 through April 2003. Women with evidence of overt thyroid disease were excluded. The remaining women were classified as being euthyroid, having subclinical hyperthyroid, or having subclinical hypothyroid, and the frequency of pregnancy-associated hypertensive disorders was compared between these groups. RESULTS: Pregnancy outcomes in 24,883 women were analyzed for pregnancy hypertension, classified as gestational hypertension, mild preeclampsia, or severe preeclampsia. The incidence of hypertensive disorders were compared between the three cohorts. The overall incidences of hypertension in pregnancy were 6.2%, 8.5%, and 10.9% in the subclinical hyperthyroid, euthyroid, and subclinical hypothyroid groups, respectively, and were found to be significant when unadjusted (Pⴝ.016). After adjusting for confounding factors, there was a significant association between subclinical hypothyroidism and severe preeclampsia (adjusted odds ratio 1.6, 95% confidence interval 1.1–2.4; Pⴝ.03). CONCLUSION: Women with subclinical hypothyroidism identified during pregnancy have an increased risk for severe preeclampsia when compared with euthyroid women. (Obstet Gynecol 2012;119:315–20) DOI: 10.1097/AOG.0b013e318240de6a LEVEL OF EVIDENCE: II From the University of Texas Southwestern Medical Center, Department of Obstetrics and Gynecology, Dallas, Texas. Corresponding author: Karen L. Wilson, MD, The University of Texas Southwestern Medical Center, Department of Obstetrics & Gynecology, 5323 Harry Hines Blvd, Dallas, TX 75390-9032; e-mail: KarenL.Wilson@ utsouthwestern.edu. Financial Disclosure The authors did not report any potential conflicts of interest. © 2012 by The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins. ISSN: 0029-7844/12 VOL. 119, NO. 2, PART 1, FEBRUARY 2012 PhD, Lisa M. Halvorson, MD, T hyroid hormones have a number of actions on cardiovascular physiology and blood pressure regulation, which are mediated by genomic mechanisms that cause ventricular remodeling or by direct effects. In most cases, cardiovascular aberrations follow long-term exposure to excessive or decreased hormone levels.1–3 The effects of long-standing subclinical thyroid disorders are less well-studied, and there has been vigorous debate for many decades whether either contributes significantly to long-term cardiovascular morbidity.4 –11 Also, it has been shown that individuals with subclinical hypothyroidism have impaired endothelium-derived vasodilatation from diminished nitric oxide secretion that is restored after thyroxine (T4) replacement.12 Possible adverse effects on pregnancy outcomes related to these subclinical thyroid disorders had renewed interest after publication of two landmark studies in 1999.13,14 Both of these investigations were of limited size and were specifically concerned with the effects of thyroid hormone deficiency on early fetal brain development. Subsequently, a number of large population-based studies that were designed to investigate any adverse effects on subclinical thyroid hormone disorders.15–23 In a study that included a smaller cohort of women, including only women screened before 20 weeks of gestation, we did not find a relationship between subclinical hypothyroidism and pregnancy-associated hypertension.16 In another study from our group, although we found a possible protective relationship between subclinical hyperthyroidism and pregnancy-associated hypertension, we did not control for the important confounder of maternal weight.17 In addition to these studies suggesting a possible link with subclinical thyroid dysfunction and pregnancy-associated hypertension, there is further evidence of vascular-related sequelae. Specifically, autoimmune thyroid disorders have been associated with an increased risk for placental abruption.15,16,19,24 OBSTETRICS & GYNECOLOGY 315 These observations, when coupled with the pathologic cardiovascular effects of overtly abnormal increased or decreased thyroid hormone production, prompted the current study to further investigate the relationship between hypertensive disorders and subclinical thyroid dysfunction in a larger cohort, including women who presented for prenatal care after 20 weeks of gestation. MATERIALS AND METHODS This