Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Thesis
TNF Inhibitors in Dermatology: From Thalidomide to Biologics
LAFFITTE, Emmanuel Alexis
Abstract
Inflammatory skin diseases represent an important part of dermatological pathology. Recent
advances in the understanding of inflammatory processes have identified various cytokines,
and in particular Tumor necrosis factor (TNF) as a potent and central proinflammatory
cytokine involved in many conditions, including rheumatic, gastrointestinal tract, and skin
diseases. Therefore, inhibition of TNF has become a major therapeutic target in the treatment
of inflammatory disorders. Thalidomide is one of the first TNF inhibitors that have been used.
It was initially prescribed by chance and pragmatically by dermatologists in inflammatory
diseases such as erythema nodosum leprosum, lupus and severe aphtosis, but its
identification as an inhibitor of TNF is more recent. The discovery of the major role of TNF
alpha in the physiopathology of certain inflammatory diseases and notably in rheumatoid
arthritis and Crohn's disease has led to the emergence of 3 new anti-TNF alpha drugs. These
so-called biologics are two monoclonal antibodies (infliximab and adalimumab) and one fusion
protein composed of a soluble TNF alpha receptor [...]
Reference
LAFFITTE, Emmanuel Alexis. TNF Inhibitors in Dermatology: From Thalidomide to
Biologics. Thèse de privat-docent : Univ. Genève, 2010
DOI : 10.13097/archive-ouverte/unige:6447
Available at:
http://archive-ouverte.unige.ch/unige:6447
Disclaimer: layout of this document may differ from the published version.
TNF inhibitors in Dermatology
From Thalidomide to Biologics
Emmanuel Laffitte
Service de Dermatologie et Vénérologie
Hôpitaux Universitaires de Genève
Thèse d’habilitation à la fonction de Privat-Docent
Faculté de Médecine de Genève
Février 2010
2
Table of contents
Acknowledgments
5
Introduction: TNF inhibition: old and new dreams
7
Part I- TNF in Dermatological diseases
9
9
10
1- Biology of TNF
2- Role of TNF in cutaneous inflammatory disorders
Part II-Thalidomide: an old drug with new clinical applications
1- Introduction
2- Pharmacology
3- Biological properties
3.1 Hypnosedative action
3.2 Immunological properties
3.3 Anti-angiogenic properties
4- Clinical applications
5- Side effects
5.1 Toxicity
5.2 Major side effects
5.2.1 Teratogenic Effect
5.2.2 Peripheral Neuropathy
5.2.3 Thalidomide and thromboses
5.3 Minor side effects:
6- Guidelines for the clinical use of Thalidomide
7- Thalidomide on Internet
8- The future? Thalidomide derivatives and lenalidomide in dermatology
8.1 Lenalidomide: the second generation imid
8.2 Lenalidomide in dermatology
8.3 Our experience with lenalidomide in cutaneous disorders
Part III- The new era: Biologics as Tumor necrosis factor antagonists
1- Introduction
2- TNF antagonists used in dermatology: Infliximab, Etanercept, Adalimumab
2.1 Etanercept
2.2 Infliximab
2.3 Adalimumab
3- TNF antagonists in psoriasis
3.1 Identification of psoriasis as a severe disease; burden of the disease, cost of illness in Switzerland
3.2 Treating chronic plaque psoriasis with biologics
3.3 Treating other forms of psoriasis with biologics
3.4 Practical use in Switzerland
4- Side effects: some dermatological particularities
4.1 Infections: Tuberculosis and tuberculosis screening in Psoriasis patients
4.2 Cutaneous side effects
4.2.1 Eczematiform and atopic rash
4.2.2 Palmoplantar pustulosis and paradoxal psoriasis
4.2.3 Other cutaneous side effects
4.3 Skin carcinomas
4.3.1 Melanoma and melanoma skin cancers
4.3.2 Cutaneous lymphoma
5- TNF antagonists in other cutaneous diseases
5.1 Cutaneous sarcoidosis and other granulomatoses
5.2 Necrobiosis lipoidica
5.3 Hidradenitis suppurativa
5.4 Behçet disease and aphtosis
5.5 Netherton syndrome
13
13
13
15
17
21
25
27
27
29
29
29
32
37
41
3
6- Perspectives for TNF antagonists
6.1 Industry independent evaluation of efficacy and safety: usefulness of registries
6.2 Development of a targeted TNF inhibition with oral molecules?
45
Conclusions
49
References
51
Appendix
63
Appendix 1:
Laffitte E, Revuz J. Thalidomide: an old drug with new clinical applications. Expert Opin
Drug Saf. 2004;3:47-56
65
Appendix 2:
Laffitte E, Revuz J. Thalidomide. Ann Dermatol Venereol. 2007;134:957-60
77
Appendix 3:
Laffitte E. Thalidomide in Kaposi sarcoma: promising or disappointing? Dermatology.
2007;215:171-2
83
Appendix 4:
Laffitte E. Thalidomide, semen distribution, teratogenicity...and cost. Br J Dermatol.
2006;154:563
87
Appendix 5:
Navarini A, Laffitte E, Conrad C, Piffaretti P, Brock E, Ruckdaeschel S, Trüeb R.
Estimation of cost-of-illness in patients with psoriasis in Switzerland. Swiss Med Wkly.
2009. in press
91
Appendix 6:
Laffitte E, Dudler J, Panizzon RG. Psoriasis unguéal et traitements anti-TNFα. Ann
Dermatol Venereol 2004;131:1S71-1S272 and presented as poster in Journées
Dermatologiques de Paris, 7-11 décembre 2004.
101
Appendix 7:
Laffitte E, Kunzle N, Mottet C, Panizzon RG. Severe psoriasis with chronic active hepatitis
C: treatment by etanercept. Brit J Dermatol 2006;154 :25, and presented as a poster in 4th
International Congress on Psoriasis - From Gene to Clinic, London, 4-6 December 2006.
105
Appendix 8:
Laffitte E, Janssens JP, Roux-Lombard P, Thielen AM, Barde C, Marazza G, Panizzon RG,
Saurat JH. Tuberculosis screening in patients with psoriasis before antitumour necrosis
factor therapy: comparison of an interferon-gamma release assay vs. tuberculin skin test. Br
J Dermatol 2009;161:797-800.
109
Appendix 9:
Dumont-Berset M, Laffitte E, Gerber C, Dudler J, Panizzon RG. Eczematous drug eruption
after infliximab. Br J Dermatol 2004;151:1272-3.
115
Appendix 10: Thielen AM, Barde C, Saurat JH, Laffitte E. Refractory chronic cutaneous sarcoidosis
responsive to dose escalation of TNF-alpha antagonists. Dermatology 2009;219:59-62.
119
Appendix 11: Laffitte E, Fontao L, Kaya G, Khelifa E, Lubbe J, Saurat J-H. Infliximab for Netherton
syndrome: Sustained clinical improvement correlated with a reduction of thymic stromal
lymphopoietin levels in skin. J Invest Dermatol 2009;129:S22, and presented as a poster in
39th Annual ESDR Meeting, 9-12 September 2009, Budapest, Hungary
125
4
Quand le disciple est prêt, le Maître apparaît...
Je tiens à remercier mon Maître le Professeur Jean-Hilaire Saurat pour son accueil, son soutien et
son enseignement tout au long de ces dernières années (bientôt 10 ans…). Je peux vraiment dire
qu’il m’a ouvert les yeux, et montré la Dermatologie comme jamais personne ne l’avait fait jusqu’à
ce que j’ai la chance inestimable (il y a bientôt 10 ans, donc) de le rencontrer…Lorsque je vins à
Genève à la fin de mon internat, en Janvier 2000, ne sachant pas trop (pas du tout) à quel endroit
serait mon avenir, le proverbe Zen cité ci-dessus prit alors tout son sens…
Mes remerciements également aux Doctoresses Anne Marie Thielen et Caroline Barde et au
Docteur Gionatta Marazza pour leur travail sur les biothérapies à Genève, au Professeur Jean
Revuz pour m’avoir mis le pied à l’étrier de ce cheval de bataille qu’est pour moi le thalidomide
depuis plusieurs années, au Docteur Jean Dudler pour son aide et son amitié, et au Professeur
Renato Panizzon pour m’avoir laissé la liberté de développer l’usage des biothérapies à Lausanne
avant de revenir à Genève…
Je dédie ce travail à mes grands parents (je pense souvent à vous cinq même si je n’en ai connu que
quatre…) et en particulier à mon grand père le Docteur Maurice Leconte qui fut un pionnier dans
son domaine, à mon père le Docteur Jacques Laffitte malheureusement parti trop vite, à ma mère
Agnès toujours présente quand il le faut.
Et merci à ma petite famille, Laurence mon épouse, Jules et Lucas, qui m’entourent de leur joie de
vivre et de leur amour joyeux et désordonné…
Genève, le 4 février 2010
5
6
Introduction
TNF inhibition: old and new dreams
Inflammatory skin diseases represent an important part of dermatological pathology. Recent
advances in the understanding of inflammatory processes have identified various cytokines, and in
particular Tumor necrosis factor (TNF) as a potent and central proinflammatory cytokine involved
in many conditions, including rheumatic, gastrointestinal tract, and skin diseases. Therefore,
inhibition of TNF has become a major therapeutic target in the treatment of inflammatory disorders.
Thalidomide is one of the first TNF inhibitors that have been used. It was initially prescribed by
chance and pragmatically by dermatologists in inflammatory diseases such as erythema nodosum
leprosum, lupus and severe aphtosis, but its identification as an inhibitor of TNF is more recent. The
discovery of the major role of TNF alpha in the physiopathology of certain inflammatory diseases
and notably in rheumatoid arthritis and Crohn's disease has led to the emergence of 3 new anti-TNF
alpha drugs. These so-called biologics are two monoclonal antibodies (infliximab and adalimumab)
and one fusion protein composed of a soluble TNF alpha receptor (etanercept) specifically directed
against TNF. The first clinical data are very impressive, but new and unexpected side effects have
progressively been described.
These powerful drugs are increasingly prescribed, and the aim of this work is to summarize the
recent knowledge on the old (thalidomide) and new (biologics) TNF inhibitors in dermatological
diseases.
7
8
Part I
TNF in Dermatological diseases
1- Biology of TNF
Tumour necrosis factor (TNF) is a proinflammatory cytokine that plays a key role in most of the
inflammatory processes, as well as in immune responses to infections and tumour antigens [1].
Human TNF-alpha, which is located on chromosome 6, is translated as a 233 amino acid, 26-kDa
proprotein that lacks a classic signal peptide. Newly synthesized proTNF-alpha is first displayed on
the plasma membrane and is then cleaved in the extracellular domain to release the mature
monomer through the actions of matrix metalloproteases, the TNF-alpha converting enzyme
(TACE) toward a soluble 17-kDa protein made up of three subunits [2].
This molecule stands at the beginning of a proinflammatory cytokines cascade and triggers off
proinflammatory signals at the target cell by binding to membrane TNF receptors. Two different
receptor types are known: a 55-kDa (TNF-RI) and a 75-k Da receptor (TNF-RII). Both TNF-RI and
TNF-RII exist as cell-surface and soluble forms, and both forms bind TNF, although with different
affinities [3]. TNF cell-surface receptors are present on nearly all cell types, including macrophages,
lymphocytes, and neutrophils [2]. TNF must bind to two or three cell-surface receptor molecules for
signal transduction to occur. Numerous biological effects of TNF are mediated by the intracellular
signalling of the high-affinity TNF-RI receptor [4] as well as the low-affinity TNF-RII receptor [5].
Soluble receptors antagonize this proinflammatory cytokine by binding free TNF [3].
TNF may play a role in normal tissue homeostasis as low levels of TNF are produced by
macrophages under physiologic conditions [6]. In disease, TNF is produced in increase amounts by
macrophages, T cells, mast cells, neutrophils, dendritic cells, fibroblasts, keratinocytes and
endothelial cells in response to infection, tissue injury or inflammation [7]. TNF is a pro
inflammatory cytokine with pleiotropic effects which increases the recruitment of leukocytes to the
site of inflammation through increased adhesion molecules expression, increase vascular
permeability, secretion of metalloproteinases and stimulation of other cytokines and chemokines
(IL-1, IL-6, IL-8, GM-CSF) [2]. Much recent work has demonstrated that soluble TNF (solTNF,
signalling primarily through TNFR1) and transmembrane TNF (tmTNF, signalling through both
TNFR1 and TNFR2) have distinctly different, and potentially opposing, functions in inflammation
9
and immunity. Several knockout and knockin mice have been widely used to show that tmTNF is
crucial in maintaining a normal innate immune response to infections including listeria, leishmania
and tuberculosis [8].
Taken together, results from genetic models suggest that soluble TNF (probably signalling through
TNFR1) may be necessary and sufficient to drive inflammation, while by contrast tmTNF (possibly
signalling through TNFR2) may be essential to maintain immunity to infections, and to tolerize
autoantigens [8, 9].
2- TNF in cutaneous inflammatory disorders
This TNF mediated induction of proinflammatory cytokines, leukocyte chemotaxis and
angiogenesis play a fundamental role in autoimmune diseases like rheumatoid arthritis (RA),
Crohn’s disease, Psoriasis or other inflammatory diseases of the skin, diseases that are characterized
by elevated TNF-serum concentrations, sometimes fever and an increase of acute-phase proteins.
The approach of treating inflammatory diseases by blocking TNF has been confirmed by the
dramatic success of thalidomide in aphtosis and erythema nodosum leprosum, and the TNF blockers
infliximab, etanercept and adalimumab in RA, juvenile idiopathic arthritis, Crohn’s disease,
psoriasis or additional chronic inflammatory dermatoses [10-13].
2.1 Psoriasis
Overexpression of TNF has been well demonstrated in psoriasis [2]. In lesional psoriasis skin, and
to a lesser extent in uninvolved psoriasis skin, TNF was found to be distributed throughout the
epidermis and was also specifically localized to the upper dermal blood vessels [14]. Other authors
have localized TNF in psoriatic lesions with dermal macrophages in the papillary dermis and
focally by keratinocytes and intraepidermal Langerhans’ cells but did not find it to be significantly
expressed in endothelial cells, mast cells, or dermal Langerhans’ cells [15]. Importantly, the two
receptors for TNF are differentially expressed in the skin. In normal skin, and uninvolved and
lesional skin from psoriasis patients, the p55 TNF-RI is associated with epidermal keratinocytes and
a network of upper dermal dendritic cells. In contrast, staining of the p75 TNF-RII in normal skin
was found to be restricted to eccrine sweat ducts and dermal dendritic cells, and was absent from
the epidermis [14]. Furthermore, a significantly elevated TNF plasma concentration was found in
psoriatic patients [16]. High levels of TNF have also been detected in psoriatic arthritis. The pattern
and the expression levels of proinflammatory Th1 cytokines, TNF and IL-1b were found to be
similar in synovial tissue of psoriatic arthritis when compared to rheumatoid arthritis [17].
2.2 Other cutaneous inflammatory disorders:
TNF plays a major role in infectious and non infectious granuloma formation [18]. Its implication
has been studied in various systemic granulomatous diseases such as tuberculosis, sarcoidosis and
oral Crohn’s disease lesion [19]. In sarcoidosis, high levels of TNF are correlated with disease
10
activity and progression [18], and the same correlation have been established in erythema nodosum
leprosum [20] or in Behçet’s disease [21].
In some other cutaneous diseases, the role of TNF was less expected:
- In pemphigus vulgaris, which is used as a prototype for an autoimmune dermatosis with blister
formation, there is no clear evidence of a central role for TNF (and IL-1) in the pathogenesis of
blister formation [12]: in vivo an increased expression of TNF and IL-6 is found at the direct site of
intraepidermal adhesion loss [22]. If, however, in vitro cultures of human keratinocytes receive antiTNF antibodies before coculturing with IgG antibodies from pemphigus patients, the phenomenon
of intercellular adhesion loss is absent [22]. This protective effect of blocking TNF can be
reproduced in vivo [12].
- Atopic dermatitis is a model of Th2 cytokine mediated cutaneous disease [23]. However, in the
pathogenesis of atopic dermatitis, TNF is released initially by infiltrating mast cells and later by
invading T-helper lymphocytes, as well as epidermal keratinocytes. TNF is involved in the upregulation of proinflammatory cytokines, such as IL-1, 6 and 8 and of adhesion molecules, such as
ICAM-1 and VCAM, on keratinocytes and vascular endothelial cells, thereby facilitating the
migration and adhesion of inflammatory cells in the epidermis [23].
- Furthermore, in Netherton syndrome (NS), which is a genodermatosis with features of atopic
dermatitis, inflammatory cutaneous flares and ichtiosis caused by mutations in SPINK5 (a gene
encoding the protease inhibitor lymphoepithelial Kazal-type–related inhibitor (LEKTI)), it has been
recently shown that pro-inflammatory cytokines such as TNF, are overexpressed [24] as well as the
pro-Th2 cytokine thymic stromal lymphopoietin (TSLP).
11
12
Part II
Thalidomide: an old drug with new clinical applications
Previously published in a shorter form, see appendix 1: Laffitte E, Revuz J. Thalidomide: an old
drug with new clinical applications. Expert Opin Drug Saf. 2004;3:47-56.
1- Introduction
Thalidomide was first synthesized in 1954 by the German pharmaceutical firm Chemie Grünenthal,
and marketed in Europe in October 1957 as an antiemetic and nonbarbiturate sedative hypnotic
[25]. The first pharmacological studies performed on rodents showed a fast sedative effect and
remarkably low toxicity even at high doses. Between 1957 and 1961 thalidomide became widely
used by pregnant women for its anti-emetic effect from morning sickness [26]. A significant
teratogenic effect of thalidomide was reported in 1961 [27] after the rise in reported cases of
phocomelia, a previously exceptional congenital malformation. Nearly 6000 cases of internal or
external deformities were attributed to thalidomide during this period [26, 28] and the drug was
withdrawn from the market. In 1965, a dramatic improvement of erythema nodosum leprosum
(ENL) treated with thalidomide was reported by Sheskin [29], and the discovery in 1991 of
thalidomide’s anti-Tumor Necrosis Factor (TNF)-α activity [30] led to renewed interest in this
drug. Since then, this anti-TNF-α effect has been studied, with several clinical indications under
investigation. There are two main strands to current research: immunomodulatory action in various
inflammatory diseases, and antiangiogenic action which seems to be of interest in oncology.
2- Pharmacology
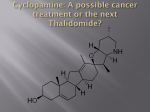
Thalidomide, or α-N-pthalimido-glutarimide, is a glutamic acid derivative (figure 1). The molecule
is a racemic mixture of the S (-) and R (+) isomers. There is some evidence to suggest that the two
enantiomers act differently: the R form could be responsible for the sedative effect [31], while the S
form could have the immunomodulatory, antiangiogenic [32] and teratogenic properties, although
this hypothesis is debatable [33]. However, in human, this difference is not relevant since chiral
interconversion between the two enantiomers leads in vivo to a racemic mixture in two hours [34].
13
Fig 1: Chemical structure of Thalidomide and Lenalidomide. Lenalidomide is a second generation
analogue of thalidomide that shares a similar chemical structure; this drug is found to be 50 000fold more potent in inhibiting TNF in vitro compared to the parent compound (cf infra).
Thalidomide
Lenalidomide
The solubility of this lipophilic molecule is low in water and alcohol, and the molecule is sensitive
to hydrolysis for pH higher than 6 [25, 35].
The pharmacokinetics of thalidomide has been studied both in humans and animals [36-39]. After
oral absorption, the plasmatic peak in healthy volunteers is reached in 3.2 +/- 1.4 to 4.39 +/- 1.27
hours (Tmax) [36, 37]; and is delayed by a high-fat meal [40]. The apparent distribution volume is
very broad: 120 liters [38] with a fast penetration of the hemato-encephalic and placental barriers
14
[41]. Studies in animal showed that thalidomide was distributed in all the tissues with a predilection
for digestive tract and kidneys [42].
The main metabolic pathway is probably non-enzymatic hydrolysis, leading to at least 12
breakdown products; some of them could have their own pharmacological activity [43].
Hydroxylated products have also been detected, suggesting that enzymes from the hepatic P-450
cytochrome family could be involved [44].
Excretion of thalidomide and its metabolites is mainly through the renal route. The plasma half-life
ranges from 6.17 +/-2.56 to 8.70 +/- 4.11 hours [36-38]. Excretion of thalidomide in semen was
studied in rabbits. After two oral doses separated by 18 hours, thalidomide was found in semen
from the sixth hour until the twelfth day. Thalidomide was not only present in the seminal fluid, but
also firmly fixed on spermatozoans [45]. In humans, thalidomide is also present in semen. After an
oral intake of 100 mg/day, thalidomide was detected in semen at week 4 with a correlation between
plasma and semen levels [46].
In a recent study, the pharmacokinetics of a single oral dose of 100 mg or 200 mg of thalidomide
was assessed in 14 asymptomatic HIV-infected men [47]. The results were overall consistent with
those given previously, with respectively for 100 and 200 Mg: Tmax of 2,5+/-1,5 H and 3,3+/-1,4
H, a half-life of 4,6+/-1,2 H and 5,3+/-2,2 H, an apparent distribution volume of 70+/-16 L and
83+/-35 L.
There is no parenteral preparation for thalidomide. The dermal absorption of thalidomide is very
low and this molecule may not be appropriate for topical delivery. Analogues have been
synthesized, and a methyl derivative could have a better dermal penetration [48].
Thalidomide enhances the activity of alcohol, barbiturates, chlorpromazine and reserpine [35, 44],
but does not affect the pharmacokinetics of orally administered hormonal contraceptives [49].
3- Biological properties
3.1 Hypnosedative action
The sedative properties of thalidomide are not well understood. Thalidomide acts by a different
mechanism than barbiturates, possibly involving activation of sleep centers that depend on gammaamino-butyric acid (GABA) receptors [38]. The effect on sleep is very particular, different from all
other hypnotic drugs by increasing the time spent in phase 3-4 and REM (rapid eye movement) and
decreasing the time spent in phase 1 [50]. This sedative action is preferentially related to enantiomer
R(+) [31].
3.2 Immunological properties
Thalidomide is able to modify inflammatory processes and to modulate immune reactions [51].
Many data, sometimes contradictory, are available about the immunomodulating action of
15
thalidomide at the cellular and molecular levels both in vivo and in vitro. Thalidomide’s effects are
clearly different from corticoids, ciclosporine, FK506 or phosphodiesterases inhibitors such as
pentoxifylline [25].
Thalidomide seems to have both an inhibiting and stimulating action on different cellular immunity
effectors. These dichotomous actions may in part be explained by the recently recognized ability of
thalidomide to act as a T-cell co-stimulant under certain circumstances. Thalidomide has an
inhibiting effect on mononuclear cells by decreasing their chemotactism and phagocytosis
capacities [44]. The lymphocytic proliferation induced by allogenic, superantigenic or mitogenic
stimulations is inhibited by thalidomide, with an additive effect by ciclosporine A [44, 52, 53].
Furthermore, thalidomide modulates the balance between the different classes of lymphocytes. In
vitro studies show that the CD8+ cytotoxic response is stimulated compared to the CD4+ response
[54]. An increased CD4+/CD8+ ratio was found in the blood and the cutaneous lesions of patients
with erythema nodosum leprosum (ENL). A inversion of this ratio was observed in some of these
patients treated by thalidomide [55], which could be one of thalidomide’s effects in ENL.
Moreover, thalidomide acts in vitro by skipping the Th1 lymphocyte response towards a Th2 type
[56]. Thalidomide has been shown to enhance production of interleukin (IL) 4 and IL5, promoting
the shift from a Th1 to a Th2 cytokine pattern. This effect could be of interest in various pathologies
associated with a dysregulation of lymphocyte subpopulations [57].
One of the most significant properties of thalidomide is its inhibition of TNF-α synthesis by
activated human monocytes [30]. The mechanism by which thalidomide suppresses TNF-α remains
unclear. It appears to enhance the degradation of TNF-α mRNA [58] and could interact with two
intracellular glycoproteins with anti-TNF-α properties [43]. This anti-TNF-α activity was
confirmed in vivo in patients with ENL, tuberculosis, and in HIV infected patients [59]. However,
contradictory results were obtained both in vitro and in vivo for the anti-TNF-α properties of
thalidomide. Recent data demonstrate that thalidomide may exert a bidirectional dose-dependent
effect on TNF-α production, depending on cell type and method of cellular activation. Thus, under
certain experimental circumstances, TNF-α production is significantly enhanced by thalidomide in
vitro [60]. Furthermore, increased levels of TNF-α in serum have been observed in patients with
toxic epidermal necrolysis treated with thalidomide [61]. It is noteworthy that in this double-blind,
placebo-controlled trial, treatment with thalidomide was associated with an increased mortality.
Increased levels of TNF-α were also observed among HIV-infected patients treated by thalidomide
for oral ulcerations [62].
16
More recently, thalidomide has been shown to inhibit NF-kappa B activation, an ubiquitous
transcription factor of central importance in the response of the host to inflammatory stimuli,
through suppressing I-kappa B kinase activity [51, 63].
Together, these data suggest that thalidomide has a complex action on the immune system: in
conditions characterized by monocyte/macrophage activation and high circulating concentrations of
TNF-α, such as ENL, the use of thalidomide to inhibit production of TNF-α may be beneficial.
However, in diseases where T-cell activation contributes to the pathogenic process, further T-cell
stimulation by thalidomide may be detrimental and result in clinical deterioration [64].
3.3 Anti-angiogenic properties
Anti-angiogenic property of thalidomide was first shown in vivo in a rabbit cornea model [65]. This
property is distinct from the anti-TNF-α action [32], and is probably responsible for the teratogenic
effect [66]. The inhibition of neovascularisation induced by thalidomide is mediated by inhibition of
angiogenic factors such as the vascular endothelial growth factor (VEGF) [67] and basic fibroblast
growth factor (b FGF) [68]. At a molecular level, thalidomide, or a breakdown product of
thalidomide, could decrease the transcription efficiency of genes related to those angiogenic factors
by specifically intercalating into their promoter sites [66]. This inhibition requires metabolic
activation, which is species-dependent [69]. These metabolites can be formed in both humans and
rabbits, but not in some species of rodents in which thalidomide has no antiangiogenic or
teratogenic effects [69].
The anti-angiogenic activity of thalidomide seems particularly interesting in the treatment of
malignancies, where angiogenesis has been shown to play an important role [70, 71]. In
experimental models of tumor and metastases, thalidomide has been shown to induce an
intratumoral hypoxia, to reduce tumor blood vessel density and tumor growth, and to decrease the
risk of metastases [72, 73].
4- Clinical applications
Thalidomide has been used in several cutaneous inflammatory disorders. Its efficiency has been
proved in erythema nodosum leprosum, severe aphtosis- isolated (figure 2), or in Behçet disease- or
associated with HIV infection, Jessner-Kanoff’s lymphocytic infiltration, resistant cutaneous lupus,
and chronic graft-versus-host reactions. Some other dermatological indications may be of interest,
such as prurigo, HIV infection, cutaneous sarcoidosis, chronic or recurrent erythema multiform
(figure 3), and pseudo-lymphomas, or numerous other inflammatory dermatoses in single case
reports [44, 74-76]. Surprisingly, thalidomide is not efficient in psoriasis [77] and in contrary,
exacerbation of psoriasis have been observed with thalidomide [78, 79], illustrating the complexity
17
of this molecule, since some paradoxal elevation of TNF have also been observed in some patients
with toxic epidermal necrolysis [61] or HIV infection [62]. For a more precise description of
clinical applications of thalidomide in dermatology, see appendix 2: Laffitte E, Revuz J.
Thalidomide. Ann Dermatol Venereol. 2000;127:603-13.
Thalidomide has been used in Kaposi’s sarcoma, with inconstant results [80-82]. Together, these
results suggest that thalidomide is not a major therapy for KS, with disappointing response rate and
limitations due to side effects, although it could be useful in some specific cases [83]. For an
editorial on Thalidomide for Kaposi sarcoma, see appendix 3: Laffitte E. Thalidomide in Kaposi
sarcoma: promising or disappointing? Dermatology. 2007;215:171-2.
Considering the good results obtained with the new biologic anti-TNFα compounds, the indication
for the use of thalidomide in other inflammatory diseases, such as rheumatoid arthritis, ankylosing
spondylitis or inflammatory bowel diseases are still under debate [84].
Thalidomide has been shown to be an active and promising anti-carcinogenic agent, as a single
agent or in combination with dexamethasone or other chemotherapeutic agents, in hematological
malignancy, such as relapsing or refractory multiple myeloma, myelodysplasia or acute myeloid
leukemia (well reviewed in [70, 85]), and also in solid tumor such as malignant glioma, prostatic,
colorectal or renal cell carcinoma [70]. The best response rates have been observed with relapsing
or refractory multiple myeloma, ranging from 25 to 69% [85]. Thalidomide could be of interest in
cancer cachexia and for distressing night sweats in advanced malignant disease [86, 87]. The dosage
and length of treatment are different in inflammatory and neoplastic diseases. A daily dose of 200
mg or less is usually enough to control erythema nodosum leprosum, severe aphtosis or cutaneous
lupus, and the dose can progressively be reduced, while in malignancy, thalidomide is started at 200
mg/d an progressively increased to 400-800 mg/d for several months [70, 85].
18
Figure 2: A 18-year old male patient with severe oral aphtosis. He was suffering for severe and
relapsing oral aphtosis since he was 9 years old, unresponsive to oral steroids. When he was 13, he
consulted in our clinic; and we started a therapy with thalidomide, 50 mg daily with a dramatic
improvement in 7 days.
Before thalidomide
After one week of thalidomide, 50 mg daily
Unfortunately, the aphtosis always recurred when the dose was lower than 25 mg twice a week, and
after 5 years of therapy, he developed a sensitive neuropathy. The thalidomide had to be
discontinued, and the aphtosis relapsed, without any response to colchicine.
19
Figure 3: a case of recurrent erythema multiform in a 25-year old woman, resistant to several
month of high dose oral corticotherapy: see painful ulceration of the tongue and oral mucosae
After one week of thalidomide, 50 mg/day: dramatic improvement of all the lesions
20
5- Side effects
Thalidomide’s side effects are listed in table 1, Appendix 1. As the number of patients receiving
thalidomide for longer periods of time and higher dosages increases (in particular for relapsing
multiple myeloma or in HIV patients), several previously unrecognized or underestimated adverse
effects have recently been observed. Some side effects can be considered as major and may have
serious consequences (teratogenicity, peripheral neuropathy and deep venous thrombosis). Some
side effects are usually considered minor, as they tend to appear at the beginning of treatment and
generally disappear after dose tapering. However, they may act as serious dose limiting factors or
lead to treatment interruption when thalidomide is used in higher dosages as an anticarcinogenic
agent (in particular somnolence, constipation and rash). The incidence of each side effect is not
accurately known and tends to vary in different studies, depending on the disease and the
administered dose of thalidomide.
5.1 Toxicity
The acute toxicity of thalidomide is so low that the toxicological studies made in the Fifties in
rodents failed to show lethality, even when in excess of 10,000 mg/kg [25]. Accidental or voluntary
overdosing never had any serious consequences, even for amounts of 14 grams [44].
5.2 Major side effects
5.2.1Teratogenic Effect
The discovery of the teratogenic properties of thalidomide was a surprise, since premarketing
animal studies, only performed in rats [25], did not detect it. Later studies showed that rats or mice
are species less sensitive to teratogenic effect of thalidomide [88, 89].
The major susceptibility of the human embryo seems to be between the 27th and the 50th day after
conception, and a single dose of 100 mg is enough to cause harm [90]. The frequency of
malformations after in utero exposure has been estimated in a range of 15 to 100%. The most
frequent fetal abnormalities seen in humans are limb defects (75% of the cases), but other
abnormalities such as craniofacial abnormalities, malformations of internal organs and central
skeletal abnormalities have been observed [26].
The specific mechanism of this embryopathy is not clear yet, and is probably complex with 24
potential mechanisms of action listed [91]. The most recent data suggest that the embryotoxic
activity could be related to the formation, under the effect of the prostaglandin H-synthetase, a
species-dependent enzyme, of a teratogenic metabolite. This metabolite could induce the production
of free radicals responsible for DNA oxidation in the embryonic cells [92]. The anti-angiogenic
properties of thalidomide may also play a role in teratogenesis [66].
21
There is a potential risk of teratogenic effect of thalidomide in treated male, as the molecule is
distributed into semen. Congenital malformations have been observed in rabbit’s newborn resulting
from breeding experiments with males having a prolonged intake of thalidomide. [45]. Such an
effect has not been described in humans yet, but since thalidomide is distributed into human semen
after oral dosing, there could be a potential risk in treated male patients [46].
The teratogenic effect is currently well controlled in Western countries with the delivery of the
product being restricted by specific control programs (the S.T.E.P.S program and its equivalent in
Europe, the Pharmion Management Risk Program, P.R.M.P) to patients using effective methods of
contraception, and women managed by repeated pregnancy tests. This is not true everywhere in the
world, and at least 34 cases of embryopathy after exposure to thalidomide have been reported in
South American lepromatous endemic areas since 1965 [93].