is another secondary analysis of a prospectively collected database initially designed to estimate normative values for thyroid hormone analytes in a large population of pregnant women.16,17 The protocol was approved by the Institutional Review Boards of the University of Texas Southwestern Medical Center and Parkland Hospital. The details of this process and the thyroid-analyze assays have been previously described.16 –18 Briefly, excess serum obtained for prenatal serologic screening from November 1, 2000 to April 14, 2003, was delivered to our immunochemistry research laboratory for thyroid analyte studies. Using a chemiluminescent assay (Immulite 2000 Analyzer), serum concentrations were determined for thyrotropin (TSH) and free T4. Women identified to have abnormal TSH levels had serum free T4 reflexively determined, and if it was either abnormally high or low, then they were contacted and referred to an obstetrical complications clinic for further evaluation and possible treatment of overt thyroid dysfunction. These women were excluded from study, whereas all other women were enrolled in the prospective cohort. For the purposes of the current study, normal values were considered to be those that comprised the range from the 2.5th to 97.5th percentiles for the entire cohort. For TSH, these values were 0.03 to 4.13 milliunits/L and for free T4 these values ranged from 0.9 to 2.0 ng/dL. All women screened and delivered at Parkland Hospital and without evidence of overt thyroid dysfunction were included. Other inclusion criteria were subsequent delivery of a singleton neonate weighing 500 g or more. Women with serum TSH values within the normal range were considered to be euthyroid. Those with an abnormally low TSH but normal free T4 levels were classified as having subclinical hyperthyroidism. Conversely, women with abnormally high TSH but normal free T4 levels were classified as having subclinical hypothyroidism. Pregnancy outcomes were retrieved from the computerized perinatal database that has been previously described.16 –18 These data are routinely entered for all women at the time of their delivery at Parkland Hospital. For this study, the incidence of pregnancy- 316 Wilson et al associated hypertensive disorders were compared for the three cohorts described. Hypertensive disorders were defined and classified according to a previously described protocol.25 Briefly, gestational hypertension was defined as persistent blood pressures of 140/90 mm Hg or more, occurring after 20 weeks of gestation, without evidence of proteinuria. Mild preeclampsia was diagnosed in hypertensive women who also had 1⫹ proteinuria determined by urine dipstick analysis from a catheterized sample as per the protocol of our institution. Severe preeclampsia was diagnosed in hypertensive women with any of the following: 2⫹ or more proteinuria by dipstick from a catheterized urine sample, blood pressure higher than 160/110 mm Hg, persistent headache, visual disturbances, right upper quadrant or epigastric pain, serum creatinine 1.2 mg/mL or more, serum aspartate transaminase levels more than twice the upper limit of normal, or thrombocytopenia less than 100,000/mL. Statistical analyses included Pearson 2, CochranArmitage 2 for trend, analysis of variance, and logistic regression. When the three-group omnibus tests were statistically significant, contrast analyses were used to examine two-group comparisons and isolate significance of difference. Multivariable analyses were included to adjust for the effect modifiers of maternal age and weight as continuous measures, and categorical effects of race (as African American, white, Hispanic, other) and parity (as 0, 1, 2, more than 2). Statistical computations were performed with SAS 9.2 and two-sided P⬍.05 was considered statistically significant. RESULTS During the 30-month study, a total of 24,883 women who delivered singleton neonates weighing more than 500 g were included in this study. Of these, 23,771 (95.5%) had TSH values within the normal range and were considered to be euthyroid; 528 (2.1%) had TSH levels more than 4.13 milliunits/L along with normal free T4 levels, therefore meeting criteria for subclinical hypothyroidism. The remaining 584 (2.3%) had TSH levels less than 0.03 milliunits/L along with normal free T4 levels, therefore meeting criteria for subclinical hyperthyroidism. Maternal demographics of the three cohorts are shown in Table 1, in which women within either the subclinical hyperthyroid cohort or the hypothyroid cohort were compared with those in the euthyroid cohort. The incidences of pregnancy-associated hypertensive disorders as well as mild and severe preeclampsia were compared between the three study cohorts. In general, as the serum TSH level increased Subclinical Thyroid Disease and Hypertension OBSTETRICS & GYNECOLOGY Table 1. Maternal Demographics in Women With Subclinical Thyroid Dysfunction Compared With Euthyroid Women Subclinical Hyperthyroid (nⴝ584) Euthyroid (nⴝ23,771) P* ⬍.001 Race African American White Hispanic Other Parity 0 1 2 More than 2 Age (y) Weight P† ⬍.001 100 (17) 10 (2) 449 (77) 25 (4) 2,690 (11) 558 (2) 20,002 (84) 521 (2) .415 195 (33) 179 (31) 117 (20) 93 (16) 25.8⫾5.5 162⫾30 Subclinical Hypothyroid (nⴝ528) 31 (6) 20 (4) 455 (86) 22 (4) .845 8,232 (35) 7,561 (32) 4,757 (20) 3,221 (14) 25.2⫾5.6 170⫾34 .009 ⬍.001 ⬍.001 .057 184 (35) 163 (31) 113 (21) 68 (13) 26.7⫾5.7 176⫾38 Data are n (%) or mean⫾standard deviation unless otherwise specified. * Compares hypothesis of equality of subclinical hyperthyroid and euthyroid. † Compares hypothesis of equality of subclinical hypothyroid and euthyroid. in the entire population, the incidence of hypertensive disorders increased concomitantly (P for trend, P⫽.004). This relationship is shown in Figure 1, in which subclinical hyperthyroid women who had the lowest TSH levels had an incidence of hypertensive disorders of 6.2% compared with 8.5% of euthyroid women and 10.9% of subclinical hypothyroid women. These differences when unadjusted were significant (P⫽.016). These were then adjusted for maternal age, race, parity, and weight using logistic regression. Shown in Figure 2 are the adjusted odds ratios when Women delivered (%; upper 95% CI) 16 14 12 10 8 6 4 2 0 Any hypertension P=.004 Mild hypertension Severe hypertension P=.018 P=.003 Hypertension classification Fig. 1. Incidence of hypertension during pregnancy and mild or severe preeclampsia according to classification of subclinical hyperthyroidism (dark gray bars), euthyroid (light gray bars), and subclinical hypothyroidism (black bars) in 24,883 pregnant women who were screened during the first prenatal visit. Wilson. Subclinical Thyroid Disease and Hypertension. Obstet Gynecol 2011. VOL. 119, NO. 2, PART 1, FEBRUARY 2012 the risks for hypertensive disorders were compared between the three cohorts. After adjustments, the only remaining significant association was in the cohort of women with subclinical hypothyroidism who were at increased risk for severe preeclampsia (adjusted odds ratio 1.6, 95% confidence interval 1.1–2.4; P ⫽.031). DISCUSSION The one salient finding of this study that included nearly 25,000 pregnant women was that those identified to have subclinical hypothyroidism had a significantly increased risk for development of severe preeclampsia when compared with euthyroid women. This association is particularly strong because its significance persisted after adjustment for factors known to increase preeclampsia risks, such as age, parity, race, and weight.26,27 There are a number of observations that support the biological plausibility of this association. These include the cardiovascular effects of abnormal concentrations of thyroid hormones, the adverse pregnancy outcomes reported for women with overt hypothyroidism, other vascularrelated pregnancy complications that have been linked to subclinical hypothyroidism, and, finally, endothelial cell activation from abnormal amounts of thyroid hormones. Regarding the first observation, there are welldocumented widespread cardiovascular effects in nonpregnant women who secrete abnormal amounts of thyroid hormones. Those that are genomically mediated include transcription of structural and regulatory proteins within myocytes that stimulate cell growth.1 Nongenomic direct T4 actions include increased cardiac contractility and decreased systemic Wilson et al Subclinical Thyroid Disease and Hypertension 317 Any