Nevertheless, one should notice that some other highly teratogenic molecules are frequently
prescribed by dermatologists, such as isotretinoin. It has been demonstrated that approximately 25
to 30 percent of fetuses exposed to isotretinoin have birth defects [94], which makes isotretinoin as
embryotoxic as thalidomide. There are some specific birth control programs associated with
isotretinoin use, such as the S.M.A.R.T program in the United States [95], which are not as heavy or
expensive as the S.T.E.P.S program.
For a discussion of the comparative teratogenic effect, see appendix 4: Laffitte E. Thalidomide,
semen distribution, teratogenicity...and cost. Br J Dermatol. 2006;154:563; author reply 563-4.
The possibility of a mutagenic effect was raised in 1994 by McBride (who had described the
teratogenic effect in 1961) following two observations of limb malformations in children born to
fathers with thalidomide embryopathy [96]. The imputability of thalidomide in the two cases
observed was low, and more than 350 victims of thalidomide indexed in England had normal
children [97-99]. However, large studies were performed in human and other animals, indicating
that thalidomide was devoid of mutagenic activity [100, 101].
5.2.2 Peripheral Neuropathy
As teratogenicity of thalidomide can be controlled by appropriate contraceptive methods, the
neurotoxicity of the drug is now one of the main factors limiting its use for a prolonged period [44,
102], especially in cutaneous inflammatory disorders. The exact mechanism of thalidomide-induced
neuropathy is still unknown. An individual susceptibility has been suggested, but no correlation
with the genetic differences in drug metabolism has been found [103]. Thalidomide neuropathy is
known to be an axonal, bilateral, and symmetrical polyneuropathy, mainly sensory, and particularly
involving distal extremities. Clinical manifestations of thalidomide-induced neuropathy consist
mainly of symmetrical distal painful paresthesia with or without sensory loss in the lower limbs
22
[44]. Electrophysiologic findings are those of a sensory axonal polyneuropathy with reduction of
sensory nerve action potential (SNAP) amplitude and relative conservation of nerve conduction
velocities [104]. A 50% decrease of sural SNAP amplitude has been reported to be the best
electrophysiologic criterion, SNAP amplitude being closely related to the clinical sensory signs and
symptoms [104, 105].
The prevalence of thalidomide-induced neuropathy has been variously estimated in retrospective
studies, from less than 1% in 34 patients treated for lepra reactions [106] to more than 70% in small
series of patients (four to eight) treated for prurigo nodularis [107-109]. A prevalence of 25% was
reported in a series of 60 patients treated for discoid lupus erythematosus during a 2 years period
(400 mg per day, then 50-100 mg per day) [110]. In a retrospective study of 42 patients, a
prevalence rate of definite thalidomide neuropathy of 21% [111] was observed. In recent series of
patients with refractory multiple myeloma treated with high doses of thalidomide, i.e. 200-800 mg
per day, neuropathy was reported to occur in 10% to 30% of treated patients [112, 113], but the
clinical and electrophysiologic criteria for neuropathy were not clearly specified. This variability in
prevalence has been interpreted as reflecting a disease-related susceptibility. In fact the
retrospective nature of the studies, the large range of daily doses used, and the heterogeneity of the
clinical and electrophysiologic criteria considered for the diagnosis of neuropathy preclude a real
estimation of the prevalence rate and risk factors of thalidomide neuropathy. Thalidomide-induced
neuropathy was recently prospectively evaluated among 135 patients treated for various
dermatologic diseases for 2 years [114]. Definite neuropathy (i.e. electrical plus clinical signs) was
present in 25% of the patients but clinical or electrophysiologic evidence of a thalidomide-induced
neuropathy were present in 56% of the patients. The incidence rate was maximal during the first
year of treatment (20%). The risk of neuropathy was related to the daily dose whatever the duration
of treatment and the risk seemed to be negligible for doses less than 25 mg per day, whatever the
duration of therapy. After peripheral neuropathy develops, it resolves slowly and is sometimes
irreversible [111, 115, 116]. In a follow-up of thalidomide-induced neuropathy over 4 to 6 years,
approximately 25% of patients had a full recovery, 25% had a slow improvement, and 50% had
persistent sensory symptoms [111, 115, 116]. In a few patients, recovery did not begin for years.
Sural nerve biopsies showed severe degeneration of large axons with little sign of regeneration. In
other patients, electrophysiologic abnormalities worsened after discontinuation of thalidomide
[104]. The use of thalidomide every other day, alternate weeks, or for brief monthly courses has
been suggested to minimize the risk of polyneuropathy. However, no studies of these alternative
courses have been performed.
It is recommended that a baseline nerve conduction study should be performed in all patients who
receive thalidomide within 3 months of initiating therapy, and then repeated every 6 months
23
thereafter [114]. If nerve conduction amplitudes are decreased by more than 30% from baseline,
more frequent testing is recommended [105]. Thalidomide should be discontinued if nerve
conduction amplitudes are decreased by 50% or more. Thalidomide therapy can be cautiously
restarted after symptoms of neuropathy resolve [102].
5.2.3 Thalidomide and thromboses
As the use of thalidomide expands, the higher incidence of deep-vein thrombosis (DVT) or
pulmonary embolism has been recently reported among patients receiving thalidomide in
combination
with
glucocorticoids
or multiagent
chemotherapy for multiple myeloma,
myelodysplasic syndromes or various carcinomas [117]. The reported rates of these events varied
from 0 to 43% of treated patients and occurred at a mean of 2 months after the introduction of
thalidomide treatment. Ten cases have been reported in patients taking thalidomide for
inflammatory dermatoses, such as lupus or aphthous stomatitis [118-122]. All of these patients had
different predisposing factors, such as antiphospholipid syndrome, trauma or Behçet disease.
In cancer patients DVT were safely treated with anticoagulation and did not necessarily warrant
discontinuation of thalidomide [117]. On the other hand, in patients with inflammatory diseases,
thrombo-embolic events were particularly severe and extensive even after anticoagulation, and
thalidomide had to be discontinued.
There is no clear explanation about the thrombogenic effect of thalidomide, but some hypotheses
have been suggested: thalidomide, chemotherapy, and glucocorticoids could increase activation of
tissue factor in the plasma membrane of tumor cells by way of apoptosis [123]. This phenomenon
could be dose-related, since no case has been recorded during a prospective survey of 170 patients
treated with daily doses of 100 mg or lower [114].
Together, clinical data suggest that thalidomide could have a thrombogenic effect for a daily dose
higher than 100 mg, in patients with predisposing diseases such as multiple myeloma or solid
carcinoma, Behçet disease or antiphospholipid syndrome, and when glucocorticoids or multiagent
chemotherapy are associated, and those patients should be carefully monitored when thalidomide is
started.
5.3 Minor side effects:
The more usual side effects are neuropsychic, digestive, endocrinological and cutaneous.
- neuropsychic in 33 to 100% of the cases [35]: somnolence (45 to 90%), asthenia, drowsiness,
cephalalgias, decreased libido, or depressive syndrome are currently observed. More recently, a
reversible dementia was reported [124].
24
- digestive: constipation (15 to 50%), weight gain (30%), xerostomia, abdominal pain and nauseas
may occur frequently. A severe hepatic toxicity has been reported once [125].
- endocrinological disorders: several studies in the 1950s and 1960s reported the effects of
thalidomide on the endocrine system. More recently, hypothyroidism and significant increases in
serum TSH levels have been found after 2 to 6 months in 20% to 74% of patients treated with
thalidomide for multiple myeloma [126]. Thalidomide therapy can result in constipation, fatigue,
lack of energy and bradycardia, but those signs may also be manifestations of hypothyroidism, and
the authors recommend assessment of serum TSH levels before starting thalidomide and every 3
months afterwards, or if the diagnosis of hypothyroidism is suspected. Secondary amenorrhea has
been reported in ten women treated with thalidomide for aphtosis or lupus [127-130]. The
amenorrhea occurred after 4 to 7 months following the beginning of the treatment, and resolved
after the discontinuation of thalidomide. Reintroduction of thalidomide in two patients again
induced amenorrhea. Increased FSH and LH levels with low estradiol levels were consistent with a
menopausal profile, suggesting a peripheral action rather than central.
- cutaneous side effects: various dermatologic side effects of thalidomide have been reported, but
recently with the use of higher dosage their prevalence appear to be higher than previously expected
[131, 132]. Skin eruptions have been noted in 46% of myeloma patients taking thalidomide alone or
in combination with dexamethasone [131]. Cutaneous side-effects are also more common in HIVinfected patients treated with thalidomide compared to non-infected individuals treated with the
drug. In a series of 56 HIV-infected patients treated with thalidomide for 14-21 days, 27% ceased
thalidomide because of cutaneous side-effects [132].The more immunosuppressed the HIV-infected
individual was, the more likely they were to experience side-effects.
These eruptions can be minor to moderate such as morbilliform or maculopapular rash, but severe
skin reaction (DRESS (Drug Rash with Eosinophilia and Systemic Symptoms) [133], exfoliative
erythroderma [134], erythema multiform or toxic epidermal necrolysis [131, 135]) have been
observed.
6- Guidelines for the clinical use of Thalidomide
Thalidomide is currently available only on special access schemes that differ from country to
country. Clinical use is restricted to severe disabling conditions that cause an unacceptable
interference with normal life, and only after other treatments have been tried and failed. Approval is
usually on an individual patient basis. Thalidomide is prescribed in an off-label setting in most
countries. In France, thalidomide has been approved since February, 1997 for erythema nodosum
leprosum, Jessner-Kanoff’s lymphocytic infiltration, resistant cutaneous lupus, chronic graft-versushost reactions, severe aphtosis either isolated or associated with Behçet disease and HIV infection,
25
and more recently resistant multiple myeloma. In the US, thalidomide has been approved since July,
1998 for erythema nodosum leprosum.
Thalidomide is available as capsules of 50 mg. Until 2008 it was distributed in Europe by
Pharmion, which had a monopole of the distribution in Europe. Since 2008, the CELGENE company
bought Pharmion laboratories, and now distributes Thalidomide (and that its derivative,
lenalidomide) in the entire world. To prevent pregnancy under thalidomide, an extremely strict
control program as been established since 2004, the Pharmion Risk Management Program (PRMP)
(except France), similar to the U.S. Program (STEPS), which has been previously described and
published [136]. This program requires an extensive infrastructure, is time-consuming and requires
laborious inputs from prescriber, patient and pharmacist. As a consequence, the price of the drug
has increased 400 per cent now with a price of approximately 14 Euros for a 50 mg capsule (2.52
Euros before 2003).
Before treatment, patients must be informed of the risks associated, side effects, and the nature of
any alternative treatments using registered drugs. Patients should be in a position to make informed
consent and be given a detailed information sheet about the drug. In women of childbearing age,
pregnancy should be excluded with a negative test prior to prescribing. If hormonal contraceptives
are the chosen means of preventing pregnancy while taking thalidomide, the hormones should be
taken for at least 1 month prior to commencing thalidomide. Men taking thalidomide should be
advised to wear condoms during sexual intercourse as thalidomide has been detected in semen.
Clinical neurological examination and electrophysiological measurements are to be recorded when
treatment is started. Risk factors for thrombo-embolism should be recorded, and TSH levels should
be determined.
During treatment, pregnancy tests and clinical neurological examinations should be performed
monthly. Monthly and electrophysiological measurements every 6 months must be performed.
Patients must be educated about the symptoms of peripheral neuropathy and instructed to consult
their doctor for electrophysiological testing in the event that such symptoms appear.
After cessation of thalidomide, pregnancy should be avoided for one month in women, and
condoms should be continued for 3 months in men (corresponding to a spermatogenesis cycle).
26
7- Thalidomide on internet
Several websites can be consulted on the net:
- The Thalidomide Victims Association of Canada. URL Address: http://www.thalidomide.ca
- US Food and Drug Administration/Center for Drug Evaluation and Research. The information
presented on this page includes consumer and patient information, thalidomide advisory committee
and workshop transcripts, the approved labeling text and the medical review on which the decision
to approve this drug was based. Also included are selected links to other web sites containing
thalidomide information.
URL Address: http://www.fda.gov/cder/news/thalinfo
- Thalidomide: potential benefits and risk, open public scientific workshop, convened on September
9 and 10, 1997, by the National Institutes of Health (NIH), the Food and Drug Administration
(FDA), and the Centers for Disease Control and Prevention (CDC)
URL Address: http://www.fda.gov/oashi/aids/thalexe.html
8- The future? Thalidomide derivatives and lenalidomide in dermatology
8.1 Lenalidomide: the second generation imid
With the “rediscovery” of thalidomide, several structural analogues have been developed in an
attempt to find compounds with thalidomide’s immunomodulatory properties without the associated
side effects [137, 138]. Preliminary results from human studies in vitro and in vivo have shown
some of these compounds to be clinically effective with reduced toxicity, but they are still under
investigation [139, 140]. In particular, lenalidomide (Revlimid®), a second-generation thalidomide
derivative has been extensively studied (figure 1). Lenalidomide was identified as more potent than
thalidomide and devoid of many of the serious adverse reactions associated with thalidomide
administration, such as neuropathy [141] or teratogenicity (in rabbit) [142]. Many potential
mechanisms of action exist for lenalidomide, including inhibition of angiogenesis, enhancement of
immune system function, inhibition of tumor stromal cell interactions, and blockade of actions of
various cytokines [141].
There is appreciable clinical activity of this drug in hematologic malignancies including
myelodysplastic syndrome, multiple myeloma, and chronic lymphocytic leukemia (CLL).
27
8.2 Lenalidomide in dermatology
In dermatology, there are only anecdotal reports of lenalidomide use: an oral aphtosis was cleared
with 10 mg/d of lenalidomide in a patient with Behçet disease [143] but was complicated by a deep
venous thrombosis, and good clinical response was obtained in two patient with resistant discoid
lupus erythematosus [144]. In 15 patients with cutaneous T-cell lymphoma receiving 25 mg of
lenalidomide daily for 21 days of a 28-day cycle, 5 patients have achieved a partial response and 6
patients have experienced minor responses such as regression of cutaneous tumor lesions, improved
lymphadenopathy, and skin improvement [145]. However, the actual extremely high price of this
drug (8789.00 CHF for 21 capsules of 25 mg), which is even higher than the current TNF inhibitors
(cf infra) will probably not contribute to his prescription for non hematologic diseases.
Some cutaneous side effects have been described in up to 30 % of the patient with lenalidomide
given for hematological malignancy, with mild to moderate morbilliform or urticarial rash, which
did not require the discontinuation of the drug [144]. More severe reaction have been reported: two
cases of acute neutrophilic dermatoses suggesting Sweet syndrome [146, 147], and 12 reports of
Stevens Johnson syndrome, three reports of erythema multiform and one report of toxic epidermal
necrolysis among approximately 57,000 patients who received lenalidomide from market launch on
December 2005 through June 2008 [148].
8.3 Our experience with lenalidomide in cutaneous disorders
We have recently treated two patients with lenalidomide that was given by Celgene Company as
compassionate use:
- One patient followed for a disfiguring non Langerhans-cell cutaneous histiocytosis, type xanthoma
disseminatum of Montgommery, with a doubtful association with a low-grade cutaneous T cell
lymphoma. After three cycles of 15 mg/days during the first 21 days of a 28-day cycle, there was no
clinical response and the patient experienced side effects as a cutaneous rash following the second
cycle and abdominal pain with diarrhea.
- A patient suffering for a severe scleromyxedema associated with a benign monoclonal
gammopathy since 7 years. According to the literature, intravenous immunoglobulin and
thalidomide are therapeutic options [148, 149]. This patient had already had 3 infusions of
immunoglobulin several years ago, with only a partial response, and was suffering for a bilateral
Carpal tunnel syndrome which is a compression of the median nerve at the wrist, that was a relative
contra-indication to thalidomide. As the disease was related to the monoclonal gammopathy, we
used the dose of Revlimid we would use to treat a myeloma, i.e. 25 mg/d during the first 21 days of
a 28-day cycle. After two cycles, a slight clinical response was observed.
28
Part III
The new era: Biologics as Tumor Necrosis Factor antagonists
1- Introduction
The discovery of the major role of TNF in the physiopathology of certain inflammatory diseases
and notably in rheumatoid arthritis and Crohn's disease has led to the emergence of new anti-TNF
drugs [8, 9]. The anti-TNF currently available are etanercept, a fusion protein composed of a
soluble TNF alpha receptor, infliximab, a chimeric monoclonal antibody and adalimumab, a fully
human IgG1 monoclonal antibody that binds with high affinity and specificity to TNF [13]. These
new therapeutic arms issued from bio-technology, so-called biological therapies (biologics) have
rapidly demonstrated their efficacy in the treatment of various inflammatory diseases [10, 11]. In
particular, these drugs have revolutionized the treatment of psoriasis and may benefit for other
cutaneous diseases, such as granulomatous diseases, Behçet’s disease or hidradenitis suppurativa
[10, 11].
However, these promising new treatments, although expensive, and with yet unknown long term
side effects, justify rigorous assessment of their efficacy and tolerance in each indication. We will
discuss the role of these anti-TNF biologics in psoriasis and other cutaneous diseases, and highlight
some side effects specific to dermatology, the other side effects of anti-TNF have been extensively
described in several reviews [11, 150-153].
2- TNF antagonists used in dermatology: Etanercept, Infliximab Adalimumab (figure 1)
2.1 Etanercept
Etanercept (Enbrel®) is a recombinant human TNF-receptor fusion protein that antagonizes the
effects of endogenous TNF by competitively inhibiting its interaction with cell-surface receptors
[149]. Etanercept is composed by 2 molecules of the extracellular domains of the p75 TNF receptor
and the constant fragment of IgG1. In vitro analyses indicate a reduced stability of etanercept-TNF
complexes compared with infliximab-TNF complexes as well as a remaining biologic activity of
TNF released from the etanercept-TNF complexes. Although etanercept contains the Fc portion of
IgG1, it does not appear to fix the complement. It is also speculated that, because of the different
binding properties of etanercept compared with infliximab, the former is unlikely to form
29
aggregates on the surface of TNF-producing cells that can activate complement-dependent lysis and
antibody-dependent cell-mediated cytotoxicity [150]. Adalimumab and infliximab induce apoptosis
of activated cultured peripheral monocytes and cells presenting the transmembrane form of TNF,
whereas etanercept does not. In humans, higher avidity and better stability of membrane-bound
TNF was demonstrated with anti-TNF mAb (infliximab and adalimumab) than with etanercept,
which leads to more efficient apoptosis [151]. This difference in reverse signalling attributable to a
difference in membrane-bound TNF targeting may have other consequences. For example, antituberculosis–specific T cells show a clear difference in effector function. Two in vitro studies
provided the same results: adjunctive infliximab or adalimumab treatment to specific human antituberculosis T cells was much more efficient in decreasing proliferation and interferon-gamma
secretion by these T cells than was adjunctive etanercept treatment [151, 152].
These data suggest that adalimumab and infliximab have a better ability for granuloma disruption
than etanercept. This may explain the lower efficacy of etanercept in granulomatous diseases such
as Crohn’s disease or sarcoidosis (cf infra), but also a lower risk for granulomatous infections such
as tuberculosis [153]. In Switzerland, etanercept is approved for the treatment of rheumatoid
arthritis, juvenile arthritis, psoriatic arthritis, ankylosing spondylarthritis, and chronic plaque
psoriasis after failure of phototherapy, and systemic treatment such as methotrexate or ciclosporine.
Etanercept is applied in the therapy of plaque psoriasis subcutaneously (SC) at a dose of 25 mg
twice weekly for cycles of 24 weeks only. For the first 12 weeks of treatment, the dosage may be
doubled to 50 mg twice weekly.
2.2 Infliximab
Infliximab (Remicade®) is a chimeric monoclonal antibody [149]. The variable regions are of
murine origin and are coupled to human IgG1 and κ Fc domains. Infliximab binds to all forms of
soluble and membrane-bound TNF with high specificity. The ability of infliximab to bind to
membrane-bound TNF appears to be linked to additional effects on TNF–producing cells
(apoptosis, complement lysis, antibody- dependent cellular cytotoxicity), which have been
described in vitro and in vivo [154] and have been proposed to contribute to the clinical efficacy of
the drug.
Infliximab (Remicade®) is administered as a short intravenous infusion over at least 2 hours at a
total dose of 5 mg/kg body weight. According to the label for plaque psoriasis, infusions are given
at weeks 0, 2, and 6 at the beginning and then every 8 weeks for maintenance therapy. In psoriasis,
infliximab is indicated for monotherapy, whereas in rheumatologic conditions, infliximab is often
used in combination with methotrexate, a regimen that has not been investigated systematically in
psoriasis yet. In Switzerland, infliximab is approved for the treatment of rheumatoid and psoriatic
30
arthritis, ankylosing spondylarthritis, Crohn's disease, and chronic plaque psoriasis after failure of
phototherapy, systemic treatment such as methotrexate, and after etanercept and adalimumab.
2.3 Adalimumab
Adalimumab (Humira®) is a fully human IgG1 monoclonal antibody that binds with high affinity
and specificity to TNF [149]. Like infliximab, adalimumab neutralizes the biologic activities of
TNF by blocking its interactions with the p55 and p75 cell surface receptors, thus modulating TNFdependent biologic responses. Binding properties of adalimumab are similar to those of infliximab.
Less is known about the ability of adalimumab to induce cell-depleting effects, but based on
structural similarities to infliximab, it is conceivable that adalimumab may induce apoptosis,
complement lysis, and antibody dependent cellular cytotoxicity.
Adalimumab is applied for plaque psoriasis as monotherapy at a dose of subcutaneously 40 mg eow
after a loading dose of 80 mg at week 0.
In Switzerland, infliximab is approved for the treatment of rheumatoid and psoriatic arthritis,
ankylosing spondylarthritis, Crohn's disease, and chronic plaque psoriasis after failure of
phototherapy, systemic treatment such as methotrexate or cyclosporine.
Figure 1: Mechanism of anti-TNF biologics. Etanercept is a recombinant human TNF-receptor
fusion protein that antagonizes the effects of soluble TNF (sol TNF) while Infliximab and
Adalimumab are monoclonal antibodies that bind to all forms of soluble and transmembrane TNF
tmTNF
Activated
macrophage
Infliximab
Adalimumab
TNF-RI: p55
Etanercept
Target
cell
solTNF
Infliximab
Adalimumab
TNF-RII: p75
Adapted from: Margolies GR, et al. In: Strand V, et al, eds. Novel Therapeutic Agents for the Treatment of Autoimmune Diseases. Monticello, NY: Marcel Dekker; 1997:141-153.
31
3- TNF antagonists in psoriasis
Treatment strategies for psoriasis include topical treatments, phototherapy, and systemic therapies
including methotrexate, cyclosporine, acitretin and biologic agents [155]. Patients with mild disease
may benefit from topical agents and phototherapy. Systemic treatments are limited to patients with
moderate-to-severe psoriasis in whom the activity of skin lesions and concurrent symptoms cannot
be sufficiently controlled with topical treatments and with phototherapy. Since 2000, moderate to
severe plaque psoriasis has been identified as a target disease by the pharmaceutical industry for the
development of anti-TNF agents. Several big and well-designed clinical studies, with hundreds of
patients have been performed, showing the efficacy of these drugs, with an acceptable tolerance
profile. Noteworthy, TNF inhibitors have been much better studied in psoriasis than the classical
(and much less expensive) systemic therapies, methotrexate and cyclosporine. In the meantime,
several epidemiological studies were done in an attempt to prove that psoriasis was a disease severe
enough to justify the extremely high cost of these new drugs.
3.1 Identification of psoriasis as a severe disease; cost of illness in Switzerland
Psoriasis is a disease affecting approximately 2% to 3% of the population in Western countries
[156]. Among several clinical phenotypes chronic plaque-psoriasis is most frequent and accounts
for about 90% of cases [156]. Psoriasis may cause substantial problems in everyday life with
significant impairment of quality of life [157], and several studies suggested that patients with
severe psoriasis have an increased risk for cardiovascular disease, depressive illness, and a
decreased life expectancy [159-163]. Currently incurable, psoriasis causes remarkable direct costs,
work limitations and productivity loss [164-166].
In 2007, we have participated to a Swiss study initiated in order to estimate the impact of psoriasis
in terms of resources used, associated costs, and quality of life impairment. We concluded that
moderate-to-severe psoriasis is associated with significant impact on quality of life and at least 4fold higher costs than mild psoriasis, indicating need for efficient control of the disease. This costof-illness study provides specific health economic data for further healthcare decision making,
particularly with the advent of new therapeutic agents for effective psoriasis control.
For the full text of the study, see Appendix 5: Navarini A, Laffitte E, Conrad C, Piffaretti P,
Brock E, Ruckdaeschel S, Trüeb R. Cost-of-illness in patients with psoriasis in Switzerland. Swiss
Med Wkly. 2009. in press
3.2 Treating chronic plaque psoriasis with biologics
The three TNF inhibitors used in psoriasis, etanercept, infliximab and more recently adalimumab
have been evaluated as monotherapy for chronic plaque psoriasis. Some tools have been used to
evaluate and compare their efficacy: the Body Surface Area (BSA), the Physican Global
Assessment (PGA) and the more precise Psoriasis Area and Severity Index (PASI) which evaluate
32
the erythema, infiltration, desquamation and surface of the psoriatic lesion. Clinical improvement is
measured by the percentage change in PASI score, and drug approval often depends on a 50%
improvement in the baseline PASI score, also known as a PASI 50; but the main objective is the
PASI 75 after 12 or 24 weeks, which reflect a significant improvement of the disease [158].
Several clinical trials have been performed since 2000 with etanercept, infliximab or adalimumab;
the results of these trials are well summarized in different recent reviews [149, 155, 159, 160]. Most
of these trials are not comparative, but are testing the drug against placebo. There is no head to head
comparative study with the different TNF inhibitors, and it is difficult to rank these drugs according
efficacy in plaque psoriasis. However, infliximab is remarkable for the rapidity of clinical response.
At week 10-12, infliximab (5 mg/kg) seems to be slightly more effective than adalimumab (40
mg/eow), and more effective than etanercept (100 mg/w) and etanercept (50 mg/w) with 75 to 80%,
71 to 79%, 49% and 34% of patients achieving PASI 75, respectively [170-175]. Only one recent
trial compares adalimumab to methotrexate (15 to 22.5 mg/w), which obtains 35 % of patients
achieving PASI75 [174].
Some long term data are now available, suggesting that there could be a lost of efficacy, at least for
infliximab when used in monotherapy and in an intermittent schedule, and etanercept which is more
efficient when used 50 mg BIW compare to 25 mg BIW [161]. For these three drugs, a long term
use in a continuous way is probably more efficient than an intermittent therapy.
3.3 Treating other forms of psoriasis with biologics
TNF inhibitors have been used with success in other form of psoriasis: psoriatic arthritis [149],
erythrodermic [162], generalized pustular psoriasis [163], recalcitrant subcorneal pustular
dermatosis (Sneddon-Wilkinson disease) [164] acrodermatitis continua of Hallopeau [165] and nail
psoriasis [173].
See appendix 6: Laffitte E, Dudler J, Panizzon RG. Psoriasis unguéal et traitements anti-TNFα.
Ann
Dermatol
Venereol
2004;131:1S71-1S272
and
presented
as
poster
in
Journées
Dermatologiques de Paris, 7-11 December 2004.
There are also some data suggesting that antiTNF can be use in patients with chronic C hepatitis.
See appendix 7: Laffitte E, Kunzle N, Mottet C, Panizzon RG. Severe psoriasis with chronic active
hepatitis C: treatment by etanercept. Brit J Dermatol 2006;154 :25, and presented as poster in 4th
International Congress on Psoriasis - From Gene to Clinic, London, 4-6 December 2006.
3.4 Practical use in Switzerland
In Switzerland, the first TNF inhibitor reimbursed by health insurances for plaque psoriasis was
etanercept in 2006, followed by adalimumab in 2008 and infliximab in 2009. Given the high cost of
these drugs compare to classical therapies (Figure 2), there are some obvious prescription
restriction by health authorities. Etanercept and adalimumab are approved for moderate to chronic
33
plaque psoriasis (with a definition of BSA>10 or PASI >10) after failure or contra-indication of
phototherapy, and systemic treatment such as acitretin, methotrexate or ciclosporine. Infliximab is
approved after failure of etanercept or adalimumab. CF table 1 for a synoptic view of TNF
inhibitors use in Switzerland.
Figure 2: Comparative cost of one year of therapy for chronic plaque psoriasis. Price are in Swiss francs.
48052
Adalimumab 40mg/w
36200
Infliximab 8 infusions/y*
31550
Etanercept 2x50/w 3 mo then 2x25/w
25650
Etanercept 2x25/w
Adalimumab 40 mg/eow
24026
Ciclosporine 5 mg/kg/d
4200
Acitretin 35 mg/d
1795
Phototherapy 25 sessions
1275
MTX 20 mg/w SC
904
MTX 20 mg/w oral
181
0
10 000 20 000 30 000 40 000 50 000
* For infliximab, price indicated is for the drug only, excluding the infusion cost
34
From Navarini AA, Kuenzli S, Yawalkar N, Laffitte E, Trüeb RM. Biothérapies du psoriasis en plaques modéré à sévère. Dermatologica Helvetica 2009 ;10 :15-16
Agent
Nom générique
Molécule
Fabricant
Enbrel®
Etanercept ETA
Wyeth / Pfizer
Mécanisme d'action Protéine de fusion recombinante
du récepteur du TNFα, se liant à
la forme soluble et membranaire
du TNF-α.
Indications
Psoriasis en plaques,
dermatologiques
rhumatisme psoriasique.
(Compendium 09)
Psoriasis infantile (en cours).
Garantie SVK
oui
Degré de sévérité
PASI >10 / BSA >10 / DLQI
>10 avec une efficacité
insuffisante de la photothérapie
ou d’un traitement systémique.
Forme
Seringue pré-remplie (25, 50mg)
d’administration
Bilan initial
FSC, ASAT/ALAT, CRP, HBsAg, HBs-Ac, HBc-Ac, HCVScreening, HIV,
Quantiferontest, Rx thorax f/p.
β-HCG urinaire.
Voie
d'administration
Dosage
Latence moyenne
d’effet
PASI 75 :
(comparaison
directe n’est pas
possible car il n’y
pas d’étude
comparative)
Coût:
Humira®
Adalimumab ADA
Abbott SA
Anti-IL12/23
(Stelara®)
Ustekinumab
Centocor / Janssen-Cilag
Anticorps monoclonal
humanisé IgG1 se liant au
TNF-α soluble et
membranaire. Lyse cellulaire.
Psoriasis en plaques,
rhumatisme psoriasique.
Anticorps monoclonal IgG1
humanisé se liant à la sousunité p40 des Il-12 et IL-23.
oui
PASI >10 / BSA >10 / DLQI
>10 avec efficacité insuffisante
photothérapie ou d’un
traitement systémique.
Seringue pré-remplie et pen.
en cours
Probablement identique aux
autres anti-TNF-α.
Solution en fiole.
FSC, ASAT/ALAT, CRP,
HBs-Ag, HBs-Ac, HBc-Ac,
HCV-Screening, HIV,
Quantiferontest, Rx thorax f/p.
β-HCG urinaire.
FSC, ASAT/ALAT, CRP,
HBs-Ag, HBs-Ac, HBc-Ac,
HCV-Screening, HIV,
Quantiferontest, Rx thorax
f/p. β-HCG urinaire.
s.c.
Anticorps monoclonal
chimérique IgG1 se liant au
TNF-α soluble et membranaire.
Lyse cellulaire.
Psoriasis en plaques, rhumatisme
psoriasique.(USA: érythrodermie
psoriasique)
oui
PASI >10 / BSA >10 / DLQI
>10 avec une efficacité
insuffisante de l'Enbrel ou de
l'Humira.
Poudre lyophilisée pour injection
intraveineuse (2 heures)
FSC, ASAT/ALAT, CRP,
HBs-Ag, HBs-Ac, HBc-Ac,
HCV-Screening, HIV,
Quantiferontest, Rx thorax f/p.
Chez la femme en âge de
procréer: β-HCG urinaire,
contraception jusqu'à 6 mois
après
i.v.
s.c.
s.c.
2x25mg/sem ou 1x50mg/sem.
En cas d'atteinte sévère ou
d'obésité: 2x50mg/sem pendant
12 sem. 0.8mg/kg/sem en
4-8 sem
5mg/kg @ sem 0,2,6, puis toutes
les 8 sem. Traitement combiné
avec MTX low-dose (10
mg/sem) recommandé.
1-4 sem
80mg @ sem 0, puis 40mg @
sem 1, puis 40mg toutes les 2
sem.
45mg @ sem 0, 4 puis. tous
les 3 mois.>100kg 90mg.
2-4 sem
Sem 12: 34% (2x25mg) / 49%
(2x50mg). Sem 24 adultes:
44%(2x25mg),
71% (1X50mg)
75-80% (sem 10)
4-8 sem (sem 4: amélioration
moyen du PASI: 57%)
71-79.6% (sem 16)
2 x 25mg ou 1 x 50mg: 25'711
CHF / an
26750-35'667 CHF / an
(seulement médicament pour
poids de 60-80kg)
non
28'030 CHF / an
Pas connu
à éviter
à éviter
@ sem 2 avant perfusion, @ sem
6 avant perfusion puis toutes les
8 sem
FSC, CRP, ASAT/ALAT (max
3x N)
PASI
23.3%, perte d'efficacité
possible.
@ sem 4,8,12 puis tous les 3
mois
@ sem 4 puis tous les 3 mois
FSC, CRP, ASAT/ALAT (max
3x N)
PASI
8.8%, perte d'efficacité
possible.
FSC CRP, ASAT/ALAT
(max 3x N.)
PASI
5%, perte d'efficacité
possible
Fenêtre
thérapeutique
Intervalle de
monitoring:
oui
Suivi biologique
FSC, CRP, ASAT/ALAT (max
3x limite sup.)
PASI
6%, pas de perte d'efficacité
Suivi clinique:
Anticorps
neutralisants
Anti-TNF-α
Remicade®
Infliximab IFX
Centocor / Essex
Aucun selon Compendium.
Mois 1, M 3, puis tous les 3 M
Psoriasis en plaques: CH: en
cours
66.7-67.1% (45mg, sem 12)
66.4-75.7% (90mg, sem 12)
35
Agent
Contre-indications:
Effets indésirables
(liste non
exhaustive, non
triés par ordre de
fréquence,
imputabilité pas
nécessairement
prouvée)
En cas de HBV
En cas de HCV
En cas de VIH
Interactions
En cas de TB
latente
Carcinogénèse
Enbrel®
Insuffisance cardiaque NYHA
III-IV, grossesse et
allaitement, infection, vaccins
vivants. Néoplasie, maladie
démyélinisante (y compris
familiale), maladies
autoimmunes.
Réactions au site d'injection
(par ex. érythème,
démangeaison en cas
d’allergie au latex), Infection
des voies respiratoires:
(pharyngite à streptocoques
chez l'enfant), prurit,
thrombo-cytopénie, urticaire,
angioedème, lupus, SEP,
vasculite, pustulose palmoplantaire, exanthème
psoriasiforme (1-5%),
psoriasis pustuleux, éruption
lupus-like , toxidermie.
Oui sous Lamivudine 3 mois
avant le début du traitement et
pendant le traitement,. HBVDNA et tests hépatiques tous
les 2 mois (avec
gastroentérologue).
Oui, contrôler la charge virale
après 2 mois, en cas
d'augmentation >20%: stop
traitement
En cours d'évaluation, pourrait
augmenter CD4
Anakinra, Abatacept
Remicade®
Insuffisance cardiaque NYHA IIIIV, grossesse et allaitement,
infection, vaccins vivants,
cytopénie, hépatopathie, néoplasie,
maladie démyélinisante (y compris
familiale), maladies autoimmunes.
Allergie aux anticorps murins.
Infection virale et bactérienne
(50% des décès annoncés), fièvre,
maladie sérique, maladie
autoimmune, lupus-like, cytopénie,
céphalées , vertige, exacerbation
d'une maladie démyélinisante,
flush, troubles gastro-intestinaux,
hépatopathie, exanthème, prurit,
réaction de perfusion (jusqu'à
l'anaphylaxie), éruption
psoriasiforme , réactivation d'une
infection opportuniste, carcinome
épidermoïde.
Humira®
Insuffisance cardiaque NYHA
III-IV, grossesse et allaitement,
infection, vaccins vivants.
néoplasie, maladie
démyélinisante (y compris
familiale), maladies
autoimmunes.
Réaction au site d'injection (16%
vs 10% contre Placebo), fièvre,
asthénie, pneumonie, infection
virale et bactérienne, cytopénie,
lupus, angioedème,
engourdissement (y compris
vertige), céphalées, troubles
neurologiques sensitifs
(paresthésie), perturbations des
enzymes hépatiques. Rarement:
SEP, PF, lymphome, tumeurs
solides (seins, ovaires,
testicules), carcinome
épidermoïde cutané, mélanome.
Oui sous Lamivudine 3 mois avant Oui sous Lamivudine 3 mois
le début du traitement et pendant le avant le début du traitement et
traitement. HBV-DNA et tests
pendant le traitement,. HBVhépatiques tous les 2 mois (avec
DNA et tests hépatiques tous les
gastroentérologue).
2 mois (avec gastroentérologue).
(Stelara®)
HBV, HCV, HIV, TB,
infection active,
néoplasie, grossesse et
allaitement, vaccins
vivants,
immunosuppression.
Infections des voies
respiratoires supérieures,
nasopharyngite,
érysipèle, dépression,
vertige, céphalées,
douleurs pharyngées,
congestion nasale,
diarrhée, prurit,
dorsalgies, myalgie,
asthénie, érythème au
site d'injection
Données insuffisantes.
Données insuffisantes.
En cours d'évaluation.
Oui avec monitoring des
fonctions hépatiques et JHCVRNA, avis d'un
gastroentérologue.
En cours d'évaluation.
Anakinra, Abatacept
Anakinra, ev. Abatacept.
Données insuffisantes.
Oui avec monitoring des fonctions
hépatiques et JHCV-RNA, avis
d'un gastroentérologue.
Sous INH et Benadon pendant Sous INH et Benadon pendant 9
9 mois. Traitement possible
mois. Traitement possible après 1
après 1 mois d'INH.,. Le
mois d'INH,
mieux documenté dans cette
situation.
Les inhibiteurs du TNFα n'augmentent pas le risque de néoplasie [166], hormis les tumeurs cutanées
épithéliales et ev. les hémopathies
Données insuffisantes.
Le traitement d'une TB
latente doit être effectué
avant l'initiation du
traitement.
Risque de néoplasie n'est
pas augmenté (phase III
population d’étude)
36
4- Side effects: some dermatological particularities
Although TNF inhibitors are generally well-tolerated, notable side effects have been reported
including injection reactions (or infusion reactions for infliximab), a risk of serious infections,
including tuberculosis or pneumocystis pneumonia, demyelinating disorders, such as multiple
sclerosis or optic neuritis, a possible increased risk of lymphoproliferative malignancies,
autoimmune diseases such as cutaneous lupus or lupus like syndrome, vasculitis, rare cases of
pancytopenia, aplastic anaemia, and aggravation of congestive heart failure. These “classical” side
effects have been extensively described in several reviews [11, 150-153, 196] and we will focus in
this work on specific and less often described side effects in dermatology.
4.1 Infections: tuberculosis and tuberculosis screening in psoriasis patients
Anti-TNF treatment increases markedly the risk of reactivating latent tuberculosis (LTBI), but very
few data are available in psoriasis patient. We have conducted a study, in which we retrospectively
compared the results of the tuberculin skin test (TST) and the T-SPOT.TB interferon gamma release
assay (IGRA) to risk factors of LTBI in 50 psoriasis patients before anti-TNF treatment [167].
Ninety percent of the patients had prior vaccination by BCG. T-SPOT.TB was strongly associated
with a presumptive diagnosis of LTBI (OR: 7.43; 95% CI 1.38-39.9), which was not the case for the
TST. Agreement between T-SPOT.TB and TST was poor κ= 0.33 (SD: 0.13). LTBI was detected
and treated in 20% of the patients. In 20% of the cases, LTBI was not retained in spite of a positive
TST in front of a negative T-SPOT.TB. All patients received an anti-TNF for a median of 56 weeks
(range: 20-188); among patients with TST+ /T-SPOT.TB-, no tuberculosis was detected with a
median follow-up duration of 64 weeks (range: 44-188). One case of disseminated TB occurred
after 28 weeks of adalimumab in a patient with LTBI in spite of LTBI treatment with rifampicine.
This study is the first to underlines the frequency of LTBI in psoriasis patients (20%), and to
support the use of IGRA instead of TST for its detection. Nevertheless, there is still a risk of
tuberculosis under anti-TNF even if LTBI is correctly diagnosed and treated.
For the complete paper, see appendix 8: Laffitte E, Janssens JP, Roux-Lombard P, Thielen AM,
Barde C, Marazza G, Panizzon RG, Saurat JH. Tuberculosis screening in patients with psoriasis
before antitumour necrosis factor therapy: comparison of an interferon-gamma release assay vs.
tuberculin skin test. Br J Dermatol 2009;161:797-800.
4.2 Cutaneous inflammatory side effects
Various and unexpected cutaneous side effects have been described with TNF inhibitors in patients
treated for rheumatic diseases or Crohn’s disease: eczematiform and atopic dermatitis like
eruptions, paradoxal onset of psoriasis with palmoplantar pustulosis, and some other and less
frequent cutaneous side effects [196, 198].
37
4.2.1 Eczematiform and atopic rash
Itchy eczematous rashes or atopic dermatitis-like eruptions have been described with the 3 TNF
blockers [198-200]. In all cases, the skin lesions were located primarily on the extremities within
the antecubital and popliteal fossae, but also in the face or trunk area (Figure 2). The eruption
usually occurs several months after the beginning of the therapy, may improve after cessation of the
drug, and switching of anti-TNF is not always associated with recurrence of the eruption. The
mechanism of these eruptions is poorly known. It is probably not an allergic reaction to the drug,
since these lesions are late, but rather a cytokine imbalance induced by the anti-TNF, leading to the
induction of an inflammatory skin reaction resembling to eczema with proTh2 cytokines.
Conversely, TNF blockers have been used to treat some severe cases of atopic dermatitis [168].
For one of the first published case, see appendix 9: Dumont-Berset M, Laffitte E, Dudler J,
Panizzon RG. Eczematous drug eruption after infliximab. Br J Dermatol 2004;151:1272-3.
4.2.2 Palmoplantar pustulosis and paradoxical psoriasis
Currently there are more than 200 reports of patients presenting new-onset and worsening of
psoriasis during TNF blockade therapy, well reviewed in [169-171]. Psoriasis occurring during
TNF blockade has been mostly reported as the pustular type occurring on the palms and soles
(Figure 3), but also generalized. This eruption can occur at any time from days to years after drug
initiation but generally after several month of therapy, and some authors suggest that the incidence
may be higher in patients treated with adalimumab [203]. This phenomenon has been reported in
nearly all diseases treated with TNF antagonists, including psoriasis, rheumatoid arthritis,
ankylosing spondylitis, and other seronegative spondylarthritides, including psoriatic arthritis,
Behçet’s disease, inflammatory bowel disease, and juvenile idiopathic arthritis. The majority of
patients were reported to have an excellent therapeutic response to the drug, with the exception of
the unexpected development of psoriatic skin lesions. The evolution of TNF-blockers induced
psoriasis is unpredictable: stopping the drug or switching to another agent leads inconstantly to
improvement of the eruption.
Despite different mechanisms of action of these agents, the lack of resolution of these cases after
switching to a different TNF blocker suggests a TNF class effect. It has been suggested that this
paradoxical occurrence of psoriasis with TNF inhibition could be linked to an imbalance between
TNF and interferon alpha (IFN) [172, 173]. An indirect relationship exists between TNF levels and
regulation and release of IFN, and a pathogenic role of IFN in the development of psoriasis has
been shown in murine models and with IFN-treated humans [171]. There is no consensus
concerning the treatment of these paradoxical eruptions. Nevertheless, the majority of authors
suggest an aggressive treatment of the skin disease with topical steroids and phototherapy before
considering a change in the TNF antagonist.
38
Figure 2: atopic-like dermatitis in a 25 year-old patient, developed after several month of
etanercept therapy for rheumatoid arthritis
Figure 3: palmoplantar pustulosis in a 40 year-old patient, developed after 10 month of
adalimumab therapy for ankylosing spondylitis
39
4.2.3 Other inflammatory cutaneous side effects
Several other cutaneous inflammatory disorders have been described: erythema multiform, Steven’s
Johnson syndrome, toxic epidermal necrolysis, vasculitis [171], granulomatous diseases such as
interstitial granulomatous dermatitis, granuloma annulare or cutaneous sarcoidosis [174], lichenoid
eruptions, bullous pemphigoid [175]. Interestingly and conversely, TNF inhibitors have also been
reported to be effective in some of these various conditions [12], illustrating the complexity of the
immunological mechanisms leading to these inflammatory disorders.
4.3 Skin carcinomas
4.3.1 Melanoma and melanoma skin cancers
In psoriasis patients, there is a well demonstrated increased risk of melanoma and squamous cell
carcinoma (SCC) among patients treated by ciclosporine and psoralen-UVA therapy (PUVA) [176,
177]. With the TNF blockers, some observations have been made of induction of eruptive
melanoma and benign melanocytic naevi by etanercept and infliximab [178, 179] but also with
azathioprine and methotrexate. Furthermore, there have been 9 reports of severe or multiple and
eruptive SCC of the skin, 3 reports of SCC of the penis and two reports of multiple basal cell
carcinoma under TNF blockers [180-186]. Interestingly, most of the patients had received
etanercept for rheumatoid arthritis (8 patients) or psoriasis (4 patients) and psoriatic arthritis (1) and
all had signs of cutaneous photodamage or had been previously treated by PUVA and Methotrexate.
The rapidity of onset of these SCC in at risk patients suggests that TNF blockers could facilitate the
revelation of preclinical SCC.
A large observational study of patients with rheumatoid arthritis demonstrated an increased risk for
the development of nonmelanoma skin cancer (odds ratio 1.5, 95% confidence interval 1.2-1.8) and
a trend toward increased risk of melanoma (odds ratio 2.3, 95% confidence interval 0.9-5.4) in
patients treated with biologic agents (largely the 3 TNF inhibitors) [187]. A large-scale cohort study
observed the incidence of NMSC in patients with RA using TNF blockers versus a control group of
patients with non-inflammatory osteoarthritis [188]. Among the 15,789 patients with RA, the
authors found that TNF antagonists displayed an increased risk of NMSC when prescribed either
alone (hazard ratio, 1.24) or in combination with MTX (hazard ratio, 1.97).
These findings contrast with the results of a study including a clinical trials’ database of 1442 RA
patients receiving etanercept (4257 patient-years) and a postmarketing database of more than
125 000 patients receiving commercial etanercept (>250 000 patient-years) [189], in which no
association was found with an increase in the incidence of cutaneous SCC.
Taking together, these data and observations suggest that, as for other immunosuppressive drugs,
TNF blockers may increase the risk SCC in subjects with risk factors (sun exposure, high amounts
40
of PUVA). However, long term follow-up studies are still lacking to evaluate this risk in psoriasis
patients.
4.3.2 Cutaneous lymphoma
Aggressive cutaneous T-cell lymphomas have been reported after etanercept, adalimumab and
infliximab treatment [190-193]. Most of these cases were remarkable for the sudden onset and rapid
progression of disease. This atypical disease progression suggests that patients may have had a preexisting T-cell lymphoma kept in check by cellular immunity. Then anti-TNF therapy may have
lifted this control and thus permitted development of the T-cell clone.
Currently, these cases are rare, and no convincing evidence exists to prove that patients treated with
anti-TNF have a higher risk of cutaneous lymphoma than the general population.
5- TNF antagonists in other cutaneous diseases
The clinical efficacy of TNF blockers has been reported in various inflammatory skin diseases, well
reviewed in [12]. We will focus on several cutaneous diseases of peculiar interest.
5.1 Cutaneous sarcoidosis
Cutaneous sarcoidosis is a dermatosis characterized by noncaseating granulomatous infiltration.
Standard therapeutic options include corticoids, antimalarials, methotrexate (monotherapy or
combination) and newer therapies including pentoxifylline, tetracyclines, isotretinoin, leflunomide,
thalidomide, chlorambucil, melatonin, cyclosporine A, allopurinol, laser surgery and medium-dose
UVA1 phototherapy [194]. Nevertheless, cutaneous sarcoidosis is often a refractory chronic disease
and aggressive therapy may be required. The mechanisms underlying the formation, maintenance,
and spontaneous resolution of the sarcoid granuloma are not well understood but there are several
pieces of evidence that TNF plays a crucial role [16]. Several case reports and small series have
reported the efficacy of different anti-TNF agents in refractory cutaneous and systemic sarcoidosis
[195-200]. Adalimumab and infliximab induce apoptosis of cells presenting the bound form of TNF
[201], whereas etanercept does not. These data suggest that adalimumab and infliximab have a
better ability to disrupt granuloma than etanercept. There are clinical pieces of evidence to support
this hypothesis, with a better activity of adalimumab and infliximab than etanercept in
granulomatous disorders such as sarcoidosis and Crohn’s disease. Moreover, paradoxical
development of noncaseating granuloma has been documented under anti-TNF agents and more
frequently with etanercept, raising the hypothesis that TNF inhibitors may sometimes leave
sufficient cytokine activation to support granuloma formation [202-205].
The optimal modalities and dosing regimen of TNF blockers in cutaneous granulomatosis has still
to be defined. We have reported the case of a patient with refractory cutaneous sarcoidosis in whom
41
anti-TNF agents were ineffective at the standard dosage, but who responded to dose escalation
(Figure 4).
See appendix 10: Thielen AM, Barde C, Saurat JH, Laffitte E. Refractory chronic cutaneous
sarcoidosis responsive to dose escalation of TNF-alpha antagonists. Dermatology 2009;219:59-62.
5.2 Necrobiosis lipoidica
Necrobiosis lipoidica is an uncommon granulomatous skin disease of non infectious origin. It is
often associated with diabetes and its high morbidity is due to chronicity and eventually ulceration.
Clinically atrophic pretibial plaques are surrounded by an erythematous infiltrated border and
histology shows palissading granulomatous inflammation affecting the entire dermis. Therapeutic
options are numerous: a non exhaustive list consists of topical or intralesional steroids, topical
tacrolimus, photochemotherapy, antimalaric drugs, photodynamic therapy (PDT), fumaric acid,
thalidomide, pentoxifylline, heparin injections and excision followed by graft [206]. None of them
is constantly effective and all have been used off-label without any comparative study.
Three reports have already described the efficacy of systemic infliximab in necrobiosis lipoidica
[207, 208]. To avoid systemic side effects considering it is a cutaneous local disease, we have
conducted a prospective study of intralesional injection of infliximab (Barde C, Thielen AM,
Campanelli A, Laffitte E, Saurat J-H. Intralesional infliximab in non infectious cutaneous
granulomas: three cases of necrobiosis lipoidica. Arch Dermatol 2009, submitted). Three patients
with necrobiosis lipoidica were treated with over one year. The lesions diminished significantly in
all the patients (Figure 5). In one patient the injections relieved pain and the remission lasted for as
long as one and a half years but a recurrence was observed in the two other cases.
Intralesional injections of infliximab have been used in Crohn’s diseases and in rheumatoid arthritis
[209-211], but this is the first report of intralesional injections of infliximab in dermatology. It is a
safe therapeutic option avoiding potential serious side effects of intravenous infliximab. The long
follow up of the patients showed that it is a suspensive treatment.
42
Figure 4: Cutaneous sarcoidosis of the left cheek. Excellent evolution 7 months after adalimumab
treatment initiation at a dosage of 80 mg every other week
Figure 5: Necrobiosis lipoidica lesion before and 6 month after local injections of infliximab
0,1ml
43
5.3 Hidradenitis suppurativa
Hidradenitis suppurativa (HS) is a chronic relapsing skin disorder characterized by recurrent
inflammatory lesions leading in later stages to sclerosis, sinus tract formation, and fistula formation
[212]. A number of treatment options are available for HS, including antibiotics, retinoids,
immunosuppressants, and surgery. Despite such treatments, HS causes significant morbidity. The
etiopathogenesis of HS remains incompletely understood, but the most relevant pathological finding
in HS is an inflammatory process with or without overlapping infection. An increasing number of
reports have been published on the use of TNF antagonists in refractory HS and this disease could
be identified as another target disease by the pharmaceutical industry for the development of antiTNF agents in dermatology. However, most of these reports are small retrospective or prospective
series of patients, and lengths of follow-up of most reported cases of HS that were treated with anti–
TNF agents were short [213-217].
5.4 Behçet’s disease and aphtosis
Behçet’s disease is a chronic inflammatory multisystem disease, and presumably occurs as a result
of a vasculitis. Aphthae of the mucous membrane and cutaneous ulcers and/or papulopustules are
amongst the main symptoms of this disease and are useful parameters for the clinical determination
of activity. In addition, the eyes, CNS, gastrointestinal tract and joints are often involved. In an
acute attack of Behçet’s disease, raised TNF serum levels can be detected. Because of the chronic
course of the disease and the occasionally poor therapeutic response, clinical trials with TNF
blockers have been carried out, extensively reviewed in [12]. Dramatic therapeutic response has
been obtained with TNF blockers in patients with orogenital ulcerations, nodular lesions,
papulopustular lesions, attacks of arthritis and uveitis [245, 246].
5.5 Netherton syndrome
Netherton syndrome (NS) is a skin disorder caused by mutations in SPINK5, a gene encoding the
protease inhibitor lymphoepithelial Kazal-type–related inhibitor (LEKTI). It has been recently
shown that the pro-Th2 cytokine thymic stromal lymphopoietin (TSLP) and pro-inflammatory
cytokines such as TNF are overexpressed in LEKTI deficient epidermis [24].
We have reported the case of a 25-year old woman with NS, confirmed by the absence of LEKTI
expression in the epidermis and mutation in SPINK5. She presented with recurrent severe
inflammatory flares with focal blistering, unresponsive to therapy with systemic dapsone, topical
steroids, tacrolimus and pimecrolimus. Following an induction phase (week 0-2-6), maintenance
therapy with infliximab was given at 5mg/kg every other month. A dramatic improvement was
44
observed after the second treatment cycle, and after one year of therapy, the skin was nearly clear of
inflammatory lesions. However, the ichtiosis was not improved.
TSLP expression was assessed by ELISA and quantitative RT-PCR in skin biopsies obtained from
inflammatory and non inflammatory lesions before and after infliximab therapy. ELISA performed
on skin protein extracts revealed an elevated TSLP production in inflammatory skin lesions before
and after infliximab therapy. Of note, after one year of anti-TNF, a reduction by 4 of TSLP
production was observed both in inflammatory and non inflammatory skin lesions. Quantitative RTPCR performed on total RNA isolated from skin biopsies gave similar results for TSLP and
revealed a strong expression of TNF in both lesional and non-lesional skin that was not modulated
by infliximab therapy.
NS is a genodermatosis caused by the absence of LEKTI protein, which induces a loss of the
stratum corneum due to hyperactivity of epidermal proteases. The inflammatory skin reaction
associated leading to eczema is poorly understood. TSLP is a cytokine produced by epithelial cells,
including keratinocytes, which drives the inflammatory response toward a Th-2 type [218, 219] and
whose role in asthma and atopic dermatitis is being increasingly identified.
In our observation, high levels of TSLP in skin were correlated to the activity of inflammatory
disease, which is consistent with recent data [24] and indicates that this cytokine seems important in
Netherton syndrome. The significant and prolonged improvement of the eruption with infliximab
suggests that TNF could play a crucial role in Netherton's syndrome and in the inflammatory
cascade mediated by TSLP. Our data suggest that an anti-TNF should be considered as a valuable
therapeutic approach for NS.
See Appendix 11: Laffitte E, Fontao L, Kaya G, Khelifa E, Lubbe J, Saurat J-H. Infliximab for
Netherton syndrome: Sustained clinical improvement correlated with a reduction of thymic stromal
lymphopoietin levels in skin. J Invest Dermatol 2009;129:S22, and presented as a poster in 39th
Annual ESDR Meeting, 9-12 September 2009, Budapest, Hungary
6- Perspectives for TNF antagonists
Two main lines of development are to be expected with TNF inhibitors. Firstly the establishment of
national and international registries of patients, in order to assess their effectiveness and tolerance
independently from the pharmaceutical industry, and secondly the emergence of new molecules
inhibiting TNF.
6.1 Independent evaluation of efficacy and safety: usefulness of registries
With the licensing of the first TNF inhibitors, independent academia-initiated but industrysponsored drug registers were set up by the national rheumatology societies in several European
countries in order to monitor the long-term safety and effectiveness of this new generation of drugs
45
[220]. In contrast to the patients in a registry who receive care in the natural clinical setting,
subjects in randomized clinical trials are selected according to study criteria and may therefore not
reflect the experience of patients in clinical practice. It is possible that particular risks and
opportunities in the real patient population may therefore go undetected in randomized clinical
trials. Moreover, with an increasing number of new drugs and multiple exposures of individual
patients the assignment of events to specific treatments has become exceedingly difficult. Major
data on drug safety with regard to infections - tuberculosis as a major example [153, 221],
malignancies, cardiovascular events, pregnancy outcomes and deaths have been obtain from these
registries [220].
In the light of the increased risk of infections and malignancies in rheumatoid arthritis patients
treated with anti-tumor necrosis factor antibodies, the production of reliable data for psoriasis is
essential, and the importance of this industry-independent way of obtaining data has been also
identified in Dermatology [222]. Following this concept, nine European countries have established
registries to collect data on systemic psoriasis treatment (Italy, Sweden, Spain, Germany, Israel,
France, United Kingdom, The Netherlands and Portugal) [223]. The main objectives of these
registers are to assess the long-term safety and effectiveness of systemic psoriasis treatments and to
identify target phenotypes that may allow for specific, individualized treatments. Even though
different in some respects of study design and monitoring, these registers share a number of
common features: they include all licensed biological agents, they observe the patients for a defined
period of time or indefinitely irrespective of the drug given and they use comparator cohorts or
national registers in order to put the results into perspective. Moreover, there have been some
initiatives to combine the results from these national registries into compatible international
databases to increase their power and impact [223, 224]. In Switzerland such an effort has been
done, with the creation of the Swiss Dermatology Network for Biologics (SDNB) which includes
representatives of the different Swiss clinics of Dermatology, and whose goal is to establish a Swiss
register of biologics.
Several informations have already been obtained from these national registries: data on current
prescription behaviour for the treatment of psoriasis in private practices in Germany [225], long
term efficacy and tolerability of etanercept in daily practice in The Netherland [226], and a
significant and unexpected number of abnormalities of liver function in UK [227].
The question of skin malignancy being precipitated by biologic therapy will only be answered by
large well-designed cohort studies, which will collect data over the medium to long term on patients
treated with these drugs. Clearly this is of major importance in a cohort of patients with psoriasis
because treatment history will often include photochemotherapy potentially predisposing to
melanoma and nonmelanoma skin cancer.
46
6.2 Development of other targeted TNF inhibitors
Since the success of anti-TNF biological agents, much effort has gone into developing other drugs.
Some are new and more targeted biologics (solTNF inhibitors), or small molecule, orally
bioavailable TNF inhibitor (TACE inhibitors and p38MAP Kinase inhibitors). Another approach is
to induce an active anti-TNF immunotherapy (TNF Kinoid). There is few data in human yet, and
these drugs have been mostly used in patients with rheumatoid arthritis (RA). But Dermatology
may benefit in a short future of these new ways of TNF inhibition.
6.2.1 solTNF inhibitors
Because mouse models show that inhibition of soluble TNF (solTNF) is anti-inflammatory, while
inhibition of transmembrane TNF (tmTNF) sensitizes to infection and exacerbates demyelinating
diseases, multiple groups are attempting to develop soluble TNF-selective antagonists [8]. For
example, a group from Geneva presented data showing that a solTNF-selective ‘dominant-negative’
TNF biologic (XPro11595) consisting of blocking solTNF while sparing tmTNF was as antiinflammatory as etanercept in a mouse arthritis model without suppressing normal innate immunity
to listeriosis or tuberculosis [228]. Another group described development of selective antagonists of
the TNFR1 receptor, including ‘R1antTNF’, a pegylated variant of TNF which blocks TNFR1
signalling but preserves signalling of tmTNF through TNFR2, which was as efficacious as
etanercept in a mouse arthritis model, yet safer in mice challenged with adenovirus infection [229].
6.2.2 TACE inhibitors and p38MAP Kinase inhibitors
One of the ways to block TNF actions in the body is to inhibit the processing of pro-TNF by
blocking TNF-alpha converting enzyme (TACE). This target has been validated in preclinical trials
for the treatment of RA. Many compounds belonging to different chemical classes have been
synthesized as selective TACE inhibitors. Although there is a growing concern among scientific
fraternity whether a TACE inhibitor would show a favourable pharmacological profile and can be
recommended for treating RA; there are many promising TACE inhibitors in the preclinical studies
[230].
Another way is to target p38 mitogen-activated protein (MAP) kinase. This kinase occupies a
central role in the regulation of IL-1beta and TNF-alpha signalling network at both the
transcriptional and translational level. Since the mid-1990s, an immense number of inhibitors of
p38 MAP kinase have been characterised in vitro, and to date several compounds have been
advanced into clinical trials. Based on very promising preclinical data, a number of pharmaceutical
companies have developed inhibitors of MAP kinase p38 that predominantly impact its alpha
subunit. Most of the therapeutics are in phase II clinical trials; the therapeutic effects have not yet
reached expectations [231].
47
6.2.3 TNF Kinoid
As an alternative to anti-human TNF monoclonal antibodies and other TNF blocker approved drugs,
an active anti-TNF immunotherapy as been developed, based on a vaccine comprised of a keyhole
limpet hemocyanin-TNF heterocomplex immunogen, namely TNF Kinoid (TNF-K) adjuvanted in
incomplete Freund’s adjuvant [232]. In mice transgenic for TNF (TTg mice) which spontaneously
develop arthritides, TNF Kinoid vaccination elicited high titers of antibodies that neutralized TNF
bioactivities. Moreover, in this mouse model, anti-TNF immunotherapy with TNF-K had a
sustained, but reversible therapeutic efficacy, supporting the potential suitability of this approach in
treating human disease [233]. Human studies are ongoing in RA and Crohn’s diseases with
promising results, but no published data are available yet.
48
Conclusions
Even if thalidomide and anti-TNF “biologics” are TNF inhibitors, their effect and side effects are
completely different; these drugs are complementary and useful drugs in dermatology.
Thalidomide is a powerful molecule with convenient oral administration which represents a
significant therapeutic option in various immunological disorders and oncology. Its use requires
assessing the risk-benefit ratio depending on the indication as this ratio varies according to country.
The main side effects can be minimized by selecting suitable patients (in particular identifying
thromboembolic and neuropathy risk factors) and carefully following published recommendations
[234]. Teratogenicity can be controlled through effective contraceptive methods, as with other
highly teratogenic molecules frequently prescribed, for example isotretinoine in acne.
Given the uniqueness and complexity of the mechanisms of action, which are not fully understood
yet, new and unexpected indications could arise in the future, like chronic heart failure or bleeding
angiodysplasias, as recently reported [235-237]. The development of thalidomide derivatives with
fewer side effects is promising, but it is not clear yet if dermatology will benefit from these new
drugs.
The “biologics” TNF inhibitors have opened a new realm of therapy for patients with psoriasis.
They have also displayed utility in many other inflammatory dermatoses. Their side effect profile,
lack of end organ toxicity, and lack of interaction with other medications, make them an excellent
therapeutic option for many patients, but as with any systemic immunosuppressant medication they
must be monitored appropriately. However, the use of TNF blockers is limited by high costs. Cost
and insurance reimbursement may therefore limit the availability of these drugs for some patients,
especially in off label cases. Moreover, there is still a need of collecting long term safety data, and
creation of industry-independent cohorts and national registers should be promoted.
49
50
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Scheinfeld N. A comprehensive review and evaluation of the side effects of the tumor
necrosis factor alpha blockers etanercept, infliximab and adalimumab. J Dermatolog Treat
2004; 15:280-94.
Schottelius Aj, Moldawer Ll, Dinarello Ca, Asadullah K, Sterry W Edwards Ck, 3rd.
Biology of tumor necrosis factor-alpha- implications for psoriasis. Exp Dermatol 2004;
13:193-222.
Frishman Ji, Edwards Ck, 3rd, Sonnenberg Mg, Kohno T, Cohen Am Dinarello Ca. Tumor
necrosis factor (TNF)-alpha-induced interleukin-8 in human blood cultures discriminates
neutralization by the p55 and p75 TNF soluble receptors. J Infect Dis 2000; 182:1722-30.
Grell M, Wajant H, Zimmermann G Scheurich P. The type 1 receptor (CD120a) is the highaffinity receptor for soluble tumor necrosis factor. Proc Natl Acad Sci U S A 1998; 95:5705.
Peschon Jj, Torrance Ds, Stocking Kl, Glaccum Mb, Otten C, Willis Cr, et al. TNF receptordeficient mice reveal divergent roles for p55 and p75 in several models of inflammation. J
Immunol 1998; 160:943-52.
Kunkel Sl, Remick Dg, Strieter Rm Larrick Jw. Mechanisms that regulate the production
and effects of tumor necrosis factor-alpha. Crit Rev Immunol 1989; 9:93-117.
Choy Eh Panayi Gs. Cytokine pathways and joint inflammation in rheumatoid arthritis. N
Engl J Med 2001; 344:907-16.
Zalevsky J, Secher T, Ezhevsky Sa, Janot L, Steed Pm, O'brien C, et al. Dominant-negative
inhibitors of soluble TNF attenuate experimental arthritis without suppressing innate
immunity to infection. J Immunol 2007; 179:1872-83.
Tansey Mg Szymkowski De. The TNF superfamily in 2009: new pathways, new indications,
and new drugs. Drug Discov Today 2009; 14:1082-8.
Blam Me, Stein Rb Lichtenstein Gr. Integrating anti-tumor necrosis factor therapy in
inflammatory bowel disease: current and future perspectives. Am J Gastroenterol 2001;
96:1977-97.