hypertension Subclinical hyperthyroidism 0.78 (0.55–1.10) Subclinical hypothyroidism 1.25 (0.94–1.66) Mild hypertension Subclinical hyperthyroidism 0.83 (0.53–1.31) Subclinical hypothyroidism 1.35 (0.95–1.94) Severe hypertension Subclinical hyperthyroidism 0.71 (0.40–1.26) Subclinical hypothyroidism 1.60 (1.08–2.37) 0.0 0.5 1.0 1.5 2.0 2.5 Wilson. Subclinical Thyroid Disease and Hypertension. Obstet Gynecol 2011. Odds ratios (95% confidence interval) vascular resistance. Also, with prolonged exposure to either abnormally excessive or decreased amounts of hormone, ventricular hypertrophy can lead to heart failure.1,2,28 Up to one fourth of overtly hypothyroid individuals are hypertensive, with a decreased pulse pressure, slowed diastolic filling, decreased ventricular filling and contractility, and increased systemic vascular resistance.1,2 Although less well-studied, there is evidence that subclinical hypothyroidism in some, usually older, patients can cause hypertension, heart failure, and atherosclerotic vascular disease.1,6,8,29 Finally, subclinical hypothyroidism has been shown to cause endothelial cell dysfunction characterized by diminished nitric oxide production with impaired vasorelaxation.12 A second observation that strengthens the biological plausibility of a link between subclinical hypothyroidism and preeclampsia is that adverse outcomes are increased in pregnant women with overt thyroid disorders. A number of investigators have reported that pregnancies in women with untreated or poorly controlled thyrotoxicosis have increased incidences of cardiovascular and related complications such as preeclampsia, placental abruption, and heart failure.3,30 –34 Similarly, reports of pregnant women with untreated overt hypothyroidism describe inordinately high rates of preeclampsia, placental abruption, and heart failure.30,33,34 The third link is derived from large prenatal screening studies designed to ascertain normal serum levels of thyroid-related analytes, as well as to study adverse pregnancy outcomes caused by thyroid disorders.19,21,35 Although in none of these was an association found between subclinical hypothyroidism or hyperthyroidism and preeclampsia, in one study pregnant women with subclinical hypothyroidism had a significant association with placental abruption, which is another vascular-related complication. In this study, such women were observed to have a significant threefold increased risk for placental abruption compared with euthyroid pregnant women.16 318 Wilson et al Fig. 2. Risk (adjusted odds ratio) of hypertension during pregnancy and mild or severe preeclampsia according to classification of subclinical thyroid dysfunction in 24,883 pregnant women who were screened during the first prenatal visit. Odds ratios are adjusted for maternal age, race, parity, and weight. Euthyroid women (n⫽23,771) served as the referent population. Additionally, in two of these large population-based studies, a significantly increased twofold to threefold risk for placental abruption was reported in women who had abnormally elevated serum antithyroid antibody levels.15,16 The unifying theme of these cited studies is that abnormal levels of thyroid hormones can lead to long-term cardiovascular sequelae that are mediated in part by chronic endothelial cell damage. In this regard, preeclampsia is thought to be a syndrome characterized by multiorgan involvement that results from endothelial cell activation.36 Thus, it seems reasonable to posit that abnormal levels of thyroid hormones are additive or synergistic toward the development of preeclampsia in women genetically predisposed.37 As such, the effects of subclinical hypothyroidism are similar to those observed in other maternal conditions characterized by chronic endothelial activation with an increased risk for preeclampsia. Some of these underlying conditions include obesity and the metabolic syndrome, chronic hypertension, diabetes, and renal disease.27,37–39 The strengths of this study are principally related to the number of women enrolled. Specifically, even after adjusting for maternal age, race, parity, and weight, the association of subclinical hypothyroidism and severe preeclampsia remains significant. Conversely, there