Furst De, Breedveld Fc, Kalden Jr, Smolen Js, Antoni Ce, Bijlsma Jw, et al. Updated
consensus statement on biological agents for the treatment of rheumatoid arthritis and other
rheumatic diseases (May 2002). Ann Rheum Dis 2002; 61 Suppl 2:ii2-7.
Jacobi A, Mahler V, Schuler G Hertl M. Treatment of inflammatory dermatoses by tumour
necrosis factor antagonists. J Eur Acad Dermatol Venereol 2006; 20:1171-87.
Kircik Lh Del Rosso Jq. Anti-TNF agents for the treatment of psoriasis. J Drugs Dermatol
2009; 8:546-59.
Kristensen M, Chu Cq, Eedy Dj, Feldmann M, Brennan Fm Breathnach Sm. Localization of
tumour necrosis factor-alpha (TNF-alpha) and its receptors in normal and psoriatic skin:
epidermal cells express the 55-kD but not the 75-kD TNF receptor. Clin Exp Immunol 1993;
94:354-62.
Nickoloff Bj, Karabin Gd, Barker Jn, Griffiths Ce, Sarma V, Mitra Rs, et al. Cellular
localization of interleukin-8 and its inducer, tumor necrosis factor-alpha in psoriasis. Am J
Pathol 1991; 138:129-40.
Asadullah K, Prosch S, Audring H, Buttnerova I, Volk Hd, Sterry W, et al. A high
prevalence of cytomegalovirus antigenaemia in patients with moderate to severe chronic
plaque psoriasis: an association with systemic tumour necrosis factor alpha overexpression.
Br J Dermatol 1999; 141:94-102.
Partsch G, Steiner G, Leeb Bf, Dunky A, Broll H Smolen Js. Highly increased levels of
tumor necrosis factor-alpha and other proinflammatory cytokines in psoriatic arthritis
synovial fluid. J Rheumatol 1997; 24:518-23.
Sweiss Nj, Curran J Baughman Rp. Sarcoidosis, role of tumor necrosis factor inhibitors and
other biologic agents, past, present, and future concepts. Clin Dermatol 2007; 25:341-6.
51
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
Odeka Eb Miller V. Thalidomide in oral Crohn's disease refractory to conventional medical
treatment. J Pediatr Gastroenterol Nutr 1997; 25:250-1.
Sampaio Ep, Kaplan G, Miranda A, Nery Ja, Miguel Cp, Viana Sm, et al. The influence of
thalidomide on the clinical and immunologic manifestation of erythema nodosum leprosum.
J Infect Dis 1993; 168:408-14.
Hamuryudan V, Mat C, Saip S, Ozyazgan Y, Siva A, Yurdakul S, et al. Thalidomide in the
treatment of the mucocutaneous lesions of the Behcet syndrome. A randomized, doubleblind, placebo-controlled trial. Ann Intern Med 1998; 128:443-50.
Feliciani C, Toto P, Amerio P, Pour Sm, Coscione G, Shivji G, et al. In vitro and in vivo
expression of interleukin-1alpha and tumor necrosis factor-alpha mRNA in pemphigus
vulgaris: interleukin-1alpha and tumor necrosis factor-alpha are involved in acantholysis. J
Invest Dermatol 2000; 114:71-7.
Leung Dy. Atopic dermatitis: new insights and opportunities for therapeutic intervention. J
Allergy Clin Immunol 2000; 105:860-76.
Briot A, Deraison C, Lacroix M, Bonnart C, Robin A, Besson C, et al. Kallikrein 5 induces
atopic dermatitis-like lesions through PAR2-mediated thymic stromal lymphopoietin
expression in Netherton syndrome. J Exp Med 2009; 206:1135-47.
Zwingenberger K Wnendt S. Immunomodulation by thalidomide: systematic review of the
literature and of unpublished observations. J Inflamm 1995; 46:177-211.
D'arcy Pf Griffin Jp. Thalidomide revisited. Adverse Drug React Toxicol Rev 1994; 13:6576.
Mcbride W. Thalidomide and congenital abnormalities. Lancet 1961; 2:1358.
Mellin Gw Katzenstein M. The saga of thalidomide: neuropathy to embryopathy, with case
reports and congenital abnormalities. N Engl J Med 1963; 267:1184-1193.
Sheskin J. Thalidomide in the treatment of lepra reactions. Clin Pharmacol Ther 1965;
6:303-306.
Sampaio Ep, Sarno En, Galilly R, Cohn Za Kaplan G. Thalidomide selectively inhibits
tumor necrosis factor alpha production by stimulated human monocytes. J Exp Med 1991;
173:699-703.
Hoglund P, Eriksson T Bjorkman S. A double-blind study of the sedative effects of the
thalidomide enantiomers in humans. J Pharmacokinet Biopharm 1998; 26:363-83.
Kenyon Bm, Browne F D'amato Rj. Effects of thalidomide and related metabolites in a
mouse corneal model of neovascularization. Exp Eye Res 1997; 64:971-8.
Wnendt S Zwingenberger K. Thalidomide's chirality. Nature 1997; 385:303-4.
Eriksson T, Bjorkman S, Roth B, Fyge A Hoglund P. Stereospecific determination, chiral
inversion in vitro and pharmacokinetics in humans of the enantiomers of thalidomide.
Chirality 1995; 7:44-52.
Gunzler V. Thalidomide in human immunodeficiency virus (HIV) patients. A review of
safety considerations. Drug Saf 1992; 7:116-34.
Teo Sk, Colburn Wa Thomas Sd. Single-dose oral pharmacokinetics of three formulations of
thalidomide in healthy male volunteers. J Clin Pharmacol 1999; 39:1162-8.
Chen Tl, Vogelsang Gb, Petty Bg, Brundrett Rb, Noe Da, Santos Gw, et al. Plasma
pharmacokinetics and urinary excretion of thalidomide after oral dosing in healthy male
volunteers. Drug Metab Dispos 1989; 17:402-5.
Boutin F Bonnet F. Le thalidomide : pharmacochimie et pharmacie clinique. Lyon Pharm
1995; 46:419-423.
Eriksson T, Bjorkman S Hoglund P. Clinical pharmacology of thalidomide. Eur J Clin
Pharmacol 2001; 57:365-76.
Teo Sk, Scheffler Mr, Kook Ka, Tracewell Wg, Colburn Wa, Stirling Di, et al. Effect of a
high-fat meal on thalidomide pharmacokinetics and the relative bioavailability of oral
formulations in healthy men and women. Biopharm Drug Dispos 2000; 21:33-40.
52
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
Nicholls Pj. A note on the absorption and excretion of 14C-labelled thalidomide in pregnant
mice. J Pharm Pharmacol 1966; 18:46-8.
Faigle J, Keberle H, Riess W Schmid K. The metabolic fate of thalidomide. Experimentia
1962; 18:389-397.
Mchugh Sm Rowland Tl. Thalidomide and derivatives: immunological investigations of
tumour necrosis factor-alpha (TNF-alpha) inhibition suggest drugs capable of selective gene
regulation. Clin Exp Immunol 1997; 110:151-4.
Tseng S, Pak G, Washenik K, Pomeranz Mk Shupack Jl. Rediscovering thalidomide: a
review of its mechanism of action, side effects, and potential uses. J Am Acad Dermatol
1996; 35:969-79.
Lutwak-Mann C, Schmid K Keberle H. Thalidomide in rabbit semen. Nature 1967;
214:1018-20.
Teo Sk, Harden Jl, Burke Ab, Noormohamed Fh, Youle M, Johnson Ma, et al. Thalidomide
is distributed into human semen after oral dosing. Drug Metab Dispos 2001; 29:1355-7.
Noormohamed Fh, Youle Ms, Higgs Cj, Kook Ka, Hawkins Da, Lant Af, et al.
Pharmacokinetics and hemodynamic effects of single oral doses of thalidomide in
asymptomatic human immunodeficiency virus-infected subjects. AIDS Res Hum
Retroviruses 1999; 15:1047-52.
Hadgraft J, Goosen C, Du Plessis J Flynn G. Predicting the dermal absorption of
thalidomide and its derivatives. Skin Pharmacol Appl Skin Physiol 2003; 16:123-9.
Scheffler Mr, Colburn W, Kook Ka Thomas Sd. Thalidomide does not alter estrogenprogesterone hormone single dose pharmacokinetics. Clin Pharmacol Ther 1999; 65:483-90.
Kanbayashi T, Shimizu T, Takahashi Y, Kitajima T, Takahashi K, Saito Y, et al.
Thalidomide increases both REM and stage 3-4 sleep in human adults: a preliminary study.
Sleep 1999; 22:113-5.
Meierhofer C Wiedermann Cj. New insights into the pharmacological and toxicological
effects of thalidomide. Curr Opin Drug Discov Devel 2003; 6:92-9.
Keenan Rj, Eiras G, Burckart Gj, Stuart Rs, Hardesty Rl, Vogelsang G, et al.
Immunosuppressive properties of thalidomide. Inhibition of in vitro lymphocyte
proliferation alone and in combination with cyclosporine or FK506. Transplantation 1991;
52:908-10.
Chuong Ph, Galons H, Voisin J, Zhu J, Righenzi S, Warnet Jm, et al. In vitro and in vivo
immunosuppressive potential of thalidomide and its derivative, N-hydroxythalidomide,
alone and in combination with cyclosporin A. Int J Immunopharmacol 1997; 19:289-96.
Haslett Pa, Corral Lg, Albert M Kaplan G. Thalidomide costimulates primary human T
lymphocytes, preferentially inducing proliferation, cytokine production, and cytotoxic
responses in the CD8+ subset. J Exp Med 1998; 187:1885-92.
Shannon Ej, Ejigu M, Haile-Mariam Hs, Berhan Ty Tasesse G. Thalidomide's effectiveness
in erythema nodosum leprosum is associated with a decrease in CD4+ cells in the peripheral
blood. Lepr Rev 1992; 63:5-11.
Mchugh Sm, Rifkin Ir, Deighton J, Wilson Ab, Lachmann Pj, Lockwood Cm, et al. The
immunosuppressive drug thalidomide induces T helper cell type 2 (Th2) and concomitantly
inhibits Th1 cytokine production in mitogen- and antigen-stimulated human peripheral
blood mononuclear cell cultures. Clin Exp Immunol 1995; 99:160-7.
Calderon P, Anzilotti M Phelps R. Thalidomide in dermatology. New indications for an old
drug. Int J Dermatol 1997; 36:881-7.
Moreira Al, Sampaio Ep, Zmuidzinas A, Frindt P, Smith Ka Kaplan G. Thalidomide exerts
its inhibitory action on tumor necrosis factor alpha by enhancing mRNA degradation. J Exp
Med 1993; 177:1675-80.
Klausner Jd, Freedman Vh Kaplan G. Thalidomide as an anti-TNF-alpha inhibitor:
implications for clinical use. Clin Immunol Immunopathol 1996; 81:219-23.
53
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
Ishikawa M, Kanno S, Takayanagi M, Takayanagi Y Sasaki K. Thalidomide promotes the
release of tumor necrosis factor-alpha (TNF-alpha) and lethality by lipopolysaccharide in
mice. Biol Pharm Bull 1998; 21:638-40.
Wolkenstein P, Latarjet J, Roujeau Jc, Duguet C, Boudeau S, Vaillant L, et al. Randomised
comparison of thalidomide versus placebo in toxic epidermal necrolysis. Lancet 1998;
352:1586-9.
Jacobson Jm, Greenspan Js, Spritzler J, Ketter N, Fahey Jl, Jackson Jb, et al. Thalidomide
for the treatment of oral aphthous ulcers in patients with human immunodeficiency virus
infection. National Institute of Allergy and Infectious Diseases AIDS Clinical Trials Group.
N Engl J Med 1997; 336:1487-93.
Keifer Ja, Guttridge Dc, Ashburner Bp Baldwin as, Jr. Inhibition of NF-kappa B activity by
thalidomide through suppression of IkappaB kinase activity. J Biol Chem 2001; 276:223827.
Klausner Jd, Kaplan G Haslett Pa. Thalidomide in toxic epidermal necrolysis. Lancet 1999;
353:324.
D'amato Rj, Loughnan Ms, Flynn E Folkman J. Thalidomide is an inhibitor of angiogenesis.
Proc Natl Acad Sci U S A 1994; 91:4082-5.
Stephens Td, Bunde Cj Fillmore Bj. Mechanism of action in thalidomide teratogenesis.
Biochem Pharmacol 2000; 59:1489-99.
Kruse Fe, Joussen Am, Rohrschneider K, Becker Md Volcker He. Thalidomide inhibits
corneal angiogenesis induced by vascular endothelial growth factor. Graefes Arch Clin Exp
Ophthalmol 1998; 236:461-6.
Or R, Feferman R Shoshan S. Thalidomide reduces vascular density in granulation tissue of
subcutaneously implanted polyvinyl alcohol sponges in guinea pigs. Exp Hematol 1998;
26:217-21.
Bauer Ks, Dixon Sc Figg Wd. Inhibition of angiogenesis by thalidomide requires metabolic
activation, which is species-dependent. Biochem Pharmacol 1998; 55:1827-34.
Kumar S, Witzig Te Rajkumar Sv. Thalidomide as an anti-cancer agent. J Cell Mol Med
2002; 6:160-74.
Drucker L, Uziel O, Tohami T, Shapiro H, Radnay J, Yarkoni S, et al. Thalidomide downregulates transcript levels of GC-rich promoter genes in multiple myeloma. Mol Pharmacol
2003; 64:415-20.
Minchinton Ai, Fryer Kh, Wendt Kr, Clow Ka Hayes Mm. The effect of thalidomide on
experimental tumors and metastases. Anticancer Drugs 1996; 7:339-43.
Joseph Ib Isaacs Jt. Macrophage role in the anti-prostate cancer response to one class of
antiangiogenic agents. J Natl Cancer Inst 1998; 90:1648-53.
Okafor Mc. Thalidomide for erythema nodosum leprosum and other applications.
Pharmacotherapy 2003; 23:481-93.
Wines Ny, Cooper Aj Wines Mp. Thalidomide in dermatology. Australas J Dermatol 2002;
43:229-38.
Laffitte E Revuz J. Thalidomide. Ann Dermatol Venereol 2000; 127:603-13.
Naafs B Faber Wr. Thalidomide therapy. An open trial. Int J Dermatol 1985; 24:131-4.
Varma K Finlay Ay. Exacerbation of psoriasis by thalidomide in a patient with erythema
multiforme. Br J Dermatol 2006; 154:789-90.
Dobson Cm Parslew Ra. Exacerbation of psoriasis by thalidomide in Behcet's syndrome. Br
J Dermatol 2003; 149:432-3.
Rubegni P, Sbano P, De Aloe G, Flori Ml Fimiani M. Thalidomide in the treatment of
Kaposi's sarcoma. Dermatology 2007; 215:240-4.
Ben M'barek L, Fardet L, Mebazaa A, Thervet E, Biet I, Kerob D, et al. A retrospective
analysis of thalidomide therapy in non-HIV-related Kaposi's sarcoma. Dermatology 2007;
215:202-5.
54
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
103.
104.
105.
Little Rf, Wyvill Km, Pluda Jm, Welles L, Marshall V, Figg Wd, et al. Activity of
thalidomide in AIDS-related Kaposi's sarcoma. J Clin Oncol 2000; 18:2593-602.
Laffitte E. Thalidomide in Kaposi sarcoma: promising or disappointing? Dermatology 2007;
215:171-2.
Ossandon A, Cassara Ea, Priori R Valesini G. Thalidomide: focus on its employment in
rheumatologic diseases. Clin Exp Rheumatol 2002; 20:709-18.
Ribas C Colleoni Gw. Advances in the treatment of multiple myeloma: the role of
thalidomide. Leuk Lymphoma 2003; 44:291-8.
Deaner Pb. The use of thalidomide in the management of severe sweating in patients with
advanced malignancy: trial report. Palliat Med 2000; 14:429-31.
Deaner P. Thalidomide for distressing night sweats in advanced malignant disease. Palliat
Med 1998; 12:208-9.
Fratta I, Sigg E Maiorana K. Teratogenic effects of thalidomide in rabbits, rats, hamsters and
mice. Toxicol App Pharmacol 1965; 7:268-286.
Hales Bf. Thalidomide on the comeback trail. Nat Med 1999; 5:489-90.
Teo Sk, Sabourin Pj, O'brien K, Kook Ka Thomas Sd. Metabolism of thalidomide in human
microsomes, cloned human cytochrome P-450 isozymes, and Hansen's disease patients. J
Biochem Mol Toxicol 2000; 14:140-7.
Stephens Td. Proposed mechanisms of action in thalidomide embryopathy. Teratology
1988; 38:229-39.
Parman T, Wiley Mj Wells Pg. Free radical-mediated oxidative DNA damage in the
mechanism of thalidomide teratogenicity. Nat Med 1999; 5:582-5.
Castilla Ee, Ashton-Prolla P, Barreda-Mejia E, Brunoni D, Cavalcanti Dp, Correa-Neto J, et
al. Thalidomide, a current teratogen in South America. Teratology 1996; 54:273-7.
Lammer Ej, Chen Dt, Hoar Rm, Agnish Nd, Benke Pj, Braun Jt, et al. Retinoic acid
embryopathy. N Engl J Med 1985; 313:837-41.
Brinker A, Kornegay C Nourjah P. Trends in adherence to a revised risk management
program designed to decrease or eliminate isotretinoin-exposed pregnancies: evaluation of
the accutane SMART program. Arch Dermatol 2005; 141:563-9.
Mcbride Wg. Thalidomide may be a mutagen. BMJ 1994; 308:1635-6.
Smithells D. Dominant gene probably caused some of defects ascribed to thalidomide. BMJ
1998; 316:149.
Smithells D. Does thalidomide cause second generation birth defects? Drug Saf 1998;
19:339-41.
Stromland K, Philipson E Andersson Gronlund M. Offspring of male and female parents
with thalidomide embryopathy: birth defects and functional anomalies. Teratology 2002;
66:115-21.
Ashby J, Tinwell H, Callander Rd, Kimber I, Clay P, Galloway Sm, et al. Thalidomide: lack
of mutagenic activity across phyla and genetic endpoints. Mutat Res 1997; 396:45-64.
Zhu X, Zhang Yp, Klopman G Rosenkranz Hs. Thalidomide and metabolites: indications of
the absence of 'genotoxic' carcinogenic potentials. Mutat Res 1999; 425:153-67.
Calabrese L Fleischer Ab. Thalidomide: current and potential clinical applications. Am J
Med 2000; 108:487-95.
Harland Cc, Steventon Gb Marsden Jr. Thalidomide-induced neuropathy and genetic
differences in drug metabolism. Eur J Clin Pharmacol 1995; 49:1-6.
Lagueny A, Rommel A, Vignolly B, Taieb A, Vendeaud-Busquet M, Doutre Ms, et al.
Thalidomide neuropathy: an electrophysiologic study. Muscle Nerve 1986; 9:837-44.
Gardner-Medwin Jm, Smith Nj Powell Rj. Clinical experience with thalidomide in the
management of severe oral and genital ulceration in conditions such as Behcet's disease: use
of neurophysiological studies to detect thalidomide neuropathy. Ann Rheum Dis 1994;
53:828-32.
55
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
Sheskin J Yaar I. Motor-conduction velocity of cubital nerves in patients with leprosy
reactions. Summary of a 13-year observation series during thalidomide therapy. Hautarzt
1979; 30:376-9.
Wulff Ch, Hoyer H, Asboe-Hansen G Brodthagen H. Development of polyneuropathy
during thalidomide therapy. Br J Dermatol 1985; 112:475-80.
Clemmensen Oj, Olsen Pz Andersen Ke. Thalidomide neurotoxicity. Arch Dermatol 1984;
120:338-41.
Aronson Ik, Yu R, West Dp, Van Den Broek H Antel J. Thalidomide-induced peripheral
neuropathy. Effect of serum factor on nerve cultures. Arch Dermatol 1984; 120:1466-70.
Knop J, Bonsmann G, Happle R, Ludolph A, Matz Dr, Mifsud Ej, et al. Thalidomide in the
treatment of sixty cases of chronic discoid lupus erythematosus. Br J Dermatol 1983;
108:461-6.
Ochonisky S, Verroust J, Bastuji-Garin S, Gherardi R Revuz J. Thalidomide neuropathy
incidence and clinico-electrophysiologic findings in 42 patients. Arch Dermatol 1994;
130:66-9.
Singhal S, Mehta J, Desikan R, Ayers D, Roberson P, Eddlemon P, et al. Antitumor activity
of thalidomide in refractory multiple myeloma. N Engl J Med 1999; 341:1565-71.
Singhal S Mehta J. Thalidomide in cancer: potential uses and limitations. BioDrugs 2001;
15:163-72.
Bastuji-Garin S, Ochonisky S, Bouche P, Gherardi Rk, Duguet C, Djerradine Z, et al.
Incidence and risk factors for thalidomide neuropathy: a prospective study of 135
dermatologic patients. J Invest Dermatol 2002; 119:1020-6.
Fullerton Pm O'sullivan Dj. Thalidomide neuropathy: a clinical electrophysiological, and
histological follow-up study. J Neurol Neurosurg Psychiatry 1968; 31:543-51.
Strauss Rs Das Km. Thalidomide-induced sensory neuropathy. J Pediatr Gastroenterol Nutr
2001; 32:322-4.
Bennett Cl, Schumock Gt, Desai Aa, Kwaan Hc, Raisch Dw, Newlin R, et al. Thalidomideassociated deep vein thrombosis and pulmonary embolism. Am J Med 2002; 113:603-6.
Esteve E Legac E. Deep vein thrombosis and pulmonary embolism in a patient with
aphthosis treated with thalidomide. Ann Dermatol Venereol 2001; 128:148-9.
Flageul B, Wallach D, Cavelier-Balloy B, Bachelez H, Carsuzaa F Dubertret L.
Thalidomide and thrombosis. Ann Dermatol Venereol 2000; 127:171-4.
Gachon J, Grob Jj Richard Ma. Thrombotic accidents induced by thalidomide: two cases.
Rev Med Interne 2002; 23:724-7.
Piette Jc, Sbai A Frances C. Warning: thalidomide-related thrombotic risk potentially
concerns patients with lupus. Lupus 2002; 11:67-70.
Pouaha J, Martin S, Trechot P, Truchetet F, Barbaud A Schmutz Jl. Thalidomide and
thrombosis: three observations. Presse Med 2001; 30:1008-9.
Wang J, Weiss I, Svoboda K Kwaan Hc. Thrombogenic role of cells undergoing apoptosis.
Br J Haematol 2001; 115:382-91.
Morgan Ae, Smith Wk Levenson Jl. Reversible dementia due to thalidomide therapy for
multiple myeloma. N Engl J Med 2003; 348:1821-2.
Trojan A, Chasse E, Gay B, Pichert G Taverna C. Severe hepatic toxicity due to thalidomide
in relapsed multiple myeloma. Ann Oncol 2003; 14:501-2.
Badros Az, Siegel E, Bodenner D, Zangari M, Zeldis J, Barlogie B, et al. Hypothyroidism in
patients with multiple myeloma following treatment with thalidomide. Am J Med 2002;
112:412-3.
Frances C, El Khoury S, Gompel A, Becherel Pa, Chosidow O Piette Jc. Transient
secondary amenorrhea in women treated by thalidomide. Eur J Dermatol 2002; 12:63-5.
Gompel A, Frances C, Piette Jc, Blanc As, Cordoliani F Piette Am. Ovarian failure with
thalidomide treatment in complex aphthosis: comment on the concise communication by
Ordi et al. Arthritis Rheum 1999; 42:2259-60.
56
129.
130.
131.
132.
133.
134.
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
Ordi J, Cortes F, Martinez N, Mauri M, De Torres I Vilardell M. Thalidomide induces
amenorrhea in patients with lupus disease. Arthritis Rheum 1998; 41:2273-5.
Passeron T, Lacour Jp, Murr D Ortonne Jp. Thalidomide-induced amenorrhoea: two cases.
Br J Dermatol 2001; 144:1292-3.
Hall Vc, El-Azhary Ra, Bouwhuis S Rajkumar Sv. Dermatologic side effects of thalidomide
in patients with multiple myeloma. J Am Acad Dermatol 2003; 48:548-52.
Haslett P, Tramontana J, Burroughs M, Hempstead M Kaplan G. Adverse reactions to
thalidomide in patients infected with human immunodeficiency virus. Clin Infect Dis 1997;
24:1223-7.
Williams I, Weller Iv, Malni A, Anderson J Waters Mf. Thalidomide hypersensitivity in
AIDS. Lancet 1991; 337:436-7.
Bielsa I, Teixido J, Ribera M Ferrandiz C. Erythroderma due to thalidomide: report of two
cases. Dermatology 1994; 189:179-81.
Rajkumar Sv, Gertz Ma Witzig Te. Life-threatening toxic epidermal necrolysis with
thalidomide therapy for myeloma. N Engl J Med 2000; 343:972-3.
Zeldis Jb, Williams Ba, Thomas Sd Elsayed Me. S.T.E.P.S.: a comprehensive program for
controlling and monitoring access to thalidomide. Clin Ther 1999; 21:319-30.
Wnendt S, Finkam M, Winter W, Ossig J, Raabe G Zwingenberger K. Enantioselective
inhibition of TNF-alpha release by thalidomide and thalidomide-analogues. Chirality 1996;
8:390-6.
Gordon Jn Goggin Pm. Thalidomide and its derivatives: emerging from the wilderness.
Postgrad Med J 2003; 79:127-32.
Hideshima T, Chauhan D, Shima Y, Raje N, Davies Fe, Tai Yt, et al. Thalidomide and its
analogs overcome drug resistance of human multiple myeloma cells to conventional therapy.
Blood 2000; 96:2943-50.
Richardson Pg, Schlossman Rl, Weller E, Hideshima T, Mitsiades C, Davies F, et al.
Immunomodulatory drug CC-5013 overcomes drug resistance and is well tolerated in
patients with relapsed multiple myeloma. Blood 2002; 100:3063-7.
Kumar S Rajkumar Sv. Thalidomide and lenalidomide in the treatment of multiple
myeloma. Eur J Cancer 2006; 42:1612-22.
Christian Ms, Laskin Ol, Sharper V, Hoberman A, Stirling Di Latriano L. Evaluation of the
developmental toxicity of lenalidomide in rabbits. Birth Defects Res B Dev Reprod Toxicol
2007; 80:188-207.
Green J, Upjohn E, Mccormack C, Zeldis J Prince Hm. Successful treatment of Behcet's
disease with lenalidomide. Br J Dermatol 2008; 158:197-8.
Shah A, Albrecht J, Bonilla-Martinez Z, Okawa J, Rose M, Rosenbach M, et al.
Lenalidomide for the treatment of resistant discoid lupus erythematosus. Arch Dermatol
2009; 145:303-6.
Querfeld C, Kuzel Tm, Guitart J Rosen St. Lenalidomide (Revlimid®) in patients with
cutaneous T-cell lymphoma. haematologica reports 2006; 2:38-39.
Thieu Kp, Rosenbach M, Xu X Kist Jm. Neutrophilic dermatosis complicating lenalidomide
therapy. J Am Acad Dermatol 2009.
Hoverson Ar, Davis Md, Weenig Rh Wolanskyj Ap. Neutrophilic dermatosis (Sweet
syndrome) of the hands associated with lenalidomide. Arch Dermatol 2006; 142:1070-1.
Castaneda Cp, Brandenburg Na, Bwire R, Burton Gh Zeldis Jb. Erythema
multiforme/Stevens-Johnson syndrome/toxic epidermal necrolysis in lenalidomide-treated
patients. J Clin Oncol 2009; 27:156-7.
Mossner R, Schon Mp Reich K. Tumor necrosis factor antagonists in the therapy of
psoriasis. Clin Dermatol 2008; 26:486-502.
Furst De, Wallis R, Broder M Beenhouwer Do. Tumor necrosis factor antagonists: different
kinetics and/or mechanisms of action may explain differences in the risk for developing
granulomatous infection. Semin Arthritis Rheum 2006; 36:159-67.
57
151.
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
162.
163.
164.
165.
166.
167.
168.
169.
170.
Hamdi H, Mariette X, Godot V, Weldingh K, Hamid Am, Prejean Mv, et al. Inhibition of
anti-tuberculosis T-lymphocyte function with tumour necrosis factor antagonists. Arthritis
Res Ther 2006; 8:R114.
Saliu Oy, Sofer C, Stein Ds, Schwander Sk Wallis Rs. Tumor-necrosis-factor blockers:
differential effects on mycobacterial immunity. J Infect Dis 2006; 194:486-92.
Tubach F, Salmon D, Ravaud P, Allanore Y, Goupille P, Breban M, et al. Risk of
tuberculosis is higher with anti-tumor necrosis factor monoclonal antibody therapy than with
soluble tumor necrosis factor receptor therapy: The three-year prospective French Research
Axed on Tolerance of Biotherapies registry. Arthritis Rheum 2009; 60:1884-94.
Van Den Brande Jm, Braat H, Van Den Brink Gr, Versteeg Hh, Bauer Ca, Hoedemaeker I,
et al. Infliximab but not etanercept induces apoptosis in lamina propria T-lymphocytes from
patients with Crohn's disease. Gastroenterology 2003; 124:1774-85.
Menter A, Gottlieb A, Feldman Sr, Van Voorhees As, Leonardi Cl, Gordon Kb, et al.
Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1.
Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J
Am Acad Dermatol 2008; 58:826-50.
Griffiths Ce Barker Jn. Pathogenesis and clinical features of psoriasis. Lancet 2007;
370:263-71.
De Korte J, Sprangers Ma, Mombers Fm Bos Jd. Quality of life in patients with psoriasis: a
systematic literature review. J Investig Dermatol Symp Proc 2004; 9:140-7.
Jacobson Cc Kimball Ab. Rethinking the Psoriasis Area and Severity Index: the impact of
area should be increased. Br J Dermatol 2004; 151:381-7.
Jackson Jm. TNF- alpha inhibitors. Dermatol Ther 2007; 20:251-64.
Schmitt J Wozel G. Targeted treatment of psoriasis with adalimumab: a critical appraisal
based on a systematic review of the literature. Biologics 2009; 3:303-18.
Castelo-Soccio L Van Voorhees As. Long-term efficacy of biologics in dermatology.
Dermatol Ther 2009; 22:22-33.
Esposito M, Mazzotta A, De Felice C, Papoutsaki M Chimenti S. Treatment of
erythrodermic psoriasis with etanercept. Br J Dermatol 2006; 155:156-9.
Newland Mr, Weinstein A Kerdel F. Rapid response to infliximab in severe pustular
psoriasis, von Zumbusch type. Int J Dermatol 2002; 41:449-52.
Voigtlander C, Luftl M, Schuler G Hertl M. Infliximab (anti-tumor necrosis factor alpha
antibody): a novel, highly effective treatment of recalcitrant subcorneal pustular dermatosis
(Sneddon-Wilkinson disease). Arch Dermatol 2001; 137:1571-4.
Thielen Am, Barde C, Marazza G Saurat Jh. Long-term control with etanercept (Enbrel) of a
severe acrodermatitis continua of Hallopeau refractory to infliximab (Remicade).
Dermatology 2008; 217:137-9.
Setoguchi S, Solomon Dh, Weinblatt Me, Katz Jn, Avorn J, Glynn Rj, et al. Tumor necrosis
factor alpha antagonist use and cancer in patients with rheumatoid arthritis. Arthritis Rheum
2006; 54:2757-64.
Laffitte E, Janssens Jp, Roux-Lombard P, Thielen Am, Barde C, Marazza G, et al.
Tuberculosis screening in patients with psoriasis before antitumour necrosis factor therapy:
comparison of an interferon-gamma release assay vs. tuberculin skin test. Br J Dermatol
2009; 161:797-800.
Rullan P Murase J. Two cases of chronic atopic dermatitis treated with soluble tumor
necrosis factor receptor therapy. J Drugs Dermatol 2009; 8:873-6.
Collamer An, Guerrero Kt, Henning Js Battafarano Df. Psoriatic skin lesions induced by
tumor necrosis factor antagonist therapy: a literature review and potential mechanisms of
action. Arthritis Rheum 2008; 59:996-1001.
Harrison Mj, Dixon Wg, Watson Kd, King Y, Groves R, Hyrich Kl, et al. Rates of newonset psoriasis in patients with rheumatoid arthritis receiving anti-tumour necrosis factor
58
171.
172.
173.
174.
175.
176.
177.
178.
179.
180.
181.
182.
183.
184.
185.
186.
187.
188.
alpha therapy: results from the British Society for Rheumatology Biologics Register. Ann
Rheum Dis 2009; 68:209-15.
Kerbleski Jf Gottlieb Ab. Dermatological complications and safety of anti-TNF treatments.
Gut 2009; 58:1033-9.
De Gannes Gc, Ghoreishi M, Pope J, Russell A, Bell D, Adams S, et al. Psoriasis and
pustular dermatitis triggered by TNF-{alpha} inhibitors in patients with rheumatologic
conditions. Arch Dermatol 2007; 143:223-31.
Fiorentino Df. The Yin and Yang of TNF-{alpha} inhibition. Arch Dermatol 2007; 143:2336.
Deng A, Harvey V, Sina B, Strobel D, Badros A, Junkins-Hopkins Jm, et al. Interstitial
granulomatous dermatitis associated with the use of tumor necrosis factor alpha inhibitors.
Arch Dermatol 2006; 142:198-202.
Stausbol-Gron B, Deleuran M, Sommer Hansen E Kragballe K. Development of bullous
pemphigoid during treatment of psoriasis with adalimumab. Clin Exp Dermatol 2009;
34:e285-6.
Paul Cf, Ho Vc, Mcgeown C, Christophers E, Schmidtmann B, Guillaume Jc, et al. Risk of
malignancies in psoriasis patients treated with cyclosporine: a 5 y cohort study. J Invest
Dermatol 2003; 120:211-6.
Stern Rs, Nichols Kt Vakeva Lh. Malignant melanoma in patients treated for psoriasis with
methoxsalen (psoralen) and ultraviolet A radiation (PUVA). The PUVA Follow-Up Study.
N Engl J Med 1997; 336:1041-5.
Bovenschen Hj, Tjioe M, Vermaat H, De Hoop D, Witteman Bm, Janssens Rw, et al.
Induction of eruptive benign melanocytic naevi by immune suppressive agents, including
biologicals. Br J Dermatol 2006; 154:880-4.
Fulchiero Gj, Jr., Salvaggio H, Drabick Jj, Staveley-O'carroll K, Billingsley Em, Marks Jg,
et al. Eruptive latent metastatic melanomas after initiation of antitumor necrosis factor
therapies. J Am Acad Dermatol 2007; 56:S65-7.
Comte C, Guilhou Jj, Guillot B Dereure O. Rapid onset and fatal outcome of two squamous
cell carcinomas of the genitalia in a patient treated with etanercept for cutaneous psoriasis.
Dermatology 2008; 217:284-5.
Esser Ac, Abril A, Fayne S Doyle Ja. Acute development of multiple keratoacanthomas and
squamous cell carcinomas after treatment with infliximab. J Am Acad Dermatol 2004;
50:S75-7.
Fryrear Rs, 2nd, Wiggins Ak, Sangueza O Yosipovitch G. Rapid onset of cutaneous
squamous cell carcinoma of the penis in a patient with psoriasis on etanercept therapy. J Am
Acad Dermatol 2004; 51:1026.
Ly L Czarnecki D. The rapid onset of multiple squamous cell carcinomas during etanercept
treatment for psoriasis. Br J Dermatol 2007; 157:1076-8.
Maire C, Delesalle F, Carpentier O, Lequint P, Delaporte E Thomas P. [Multiple basal cell
carcinomas after etanercept treatment for psoriasis]. Ann Dermatol Venereol 2009; 136:3559.
Smith Kj Skelton Hg. Rapid onset of cutaneous squamous cell carcinoma in patients with
rheumatoid arthritis after starting tumor necrosis factor alpha receptor IgG1-Fc fusion
complex therapy. J Am Acad Dermatol 2001; 45:953-6.
Sheppard J, Raza K Buckley Cd. Skin cancer in psoriatic arthritis treated with anti-TNF
therapy. Rheumatology (Oxford) 2007; 46:1622-3.
Wolfe F Michaud K. Biologic treatment of rheumatoid arthritis and the risk of malignancy:
analyses from a large US observational study. Arthritis Rheum 2007; 56:2886-95.
Chakravarty Ef, Michaud K Wolfe F. Skin cancer, rheumatoid arthritis, and tumor necrosis
factor inhibitors. J Rheumatol 2005; 32:2130-5.
59
189.
190.
191.
192.
193.
194.
195.
196.
197.
198.
199.
200.
201.
202.
203.
204.
205.
206.
207.
208.
209.
Lebwohl M, Blum R, Berkowitz E, Kim D, Zitnik R, Osteen C, et al. No evidence for
increased risk of cutaneous squamous cell carcinoma in patients with rheumatoid arthritis
receiving etanercept for up to 5 years. Arch Dermatol 2005; 141:861-4.
Adams Ae, Zwicker J, Curiel C, Kadin Me, Falchuk Kr, Drews R, et al. Aggressive
cutaneous T-cell lymphomas after TNFalpha blockade. J Am Acad Dermatol 2004; 51:6602.
Dalle S, Balme B, Berger F, Hayette S Thomas L. Mycosis fungoides-associated follicular
mucinosis under adalimumab. Br J Dermatol 2005; 153:207-8.
Lafaille P, Bouffard D Provost N. Exacerbation of undiagnosed mycosis fungoides during
treatment with etanercept. Arch Dermatol 2009; 145:94-5.
Michot C, Costes V, Gerard-Dran D, Guillot B, Combes B Dereure O. Subcutaneous
panniculitis-like T-cell lymphoma in a patient receiving etanercept for rheumatoid arthritis.
Br J Dermatol 2009; 160:889-90.
Badgwell C Rosen T. Cutaneous sarcoidosis therapy updated. J Am Acad Dermatol 2007;
56:69-83.
Callejas-Rubio Jl, Ortego-Centeno N, Lopez-Perez L Benticuaga Mn. Treatment of therapyresistant sarcoidosis with adalimumab. Clin Rheumatol 2006; 25:596-7.
Heffernan Mp Anadkat Mj. Recalcitrant cutaneous sarcoidosis responding to infliximab.
Arch Dermatol 2005; 141:910-1.
Heffernan Mp Smith Di. Adalimumab for treatment of cutaneous sarcoidosis. Arch
Dermatol 2006; 142:17-9.
Mallbris L, Ljungberg A, Hedblad Ma, Larsson P Stahle-Backdahl M. Progressive
cutaneous sarcoidosis responding to anti-tumor necrosis factor-alpha therapy. J Am Acad
Dermatol 2003; 48:290-3.
Philips Ma, Lynch J Azmi Fh. Ulcerative cutaneous sarcoidosis responding to adalimumab.
J Am Acad Dermatol 2005; 53:917.
Stagaki E, Mountford Wk, Lackland Dt Judson Ma. The treatment of lupus pernio: results of
116 treatment courses in 54 patients. Chest 2009; 135:468-76.
Mitoma H, Horiuchi T, Tsukamoto H, Tamimoto Y, Kimoto Y, Uchino A, et al.
Mechanisms for cytotoxic effects of anti-tumor necrosis factor agents on transmembrane
tumor necrosis factor alpha-expressing cells: comparison among infliximab, etanercept, and
adalimumab. Arthritis Rheum 2008; 58:1248-57.
Gonzalez-Lopez Ma, Blanco R, Gonzalez-Vela Mc, Fernandez-Llaca H Rodriguez-Valverde
V. Development of sarcoidosis during etanercept therapy. Arthritis Rheum 2006; 55:817-20.
Ishiguro T, Takayanagi N, Kurashima K, Matsushita A, Harasawa K, Yoneda K, et al.
Development of sarcoidosis during etanercept therapy. Intern Med 2008; 47:1021-5.
Metyas Sk, Tadros Rm Arkfeld Dg. Adalimumab-induced noncaseating granuloma in the
bone marrow of a patient being treated for rheumatoid arthritis. Rheumatol Int 2009;
29:437-9.
Toussirot E, Pertuiset E, Kantelip B Wendling D. Sarcoidosis occuring during anti-TNFalpha treatment for inflammatory rheumatic diseases: report of two cases. Clin Exp
Rheumatol 2008; 26:471-5.
Peyri J, Moreno A Marcoval J. Necrobiosis lipoidica. Semin Cutan Med Surg 2007; 26:879.
Hu Sw, Bevona C, Winterfield L, Qureshi Aa Li Vw. Treatment of refractory ulcerative
necrobiosis lipoidica diabeticorum with infliximab: report of a case. Arch Dermatol 2009;
145:437-9.
Kolde G, Muche Jm, Schulze P, Fischer P Lichey J. Infliximab: a promising new treatment
option for ulcerated necrobiosis lipoidica. Dermatology 2003; 206:180-1.
Asteria Cr, Ficari F, Bagnoli S, Milla M Tonelli F. Treatment of perianal fistulas in Crohn's
disease by local injection of antibody to TNF-alpha accounts for a favourable clinical
response in selected cases: a pilot study. Scand J Gastroenterol 2006; 41:1064-72.
60
210.
211.
212.
213.
214.
215.
216.
217.
218.
219.
220.
221.
222.
223.
224.
225.
226.
227.
228.
Biancone L, Cretella M, Tosti C, Palmieri G, Petruzziello C, Geremia A, et al. Local
injection of infliximab in the postoperative recurrence of Crohn's disease. Gastrointest
Endosc 2006; 63:486-92.
Bokarewa M Tarkowski A. Local infusion of infliximab for the treatment of acute joint
inflammation. Ann Rheum Dis 2003; 62:783-4.
Kurzen H, Kurokawa I, Jemec Gb, Emtestam L, Sellheyer K, Giamarellos-Bourboulis Ej, et
al. What causes hidradenitis suppurativa? Exp Dermatol 2008; 17:455-6; discussion 457-72.
Blanco R, Martinez-Taboada Vm, Villa I, Gonzalez-Vela Mc, Fernandez-Llaca H, Agudo
M, et al. Long-term successful adalimumab therapy in severe hidradenitis suppurativa. Arch
Dermatol 2009; 145:580-4.
Fardet L, Dupuy A, Kerob D, Levy A, Allez M, Begon E, et al. Infliximab for severe
hidradenitis suppurativa: transient clinical efficacy in 7 consecutive patients. J Am Acad
Dermatol 2007; 56:624-8.
Giamarellos-Bourboulis Ej, Pelekanou E, Antonopoulou A, Petropoulou H, Baziaka F,
Karagianni V, et al. An open-label phase II study of the safety and efficacy of etanercept for
the therapy of hidradenitis suppurativa. Br J Dermatol 2008; 158:567-72.
Lee Ra, Dommasch E, Treat J, Sciacca-Kirby J, Chachkin S, Williams J, et al. A prospective
clinical trial of open-label etanercept for the treatment of hidradenitis suppurativa. J Am
Acad Dermatol 2009; 60:565-73.
Pelekanou A, Kanni T, Savva A, Mouktaroudi M, Raftogiannis M, Kotsaki A, et al. Longterm efficacy of etanercept in hidradenitis suppurativa: results from an open-label phase II
prospective trial. Exp Dermatol 2009.
Liu Yj. Thymic stromal lymphopoietin: master switch for allergic inflammation. J Exp Med
2006; 203:269-73.
Wang Yh, Ito T, Homey B, Watanabe N, Martin R, Barnes Cj, et al. Maintenance and
polarization of human TH2 central memory T cells by thymic stromal lymphopoietinactivated dendritic cells. Immunity 2006; 24:827-38.
Zink A, Askling J, Dixon Wg, Klareskog L, Silman Aj Symmons Dp. European biologicals
registers: methodology, selected results and perspectives. Ann Rheum Dis 2009; 68:1240-6.
Gomez-Reino Jj, Carmona L Angel Descalzo M. Risk of tuberculosis in patients treated
with tumor necrosis factor antagonists due to incomplete prevention of reactivation of latent
infection. Arthritis Rheum 2007; 57:756-61.
Schmitt-Egenolf M. Psoriasis therapy in real life: the need for registries. Dermatology 2006;
213:327-30.
Lecluse Ll, Naldi L, Stern Rs Spuls Pi. National registries of systemic treatment for
psoriasis and the European 'Psonet' initiative. Dermatology 2009; 218:347-56.
Schmitt-Egenolf M. PsoReg--the Swedish registry for systemic psoriasis treatment. The
registry's design and objectives. Dermatology 2007; 214:112-7.
Nast A, Reytan N, Rosumeck S, Erdmann R Rzany B. Low prescription rate for systemic
treatments in the management of severe psoriasis vulgaris and psoriatic arthritis in
dermatological practices in Berlin and Brandenburg, Germany: results from a patient
registry. J Eur Acad Dermatol Venereol 2008; 22:1337-42.
Driessen Rj, Boezeman Jb, Van De Kerkhof Pc De Jong Em. Three-year registry data on
biological treatment for psoriasis: the influence of patient characteristics on treatment
outcome. Br J Dermatol 2009; 160:670-5.
Warren Rb, Brown Bc, Lavery D, Ashcroft Dm Griffiths Ce. Biologic therapies for
psoriasis: practical experience in a U.K. tertiary referral centre. Br J Dermatol 2009;
160:162-9.
Olleros Ml, Vesin D, Lambou Af, Janssens Jp, Ryffel B, Rose S, et al. Dominant-negative
tumor necrosis factor protects from Mycobacterium bovis Bacillus Calmette Guerin (BCG)
and endotoxin-induced liver injury without compromising host immunity to BCG and
Mycobacterium tuberculosis. J Infect Dis 2009; 199:1053-63.
61
229.
230.
231.
232.
233.
234.
235.
236.
237.
Shibata H, Yoshioka Y, Abe Y, Ohkawa A, Nomura T, Minowa K, et al. The treatment of
established murine collagen-induced arthritis with a TNFR1-selective antagonistic mutant
TNF. Biomaterials 2009; 30:6638-47.
Dasgupta S, Murumkar Pr, Giridhar R Yadav Mr. Current perspective of TACE inhibitors: a
review. Bioorg Med Chem 2009; 17:444-59.
Ivanenkov Ya, Balakin Kv Tkachenko Se. New approaches to the treatment of inflammatory
disease : focus on small-molecule inhibitors of signal transduction pathways. Drugs R D
2008; 9:397-434.
Le Buanec H, Delavallee L, Bessis N, Paturance S, Bizzini B, Gallo R, et al. TNFalpha
kinoid vaccination-induced neutralizing antibodies to TNFalpha protect mice from
autologous TNFalpha-driven chronic and acute inflammation. Proc Natl Acad Sci U S A
2006; 103:19442-7.
Delavallee L, Semerano L, Assier E, Vogel G, Vuagniaux G, Laborie M, et al. Active
immunization to tumor necrosis factor-alpha is effective in treating chronic established
inflammatory disease: a long term study in a transgenic model of arthritis. Arthritis Res Ther
2009; 11:R195.
Powell Rj Gardner-Medwin Jm. Guideline for the clinical use and dispensing of
thalidomide. Postgrad Med J 1994; 70:901-4.
Shurafa M Kamboj G. Thalidomide for the treatment of bleeding angiodysplasias. Am J
Gastroenterol 2003; 98:221-2.
Perez-Encinas M, Rabunal Martinez Mj Bello Lopez Jl. Is thalidomide effective for the
treatment of gastrointestinal bleeding in hereditary hemorrhagic telangiectasia?
Haematologica 2002; 87:ELT34.
Gullestad L, Semb Ag, Holt E, Skardal R, Ueland T, Yndestad A, et al. Effect of
thalidomide in patients with chronic heart failure. Am Heart J 2002; 144:847-50.
62
Appendix
63
64
Appendix 1
Laffitte E, Revuz J. Thalidomide: an old drug with new clinical applications.
Expert Opin Drug Saf. 2004;3:47-56.
65
66
Review
General
bi
te
d
Thalidomide: an old drug with
new clinical applications
Emmanuel Laffitte & Jean Revuz†
Department of Dermatology, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne,
Switzerland; and †Université Paris XII, Hôpital Henri Mondor (AP-HP), Créteil, France
oh
i
1. Introduction
pr
2. Pharmacology
3. Biological properties
Thalidomide has several targets and mechanisms of action: a hypnosedative
effect, several immunomodulatory properties with an effect on the production of TNF-α and the balance between the different lymphocyte subsets
and an antiangiogenic action. Thalidomide has been used in several cutaneous inflammatory disorders (e.g., erythema nodosum leprosum in lepromatous leprosy, cutaneous lupus erythematosus and severe aphtosis),
cancers (e.g., relapsed/refractory multiple myeloma, malignant melanoma
and systemic signs in cancer) and inflammatory conditions (e.g., Crohn’s disease and rheumatoid arthritis). Several side effects are associated with thalidomide. Some are major, such as teratogenicity, peripheral neuropathy
and deep vein thrombosis. Somnolence and rash are frequently reported
when thalidomide is used at higher doses as an anticarcinogenic agent and
can lead to dose reduction or treatment discontinuation depending on
severity. Minor side effects include abdominal pain and endocrine disturbances. To prevent the teratogenicity, use of thalidomide is strictly controlled in western countries with close adherence to a birth control
programme. Close monitoring for early development of peripheral neuropathy is also recommended.
tly
4. Thalidomide derivatives
ric
5. Clinical applications
st
6. Side effects
io
n
7. Guidelines for the clinical use
of thalidomide
ib
ut
8. Thalidomide on the net
d.
Pr
in
tin
g
an
d
di
s
tr
9. Expert opinion
ns
Lt
Keywords: cutaneous inflammatory disorders, deep vein thrombosis (DVT),
peripheral neuropathy, relapsed/refractory multiple myeloma, teratogenicity, thalidomide, TNF-α
C
op
yr
ig
ht
of
A
sh
le
y
Pu
b
lic
at
io
Expert Opin. Drug Saf. (2004) 3(1):47-56
Ashley Publications
www.ashley-pub.com
1. Introduction
Thalidomide was first synthesised in 1954 by the German pharmaceutical firm
Chemie Grünenthal, and was marketed in Europe in October 1957 as an
antiemetic and non-barbiturate sedative hypnotic [1]. The first pharmacological
studies performed on rodents showed a fast sedative effect and remarkably low
toxicity even at high doses. Between 1957 and 1961, thalidomide was widely
used by pregnant women for its antiemetic effect in the treatment of morning
sickness [2]. A significant teratogenic effect of thalidomide was reported in 1961
[3] after a rise in reported cases of phocomelia, a previously rare congenital malformation. Almost 6000 cases of internal or external deformities were attributed
to thalidomide during this period [2,4] and the drug was withdrawn from the market. In 1965, a dramatic improvement of erythema nodosum leprosum (ENL)
treated with thalidomide was reported by Sheskin [5], and the discovery in 1991
of thalidomide’s anti-TNF-α activity [6] led to renewed interest in this drug.
Since then, this anti-TNF- α effect has been studied, with several clinical indications under investigation. There are two main avenues of current research:
immunomodulatory action in various inflammatory diseases and antiangiogenic
action, which seems to be of interest in oncology.
2004 © Ashley Publications Ltd ISSN 1474-0338
47
Thalidomide: an old drug with new clinical applications
3. Biological
Thalidomide, or α-(N-pthalimido)-glutarimide, is a glutamic
acid derivative. The molecule is a racemic mixture of the (S)
and (R) enantiomers. There is some evidence to suggest that
the two enantiomers act differently: the (R) enantiomer could
be responsible for the sedative effect [7], whilst the (S) enantiomer could have the immunomodulatory, antiangiogenic [8]
and teratogenic properties, although this hypothesis is debatable [9]. However, in humans, this difference is not relevant
since chiral interconversion between the two enantiomers
in vivo leads to a racemic mixture in 2 h [10]. The solubility of
this lipophilic molecule is low in water and alcohol and the
molecule is sensitive to hydrolysis at a pH of > 6 [1,11].
The pharmacokinetics of thalidomide have been studied
both in humans and animals [12-15]. After oral absorption in
healthy volunteers, the peak plasma concentration is reached in
3.2 ± 1.4 – 4.39 ± 1.27 h (Tmax) [12,13]; this is delayed by consumption of a high-fat meal [16]. The apparent volume of distribution (Vd) is very broad, 120 l [14], with a rapid penetration
of the haematoencephalic and placental barriers [17]. Animal
studies have shown that thalidomide is distributed in all tissues,
with a predilection for the digestive tract and the kidneys [18].
The principal metabolic pathway is probably non-enzymatic hydrolysis, leading to at least 12 breakdown products,
some of which could have their own pharmacological activity [19]. Hydroxylated products have also been detected, suggesting that enzymes from the cytochrome P450 family
could be involved [20].
Excretion of thalidomide and its metabolites is mainly
via the kidneys. The plasma half-life ranges from
6.17 ± 2.56 to 8.70 ± 4.11 h [12-14]. Excretion of thalidomide in semen was studied in rabbits. After two oral doses
separated by 18 h, thalidomide was found in semen from
the 6th hour until the 12th day. Thalidomide was not only
present in the seminal fluid but was also firmly fixed on
spermatozoans [21]. In humans, thalidomide is also present
in semen. After an oral dose of 100 mg/day, thalidomide
was detected in semen at week 4 with a correlation between
plasma and semen levels [22].
In a recent study, the pharmacokinetics of a single oral dose
of 100 or 200 mg of thalidomide was assessed in
14 asymptomatic HIV-infected men [23]. Overall, the results
were consistent with those provided previously, with, for
100 and 200 mg, respectively: Tmax of 2.5 ± 1.5 and 3.3 ± 1.4 h;
a half-life of 4.6 ± 1.2 and 5.3 ± 2.2 h; and an apparent Vd of
70 ± 16 and 83 ± 35 l.
There is no parenteral preparation for thalidomide. The
dermal absorption of thalidomide is very low and therefore it
may not be appropriate for topical delivery. Analogues have
been synthesised and a methyl derivative could have better
dermal penetration [24].
Thalidomide enhances the activity of alcohol, barbiturates,
chlorpromazine and reserpine [11,20] but does not affect the pharmacokinetics of orally-administered hormonal contraceptives [25].
3.1 Hypnosedative action
st
3.2 Immunological properties
ric
tly
pr
oh
i
bi
te
The sedative properties of thalidomide are not well-understood. Thalidomide acts by a different mechanism to
barbiturates, possibly involving activation of sleep centres
that depend on GABA receptors [14]. The effect of thalidomide on sleep is very particular, and differs from all other
hypnotic drugs by increasing the time spent in Phases 3 – 4
and REM (rapid eye movement) and decreasing the time
spent in Phase I [26]. This sedative action is preferentially
related to the (R) enantiomer [7].
tin
g
an
d
di
s
tr
ib
ut
io
n
Thalidomide is able to modify inflammatory processes and
modulate immune reactions [27]. There is an abundance of data,
sometimes contradictory, available concerning the immunomodulatory action of thalidomide at the cellular and molecular
levels both in vivo and in vitro. Thalidomide’s effects are clearly
different from corticoids, cyclosporin, FK-506, and phosphodiesterase inhibitors such as pentoxifylline [1].
Thalidomide seems to have both inhibitory and stimulatory actions on different cellular immunity effectors. These
dichotomous actions may, in part, be explained by the
recently recognised ability of thalidomide to act as a T cell costimulant under certain circumstances. Thalidomide has an
inhibitory effect on mononuclear cells by decreasing their
chemotactic and phagocytic capacities [20]. The lymphocytic
proliferation induced by allogenic, superantigenic or
mitogenic stimulation is inhibited by thalidomide, with an
additive effect by cyclosporin A [20,28,29]. Furthermore, thalidomide modulates the balance between the different classes of
lymphocytes. In vitro studies show that the CD8+ cytotoxic
response is stimulated compared to the CD4+ response [30].
An increased CD4+/CD8+ ratio was found in the blood and
the cutaneous lesions of patients with ENL. An inversion of
this ratio was observed in some of these patients treated with
thalidomide [31], which could be one of thalidomide’s effects
in ENL. Moreover, thalidomide acts in vitro by skipping the
TH1 lymphocyte response towards a TH2 type [32]. Thalidomide has been shown to enhance production of IL-4 and -5,
promoting the shift from a TH1 to a TH2 cytokine pattern.
This effect could be of interest in various pathologies associated with dysregulation of lymphocyte subpopulations [33].
One of the most significant properties of thalidomide is its
inhibition of TNF-α synthesis by activated human monocytes
[6]. The mechanism by which thalidomide suppresses TNF-α
remains unclear. It appears to enhance the degradation of
TNF-α mRNA [34] and could interact with two intracellular
glycoproteins with anti-TNF-α properties [19]. This
anti-TNF-α activity was confirmed in vivo in patients with
ENL, tuberculosis and in HIV-infected patients [35]. However,
contradictory results were obtained both in vitro and in vivo
for the anti-TNF-α properties of thalidomide. Recent data
demonstrate that thalidomide may exert a bidirectional
Pr
in
d.
Lt
ns
io
at
lic
Pu
b
y
le
A
sh
of
ht
yr
ig
C
op
48
properties
d
2. Pharmacology
Expert Opin. Drug Saf. (2004) 3(1)
Laffitte & Revuz
these compounds to be clinically effective with reduced toxicity, but they are still under investigation [52,53].
applications
bi
te
d
5. Clinical
g
an
d
di
s
tr
ib
ut
io
n
st
ric
tly
pr
oh
i
Thalidomide has been used in several cutaneous inflammatory disorders. Its efficiency has been proven in ENL, severe
aphtosis (either isolated or associated with Behçet’s disease or
HIV infection), Jessner–Kanoff lymphocytic infiltration,
resistant cutaneous lupus, and chronic graft-versus-host reactions. Some other dermatological indications may be of interest, such as prurigo, HIV infection, cutaneous sarcoidosis,
chronic or recurrent erythema multiforme, pseudolymphomas, and numerous other inflammatory dermatoses in single
case reports [20,54-56]. Considering the good results obtained
with the new biological anti-TNF-α compounds, the use of
thalidomide in other inflammatory diseases, such as rheumatoid arthritis, ankylosing spondylitis or inflammatory bowel
diseases, is still under debate [57].
Thalidomide has been shown to be an active and promising
anticarcinogenic agent, both as a single agent or in combination with dexamethasone or other chemotherapeutic agents,
in haematological malignancy, such as relapsing or refractory
multiple myeloma, myelodysplasia or acute myeloid leukaemia (reviewed well in [46,58]), and also in solid tumours such as
malignant glioma, prostatic, colorectal or renal cell carcinoma
[46]. The best response rates have been observed with relapsing
or refractory multiple myeloma, ranging 25 – 69% [58]. Thalidomide could be of interest in cancer cachexia and for distressing night sweats in advanced malignant disease [59,60].
The dosage and duration of treatment differ in inflammatory
and neoplastic diseases. A daily dose of ≤ 200 mg is usually
enough to control ENL, severe aphtosis or cutaneous lupus,
and the dose can progressively be reduced, whilst in malignancy, thalidomide is started at 200 mg/day and progressively
increased to 400 – 800 mg/day for several months [46,58].
tin
dose-dependent effect on TNF-α production, depending on
cell type and method of cellular activation. Thus, under certain experimental conditions, TNF-α production is significantly enhanced by thalidomide in vitro [36]. Furthermore,
increased levels of TNF-α in serum have been observed in
patients with toxic epidermal necrolysis treated with thalidomide [37]. It is noteworthy that in this double-blind, placebocontrolled trial, treatment with thalidomide was associated
with increased mortality. Increased levels of TNF-α were also
observed among HIV-infected patients treated with thalidomide for oral ulcerations [38].
More recently, thalidomide has been shown to inhibit
NF-κB activation, a ubiquitous transcription factor of
upmost importance in the response of the host to inflammatory stimuli, through suppression of inhibitor κB (I-κB)
kinase activity [27,39].
Together, these data suggest that thalidomide has a complex
action on the immune system: in conditions characterised by
monocyte/macrophage activation and high circulating concentrations of TNF-α, such as ENL, the use of thalidomide to
inhibit production of TNF-α may be beneficial. However, in
diseases where T cell activation contributes to the pathogenic
process, further T cell stimulation by thalidomide may be detrimental and result in clinical deterioration [40].
Pr
in
3.3 Antiangiogenic properties
6.
Side effects
C
op
yr
ig
ht
of
A
sh
le
y
Pu
b
lic
at
io
ns
Lt
d.
The antiangiogenic properties of thalidomide were first demonstrated in vivo in a rabbit cornea model [41]. This property is distinct from the anti-TNF-α action [8] and is probably responsible
for the teratogenic effects [42]. The inhibition of neovascularisation induced by thalidomide is mediated by inhibition of angiogenic factors such as vascular endothelial growth factor (VEGF)
[43] and basic fibroblast growth factor (bFGF) [44]. At a molecular
level, thalidomide, or a breakdown product of thalidomide, could
decrease the transcription efficiency of genes related to those angiogenic factors by specifically intercalating into their promoter
sites [42]. This inhibition requires metabolic activation, which is
species-dependent [45]. These metabolites can be formed in both
humans and rabbits but not in some species of rodents in which
thalidomide has no antiangiogenic or teratogenic effects [45].
The antiangiogenic activity of thalidomide seems particularly interesting in the treatment of malignancies, where angiogenesis has been shown to play an important role [46,47]. In
experimental models of tumours and metastases, thalidomide
has been shown to induce an intratumoural hypoxia, to
reduce tumour blood vessel density and tumour growth, and
to decrease the risk of metastases [48,49].
4. Thalidomide
derivatives
With the ‘rediscovery’ of thalidomide, several structural analogues have been developed in an attempt to discover compounds with thalidomide’s immunomodulatory properties
without the associated side effects [50,51]. Preliminary results
from human studies in vitro and in vivo have shown some of
Thalidomide’s side effects are listed in Box 1. As the number of
patients receiving thalidomide for longer periods of time and at
higher doses increases (in particular, for relapsing multiple myeloma or in HIV patients), several previously unrecognised or
underestimated adverse effects have recently been observed.
Some side effects can be considered as major and may have serious consequences (teratogenicity, peripheral neuropathy and
deep vein thrombosis [DVT]). Some side effects are usually
considered minor, as they tend to appear at the beginning of
treatment and generally disappear after dose tapering. However,
they may act as serious dose-limiting factors or lead to treatment
interruption when thalidomide is used at higher doses as an
anticarcinogenic agent (in particular, somnolence, constipation
and rash). The incidence of each side effect is not accurately
known and tends to vary in different studies, depending on the
disease and the administered dose of thalidomide.
Expert Opin. Drug Saf. (2004) 3(1)
49
Thalidomide: an old drug with new clinical applications
6.2 Major side effects
Box 1. Adverse effects of thalidomide [20,55,56].
oh
i
ric
tly
pr
Minor (but may be dose-limiting side effects for
higher doses)
Somnolence
Constipation
Weight gain
Morbilliform or maculopapular rash
tin
g
an
d
di
s
tr
ib
ut
io
n
st
Less frequent side effects
Cutaneous
Erythema multiforme
Toxic epidermal necrolysis
DRESS
Allergic vasculitis
Erythroderma
ENL
Brittle finger nails
Dry mouth
Pruritus
Pustuloderma
Red palms
ns
Lt
d.
Pr
in
Endocrinological
Hypothyroidism
Amenorrhoea
Genital bleeding
Galactorrhoea
Hypoglycemia/hyperglycemia
at
io
Haematological
Leukopenia
Pu
b
y
le
yr
ig
ht
of
A
sh
Gastrointestinal
Abdominal distension
Increased appetite
Nausea
Hepatitis
lic
Neuropsychological
Headache
Intermittent shaking
Reversible dementia
Depression
Loss of libido
op
DRESS: Drug rash with eosinophilia and systemic symptoms;
DVT: Deep vein thrombosis; ENL: Erythema nodosum leprosum.
C
The discovery of the teratogenic properties of thalidomide was a
surprise, since premarketing animal studies, only performed in
rats [1], did not detect it. Later studies showed that rats and mice
are less sensitive to the teratogenic effects of thalidomide [61,62].
The major susceptibility of the human embryo to the
effects of thalidomide seems to occur between 27 and 50 days
after conception; a single dose of 100 mg is enough to cause
harm [63]. The frequency of malformations after in utero exposure has been estimated to be in the range 15 – 100%. The
most frequent fetal abnormalities seen in humans are limb
defects (75% of the cases) but other abnormalities such as
craniofacial abnormalities, malformations of internal organs
and central skeletal abnormalities have been observed [2].
The specific mechanism of this embryopathy is not yet
clear and is probably complex, with 24 potential mechanisms of action listed [64]. The most recent data suggest that
the embryotoxic activity could be related to the formation,
under the effect of the prostaglandin H-synthetase, a species-dependent enzyme, of a teratogenic metabolite. This
metabolite could induce the production of free radicals
responsible for DNA oxidation in the embryonic cells [65].
The antiangiogenic properties of thalidomide may also play
a part in teratogenesis [42].
There is a potential risk for teratogenic effects of thalidomide in the treated male, as the molecule is distributed into
semen. Congenital malformations have been observed in rabbits born as a result of breeding experiments with males having a prolonged intake of thalidomide [21]. Such an effect has
not yet been described in humans, but since thalidomide is
distributed into human semen after oral dosing, there could
be a potential risk in treated male patients [22].
The teratogenic effects of thalidomide are currently wellcontrolled in western countries, with the delivery of the product being restricted to patients using effective methods of contraception and women managed by repeated pregnancy tests.
This is not true everywhere in the world, and at least 34 cases of
embryopathy after exposure to thalidomide have been reported
in South American lepromatous endemic areas since 1965 [66].
The possibility of a mutagenic effect was raised in 1994 by
McBride (who had described the teratogenic effects in 1961)
following two observations of limb malformations in children
born to fathers with thalidomide embryopathy [67]. The
imputability of thalidomide in the two cases observed was
low, and more than 350 victims of thalidomide indexed in
England had normal children [68-70]. However, large studies
were performed in humans and animals, indicating that thalidomide was devoid of mutagenic activity [71,72].
bi
te
Frequent side effects
Major
Teratogenicity
Peripheral neuropathy
DVT
6.1 Toxicity
The acute toxicity of thalidomide is so low that the toxicological studies conducted in rodents in the 1950s failed to show
lethality, even when at doses in excess of 10,000 mg/kg [1].