are three weaknesses that are apparent. One is that the majority of women are of Hispanic heritage, and thus our observations may not be applicable in other ethnic populations. A second is that our database precluded identification of women with chronic hypertension or other such risk factors that are known to increase the risk for preeclampsia. Finally, because height was not recorded for all women enrolled in the first part of the study, we adjusted using weight as a continuous variable instead of body mass index, which many consider to be a more accurate indicator of obesity. What are the implications of this persistent association between subclinical hypothyroidism and se- Subclinical Thyroid Disease and Hypertension OBSTETRICS & GYNECOLOGY vere preeclampsia? We are of the opinion that our findings are more biologically significant than clinically relevant. Our observations add to accruing data that subclinical hypothyroidism, a relatively common finding in women of childbearing age, may be associated with some adverse perinatal outcomes. Nonetheless, we remain convinced that routine prenatal screening for thyroid disorders should not be implemented until clear benefit is established. The Eunice Kennedy Shriver National Institute of Child Health and Human Development–sponsored randomized intervention trial of women identified to have subclinical thyroid disorders currently being conducted by the Maternal-Fetal Medicine Units Network may provide such data. REFERENCES 1. Danzi S, Klein I. Thyroid hormone and blood pressure regulation. Curr Hypertens Rep 2003;5:513–20. 2. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl J Med 2001;344:501–9. 3. Sheffield JS, Cunningham FG. Thyrotoxicosis and heart failure that complicate pregnancy. Am J Obstet Gynecol 2004;190: 211–7. 4. Cappola AR, Fried LP, Arnold AM, Danese MD, Kuller LH, Burke GL, et al. Thyroid status, cardiovascular risk, and mortality in older adults. JAMA 2006;295:1033– 41. 5. Dorr M, Wolff B, Robinson DM, John U, Ludemann J, Meng W, et al. The association of thyroid function with cardiac mass and left ventricular hypertrophy. J Clin Endocrinol Metab 2005;90:673–7. 6. Duan Y, Peng W, Wang X, Tang W, Liu X, Xu S, et al. Community-based study of the association of subclinical thyroid dysfunction with blood pressure. Endocrinology 2009;35: 136 – 42. 7. Volzke H, Ittermann T, Schmidt CO, Dorr M, John U, Wallaschofski H, et al. Subclinical hyperthyroidism and blood pressure in a population-based prospective cohort study. Eur J Endocrinol 2009;161:615–21. 8. Liu D, Jiang F, Shan Z, Wang B, Wang J, Lai Y, et al. A cross-sectional survey of relationship between serum TSH level and blood pressure. J Hum Hypertension 2010;24: 134 – 8. 9. Imaizumi M, Akahoshi M, Ichimaru S, Nakashima E, Hida A, Soda M, et al. Risk for ischemic heart disease and all-cause mortality in subclinical hypothyroidism. J Clin Endocrinol Metab 2004;89:3365–70. and subsequent neuropsychological development of the child. N Engl J Med 1999;341:549 –55. 14. Pop VJ, Kuijpens JL, van Baar AL, Verkerk G, van Son MM, de Vijlder JJ, et al. Low maternal free thyroxine concentrations during early pregnancy are associated with impaired psychomotor development in infancy. Clin Endocrinol (Oxf) 1999;50:149 –55. 15. Abbassi-Ghanavati M, Casey BM, Spong CY, McIntire DD, Halvorson LM, Cunningham FG. Pregnancy outcomes in women with thyroid peroxidase antibodies. Obstet Gynecol 2010;116:381– 6. 16. Casey BM, Dashe JS, Wells CE, McIntire DD, Byrd W, Leveno KJ, et al. Subclinical hypothyroidism and pregnancy outcomes. Obstet Gynecol 2005;105:239 – 45. 17. Casey BM, Dashe JS, Wells CE, McIntire DD, Leveno KJ, Cunningham FG. Subclinical hyperthyroidism and pregnancy outcomes. Obstet Gynecol 2006;107:337– 41. 18. Casey BM, Dashe JS, Spong CY, McIntire DD, Leveno KJ, Cunningham GF. Perinatal significance of isolated maternal hypothyroxinemia identified in the first half of pregnancy. Obstet Gynecol 2007;109:1129 –35. 19. Cleary-Goldman J, Malone FD, Lambert-Messerlian G, Sullivan L, Canick J, Porter TF, et al. Maternal thyroid hypofunction and pregnancy outcome. Obstet Gynecol 2008;112:85–92. 20. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol (Oxf) 2003;59:282– 8. 