Accidental or voluntary overdosing never had any serious consequences, even for doses of 14 g [20].
50
d
6.2.1 Teratogenic effects
6.2.2 Peripheral neuropathy
As the teratogenicity of thalidomide can be controlled by
appropriate contraceptive methods, the neurotoxicity of the
drug is now one of the main factors limiting its use for a prolonged period [20,73], especially in cutaneous inflammatory
Expert Opin. Drug Saf. (2004) 3(1)
Laffitte & Revuz
st
ric
tly
pr
oh
i
bi
te
d
thalidomide every other day, on alternate weeks or for brief
monthly courses has been suggested to minimise the risk of
polyneuropathy. However, no studies of these alternative
courses have been performed.
It is recommended that a baseline nerve conduction study
should be performed in all patients who receive thalidomide
within 3 months of initiating therapy and then repeated every
6 months thereafter [85]. If nerve conduction amplitudes are
decreased by > 30% from baseline, more frequent testing is
recommended [76]. Thalidomide should be discontinued if
nerve conduction amplitudes are decreased by ≥ 50%. Thalidomide therapy can be cautiously restarted after symptoms of
neuropathy resolve [73].
io
n
6.2.3 Thalidomide and thromboses
g
an
d
di
s
tr
ib
ut
As the use of thalidomide expands, a higher incidence of DVT or
pulmonary embolism has been recently reported among patients
receiving thalidomide in combination with glucocorticoids or
multi-agent chemotherapy for multiple myeloma, myelodysplasic
syndromes or various carcinomas [88]. The reported rates of these
events varied from 0 to 43% of treated patients and occurred at a
mean of 2 months after the introduction of thalidomide treatment. Ten cases have been reported in patients taking thalidomide for inflammatory dermatoses such as lupus or aphtosis
[89-93]. All of these patients had different predisposing factors,
such as antiphospholipid syndrome, trauma or Behçet’s disease.
In cancer patients, DVTs were safely treated with anticoagulation and did not necessarily warrant discontinuation of
thalidomide [88]. On the other hand, in patients with inflammatory diseases, thromboembolic events were particularly
severe and extensive even after anticoagulation, and thalidomide had to be discontinued.
There is no clear explanation about the thrombogenic
effect of thalidomide, but some hypotheses have been suggested. For example, thalidomide, chemotherapy and glucocorticoids could increase activation of tissue factor in the
plasma membrane of tumour cells by way of apoptosis [94].
This phenomenon could be dose-related, since no case has
been recorded during a prospective survey of 170 patients
treated with daily doses of ≤ 100 mg [85].
Together, clinical data suggest that thalidomide could have
a thrombogenic effect at a daily dose of > 100 mg in patients
with predisposing diseases such as multiple myeloma or solid
carcinoma, Behçet’s disease or antiphospholipid syndrome,
and when glucocorticoids or multi-agent chemotherapy are
associated with thalidomide; all such patients should be carefully monitored when treatment with thalidomide is started.
C
op
yr
ig
ht
of
A
sh
le
y
Pu
b
lic
at
io
ns
Lt
d.
Pr
in
tin
disorders. The exact mechanism of thalidomide-induced neuropathy is still unknown. An individual susceptibility has
been suggested but no correlation with the genetic differences
in drug metabolism has been found [74]. Thalidomide neuropathy is known to be an axonal, bilateral and symmetrical
polyneuropathy, mainly sensory and particularly involving
distal extremities. Clinical manifestations of thalidomideinduced neuropathy consist mainly of symmetrical distal
painful paresthesia with or without sensory loss in the lower
limbs [20]. Electrophysiological findings are those of a sensory
axonal polyneuropathy with reduction of sensory nerve action
potential (SNAP) amplitude and relative conservation of
nerve conduction velocities [75]. A 50% decrease of sural
SNAP amplitude has been reported to be the best electrophysiological criterion, as SNAP amplitude is closely related to the
clinical sensory signs and symptoms [75,76].
Various estimates of the prevalence of thalidomide-induced
neuropathy have been made in retrospective studies, from
< 1% in 34 patients treated for lepra reactions [77], to > 70% in
a small series of patients (four to eight) treated for prurigo
nodularis [78-80]. A prevalence of 25% was reported in a series
of 60 patients treated for discoid lupus erythematosus over a
2-year period (400 mg/day, followed by 50 – 10 0mg/day) [81].
In a retrospective study of 42 patients, a prevalence rate of definite thalidomide neuropathy of 21% [82] was observed. In a
recent series of patients with refractory multiple myeloma
treated with high doses of thalidomide, i.e., 200 – 800 mg/day,
neuropathy was reported to occur in 10 – 30% of treated
patients [83,84], but the clinical and electrophysiological criteria
for neuropathy were not clearly specified. This variability in
prevalence has been interpreted as reflecting a disease-related
susceptibility. In fact, the retrospective nature of the studies,
the large range of daily doses used and the heterogeneity of the
clinical and electrophysiological criteria considered for the
diagnosis of neuropathy preclude a real estimation of the prevalence rate and risk factors of thalidomide neuropathy. Thalidomide-induced neuropathy was recently prospectively
evaluated among 135 patients treated for various dermatological diseases for 2 years [85]. Definite neuropathy (i.e., electrical
plus clinical signs) was present in 25% of the patients, but clinical or electrophysiological evidence of a thalidomide-induced
neuropathy were present in 56% of the patients. The incidence
rate was maximal during the first year of treatment (20%). The
risk of neuropathy was related to the daily dose, whatever the
duration of treatment, and the risk seemed to be negligible for
doses of < 25 mg/day, whatever the duration of therapy. After
peripheral neuropathy develops, it resolves slowly and is sometimes irreversible [82,86,87]. In a follow-up of thalidomideinduced neuropathy over 4 – 6 years, ∼ 25% of patients made
a full recovery, 25% had a slow improvement and 50% had
persistent sensory symptoms [82,86,87]. In a few patients, recovery did not begin for years. Sural nerve biopsies showed severe
degeneration of large axons with little sign of regeneration. In
other patients, electrophysiological abnormalities worsened
after discontinuation of thalidomide [75]. The use of
6.3 Minor side effects
The most common side effects are neuropsychological, digestive, endocrinological and cutaneous.
6.3.1 Neuropsychological
In 33 – 100% of the cases [11], somnolence (45 – 90%), asthenia, drowsiness, cephalgias, decreased libido or depressive
Expert Opin. Drug Saf. (2004) 3(1)
51
bi
te
oh
i
pr
tly
ric
st
io
n
ut
ib
tr
di
s
d
disorders
Several studies in the 1950s and 60s reported the effects of thalidomide on the endocrine system. More recently, hypothyroidism and significant increases in serum thyroid-stimulating
hormone (TSH) levels have been found after 2 – 6 months in
20 – 74% of patients treated with thalidomide for multiple
myeloma [97]. Thalidomide therapy can result in constipation,
fatigue, lack of energy, and bradycardia, but these signs may
also be manifestations of hypothyroidism, and the authors recommend assessment of serum TSH levels before starting thalidomide and every 3 months afterwards or if the diagnosis of
hypothyroidism is suspected. Secondary amenorrhoea has been
reported in ten women treated with thalidomide for aphtosis
or lupus [98-101]. The amenorrhoea occurred 4 – 7 months following the start of treatment and resolved after the discontinuation of thalidomide. Re-introduction of thalidomide in two
patients again induced amenorrhea. Increased FSH and luteinising hormone (LH) levels with low oestradiol levels were consistent with a menopausal profile, suggesting a peripheral
rather than central action.
d.
Pr
in
6.3.3 Endocrinological
an
Constipation (15 – 50% of cases), weight gain (30% of cases),
xerostomia, abdominal pain, and nausea may occur frequently. Severe hepatic toxicity has once been reported [96].
g
6.3.2 Digestive
unacceptable disruption to normal life and only after other
treatments have been tried and then subsequently fail.
Approval is usually on an individual patient basis. Thalidomide is prescribed in an off-label setting in most countries.
In France, thalidomide has been approved since
February, 1997 for ENL, Jessner–Kanoff lymphocytic infiltration, resistant cutaneous lupus, chronic graft-versus-host
reactions, severe aphtosis either isolated or associated with
Behçet’s disease and HIV infection, and, more recently,
resistant multiple myeloma. In the US, thalidomide has been
approved since July, 1998 for ENL. The US safety programme for thalidomide has been described previously and is
published as STEPS® (System for Thalidomide Education
and Prescribing Safety) [107].
Before treatment, patients must be informed of the associated risks, side effects and the nature of any alternative treatments using registered drugs. Patients should be in a position
to give informed consent and to receive a detailed information sheet about the drug. In women of childbearing age,
pregnancy should be excluded with a negative test prior to
prescribing. If hormonal contraceptives are the chosen means
of preventing pregnancy whilst taking thalidomide, then
they should be taken for at least 1 month prior to commencing thalidomide treatment. Men taking thalidomide should
be advised to wear condoms during sexual intercourse, as
thalidomide has been detected in semen. Clinical neurological examination and electrophysiological measurements are
to be recorded when treatment is started. Risk factors for
thromboembolism should be recorded and TSH levels
should be determined.
During treatment, pregnancy tests and clinical neurological examinations should be performed monthly and electrophysiological measurements every 6 months. Patients must
be educated about the symptoms of peripheral neuropathy
and instructed to consult their doctor for electrophysiological testing in the event that such symptoms appear.
After cessation of thalidomide, pregnancy should be
avoided for 1 month in women, and condoms should be
worn by men for at least 3 months (corresponding to a
spermatogenesis cycle).
tin
syndrome are currently observed. More recently, a reversible
dementia was reported [95].
Lt
6.3.4 Cutaneous side effects
C
op
yr
ig
ht
of
A
sh
le
y
Pu
b
lic
at
io
ns
Various dermatological side effects of thalidomide have been
reported but, recently, with the use of higher doses, their
prevalence appears to be higher than previously expected
[102,103]. Skin eruptions have been noted in 46% of myeloma
patients taking thalidomide alone or in combination with
dexamethasone [102]. Cutaneous side effects are also more
common in HIV-infected patients treated with thalidomide
compared to non-infected individuals treated with the drug.
In a series of 56 HIV-infected patients treated with thalidomide for 14 – 21 days, 27% stopped taking thalidomide
because of cutaneous side effects [103]. The more immunosuppressed the HIV infected individual, the more likely they
were to experience side effects.
These eruptions can be minor-to-moderate, for example,
morbilliform or maculopapular rash, but severe skin reactions (drug rash with eosinophilia and systemic symptoms
[DRESS] [104], exfoliative erythroderma [105], erythema
multiforme or toxic epidermal necrolysis [102,106]) have
been observed.
7. Guidelines
for the clinical use of thalidomide
Thalidomide is currently available only through special
access schemes that differ from country to country. Clinical
use is restricted to severe disabling conditions that cause an
52
d
Thalidomide: an old drug with new clinical applications
8. Thalidomide
on the net
Several websites can be consulted on the net:
• Thalidomide Victims Association of Canada (TVAC)
(http://www.thalidomide.ca).
• US FDA/Center for Drug Evaluation and Research (CDER)
(http://www.fda.gov/cder/news/thalinfo). The information
presented on this page includes consumer and patient information, thalidomide advisory committee and workshop
transcripts, the approved labelling text and the medical
review on which the decision to approve this drug was based.
Also included are selected links to other websites containing
information on thalidomide.
Expert Opin. Drug Saf. (2004) 3(1)
Laffitte & Revuz
bi
te
oh
i
The authors would like to thank J Bryant for reading the
manuscript and for his helpful suggestions.
Bibliography
9.
Papers of special note have been highlighted as
either of interest (•) or of considerable interest (••)
to readers.
WNENDT S, ZWINGENBERGER K:
Thalidomide’s chirality. Nature (1997)
385:303-304.
10.
ERIKSSON T, BJORKMAN S, ROTH B,
FYGE A, HOGLUND P:
Stereospecific determination,
chiral inversion in vitro and
pharmacokinetics in humans of the
enantiomers of thalidomide.
Chirality (1995) 7:44-52.
4.
MELLIN GW, KATZENSTEIN M:
The saga of thalidomide:
neuropathy to embryopathy, with case
reports and congenital abnormalities.
N. Engl. J. Med. (1963) 267:1184-1193.
at
lic
Pu
b
13.
SHESKIN J: Thalidomide in the treatment
of lepra reactions. Clin. Pharmacol. Ther.
(1965) 6:303-306.
6.
SAMPAIO EP, SARNO EN, GALILLY R,
COHN ZA, KAPLAN G: Thalidomide
selectively inhibits tumour necrosis factor α
production by stimulated human monocytes.
J. Exp. Med. (1991) 173:699-703.
yr
ig
ht
of
A
sh
le
y
5.
op
C
8.
ut
ib
tr
di
s
MCHUGH SM, ROWLAND TL:
Thalidomide and derivatives: immunological
investigations of tumour necrosis factor-α
(TNF-α) inhibition suggest drugs capable of
selective gene regulation.
Clin. Exp. Immunol. (1997) 110:151-154.
20.
TSENG S, PAK G, WASHENIK K,
POMERANZ MK, SHUPACK JL:
Rediscovering thalidomide: a review of its
mechanism of action, side effects and
potential uses. J. Am. Acad. Dermatol. (1996)
35:969-979.
21.
LUTWAK-MANN C, SCHMID K,
KEBERLE H: Thalidomide in rabbit semen.
Nature (1967) 214:1018-1020.
22.
TEO SK, HARDEN JL, BURKE AB et al.:
Thalidomide is distributed into human
semen after oral dosing. Drug Metab. Dispos.
(2001) 29:1355-1357.
23.
NOORMOHAMED FH, YOULE MS,
HIGGS CJ et al.: Pharmacokinetics and
hemodynamic effects of single oral doses of
thalidomide in asymptomatic human
immunodeficiency virus-infected subjects.
AIDS Res. Hum. Retroviruses (1999)
15:1047-1052.
HOGLUND P, ERIKSSON T,
BJORKMAN S: A double-blind study of the
sedative effects of the thalidomide
enantiomers in humans. J. Pharmacokinet.
Biopharm. (1998) 26:363-383.
24.
HADGRAFT J, GOOSEN C,
DU PLESSIS J, FLYNN G:
Predicting the dermal absorption of
thalidomide and its derivatives.
Skin Pharmacol. Appl. Skin Physiol. (2003)
16:123-129.
KENYON BM, BROWNE F,
D’AMATO RJ: Effects of thalidomide and
related metabolites in a mouse corneal model
of neovascularization. Exp. Eye Res. (1997)
64:971-978.
GUNZLER V: Thalidomide in human
immunodeficiency virus (HIV) patients.
A review of safety considerations.
Drug Saf. (1992) 7:116-134.
Lt
ns
MCBRIDE W: Thalidomide and congenital
abnormalities. Lancet (1961) 2:1358.
12.
io
3.
7.
19.
d.
D’ARCY PF, GRIFFIN JP:
Thalidomide revisited. Adverse Drug React.
Toxicol. Rev. (1994) 13:65-76.
2.
FAIGLE J, KEBERLE H, RIESS W,
SCHMID K: The metabolic fate of
thalidomide. Experimentia (1962)
18:389-397.
d
11.
TEO SK, COLBURN WA, THOMAS SD:
Single-dose oral pharmacokinetics of three
formulations of thalidomide in healthy male
volunteers. J. Clin. Pharmacol. (1999)
39:1162-1168.
CHEN TL, VOGELSANG GB,
PETTY BG et al.: Plasma pharmacokinetics
and urinary excretion of thalidomide after
oral dosing in healthy male volunteers.
Drug Metab. Dispos. (1989)
17:402-405.
14.
BOUTIN F, BONNET F: Le thalidomide:
pharmacochimie et pharmacie clinique.
Lyon Pharm. (1995) 46:419-423.
15.
ERIKSSON T, BJORKMAN S,
HOGLUND P: Clinical pharmacology of
thalidomide. Eur. J. Clin. Pharmacol. (2001)
57:365-376.
Recent data and extensive review of
thalidomide's pharmacokinetics.
••
16.
TEO SK, SCHEFFLER MR, KOOK KA
et al.: Effect of a high-fat meal on
thalidomide pharmacokinetics and the
relative bioavailability of oral formulations
in healthy men and women.
Biopharm. Drug Dispos. (2000) 21:33-40.
Expert Opin. Drug Saf. (2004) 3(1)
NICHOLLS PJ: A note on the absorption
and excretion of 14C-labelled thalidomide in
pregnant mice. J. Pharm. Pharmacol. (1966)
18:46-48.
18.
an
g
tin
••
ZWINGENBERGER K, WNENDT S:
Immunomodulation by thalidomide:
systematic review of the literature and of
unpublished observations.
J. Inflamm. (1995) 46:177-211.
Excellent review discussing the
immunomodulatory properties
of thalidomide.
17.
Pr
in
1.
pr
tly
Acknowledgements
ric
Thalidomide is a powerful molecule that represents a significant
therapeutic option in various immunological disorders and
oncology. Its use requires assessing the risk–benefit ratio depending on the indication, as this ratio varies from country to country. The main side effects can be minimised by selecting suitable
patients (in particular, identifying thromboembolic and neuropathy risk factors) and carefully following published
st
opinion
io
n
9. Expert
recommendations [108]. Teratogenicity can be controlled
through effective contraceptive methods, as with other highly
teratogenic molecules frequently prescribed (e.g., isotretinoine in
acne). The use of thalidomide derivatives with fewer side effects
could be interesting but there is no data currently available relating to their potential neurotoxic effect. Given the unique nature
and complexity of the mechanisms of action of thalidomide,
which are not yet fully understood, new and unexpected indications could arise in the future, such as chronic heart failure or
bleeding angiodysplasias, as recently reported [109-111].
d
• Thalidomide: potential benefits and risks, open public scientific workshop, convened on 9th and 10th September,
1997, organised by the National Institutes of Health (NIH),
the FDA and the Centers for Disease Control and Prevention (CDC) (http://www.fda.gov/oashi/aids/thalexe.html).
53
Thalidomide: an old drug with new clinical applications
HASLETT PA, CORRAL LG, ALBERT M,
KAPLAN G: Thalidomide costimulates
primary human T lymphocytes,
preferentially inducing proliferation,
cytokine production and cytotoxic responses
in the CD8+ subset. J. Exp. Med. (1998)
187:1885-1892.
Pu
b
SHANNON EJ, EJIGU M,
HAILE-MARIAM HS, BERHAN TY,
TASESSE G: Thalidomide’s effectiveness in
erythema nodosum leprosum is associated
with a decrease in CD4+ cells in the
peripheral blood. Lepr. Rev. (1992) 63:5-11.
yr
ig
op
C
33.
54
CALDERON P, ANZILOTTI M,
PHELPS R: Thalidomide in dermatology.
New indications for an old drug.
Int. J. Dermatol. (1997) 36:881-887.
ric
st
io
n
••
47.
d
KLAUSNER JD, KAPLAN G,
HASLETT PA: Thalidomide in toxic
epidermal necrolysis. Lancet (1999) 353:324.
41.
D’AMATO RJ, LOUGHNAN MS,
FLYNN E, FOLKMAN J: Thalidomide is
an inhibitor of angiogenesis. Proc. Natl.
Acad. Sci. USA (1994) 91:4082-4085.
This article provides an insight into the
antiangiogenic properties of thalidomide.
42.
••
43.
STEPHENS TD, BUNDE CJ,
FILLMORE BJ: Mechanism of action in
thalidomide teratogenesis.
Biochem. Pharmacol. (2000) 59:1489-1499.
Comprehensive review of thalidomide's
teratogenicity and relationship
with angiogenesis.
KRUSE FE, JOUSSEN AM,
ROHRSCHNEIDER K, BECKER MD,
VOLCKER HE: Thalidomide inhibits
corneal angiogenesis induced by vascular
endothelial growth factor. Graefes Arch. Clin.
Exp. Ophthalmol. (1998) 236:461-466.
Expert Opin. Drug Saf. (2004) 3(1)
DRUCKER L, UZIEL O, TOHAMI T
et al.: Thalidomide downregulates transcript
levels of GC-rich promoter genes in multiple
myeloma. Mol. Pharmacol. (2003)
64:415-420.
48.
MINCHINTON AI, FRYER KH,
WENDT KR, CLOW KA, HAYES MM:
The effect of thalidomide on experimental
tumours and metastases. Anticancer Drugs
(1996) 7:339-343.
49.
JOSEPH IB, ISAACS JT:
Macrophage role in the antiprostate cancer
response to one class of antiangiogenic
agents. J. Natl. Cancer Inst. (1998)
90:1648-1653.
50.
WNENDT S, FINKAM M, WINTER W,
OSSIG J, RAABE G,
ZWINGENBERGER K:
Enantioselective inhibition of TNF-α release
by thalidomide and thalidomide-analogues.
Chirality (1996) 8:390-396.
51.
GORDON JN, GOGGIN PM:
Thalidomide and its derivatives:
emerging from the wilderness.
Postgrad. Med. J. (2003) 79:127-132.
An article focusing on
thalidomide analogues.
g
Pr
in
KEIFER JA, GUTTRIDGE DC,
ASHBURNER BP, BALDWIN AS Jr:
Inhibition of NF-κB activity by thalidomide
through suppression of IκB kinase activity.
J. Biol. Chem. (2001) 276:22382-22387.
40.
•
bi
te
oh
i
JACOBSON JM, GREENSPAN JS,
SPRITZLER J et al.: Thalidomide for the
treatment of oral aphthous ulcers in patients
with human immunodeficiency virus
infection. National Institute of Allergy and
Infectious Diseases AIDS Clinical Trials
Group. N. Engl. J. Med. (1997)
336:1487-1493.
tly
pr
38.
39.
d
KUMAR S, WITZIG TE,
RAJKUMAR SV: Thalidomide as an
anticancer agent. J. Cell Mol. Med. (2002)
6:160-174.
Good overview of the use of thalidomide in
clinical oncology.
ut
WOLKENSTEIN P, LATARJET J,
ROUJEAU JC et al.:
Randomised comparison of thalidomide
versus placebo in toxic epidermal necrolysis.
Lancet (1998) 352:1586-1589.
le
A
sh
of
MCHUGH SM, RIFKIN IR,
DEIGHTON J et al.:
The immunosuppressive drug thalidomide
induces T helper cell Type 2 (TH2) and
concomitantly inhibits TH1 cytokine
production in mitogen- and
antigen-stimulated human peripheral blood
mononuclear cell cultures.
Clin. Exp. Immunol. (1995) 99:160-167.
ht
32.
46.
di
s
37.
y
31.
BAUER KS, DIXON SC, FIGG WD:
Inhibition of angiogenesis by thalidomide
requires metabolic activation, which is
species-dependent. Biochem. Pharmacol.
(1998) 55:1827-1834.
tin
CHUONG PH, GALONS H, VOISIN J
et al.: In vitro and in vivo
immunosuppressive potential of thalidomide
and its derivative, N-hydroxythalidomide,
alone and in combination with
cyclosporin A. Int. J. Immunopharmacol.
(1997) 19:289-296.
lic
30.
45.
d.
29.
KEENAN RJ, EIRAS G, BURCKART GJ
et al.: Immunosuppressive properties of
thalidomide. Inhibition of in vitro
lymphocyte proliferation alone and in
combination with cyclosporin or FK506.
Transplantation (1991) 52:908-910.
ISHIKAWA M, KANNO S,
TAKAYANAGI M, TAKAYANAGI Y,
SASAKI K: Thalidomide promotes the
release of tumour necrosis factor-α (TNF-α)
and lethality by lipopolysaccharide in mice.
Biol. Pharm. Bull. (1998) 21:638-640.
ns
28.
36.
OR R, FEFERMAN R, SHOSHAN S:
Thalidomide reduces vascular density in
granulation tissue of subcutaneously
implanted polyvinyl alcohol sponges in
guinea-pigs. Exp. Hematol. (1998)
26:217-221.
io
•
MEIERHOFER C, WIEDERMANN CJ:
New insights into the pharmacological and
toxicological effects of thalidomide.
Curr. Opin. Drug Discov. Devel. (2003)
6:92-99.
An extensive review of the biological
activity of thalidomide.
KLAUSNER JD, FREEDMAN VH,
KAPLAN G: Thalidomide as an
antiTNF-α inhibitor: implications for
clinical use. Clin. Immunol. Immunopathol.
(1996) 81:219-223.
at
27.
35.
44.
ib
KANBAYASHI T, SHIMIZU T,
TAKAHASHI Y et al.:
Thalidomide increases both REM and
Stage 3 – 4 sleep in human adults:
a preliminary study. Sleep (1999)
22:113-115.
MOREIRA AL, SAMPAIO EP,
ZMUIDZINAS A, FRINDT P,
SMITH KA, KAPLAN G:
Thalidomide exerts its inhibitory action on
tumour necrosis factor α by enhancing
mRNA degradation. J. Exp. Med. (1993)
177:1675-1680.
tr
26.
34.
an
SCHEFFLER MR, COLBURN W,
KOOK KA, THOMAS SD:
Thalidomide does not alter
oestrogen–progesterone hormone single dose
pharmacokinetics. Clin. Pharmacol. Ther.
(1999) 65:483-490.
Lt
25.
•
52.
HIDESHIMA T, CHAUHAN D,
SHIMA Y et al.: Thalidomide and its
analogs overcome drug resistance of human
multiple myeloma cells to conventional
therapy. Blood (2000) 96:2943-2950.
53.
RICHARDSON PG, SCHLOSSMAN RL,
WELLER E et al.: Immunomodulatory drug
CC-5013 overcomes drug resistance and is
well-tolerated in patients with relapsed
multiple myeloma. Blood (2002)
100:3063-3067.
A recent paper on thalidomide's analogues
using human data.
•
Laffitte & Revuz
59.
DEANER PB: Thalidomide for distressing
night sweats in advanced malignant disease.
Palliat. Med. (1998) 12:208-209.
61.
FRATTA I, SIGG E, MAIORANA K:
Teratogenic effects of thalidomide in rabbits,
rats, hamsters and mice.
Toxicol. App. Pharmacol. (1965) 7:268-286.
at
io
HALES BF: Thalidomide on the comeback
trail. Nat. Med. (1999) 5:489-490.
LAGUENY A, ROMMEL A,
VIGNOLLY B et al.: Thalidomide
neuropathy: an electrophysiologic study.
Muscle Nerve (1986) 9:837-844.
76.
lic
y
67.
A
sh
CASTILLA EE, ASHTON-PROLLA P,
BARREDA-MEJIA E et al.:
Thalidomide, a current teratogen in
South America. Teratology (1996)
54:273-277.
MCBRIDE WG: Thalidomide may be a
mutagen. Br. Med. J. (1994) 308:1635-1636.
77.
78.
79.
d
bi
te
tly
pr
oh
i
75.
le
66.
PARMAN T, WILEY MJ, WELLS PG:
Free radical-mediated oxidative
DNA damage in the mechanism of
thalidomide teratogenicity.
Nat. Med. (1999) 5:582-585.
ric
HARLAND CC, STEVENTON GB,
MARSDEN JR: Thalidomide-induced
neuropathy and genetic differences in drug
metabolism. Eur. J. Clin. Pharmacol. (1995)
49:1-6.
ht
C
op
yr
ig
65.
io
n
st
74.
TEO SK, SABOURIN PJ, O’BRIEN K,
KOOK KA, THOMAS SD:
Metabolism of thalidomide in human
microsomes, cloned human cytochrome
P450 isozymes and Hansen’s disease
patients. J. Biochem. Mol. Toxicol. (2000)
14:140-147.
STEPHENS TD: Proposed mechanisms of
action in thalidomide embryopathy.
Teratology (1988) 38:229-239.
ut
CALABRESE L, FLEISCHER AB:
Thalidomide: current and potential clinical
applications. Am. J. Med. (2000) 108:487-495.
of
64.
OCHONISKY S, VERROUST J,
BASTUJI-GARIN S, GHERARDI R,
REVUZ J: Thalidomide neuropathy
incidence and clinico-electrophysiologic
findings in 42 patients. Arch. Dermatol.
(1994) 130:66-69.
The first prospective study of the
neurotoxicity of thalidomide.
•
73.
Pu
b
63.
ZHU X, ZHANG YP, KLOPMAN G,
ROSENKRANZ HS: Thalidomide and
metabolites: indications of the absence of
‘genotoxic’ carcinogenic potentials.
Mutat. Res. (1999) 425:153-167.
82.
83.
SINGHAL S, MEHTA J, DESIKAN R
et al.: Antitumour activity of thalidomide in
refractory multiple myeloma.
N. Engl. J. Med. (1999) 341:1565-1571.
84.
SINGHAL S, MEHTA J:
Thalidomide in cancer: potential uses and
limitations. BioDrugs (2001) 15:163-172.
85.
BASTUJI-GARIN S, OCHONISKY S,
BOUCHE P et al.: Incidence and risk
factors for thalidomide neuropathy:
a prospective study of 135 dermatologic
patients.J. Invest. Dermatol. (2002)
119:1020-1026.
86.
FULLERTON PM, O’SULLIVAN DJ:
Thalidomide neuropathy: a clinical
electrophysiological and histological
follow-up study. J. Neurol. Neurosurg.
Psychiatry (1968) 31:543-551.
87.
STRAUSS RS, DAS KM:
Thalidomide-induced sensory neuropathy.
J. Pediatr. Gastroenterol. Nutr. (2001)
32:322-324.
88.
BENNETT CL, SCHUMOCK GT,
DESAI AA et al.: Thalidomide-associated
deep vein thrombosis and pulmonary
embolism. Am. J. Med. (2002) 113:603-606.
Extensive review of the potential
thrombogenic effect of thalidomide in
multiple myeloma.
di
s
DEANER PB: The use of thalidomide in the
management of severe sweating in patients
with advanced malignancy: trial report.
Palliat. Med. (2000) 14:429-431.
60.
62.
72.
ASHBY J, TINWELL H,
CALLANDER RD et al.:
Thalidomide: lack of mutagenic activity
across phyla and genetic end points.
Mutat. Res. (1997) 396:45-64.
g
••
RIBAS C, COLLEONI GW:
Advances in the treatment of multiple
myeloma: the role of thalidomide.
Leuk. Lymphoma (2003) 44:291-298.
Recent data and extensive review of the use
of thalidomide in multiple myeloma.
KNOP J, BONSMANN G, HAPPLE R
et al.: Thalidomide in the treatment of sixty
cases of chronic discoid lupus
erythematosus. Br. J. Dermatol. (1983)
108:461-466.
Pr
in
58.
71.
81.
ib
OSSANDON A, CASSARA EA,
PRIORI R, VALESINI G:
Thalidomide: focus on its employment in
rheumatologic diseases.
Clin. Exp. Rheumatol. (2002) 20:709-718.
STROMLAND K, PHILIPSON E,
ANDERSSON GRONLUND M:
Offspring of male and female parents with
thalidomide embryopathy: birth defects and
functional anomalies. Teratology (2002)
66:115-121.
d
57.
70.
ARONSON IK, YU R, WEST DP,
VAN DEN BROEK H, ANTEL J:
Thalidomide-induced peripheral neuropathy.
Effect of serum factor on nerve cultures.
Arch. Dermatol. (1984) 120:1466-1470.
an
LAFFITTE E, REVUZ J:
Thalidomide. Ann. Dermatol. Venereol.
(2000) 127:603-613.
SMITHELLS D: Does thalidomide cause
second generation birth defects?
Drug. Saf. (1998) 19:339-341.
tin
56.
69.
80.
tr
WINES NY, COOPER AJ, WINES MP:
Thalidomide in dermatology.
Australas. J. Dermatol. (2002) 43:229-238.
SMITHELLS D: Dominant gene probably
caused some of defects ascribed to
thalidomide. Br. Med. J. (1998) 316:149.
d.
55.
68.
Lt
•
OKAFOR MC: Thalidomide for erythema
nodosum leprosum and other applications.
Pharmacotherapy (2003) 23:481-493.
Good review of thalidomide's
clinical applications.
ns
54.
GARDNER-MEDWIN JM, SMITH NJ,
POWELL RJ: Clinical experience with
thalidomide in the management of severe
oral and genital ulceration in conditions
such as Behcet’s disease: use of
neurophysiological studies to detect
thalidomide neuropathy. Ann. Rheum. Dis.
(1994) 53:828-832.
SHESKIN J, YAAR I: [Motor-conduction
velocity of cubital nerves in patients with
leprosy reactions. Summary of a 13-year
observation series during thalidomide
therapy]. Hautarzt (1979) 30:376-379.
German.
89.
WULFF CH, HOYER H,
ASBOE-HANSEN G, BRODTHAGEN H:
Development of polyneuropathy during
thalidomide therapy. Br. J. Dermatol. (1985)
112:475-480.
ESTEVE E, LEGAC E:
Deep vein thrombosis and pulmonary
embolism in a patient with aphthosis treated
with thalidomide. Ann. Dermatol. Venereol.
(2001) 128:148-149.
90.
FLAGEUL B, WALLACH D,
CAVELIER-BALLOY B, BACHELEZ H,
CARSUZAA F, DUBERTRET L:
Thalidomide and thrombosis. Ann. Dermatol.
Venereol. (2000)127:171-174.
CLEMMENSEN OJ, OLSEN PZ,
ANDERSEN KE:
Thalidomide neurotoxicity. Arch. Dermatol.
(1984) 120:338-341.
Expert Opin. Drug Saf. (2004) 3(1)
••
55
Thalidomide: an old drug with new clinical applications
103. HASLETT P, TRAMONTANA J,
TROJAN A, CHASSE E, GAY B,
PICHERT G, TAVERNA C:
Severe hepatic toxicity due to thalidomide in
relapsed multiple myeloma.
Ann. Oncol. (2003) 14:501-502.
tin
g
an
Pr
in
104. WILLIAMS I, WELLER IV, MALNI A,
d.
ANDERSON J, WATERS MF:
Thalidomide hypersensitivity in AIDS.
Lancet (1991) 337:436-437.
105. BIELSA I, TEIXIDO J, RIBERA M,
FERRANDIZ C: Erythroderma due to
thalidomide: report of two cases.
Dermatology (1994) 189:179-181.
106. RAJKUMAR SV, GERTZ MA,
op
yr
ig
ht
of
A
sh
le
y
Pu
b
WITZIG TE: Life-threatening toxic
C
56
Expert Opin. Drug Saf. (2004) 3(1)
d
bi
te
oh
i
pr
tly
d
BURROUGHS M, HEMPSTEAD M,
KAPLAN G: Adverse reactions to
thalidomide in patients infected with human
immunodeficiency virus. Clin. Infect. Dis.
(1997) 24:1223-1227.
BADROS AZ, SIEGEL E, BODENNER D
et al.: Hypothyroidism in patients with
multiple myeloma following treatment with
thalidomide. Am. J. Med. (2002) 112:412-413.
FRANCES C, EL KHOURY S,
GOMPEL A, BECHEREL PA,
CHOSIDOW O, PIETTE JC:
Transient secondary amenorrhea in women
treated by thalidomide. Eur. J. Dermatol.
(2002) 12:63-65.
ric
BOUWHUIS S, RAJKUMAR SV:
Dermatologic side effects of thalidomide in
patients with multiple myeloma.
J. Am. Acad. Dermatol. (2003) 48:548-552.
MORGAN AE, SMITH WK,
LEVENSON JL: Reversible dementia due to
thalidomide therapy for multiple myeloma.
N. Engl. J. Med. (2003) 48:1821-1822.
lic
98.
109. SHURAFA M, KAMBOJ G:
Thalidomide for the treatment of bleeding
angiodysplasias. Am. J. Gastroenterol. (2003)
98:221-222.
102. HALL VC, EL-AZHARY RA,
Lt
97.
Guideline for the clinical use and dispensing
of thalidomide. Postgrad. Med. J. (1994)
70:901-904.
ORTONNE JP: Thalidomide-induced
amenorrhoea: two cases. Br. J. Dermatol.
(2001) 144:1292-1293.
WANG J, WEISS I, SVOBODA K,
KWAAN HC: Thrombogenic role of cells
undergoing apoptosis. Br. J. Haematol.
(2001) 115:382-391.
ns
96.
108. POWELL RJ, GARDNER-MEDWIN JM:
101. PASSERON T, LACOUR JP, MURR D,
io
95.
•
MAURI M, DE TORRES I,
VILARDELL M: Thalidomide induces
amenorrhea in patients with lupus disease.
Arthritis Rheum. (1998) 41:2273-2275.
at
94.
100. ORDI J, CORTES F, MARTINEZ N,
st
POUAHA J, MARTIN S, TRECHOT P,
TRUCHETET F, BARBAUD A,
SCHMUTZ JL: Thalidomide and
thrombosis: three observations.
Presse Med. (2001) 30:1008-1009.
THOMAS SD, ELSAYED ME:
S.T.E.P.S.: a comprehensive programme for
controlling and monitoring access to
thalidomide. Clin. Ther. (1999) 21:319-330.
This article describes in detail the
STEPS programme.
io
n
93.
107. ZELDIS JB, WILLIAMS BA,
ut
PIETTE JC, SBAI A, FRANCES C:
Warning: thalidomide-related thrombotic
risk potentially concerns patients with lupus.
Lupus (2002) 11:67-70.
epidermal necrolysis with thalidomide
therapy for myeloma. N. Engl. J. Med.
(2000) 343:972-973.
ib
92.
GOMPEL A, FRANCES C, PIETTE JC,
BLANC AS, CORDOLIANI F,
PIETTE AM: Ovarian failure with
thalidomide treatment in complex aphthosis:
comment on the concise communication by
Ordi et al. Arthritis Rheum. (1999)
42:2259-2260.
99.
110. PEREZ-ENCINAS M,
tr
GACHON J, GROB JJ, RICHARD MA:
Thrombotic accidents induced by
thalidomide: two cases. Rev. Med. Interne.
(2002) 23:724-727.
di
s
91.
RABUNAL MARTINEZ MJ,
BELLO LOPEZ JL: Is thalidomide effective
for the treatment of gastrointestinal bleeding
in hereditary hemorrhagic telangiectasia?
Haematologica (2002) 87:ELT34.
111. GULLESTAD L, SEMB AG, HOLT E
et al.: Effect of thalidomide in patients with
chronic heart failure. Am. Heart J. (2002)
144:847-850.
Affiliation
Emmanuel Laffitte MD 1† & Jean Revuz MD2
†Author for correspondence
1Department of Dermatology, Centre Hospitalier
Universitaire Vaudois (CHUV), Lausanne,
Switzerland; and 2Université Paris XII,
Hôpital Henri Mondor (AP-HP), Créteil, France
Tel: +41 21 314 04 00; Fax: +41 21 314 03 92;
E-mail: [email protected]
Appendix 2
Laffitte E, Revuz J. Thalidomide. Ann Dermatol Venereol. 2007;134:957-60
77
78
Traitements lourds
Ann Dermatol Venereol
2007;134:957-60
Thalidomide
E. LAFFITTE (1), J. REVUZ (2)
L
e thalidomide est un médicament aux propriétés multiples, qui est utilisé essentiellement par les dermatologues du fait de son activité sur de nombreuses
pathologies inflammatoires cutanées, mais qui est peu à peu
redécouvert par d’autres spécialistes, en particulier les oncohématologues.
sorption cutanée est très basse et cette molécule n’est pas
adaptée à un usage topique. Le thalidomide augmente l’action
des barbituriques et de l’alcool, mais n’affecte pas le métabolisme des contraceptifs oraux.
Indications en dermatologie
Propriétés biologiques [1]
Le thalidomide possède différents modes d’action distincts et
dont le mécanisme n’est pas toujours élucidé.
– Action hypnosédative : l’effet est différent des barbituriques, peut-être par une activation directe des centres du sommeil.
– Action immunomodulatrice : le thalidomide module
l’équilibre entre les différentes classes de lymphocytes, mais
il diminue surtout la synthèse du TNF-α par les monocytes
humains stimulés en augmentant la dégradation de son
ARN messager.
– Action anti-angiogène : cette propriété est médiée par
l’inhibition de facteurs angiogènes dont le VEGF. Cette activité semble intéressante dans le traitement des néoplasies,
pour lesquelles l’angiogenèse joue un rôle important.
Pharmacologie [2]
L’absorption orale est rapide, avec un pic plasmatique à
4 heures et une élimination par voie urinaire avec une demivie d’élimination plasmatique de 9 heures. Le thalidomide est
retrouvé dans le sperme, avec une corrélation aux taux plasmatiques. Il n’existe pas de forme à usage parentéral, l’ab-
(1) Service de Dermatologie et Vénérologie, Centre Hospitalier
Universitaire Vaudois (CHUV), rue du Bugnon 46, CH-1011 Lausanne, Suisse.
(2) Service de Dermatologie, CHU Henri Mondor, Créteil.
Tirés à part : E. LAFFITTE, à l’adresse ci-dessus (1).
E-mail : [email protected]
Le Dr E. Laffitte qui a réalisé le chapitre « Thalidomide » pour le numéro spécial
sur les « Traitements lourds en dermatologie » déclare ce jour ne pas avoir de
conflit d’intérêts.
Le Pr J. Revuz qui a réalisé le chapitre « Thalidomide » pour le numéro spécial sur
les « Traitements lourds en dermatologie » déclare ce jour avoir des conflits
d’intérêts avec les laboratoires Laphal.
Le thalidomide est employé dans des pathologies cutanées
inflammatoires chroniques. Dans la majorité des cas, il n’a
qu’une action suspensive ; les lésions récidivent à l’arrêt. Le
thalidomide n’est pas contre-indiquée chez l’enfant où il est
utilisé pour des indications similaires à celles de l’adulte.
Indications clairement établies
– Érythème noueux lépreux ou réaction lépreuse de type 2 ;
– aphtoses et ulcérations muqueuses sévères isolées ou associées à la maladie de Behçet (inefficace sur l’atteinte systémique) ou l’infection par le VIH ;
– infiltrat lymphocytaire cutané de Jessner et Kanoff ;
– lupus érythémateux cutané (inefficace sur l’atteinte
systémique) ;
– GvH chronique à prédominance cutanée résistante aux
immunosuppresseurs.
Indications dermatologiques
potentiellement intéressantes
– Prurigos : nodulaire, actinique, du dialysé ;
– maladie de Kaposi ;
– érythème polymorphe chronique ou récidivant ;
– sarcoïdose cutanée ;
– pseudolymphomes.
Autres indications plus anecdotiques
– Histiocytose langerhansienne ;
– pyoderma gangrenosum ;
– pemphigoïde bulleuse et pemphigoïde cicatricielle ;
– pemphigus muqueux ;
– porphyrie cutanée tardive ;
– lichen plan, lichen érosif buccal ;
957
Ann Dermatol Venereol
2007;134:957-60
E. LAFFITTE, J. REVUZ
– maladie de Weber Christian ;
– syndrome de Melkersson-Rosenthal.
– thromboses veineuses profondes ; pour des doses supérieures à 100 mg/jour, et chez des patients présentant des
facteurs de risques thromboemboliques (syndrome des antiphospholipides, association avec des stéroïdes ou polychimiothérapie).
Contre-indications
Pas de contre-indication absolue à part une grossesse évolutive ou désir de conception. Contre-indication relative en cas de
neuropathie avérée (à part une neuropathie dans le cadre
d’un érythème noueux lépreux (ENL), cf. tableau I) ou de pathologie thromboembolique évolutive.
Effets secondaires mineurs
– Fréquents : somnolence, céphalées, douleurs abdominales,
constipation, impuissance ;
– rares : réactions cutanées ou perturbations endocriniennes (aménorrhée, hypothyroïdie).
Surdosage
Effets secondaires (tableau II)
Certains effets secondaires du thalidomide sont majeurs, avec
des conséquences graves, d’autres sont mineurs, apparaissant
au début et disparaissant après diminution des doses.
Effets secondaires majeurs
La toxicité aiguë du thalidomide est très faible. Des surdosages accidentels ou volontaires n’ont eu aucune conséquence
grave, même pour des doses de 14 g.
Prescription et surveillance
– Effet tératogène, pouvant théoriquement s’exprimer également chez la partenaire de l’homme traité, le thalidomide
étant excrété dans le sperme ; il n’y a pas d’effet mutagène.
À noter que l’isotrétinoïne, prescrite de pratique courante
dans l’acné chez des patientes en âge de procréer, est aussi
tératogène que le thalidomide (risque de malformation fœtale
de 25 à 30 p. 100 après une prise) ;
– neuropathie axonale, sensitive bilatérale et symétrique à
début distal. Le risque semble maximal la première année de
traitement, pour des doses supérieures à 25 mg/jour ;
La seule forme existante est la forme orale, sous forme de gélules dosées à 50 mg et 100 mg, distribuées en Europe par les
laboratoires Pharmion.
Modalités d’obtention
En France, le thalidomide ne peut être obtenue que par le
biais d’un programme extrêmement strict de contrôle des
prescriptions ayant pour but de prévenir toute grossesse sous
Tableau I. – Indications clairement établies du thalidomide : posologies recommandées dans les indications dermatologiques
habituelles.
Indication
Érythème noueux lépreux (ENL)
Dose d’attaque
100-400 mg/j en 2 prises
jusqu’à sédation des signes,
7 jours en moyenne
Dose d’entretien
diminution progressive
jusqu’à 50 mg 2 fois
par semaine
Aphtoses et ulcérations
muqueuses sévères
(dont VIH et Behçet)
Lupus cutané
100-200 mg/j pendant 1 mois
diminution progressive
jusqu’à 50 mg 2 fois
par semaine
50 mg/j à 50 mg 2 fois
par semaine
Infiltrat lymphocytaire cutané
de Jessner-Kanoff
100-200 mg/j pendant 1 mois
Réaction du greffon contre
l’hôte (GvH) après greffe
de moelle allogénique
958
100-200 mg/j pendant 1 mois
600-800 mg/j chez l’adulte
12 mg/kg/j chez l’enfant
50 mg/j à 50 mg 2 fois
par semaine
Remarques
Pas de contre-indication en cas de neuropathie
lépreuse dans le cadre d’un ENL :
le thalidomide traite le processus inflammatoire
périnerveux et améliore les symptômes
neurologiques
Après échec de la colchicine
Pas d’action sur les manifestations systémiques
dans la maladie de Behçet
En deuxième intention si contre-indication
ou inefficacité de 3 mois d’antipaludéens
de synthèse
Pas d’action sur les manifestations
systémiques du lupus
Efficacité purement suspensive,
une récidive survenant 2 à 3 semaines
après l’arrêt du traitement
Dans les formes chroniques à prédominance
cutanée résistantes aux traitements
immunosuppresseurs. Pas d’effet dans la prévention
de la GvH chronique ou dans la GvH aiguë
Ann Dermatol Venereol
2007;134:957-60
Thalidomide
Tableau II. – Effets secondaires du thalidomide [2, 3].
FRÉQUENTS
Majeurs
Tératogénicité
Neuropathie périphérique
Thromboses veineuses profondes
Mineurs (mais peuvent être limitant à haute dose)
Somnolence
Constipation, prise de poids, douleurs abdominales
MOINS FRÉQUENTS
Cutanés
Éruption cutanée maculopapuleuse
Érythème polymorphe, syndrome de Lyell, érythrodermie,
érythème noueux
Vasculite
Fragilité unguéale
Sécheresse buccale
Prurit
Érythème palmoplantaire
Endocriniens
Hypothyroïdie
Aménorrhée
Galactorrhée
Saignements génitaux
Hypoglycémie/hyperglycémie
Hématologiques
Leucopénie
Neuropsychiques
Maux de tête
Tremblements intermittents
Démence réversible
Dépression
Perte de libido
Gastro-intestinaux
Distension abdominale
Augmentation de l’appétit
Nausées
Hépatite
Système cardiovasculaire
Bradycardie, tachycardie
Hypertension, hypotension
thalidomide. Il n’y a pas d’autorisation de mise sur le
marché ; la délivrance du médicament est faite par une pharmacie hospitalière sur une base mensuelle après prescription
d’un médecin hospitalier, selon deux types d’autorisations
temporaires d’utilisation (ATU) :
– ATU de cohorte pour 6 indications : ENL, aphtoses sévères et maladie de Behçet, maladie de Jessner-Kanoff, lupus
érythémateux cutané ayant résisté aux traitements classiques, GvH chronique, myélome réfractaire et/ou en rechute
après au moins une ligne thérapeutique ayant comporté des
alkylants. Les patients sont suivis en cohorte et non nommément désignés.
– ATU nominative : pour toute autre indication, les malades sont nommément désignés et un accord préalable de
l’Agence Française de Sécurité Sanitaire des Produits de Santé (AFSSAPS, service des ATU) doit être obtenu.
Conduite du traitement et surveillance
– Posologies : cf. tableau I ;
– conduite pratique et surveillance : cf. « Fiche pratique »
en fin d’article.
Thalidomide sur Internet
Plusieurs sites traitant du thalidomide sont actuellement consultables sur Internet :
– The Thalidomide Victims Association of Canada. Site de
l’association canadienne des victimes du thalidomide. Cette
organisation représente environ 125 victimes canadiennes
du thalidomide, et propose différentes informations concernant le thalidomide, des questions d’actualité concernant le
grand public. Adresse URL : http://www.thalidomide.ca.
– US Food and Drug Administration/Center for Drug Evaluation and Research. Site de la FDA, rubrique thalidomide.
Ce site propose différentes informations sur le thalidomide,
les indications et le mode de prescription aux Etats-Unis.
Adresse URL : http://www.fda.gov/cder/news/thalinfo.
Conclusion
Le thalidomide est une molécule puissante qui représente
une option thérapeutique très utile dans de nombreuses pathologies dermatologiques difficiles à traiter. Les principaux
effets secondaires peuvent être minimisés avec une bonne sélection des patients, en particulier en identifiant les facteurs
de risques de neuropathie et d’accidents thromboemboliques.
Les médecins prescripteurs ne doivent donc pas être effrayés
par le thalidomide, qui reste une molécule utile pour de nombreuses pathologies, sous réserve d’une surveillance rigoureuse.
Références
1. Zwingenberger K, Wnendt S. Immunomodulation by thalidomide: systematic review of the literature and of unpublished observations. J Inflamm 1995;46:177-211.
2. Laffitte E, Revuz J. Thalidomide: an old drug with new clinical applications. Expert Opin Drug Saf 2004;3:47-56.
3. Tseng S, Pak G, Washenik K, Pomeranz MK, Shupack JL. Rediscovering
thalidomide: a review of its mechanism of action, side effects, and potential uses. J Am Acad Dermatol 1996;35:969-79.
959
Ann Dermatol Venereol
2007;134:957-60
E. LAFFITTE, J. REVUZ
FICHE PRATIQUE – THALIDOMIDE
Avant le traitement
Pendant le traitement
Formalités administratives
Administration
Avec la pharmacie hospitalière : déclaration en ATU de cohorte ou nominative en fonction de l’indication
Avec l’Agence Française de Sécurité Sanitaire des Produits de
Santé (AFSSAPS, service des ATU) : un accord préalable
doit être obtenu en cas d’ATU nominative
Avec le patient : information concernant les risques tératogènes et signature d’un accord de soins et de contraception
Prise recommandées le soir (somnolence)
Ordonnance mensuelle de renouvellement
Bilan pré-thérapeutique
Examen neurologique et EMG
TSH
Chez la femme en âge de procréer : dosage de βHCG qui
doit être négatif 3 jours avant le début de la prescription
Mise en place d’une contraception par 2 méthodes efficaces (femme), port du préservatif (homme)
960
Surveillance
Mensuelle : examen neurologique, dosage de βHCG chez
la femme en âge de procréer
Semestrielle : EMG
Contre-indication : grossesse, dons de sang et de sperme
Après le traitement
Grossesse possible
– Chez la femme : dès le premier cycle suivant l’arrêt du
traitement
– Chez l’homme : attendre 3 mois après arrêt du traitement (correspondant à un cycle de spermatogenèse)
Appendix 3
Laffitte E. Thalidomide in Kaposi sarcoma: promising or disappointing?
Dermatology. 2007;215:171-2
83
84
Editorial
Dermatology 2007;215:171–172
DOI: 10.1159/000106571
Thalidomide in Kaposi Sarcoma:
Promising or Disappointing?
Emmanuel Laffitte
Department of Dermatology and Venerology, Centre Hospitalier Universitaire Vaudois (CHUV),
Lausanne, Switzerland
Thalidomide, well known by dermatologists for its
anti-tumor necrosis factor- activity, is used for several
inflammatory cutaneous disorders. Anti-angiogenic
properties of thalidomide, mediated by inhibition of angiogenic factors such as vascular endothelial growth factor and basic fibroblast growth factor, were first shown in
1994 on a rabbit cornea model [1]. Since the mid 1990’s,
the discovery of this anti-angiogenic effect has led to renewed interest for this drug, especially in oncology [2].
Thalidomide has been shown to be an active and promising anti-carcinogenic drug, as a single agent or in combination with dexamethasone in hematological malignancy, such as relapsing or refractory multiple myeloma, myelodysplasia or acute myeloid leukemia [3]. Since Kaposi
sarcoma (KS) is an angiogenic neoplasm, it has been logically hypothesized that thalidomide might be of interest
in KS.
Thalidomide was first studied in HIV-associated KS.
In four publications that involved a total of 50 patients
[4–7], well reviewed and analyzed by Krown [8], 17 patients (34%) showed objective KS regression. Dosages
ranged from 100 to 1,000 mg/day during 8 weeks to 12
months; no complete response was observed, and HHV-8
viral load was reduced only in 3 responding cases. Eleven
patients (22%) withdrew because of toxicity.
In this issue of Dermatology, the effect of thalidomide
is assessed for non-HIV KS (iatrogenic or classic) in two
© 2007 S. Karger AG, Basel
1018–8665/07/2153–0171$23.50/0
Fax +41 61 306 12 34
E-Mail [email protected]
www.karger.com
Accessible online at:
www.karger.com/drm
retrospective studies [9, 10]. In the first study, Rubegni et
al. [9] treated 3 patients with 100 mg/day of thalidomide
for 1 year and observed a complete response in 2 patients
(including an immunosuppressed patient with systemic
KS) and a partial response in the third. In the two responding cases, they observed a negativation of the HHV8 viral load in the skin and the blood. In the second study
[10], 11 patients were treated with a median dose of 100
mg/day for a median time of 3 months. The results are
less impressive, with only 3 patients (27%) achieving a
partial response. Out of these 14 patients, 4 (28%) discontinued thalidomide for side-effects. The overall response
rate appears thus to be quite similar in KS, whether HIV
associated or not, and lower than the response rates obtained with other systemic therapies such as interferon,
pegylated liposomal doxorubicin [10] or even radiotherapy in localized cases [11].
Taken together, these results suggest that thalidomide
is not a major therapy for KS, with a disappointing response rate and limitations due to side-effects, although
it could be useful in some specific cases as shown by Rubegni et al. [9]. However, an anti-angiogenic approach
may still be interesting in KS, as suggested by Ben M’barek
et al. [10]. With the ‘rediscovery’ of thalidomide, several
structural analogues have been developed in an attempt
to find compounds with thalidomide’s properties without the associated side-effects. In particular, lenalidoEmmanuel Laffitte, MD
Department of Dermatology and Venerology
Centre Hospitalier Universitaire Vaudois (CHUV)
CH–1011 Lausanne (Switzerland)
Tel. +41 21 314 0406, Fax +41 21 314 0392, E-Mail [email protected]
mide (Revlimid), a second-generation thalidomide derivative, has been extensively studied in patients with myelodysplastic syndromes. Lenalidomide was identified as
more potent than thalidomide and devoid of many of the
serious adverse reactions associated with thalidomide
administration, such as neuropathy [12]. Moreover, it has
been recently shown that oral administration of lenalidomide inhibits angiogenesis in rat in vivo models [13].
Thus, lenalidomide could be the next promising step for
an oral anti-angiogenic therapy in KS.
References
1 D’Amato RJ, Loughnan MS, Flynn E, Folkman J: Thalidomide is an inhibitor of angiogenesis. Proc Natl Acad Sci USA 1994; 91:
4082–4085.
2 Laffitte E, Revuz J: Thalidomide: an old drug
with new clinical applications. Expert Opin
Drug Saf 2004;3:47–56.
3 Morgan GJ, Krishnan B, Jenner M, Davies
FE: Advances in oral therapy for multiple
myeloma. Lancet Oncol 2006;7:316–325.
4 Politi PM: Thalidomide. Clinical trials in
cancer (Spanish). Medicina (B Aires) 2000;
60(suppl 2):61–65.
5 Little RF, Wyvill KM, Pluda JM, Welles L,
Marshall V, Figg WD, Newcomb FM, Tosato
G, Feigal E, Steinberg SM, Whitby D, Goedert JJ, Yarchoan R: Activity of thalidomide in
AIDS-related Kaposi’s sarcoma. J Clin Oncol
2000;18:2593–2602.
172
6 Fife K, Howard MR, Gracie F, Phillips RH,
Bower M: Activity of thalidomide in AIDSrelated Kaposi’s sarcoma and correlation
with HHV8 titre. Int J STD AIDS 1998; 9:
751–755.
7 Soler RA, Howard M, Brink NS, Gibb D, Tedder RS, Nadal D: Regression of AIDS-related
Kaposi’s sarcoma during therapy with thalidomide. Clin Infect Dis 1996; 23: 501–503;
discussion 504–505.
8 Krown SE: Management of Kaposi sarcoma:
the role of interferon and thalidomide. Curr
Opin Oncol 2001;13:374–381.
9 Rubegni P, Sbano P, De Aloe G, Flori ML,
Fimiani M: Thalidomide in the treatment of
Kaposi’s sarcoma. Dermatology 2007;215:
240–244.
Dermatology 2007;215:171–172
10 Ben M’barek L, Fardet L, Mebazaa A, Thervet E, Biet I, Kérob D, Morel P, Lebbe C: A
retrospective analysis of thalidomide therapy in non-HIV-related Kaposi’s sarcoma.
Dermatology 2007; 215:202–205.
11 Kigula-Mugambe JB, Kavuma A: Epidemic
and endemic Kaposi’s sarcoma: a comparison of outcomes and survival after radiotherapy. Radiother Oncol 2005;76:59–62.
12 Kumar S, Rajkumar SV: Thalidomide and lenalidomide in the treatment of multiple myeloma. Eur J Cancer 2006;42:1612–1622.
13 Dredge K, Horsfall R, Robinson SP, Zhang
LH, Lu L, Tang Y, et al: Orally administered
lenalidomide (CC-5013) is anti-angiogenic
in vivo and inhibits endothelial cell migration and Akt phosphorylation in vitro. Microvasc Res 2005;69:56–63.
Laffitte
Appendix 4
Laffitte E. Thalidomide, semen distribution, teratogenicity...and cost. Br J
Dermatol. 2006;154:563; author reply 563-4.
87
88
Correspondence 563
8 McMenamin ME, Fletcher CD. Reactive angioendotheliomatosis. a
study of 15 cases demonstrating a wide clinicopathologic spectrum. Am J Surg Pathol 2002; 26:685–97.
9 Lazova R, Slater C, Scott G. Reactive angioendotheliomatosis. Case
report and review of the literature. Am J Dermatopathol 1996; 18:63–9.
10 Asagoe K, Fujimoto W, Yoshino T et al. Intravascular lymphomatosis of the skin as a manifestation of recurrent B-cell lymphoma.
J Am Acad Dermatol 2003; 48:S1–4.
Conflicts of interest: none declared.
Thalidomide, semen distribution,
teratogenicity… and cost
DOI: 10.1111/j.1365-2133.2005.07083.x
SIR, I read with interest the recent article on thalidomide in
this journal by Wu et al.1 with the detailed recommendations
to prevent thalidomide embryopathy. However, I have two
remarks.
First, the authors do not mention that there is a potential risk
of a teratogenic effect of thalidomide with treated male patients,
as the molecule is distributed into semen. In rabbits, the molecule is not only present in the seminal fluid, but is also firmly
fixed on spermatozoa.2 In humans, after an oral intake of
100 mg daily, thalidomide is detected in semen at week 4 with
a correlation between plasma and semen levels.3 Congenital
malformations have been observed in newborn rabbits resulting
from breeding experiments with males having a prolonged
intake of thalidomide.2 Such an effect has not yet been described
in humans, but there could be a potential risk of fetal exposure
to thalidomide in pregnant women through transmission by
semen of treated male patients.4 As a consequence, men treated
with thalidomide should avoid sperm donation, and use condoms during the therapy and for 3 months after its cessation
(corresponding to a spermatogenesis cycle).
Secondly, one should notice that some other highly teratogenic molecules are frequently prescribed by dermatologists,
such as isotretinoin. It has been demonstrated that approximately 25–30% of fetuses exposed to isotretinoin have birth
defects,5 which makes isotretinoin as embryotoxic as thalidomide. There are some specific birth control programmes associated with isotretinoin use, such as the SMART (System to
Manage Accutane-Related Teratogenicity) programme in the
U.S.A.,6 which are not as comprehensive or expensive as the
STEPS (System for Thalidomide Education and Prescribing
Safety) programme. However, the Food and Drug Administration has recently approved a strengthened risk management
programme for isotretinoin called iPLEDGE, use of which will
become mandatory in the U.S.A. on 31 December 2005.7
Thus, dermatologists should not be afraid of thalidomide,
as teratogenicity is currently well controlled in Western countries through managed effective contraceptive methods and
repeated pregnancy tests. This is not true everywhere in the
world, and at least 34 cases of embryopathy after exposure to
thalidomide have been reported in South American leprosy
endemic areas since 1965.8
The main factors limiting the use of thalidomide are currently its neurotoxicity, and the weightiness of the STEPS programme (and its equivalent in Europe, the Pharmion Risk
Management Programme, PRMP) which is time consuming
and requires laborious inputs from prescriber, patient and
pharmacist. Another limiting factor is the price of the drug,
which has increased 400% since the sponsorship was transferred to Pharmion Development in Europe, with the introduction of the PRMP. Health insurances often do not pay for
this orphan drug, and therefore patients may have to bear
much of the cost themselves. This fact should also have been
discussed by Wu et al.
Department of Dermatology,
Centre Hospitalier Universitaire Vaudois,
CH-1011 Lausanne, Switzerland
E.LAFFITTE
E-mail: [email protected]
References
1 Wu JJ, Huang DB, Pang KR et al. Thalidomide: dermatological indications, mechanisms of action and side-effects. Br J Dermatol 2005;
153:254–73.
2 Lutwak-Mann C, Schmid K, Keberle H. Thalidomide in rabbit
semen. Nature 1967; 214:1018–20.
3 Teo SK, Harden JL, Burke AB et al. Thalidomide is distributed into
human semen after oral dosing. Drug Metab Dispos 2001; 29:1355–7.
4 Laffitte E, Revuz J. Thalidomide: an old drug with new clinical
applications. Expert Opin Drug Saf 2004; 3:47–56.
5 Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy.
N Engl J Med 1985; 313:837–41.
6 Brinker A, Kornegay C, Nourjah P. Trends in adherence to a revised
risk management program designed to decrease or eliminate isotretinoin-exposed pregnancies: evaluation of the Accutane SMART program. Arch Dermatol 2005; 141:563–9.
7 http://www.fda.gov/cder/drug/advisory/isotretinoin2005.htm
8 Castilla EE, Ashton-Prolla P, Barreda-Mejia E et al. Thalidomide, a
current teratogen in South America. Teratology 1996; 54:273–7.
Conflicts of interest: none declared.
Thalidomide, semen distribution, teratogenicity… and cost: reply from authors
DOI: 10.1111/j.1365-2133.2005.07084.x
SIR, Unfortunately, due to space limitations we could not
address all possible issues concerning thalidomide use.1 However, we agree about the two concerns of the potential risk of
thalidomide in male patients and of cost. It was demonstrated
that thalidomide causes loss of elongating and round spermatids
2005 British Association of Dermatologists • British Journal of Dermatology 2006 154, pp551–577
90
Appendix 5
Navarini A, Laffitte E, Conrad C, Piffaretti P, Brock E, Ruckdaeschel S, Trüeb
R. Cost-of-illness in patients with psoriasis in Switzerland. Swiss Med Wkly.
2009. in press
91
92
Introduction
Estimation of cost-of-illness in patients with psoriasis in
Switzerland
Psoriasis is a chronic inflammatory skin disease with a substantial economic burden [1-9]. It is highly
prevalent, affecting about 2% of the adult Western population. The chronic, very noticeable and
Alexander A. Navarinia, Emanuel Laffitteb, Curdin Conrada, Paolo Piffarettic, Elisabeth
symptomatic skin lesions frequently result in work day loss. Discomfort, time and energy invested in
Brockd, Stephan Ruckdaescheld and Ralph M. Trüeba,*
treatment and the stigmatization associated with the disease have significant adverse impact on
quality-of-life. Due to lack of a definite cure, continuous care is often required.
aDepartment of Dermatology, University of Zurich, Zurich, Switzerland
Tel. +41 44 255 11 11, Fax. +41 44 255 45 49
As psoriasis is not a life-threatening disease, the medical and socioeconomic burden are often
email : [email protected]
underestimated by health care professionals. However, for several Western countries, it has been
bService de Dermatologie, Hôpitaux Universitaires de Genève
shown that psoriasis represents a financial burden both for the affected individual and for the health
care system [1-9]. According to reports from Germany [7-9], cost estimates range from about € 160
cWyeth Pharmaceuticals AG, Zug, Switzerland
million [10] for inpatient treatment per year to annual severity-related costs of € 2’866 per patient per
dHealthEcon AG, Basel, Switzerland
year for moderate psoriasis to € 4’985 for severe psoriasis in one study [7], and mean total costs of €
* corresponding author
6’709 per patient per year in the other study [8]. In contrast, little is known about the economic impact
Running head: The direct cost of Psoriasis in Switzerland
and ambulatory care costs. However, both of these expenditures play an important budgetary role for
of psoriasis in Switzerland, specifically, there is a lack of knowledge regarding out-of pocket expenses
psoriasis patients and their families. Thus, the present study was initiated in order to estimate the
Key Words: Moderate-to-severe psoriasis – Quality of life – Cost-of-illness - Switzerland
impact of psoriasis in terms of resources used, associated costs, and quality of life impairment,
specifically for Switzerland. This is intended to convey a picture of the burden of the disease, which
Word count: Abstract: 231 words, Manuscript: 3584 words, 23640 chrs (with spaces).
can be used in evaluations of the cost-effectiveness of specific therapies, i.e. new therapeutic agents
for effective psoriasis control.