21. Mannisto T, Vaarasmaki M, Pouta A, Hartikainen AL, Ruokonen A, Surcel HM, et al. Perinatal outcome of children born to mothers with thyroid dysfunction or antibodies: a prospective population-based cohort study. J Clin Endocrinol Metab 2009;94:772–9. 22. Mannisto T, Vaarasmaki M, Pouta A, Hartikainen AL, Ruokonen A, Surcel HM, et al. Thyroid dysfunction and autoantibodies during pregnancy as predictive factors of pregnancy complications and maternal morbidity in later life. J Clin Endocriniol Metab 2010;95:1084 –94. 23. Stagnaro-Green A, Chen X, Bogden JD, Davies TF, Scholl TO. The thyroid and pregnancy: a novel risk factor for very preterm delivery. Thyroid 2005;15:351–57.24. 24. Haddow JE, McClain MR, Palomaki GE, Neveux LM, Lambert-Messerlian G, Canick JA, et al. Thyroperoxidase and thyroglobulin antibodies in early pregnancy and placental abruption. Obstet Gynecol 2011;117(2 Pt 1):287–92. 25. Alexander JM, McIntire DD, Leveno KJ, Cunningham FG. Selective magnesium sulfate prophylaxis for the prevention of eclampsia in women with gestational hypertension. Obstet Gynecol 2006;108:826 –32. 10. Volzke H, Robinson DM, Schminke U, Ludemann J, Rettig R, Felix SB, et al. Thyroid function and carotid wall thickness. J Clin Endocrinol Metab 2004;89:2145–9. 26. Ness RB, Roberts JM. Epidemiology of pregnancy-related hypertension. In: Lindheimer MD, Roberts JM, Cunningham FG, editors. Chesley’s hypertensive disorders in pregnancy. San Diego (CA): Elsevier; 2009. p. 37–50. 11. Walsh JP, Bremner AP, Bulsara MK, O’Leary P, Leedman PJ, Feddema P, et al. Subclinical thyroid dysfunction as a risk factor for cardiovascular disease. Arch Intern Med 2005;165: 2467–72. 27. Hubel CA, Roberts JM. Metabolic syndrome and preeclampsia. In: Lindheimer MD, Roberts JM, Cunningham FG, editors. Chesley’s hypertensive disorders in pregnancy. San Diego (CA): Elsevier; 2009. p. 105–28. 12. Taddei S, Caraccio N, Virdis A, Dardano A, Versari D, Ghiadoni L, et al. Impaired endothelium-dependent vasodilation in subclinical hypothyroidism: Beneficial effect of levothyroxine therapy. J Clin Endocrinol Metab 2003;88:3731–7. 28. Fletcher AK, Weetman AP. Hypertension and hypothyroidism. J Hum Hypertension 1998;12:79 – 82. 13. Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, et al. Maternal thyroid deficiency during pregnancy VOL. 119, NO. 2, PART 1, FEBRUARY 2012 29. Rodondi N, Newman AB, Vittinghoff E, de Rekeneire N, Satterfield S, Harris TB, et al. Subclinical hypothyroidism and the risk of heart failure, other cardiovascular events, and death. Arch Intern Med 2010;165:2460 – 6. Wilson et al Subclinical Thyroid Disease and Hypertension 319 30. Davis LE, Lucas MJ, Hankins GD, Roark ML, Cunningham FG. Thyrotoxicosis complicating pregnancy. Am J Obstet Gynecol 1989;160:63–70. 31. Kriplani A, Buckshee K, Bhargava VL, Takkar D, Ammini AC. Maternal and perinatal outcome in thyrotoxicosis complicating pregnancy. Eur J Obstet Gynecol Reprod Biol 1994;54: 159 – 63. 32. Mestman JH. Hyperthyroidism in pregnancy. Clin Obstet Gynecol 1997;40:45– 64. 33. Abalovich M, Gutierrez S, Alcaraz G, Maccallini G, Garcia A, Levalle O. Overt and subclinical hypothyroidism complicating pregnancy. Thyroid 2002;12:63– 8. 34. Leung AS, Millar LK, Koonings PP, Montoro M, Mestman JH. Perinatal outcome in hypothyroid pregnancies. Obstet Gynecol 1993;81:349 –53. 320 Wilson et al 35. Dashe JS, Casey BM, Wells CE, McIntire DD, Byrd EW, Leveno KJ, et al. Thyroid-stimulating hormone in singleton and twin pregnancy: importance of gestational age-specific reference ranges. Obstet Gynecol 2005;106:753–7. 36. Taylor RN, Davidge ST, Roberts JM. Endothelial cell dysfunction and oxidative stress. In: Lindheimer MD, Roberts JM, Cunningham FG, editors. Chesley’s hypertensive disorders in pregnancy. San Diego (CA): Elsevier; 2009. p. 143– 68. 37. Maynard SE, Karumanchi SA. Angiogenic factors and preeclampsia. Semin Nephrol 2011;31:33– 46. 38. Cornelis T, Odutayo A, Keunen J, Hladunewich M. The kidney in normal pregnancy and preeclampsia. Semin Nephrol 2011;31:4 –14. 39. Davison JM, Lindheimer MD. Pregnancy and chronic kidney disease. Semin Nephrol 2011;31:86 –99. Subclinical Thyroid Disease and Hypertension OBSTETRICS & GYNECOLOGY