Abstract:
Background: Evaluation of the current clinical treatment of psoriasis in Switzerland remains to be
Design and Methods
measured with the parameters cost-of-illness and quality of life.
Hypothesis
Objective: To obtain data on out-of-pocket expenses, costs of outpatient/office-based care and
inpatient care for psoriasis, and to extrapolate total costs by state of severity in the entire Swiss
1. Patients with plaque-type psoriasis in Swiss dermatological practices and outpatient clinics as well
population.
Methods: 1’200 retrospective surveys were distributed to patient members of the Swiss Psoriasis and
Vitiligo Society, and 400 surveys to office-/hospital-based Swiss dermatologists. The reference year
for data collection was 2005. Patients were stratified into three subgroups according to severity of
disease. Costs of inpatient care was measured by the amount of hospital days of psoriatic patients
as patient members of the Swiss Psoriasis and Vitiligo Association show a substantial and
disease-activity dependent burden of illness.
2. Direct costs of the disease rise disproportionately with disease activity.
Design of the study
from the Swiss Federal Hospital Statistics.
Results: 383 patient questionnaires, and 170 cases documented by 57 dermatologists were analyzed.
The study is a retrospective cost-of-illness analysis in relation to severity of disease. It is based on
Out-of-pocket expenses/costs for ambulatory care per patient and year ranged from CHF 600-1’100
data collected through a patient survey to evaluate the impact of disease on health-related quality of
for mild psoriasis to CHF 2’400-9’900 for severe psoriasis. Including costs for inpatient care of approx.
Life (HRQoL) and patients’ out-of-pocket expenses, a physicians’ survey to estimate ambulatory care
CHF 60 million, the total annual costs for psoriasis in Switzerland in 2004/5 amounted to
costs, and inpatient data obtained from the Federal Statistical Office (FSO) regarding the number of
approximately CHF 314-458 million.
cases treated for psoriasis in the hospital and average length of hospital stay. Patients covered by the
Conclusions: Moderate-to-severe psoriasis is associated with significant impact on quality of life and
two surveys were not identical. The reference year for data collection for outpatients was 2005, for
at least 4-fold higher costs than mild psoriasis, indicating need for efficient control of the disease. This
inpatients 2004.
cost-of-illness study provides specific health economic data for further healthcare decision making,
particularly with the advent of new therapeutic agents for effective psoriasis control.
1/13
2/13
Aim of the study
The burden of disease for the individual patient in terms of health-related quality of life and the
The objective of the study was to obtain data on out-of-pocket expenses, costs of outpatient/office-
Collected data were assessed for plausibility and completeness by two experienced representatives of
based care and inpatient care for psoriasis, and to extrapolate total costs by state of severity in the
HealthEcon. Incompletely filled questionnaires were conservatively completed if necessary by applying
entire Swiss population.
information from patients that provided valid reports for the respective category or item of resource
disease’s impact on daily activities was measured with the Dermatology Life Quality Index (DLQI) [11].
use. Where no plausible data regarding i.e. treatment costs could be identified based on other patients
Patients
in the same survey, data was substituted based on official publications such as the Drug Reference
A questionnaire package accompanied by cover letters and prepaid return envelopes addressed to
HealthEcon Ltd, Basel were distributed by the Swiss Psoriasis and Vitiligo Society (SPVG), the Swiss
patient association, to its 1’200 members in November 2005. SPVG added a cover letter encouraging
Manual of Switzerland (“Arzneimittel-Kompendium der Schweiz”) or other sources. Missing data was
supplemented in such a way as to underestimate costs, rather than overestimating them.
Data Collection – Physicians
members to participate in the study. Questionnaires and cover letters were provided in German and in
French.
Similar to the patient survey, data on resource use in ambulatory care were collected using a “bottomup” approach based on a specifically developed semi-structured, self-reported questionnaire for
Physicians were issued with questionnaires for patient documentation, a cover letter and a return
prepaid envelope addressed to HealthEcon Ltd. This Switzerland-wide survey addressed only
dermatologists. Questionnaire and cover letter were again provided in German and in French
physicians. The physician questionnaire requested information on demographics, assessment of
disease severity (using the Psoriasis Area Severity Index (PASI) if available), co-morbidities, drugs,
medical services and rehabilitation.
language. A total of 400 dermatologists were contacted, representing office-based physicians as well
as physicians providing ambulatory care in hospitals.
The information concerning resource consumption was retrospectively extracted from the patient’s
records. The documentation of drug treatment was structured according to different drug classes.
Inclusion Criteria
Based on prescription information the overall costs of drugs were calculated by multiplying the
Patients aged 18 years or more with psoriasis independent of severity were included in the study.
Patients were enrolled by physicians if they had been treated by the participating dermatologist for at
least 12 months before enrollment. Physicians were asked to document the last three psoriasis
prescriptions with the corresponding prices. Regarding medical services, the participating
dermatologists were asked to document the frequency of diagnostic and therapeutic procedures
performed for the given patient, including a wide range of services from basic consultation to, e.g.
phototherapy. Given this structural framework, the questionnaire demanded the documentation of the
patients appearing in their office for psoriasis.
medical and technical services provided, the number of applications, the respective Tarmed (individual
Inpatient data were obtained from the FSO regarding the number of patients with relevant ICD-10
outpatient service tariff) position and/or tax points. The costs of this service charged to the Swiss
codes (L40.0-40.9). FSO supplied the number of cases treated in hospital with a primary or secondary
obligatory health insurance were calculated by multiplying frequency, tax points and tax point value.
diagnosis of psoriasis and length of hospital stay.
Missing data were, if necessary, conservatively supplemented in such a way as to underestimate
costs, rather than overestimating them.
Outpatients were stratified into three subgroups according to affected body surface area (BSA): mild: <
2% BSA; moderate: 2 – 10% BSA; severe: > 10% BSA.
Data Collection – FSO, SVK
Data Collection – Patients
Extracting costs for inpatient care differs from the data obtained through the patient and physician
survey in that it used a “top-down” approach instead of the “bottom-up” calculation used to estimate
The patient survey was performed with a semi-structured, patient-administered questionnaire to collect
costs for ambulatory care and out-of-pocket expenses. The information supplied by the FSO regarding
individual patients’ data using a “bottom-up” methodology. The questionnaire asked for patients’
the number of cases treated in the hospital for psoriasis and the average length of stay (LOS) was
demographic data, duration and severity of disease including affected body areas, patients’ out-of-
translated into number of patients by using the rate “cases per patient” also supplied by the FSO.
pocket expenses for drugs, skin care products and services, privately paid hospital and inpatient
Average LOS per patient in 2004 was calculated on the number of cases per ICS-10 subgroup, the
treatments, as well as psoriasis-related absence from work. Patients were asked to measure the area
average length of stay per case, and the number of cases per patient. As all patients hospitalized with
of their plaques in amounts of their own palmar surface, a reliable method frequently used in clinical
the respective diagnosis are included, the data provides a total sum of costs for inpatient care caused
practice.
by patients hospitalized due to psoriasis. Costs of inpatient care calculated that way are the total costs
3/13
4/13
incurring for Switzerland that year. Along common Swiss medical practice, as a rule only severe
383 documented records of patients’ out-of-pocket expenses were returned (32%, comparable to other
psoriasis cases require hospital treatment. The costs for inpatient care as derived from FSO data were
questionnaire-based studies [13]) and analyzed. The majority of patients were between 30 and 65
therefore completely assigned to patients with severe psoriasis when extrapolating the costs of
years old, with the mean at 55 years. 226 (59%) of the 383 patients were male. In 50% of patients,
psoriasis for Switzerland. In 2005, 229 patients received biologic treatment for severe psoriasis. The
psoriasis had been diagnosed between 55 and 25 years ago and in 41% between 5 and 25 years ago.
respective costs were obtained from the “Schweizerischer Krankenkassen Verband” (SVK, Swiss
In 60% of cases, the diagnosis had been posed by a dermatologist.
Medical Insurance Association).
Using the body surface area affected as a measure for severity, 38% reported mild disease (BSA <
Costs
2%), 43% moderate disease (BSA 2-10%) and 19% severe disease (BSA > 10%). On average,
patients reported more than seven affected body areas. The relative proportion of body areas affected
Patients estimated their resource use regarding OTC medication, skin care products, as well as non-
is shown in Table 1.
reimbursed treatments. The overall costs estimate for each of the surveyed patients was calculated by
multiplying the amount of units of psoriasis-related physical resources consumed by each patient with
Overall 65% of patients had been using drugs against psoriasis one month prior to filling out the
the costs per unit given by the patient or – depending on the patient’s reporting – by adding up the
questionnaire. 8% reported having been free of symptoms during the previous week. Out-of-pocket
total amount of expenses the patient reported to have spent for products or services in 2005. This
expenses relating to the category of severity are shown in Table 2. We found a considerable increase
calculation was performed differentiating for disease severity (mild, moderate, severe) and resulted in
in total average out-of-pocket expenses depending on the severity of disease from CHF 630 per
patient and year in mild psoriasis to CHF 2’400 in severe psoriasis. 30% of patients reported a large or
total costs for patients in the respective category of severity.
very large effect of their psoriasis on quality of life, two thirds indicated a small or moderate influence,
To evaluate ambulatory treatment costs as reported by physicians, the average frequency of
and only 8% reported no effect. The greater the affected skin area, the higher the impact on the quality
diagnostic or treatment services was multiplied with the corresponding cost for this service. Charges
of life (Figure 1).
for outpatient services were estimated using points published in the Swiss tariff list (Tarmed) multiplied
by the average value per point based on the straight unweighted arithmetic mean of the tax point
values across all cantons of Switzerland for 2005, which was CHF 0.86 (for procedures and services).
For laboratory tests, a national rate of CHF 1.00 per tax point was applied. Tarmed positions and
Physician survey
associated tax points were obtained from the Tarmed Browser 1.2 which was valid for the year 2005.
The
2005
tax
point
values
were
obtained
from
Santesuisse’s
website
(www.santesuisse.ch/datasheets/files/200602011439030.xls) in June 2006. Respective data for
laboratory tests were obtained in June 2006 from the document “Analysenliste” on the website of the
Swiss Ministry of Health (www.bag.admin.ch/kv/gesetze/d/index.htm). Drug prices were obtained from
the 2005 Drug Reference Manual of Switzerland. Like for the patient survey, costs calculated in this
way were added up over all patients who were reported being given a specific drug or service in 2005
to result in total costs for all patients that reported use of this particular parameter in the respective
category of disease severity (mild, moderate, severe).
170 patients were documented by 57 dermatologists. Comparable to the patient survey, the majority of
patient was between 30 and 65 years old, with a mean age of 48 years. 19% of patients were
diagnosed with psoriasis between 55 and 25 years ago, 58% between 25 and 5 years ago, and 18%
less than 5 years ago.
Disease activity of psoriasis documented by the dermatologists was skewed towards higher severity
compared to the patient survey: 34% were reported as severe and 22% as moderate. In 21 patients,
PASI scores had been measured with the mean at 12.5. Patients indicated more involvement of nail
(54% vs. 31% by dermatologists), scalp (82 vs. 68% by dermatologists), and intertriginous (arm pits,
To estimate the costs of inpatient care a targeted analysis of Swiss Hospital Statistics was used. Costs
for inpatient care was estimated by multiplying the average LOS per patient with the average costs per
hospital day. In 2005 the average costs per day in hospital amounted to approximately CHF 1’070
[12].
genital, anal region) regions (19 vs. 9%, 32 vs. 25%, 33 vs. 20% resp. by dermatologists) than
identified by the dermatologists.
The results of the physician survey show the same trend of costs rising disproportionately with disease
severity: ambulatory costs range on average from CHF 1′100 per patient per year for mild psoriasis, to
CHF 2’500 for moderate psoriasis and CHF 9’900 for severe psoriasis. As expected, a relation
between ambulatory costs and severity of disease was observed (Table 3).
Results
Patient survey
5/13
6/13
Treatment with Biologics
The total direct cost of psoriasis in Switzerland is approximately CHF 314 to 458 million per year (cost
basis year 2005), depending on the severity distribution pattern used for the analysis and considering
In 2005, some patients with severe psoriasis received biologics, namely Enbrel (Etanercept), Amevive
out-of-pocket-expenses as well as costs for ambulatory and inpatient care (Table 4).
(Alefacept) or Raptiva (Efalizumab), resulting in total costs of CHF 2’154’547. These costs were added
to the treatment cost for severe psoriasis.
Discussion
Inpatient care
The aim of this study was to estimate the cost-of-illness for patients with psoriasis in Switzerland from
both a societal and individual perspective. In addition to the socioeconomic impact of psoriasis for the
Based on ICD-10 codes a total of 3’578 cases referring to 3’043 patients with diagnosis of psoriasis
whole society, the disease imposes a high financial burden on the patients themselves. To obtain data
were registered in Swiss hospitals in 2004. An average LOS of 16.71 days per hospitalized male
on out-of-pocket expenses and costs of outpatient/office-based care, surveys were distributed to
patient and 20.68 days per hospitalized female patient was reported, resulting in a weighted average
members of the Swiss Psoriasis and Vitiligo Society (SPVG), and office-/hospital-based Swiss
LOS for men (60%) and women (40%) of 18.3 days.
dermatologists, respectively. Additional inpatient costs were calculated on the basis of data obtained
from the Federal Statistical Office (FSO) regarding the number of cases treated for psoriasis in the
Resource use is documented by the Swiss hospital statistics in terms of the average length of stay
hospital and average length of hospital stay.
(LOS) in days per case. The reported 3’578 cases corresponded to 3’043 patients in 2004. Based on a
weighted average LOS of 18.3 days and average costs for one hospital day of approximately CHF
Cost-of-illness studies are a well-recognized tool to show the financial burden of diseases in a
1’070 [12], the costs of inpatient care amounts to approximately CHF 17’800 per year for a male and
particular country and to identify subgroups for which the costs are particularly high. Regardless of the
CHF 22’100 per year for a female patient hospitalized for psoriasis.
specific health system, cost-of-illness studies on psoriasis so far performed indicate considerable
economic consequences in countries such as the UK [1], Italy [3], the USA [4], Australia [5], and
Germany [7-9]. These studies have shown that the costs for psoriasis patients depend on disease
severity, with higher costs in the more severe cases. For this reason the resulting empirically derived
Extrapolating total direct costs of moderate-to-severe psoriasis for Switzerland
cost estimates for psoriasis extrapolated to the total adult population of Switzerland was of particular
Total costs of psoriasis for Switzerland were estimated for an estimated adult population of 5.8 million
interest for patients with moderate-to-severe psoriasis. One of the distinguishing characteristics of this
based on the numbers reported by the SFO. Assuming a conservative overall prevalence rate of
study is that it is the first to present total psoriasis-related costs on a patient-covered out-of-pocket
psoriasis of 1.5% based on observed prevalence rates in Western countries of 2-3% [2, 3, 14-17], a
basis and in an outpatient setting.
psoriasis patient population was of 86’170 was assumed in Switzerland.
In the US the 1998 National Psoriasis Foundation patient-membership survey identified 40% of the
To extrapolate costs, we used both the relative distribution of the categories of psoriasis severity
in a prevalence of severe psoriasis of 0.8% in the general population. However in a population-based
gained from the patient survey, namely 38% mild, 43% moderate and 19% severe psoriasis (Table 4,
study the prevalence of severe psoriasis was found to be ten times less (0.06% of the general
left half), as well as the often cited distribution by Crown et al. [18], with 79% of patients indicating
population) (Stern, J Invest Dermatol Symp Proc 2004; 9:136-9). Our calculation results were in the
mild, 12% moderate and 9% severe psoriasis (Table 4, right half).
range between these two publications, with a prevalence of 0.77% for moderate to severe psoriasis.
psoriasis patients to suffer from severe psoriasis (Krueger, Arch Dermatol 2001; 137: 280-4), resulting
The proportion of patients with mild (37%), moderate (42%) or severe psoriasis (19%) found here
Costs per patient increase considerably with the degree of disease severity, i.e. total costs per patient
differs somewhat from the epidemiological figures of often cited other works that have identified 21%
per year double from CHF 1’800 in mild psoriasis to CHF 3’600 in moderate psoriasis and increase
of all patients to suffer moderate to severe psoriasis [19], of which 56% have moderate and 44%
exponentially to between CHF 17’000-20’000 in severe psoriasis. Costs per severe patient vary with
severe psoriasis [7]. Based on these figures, an estimated 79% of patients would have mild, 12%
changes in prevalence rate as the costs of inpatient care were exclusively assigned to severe
moderate and 9% severe psoriasis. Our distribution might therefore not be representative for the
psoriasis as described above.
general population. Our sample was composed out of patient members of the SPVG and patients
treated in dermatologic practices. Both groups might be skewed towards higher severity of psoriasis.
In addition, the patients’ own estimation of body surface might be incorrect, however we believe this to
be unlikely, because relative accuracy of patients’ estimations with a much more complicated
7/13
8/13
instrument (SAPASI) has been described [20]. To obtain a sound estimate of costs, we used both
In conclusion, the present study indicates that psoriasis imposes a substantial economic burden on
severity pattern distributions (Table 4) for the calculations, reaching comparable total cost within a
Swiss society, the health insurance system, and the affected individuals themselves. The Swiss health
range of 31% (CHF 314 – 458 million).
insurance system is confronted with high direct in- and outpatient treatment costs of CHF 312-458
million per year. Moderate-to-severe psoriasis is associated with significant impact on quality of life
We found a relationship between the patient-reported effect of psoriasis on quality of life and the
and important costs, indicating need for efficient control of the disease. This cost-of-illness study
severity of disease as represented by the body surface area affected. The finding is not unexpected,
provides specific health economic data for further healthcare decision making, particularly with the
as it corresponds to a recently published report [9].
advent of new therapeutic agents that require economic assessment.
Potential limitations of this study include the rather low response rate of 32%. It is possible that the
Acknowledgements and Disclosure of Interest
patients with higher quality of life impairment responded to a larger extent than patients with
comparable to the literature [13, 21, 22]. and a possible recall bias of patients regarding their out-of-
The study was carried out by HealthEcon Ltd., Basel and funded by Wyeth Pharmaceuticals Ltd., Zug,
pocket expenses over the past 12 months. In addition, personal expenses on certain products, such
Switzerland. Particularly we would like to thank the participating patients and their organization, the
as skin care products and dietary supplements, do not necessarily reflect the patient’s current disease
Swiss Psoriasis and Vitiligo Society (SPVG), as well as contributing 57 Swiss dermatologists for their
status, but may merely reflect habitual use. As this study included only patients that are in the SPVG
cooperation in the surveys. The design, analysis and reporting of the study was performed by
or receiving treatment by a dermatologist, both with presumably relatively high loss of quality of life,
HealthEcon Ltd. according to pre-set objectives unrestricted by Wyeth Pharmaceuticals Ltd. and with
the proportion of patients that treat their psoriasis minimally was not included. In addition, patients
the scientific advice of RMT. Paolo Piffaretti is a representative of Wyeth. Elisabeth Brock and
organized in patients groups are likely to spend more money on their illness. The issue of missing data
Stephan Ruckdaeschel are employed by HealthEcon Ltd.
and the need to make some assumptions is of general concern in any questionnaire-based survey.
This was addressed by attempting to make assumptions likely to lead to an underestimate of costs,
rather than an overestimate, i.e. such as assuming the use of the smallest package size if information
on package size was missing. Regarding the cost of hospitalized patients, we could not differentiate
whether all patients were in the hospital for their psoriasis or had psoriasis as a secondary diagnosis.
Therefore, the real cost generated for the treatment of psoriasis in the hospital setting might be
somewhat lower.
Despite these limitations, the estimate provided by this study offers an approximation of the direct
costs associated with psoriasis in Switzerland. The results obtained were comparable to the results
from former studies in other countries [6-8]. In Germany, costs for inpatient treatment are estimated at
approximately € 160 million (CHF 239 million) ( [10] per year, compared to € 39 million (CHF 59
million) in Switzerland. This result is in line with the difference in population and higher Swiss hospital
costs. Regarding annual severity-related costs, one German study reported costs of € 2’866 (CHF
4’281) per patient and year for moderate, and € 4’985 (CHF 7’447) for severe psoriasis [7]. Another
study estimated mean total costs as € 6’709 (CHF 10’000) per patient and year [8]. The
corresponding costs in Switzerland amount to approximately € 2’410 (CHF 3’600) per patient per year
for moderate to approximately € 12’000 (CHF 16’000-20’000) for severe psoriasis.
The results of the present study indicate that the total burden of psoriasis in Switzerland amounts to
approximately CHF 312–458 million per year (cost basis year 2005). This represents between 0.61.1% of total direct health care expenditures in 2005 in Switzerland. Although the estimated total direct
costs for psoriasis amount to approximately 1% of total health care expenditures in Switzerland, these
costs are incurred by a relatively small group of patients (1-2% of total population).
9/13
10/13
Table 3: Costs of ambulatory care per patient per year according to state of severity
Figures and Tables
Table 1: Body areas affected as reported from patient and physician survey (multiple answers
were possible)
State of Severity
Cost Category
Body area
affected
Results from patient survey
Results from physician survey
Number and proportion of
patients reporting respective
area (n=383)
Number and proportion of
dermatologists reporting
respective area (n=170)
Back
193
50.40%
109
64.10%
Feet
136
35.50%
60
35.30%
Knee
244
63.70%
112
65.90%
Nails
208
54.30%
53
31.20%
(n=38)
1679
(n=74)
8466
(n=58)
(n=38)
813
(n=74)
1413
(n=58)
Total Ambulatory
Care
1136
(n=38)
2492
(n=74)
9878
(n=58)
Table 4: Total Costs across all Categories of Severity in Switzerland
Estimated prevalence rate 1.5%, distribution along
patients' indication:
18.80%
16
9.40%
57.70%
111
65.30%
Elbows
318
83.00%
126
74.10%
Genitals
124
32.40%
43
25.30%
Legs
275
71.80%
124
72.90%
Drugs
Scalp
314
82.00%
116
68.20%
Face
130
33.90%
40
23.50%
Skin Care
Products
Bathing Therapy
Hands
160
41.80%
73
42.90%
Sacral bone
135
35.20%
66
38.80%
43.60%
103
60.60%
33.40%
34
20.00%
Table 2: Out-of-pocket expenses per patient per year according to state of severity
State of Severity
Mild
Valid N
720
72
128
Valid N
416
221
167
Valid N
Severe
Mean Costs
[CHF]
Medical Services
Arms
Anal region
Moderate
Mean Costs
[CHF]
Prescribed Drugs
Arm pits
Upper part of
body
Mild
Mean Costs
[CHF]
Moderate
Severe
Mean Costs
[CHF]
Valid N
Mean Costs
[CHF]
Valid N
Mean Costs
[CHF]
Valid N
Drugs
43
(n=21)
49
(n=28)
330
(n=16)
Skin Care Products
135
(n=80)
216
(n=97)
318
(n=39)
Bathing Therapy
259
(n=26)
551
(n=49)
888
(n=19)
Other Measures
195
(n=32)
305
(n=43)
906
(n=37)
Total out-of-pocket
expenses
631
(n=143)
1122
(n=161)
2442
(n=71)
Mild
Moderate
severe
Mild
Moderate
Severe
38%, n=32534
43%, n=36930
19%, n=16706
79%, n=68074
12%, n=10134
9%, n=7962
1'387'674
1'820'325
5'518'079
2'903'608
499'517
4'377'296
7'967'522
5'315'580
9'159'175
2'186'376
2'533'456
8'410'832
20'362'590
14'838'861
17'599'058
5'587'720
7'072'342
Other Measures
6'358'743
11'279'546
15'130'220
13'305'211
3'095'232
7'211'206
Total out-ofpocket expenses
20'534'544
41'429'982
40'802'739
42'967'051
11'368'845
19'446'973
2'629'969
69'561'871
Prescribed Drugs
23'434'898
61'989'812
143'585'475
49'035'831
17'010'689
Medical Services
13'534'424
30'021'815
23'599'665
28'319'804
8'238'318
11'247'825
Total costs for
ambulatory care
36'969'321
92'011'626
167'185'140
77'355'635
25'249'007
80'809'696
Total costs for
inpatient Care
Total costs by
state of severity
Cost Category
Estimated prevalence rate 1.5%, costs calculated with
commonly assumed severity grades:
59'584'983
57'503'865
133'441'608
267'572'862
59'584'983
120'322'686
36'617'851
159'841'652
Total costs of
moderate to
severe psoriasis
401'014'470
196'459'504
Total costs
across all states
of severity
458'518'335
316'782'190
Total costs per
patient and
severity
1'768
3'613
16'017
1'768
3'613
20'076
“Valid n” denotes the number of patients reporting valid data for any particular cost category. 16
patients with severe psoriasis reported out-of-pocket expenses for drugs in 2005. Dividing the total
expenses on drugs reported by these 16 patients (in total approximately CHF 23’000; not shown in this
table) by all patients with severe psoriasis (n=71) results in the average out-of-pocket expenses of
CHF 330 for drugs per patient in the severe state of disease. Without this change in denominator the
respective expenses would be overestimated.
11/13
12/13
Figure 1: Relation between Disease Severity and Impact on Quality of Life
References
1.
Poyner T, Wall A, Adnitt P, A. M. Economic impact of psoriasis treatment on the patient
and on the National Health Service. J Dermatological Treatment 1999:25-9
2.
Galadari I, Rigel E, Lebwohl M. The cost of psoriasis treatment. J Eur Acad Dermatol
Venereol 2001;15:290-1.
3.
Finzi AF, Mantovani LG, Belisari A. The cost of hospital-related care of patients with
psoriasis in Italy based on the AISP study. Associazione Italiana Studi Psoriasi. J Eur Acad
Dermatol Venereol 2001;15:320-4.
4.
Javitz HS, Ward MM, Farber E, Nail L, Vallow SG. The direct cost of care for psoriasis
and psoriatic arthritis in the United States. J Am Acad Dermatol 2002;46:850-60.
5.
Jenner N, Campbell J, Plunkett A, Marks R. Cost of psoriasis: a study on the morbidity
and financial effects of having psoriasis in Australia. Australas J Dermatol 2002;43:255-61.
6.
Crown WH, Bresnahan BW, Orsini LS, Kennedy S, Leonardi C. The burden of illness
associated with psoriasis: cost of treatment with systemic therapy and phototherapy in the US.
Curr Med Res Opin 2004;20:1929-36.
7.
Berger K, Ehlken B, Kugland B, Augustin M. Cost-of-illness in patients with moderate
and severe chronic psoriasis vulgaris in Germany. J Dtsch Dermatol Ges 2005;3:511-8.
8.
Sohn S, Schoeffski O, Prinz J, Reich K, Schubert E, Waldorf K, et al. Cost of moderate
to severe plaque psoriasis in Germany: a multicenter cost-of-illness study. Dermatology
2006;212:137-44.
9.
Schoffski O, Augustin M, Prinz J, Rauner K, Schubert E, Sohn S, et al. Costs and quality
of life in patients with moderate to severe plaque-type psoriasis in Germany: a multi-center
study. J Dtsch Dermatol Ges 2007;5:209-18.
10.
Traupe H, Robra B. Psoriasis. Gesundheitsberichterstattung des Bundes 2002.
11.
Finlay AY, Khan GK, Luscombe DK, Salek MS. Validation of Sickness Impact Profile and
Psoriasis Disability Index in Psoriasis. Br J Dermatol 1990;123:751-6.
12.
Press release 0350-0703-10 from March 19th, 2007. Federal Statistical Office (FSO) of
Switzerland.
13.
Zachariae R, Zachariae H, Blomqvist K, Davidsson S, Molin L, Mork C, et al. Quality of
life in 6497 Nordic patients with psoriasis. Br J Dermatol 2002;146:1006-16.
14.
Nevitt GJ, Hutchinson PE. Psoriasis in the community: prevalence, severity and
patients' beliefs and attitudes towards the disease. Br J Dermatol 1996;135:533-7.
15.
Ferrandiz C, Bordas X, Garcia-Patos V, Puig S, Pujol R, Smandia A. Prevalence of
psoriasis in Spain (Epiderma Project: phase I). J Eur Acad Dermatol Venereol 2001;15:20-3.
16.
Naldi L. Epidemiology of psoriasis. Curr Drug Targets Inflamm Allergy 2004;3:121-8.
17.
Amblard P. [Psoriasis. Diagnosis, clinical course, prognosis, treatment]. Rev Prat
1993;43:229-31.
18.
Crown WH. The cost of psoriasis. Manag Care 2003;12:10-3; discussion 20-1.
19.
The Burden of Skin Diseases 2005. In: Prepared for The Society for Investigative
Dermatology and The American Academy of Dermatology Association: LEWIN GROUP 2005.
20.
Fleischer AB, Jr., Feldman SR, Dekle CL. The SAPASI is valid and responsive to
psoriasis disease severity changes in a multi-center clinical trial. J Dermatol 1999;26:210-5.
21.
Blumberg HH, Fuller C, Hare AP. Response Rates in Postal Surveys. Public Opinion
Quarterly 1974;38:113-23.
22.
Eaker S, Bergstrom R, Bergstrom A, Adami HO, Nyren O. Response rate to mailed
epidemiologic questionnaires: a population-based randomized trial of variations in design and
mailing routines. Am J Epidemiol 1998;147:74-82.
13/13
14/13
100
Appendix 6
Laffitte E, Dudler J, Panizzon RG. Psoriasis unguéal et traitements anti-TNFα
α.
Ann Dermatol Venereol 2004;131:1S71-1S272 and presented as a poster in
Journées Dermatologiques de Paris, 7-11 décembre 2004.
101
102
Psoriasis unguéal et traitements anti-TNFα
E Laffitte, J Dudler*, RG Panizzon
Services de Dermatologie et Vénéréologie et *Rhumatologie, Centre Hospitalier
Universitaire Vaudois, DHURDV, Lausanne, Suisse
INTRODUCTION
Le psoriasis unguéal est fréquent, interfère sévèrement avec la qualité de vie des patients (1), et est de traitement difficile, surtout lorsque
l'atteinte est mutiple. Nous rapportons l'efficacité des anti TNFα (infliximab et etanercept) dans un cas de psoriasis cutané et unguéal.
OBSERVATION
Un homme de 45 ans, était hospitalisé pour une poussée de psoriasis cutané étendu avec atteinte des 20 ongles, sans amélioration après
deux mois de traitement par 25 mg/semaine de méthotrexate (MTX). Des injections intraveineuses d'infliximab (Rémicade®) étaient
ajoutées. Le patient était blanchi en 21 jours. Après 4 mois de traitement, les ongles des mains étaient redevenus normaux.
1
2
3
Aspect de l’ongle avant (1), après deux mois (2) et 4 mois (3) du traitement par MTX et infliximab: guérison progressive de l’atteinte psoriasique unguéale
Après 10 mois, le MTX et l'infliximab étaient interrompus suite à un abcès périanal, les lésions cutanées et unguéales récidivaient. La
reprise du MTX associé à des injections sous cutanées d'etanercept (Enbrel®) contrôlait le psoriasis cutané et unguéal en 4 mois.
4
5
6
Réapparition du psoriasis unguéal après arrêt de l’infliximab (4), reprise du processus de guérison après deux mois (5) et 4 mois (6) du traitement par MTX et etanercept
COMMENTAIRES
La prise en charge du psoriasis unguéal avec atteinte multiple est difficile. Les traitements locaux sont inadaptés, les traitement
systémiques peuvent être efficaces, souvent en parallele avec l'atteinte cutanée (1). Les traitements biologiques dirigés contre le TNFα
semblent améliorer le psoriasis unguéal, mais leur action ne pourrait être que suspensive, comme pour les autres traitements du psoriasis.
REFERENCES
1- De Berker D. Management of nail psoriasis. Clin Exp Dermatol 2000, 25:357-62
104
Appendix 7
Laffitte E, Kunzle N, Mottet C, Panizzon RG. Severe psoriasis with chronic
active hepatitis C: treatment by etanercept. Brit J Dermatol 2006;154 :25, and
presented as a poster in 4th International Congress on Psoriasis - From Gene to
Clinic, London, 4-6 December 2006.
105
106
Psoriasis with chronic active hepatitis C:
treatment with etanercept (Enbrel®)
E Laffitte, N Kunzle, C Mottet*, RG Panizzon
Depts of Dermatology and *Gastro-enterology , CHUV/DHURDV, Lausanne, Switzerland
INTRODUCTION
The therapy of severe psoriasis is difficult in patients with chronic hepatitis C. We report two cases of psoriasis in patients with chronic,
active hepatitis C, treated with etanercept without worsening of the hepatitis.
CASES REPORT
Two patients were followed for chronic active hepatitis C and a severe psoriasis. A treatment with etanercept, 25 mgx2 per week was
started. The psoriasis was improved (obtaining the PASI 90 for a case, and PASI 75 for the other), the viremia and hepatic parameters
remained stable with respectively 16 and 9 months of follow-up.
Pal (N 36-108)
Units/l
150
Mois
100
gGT (N 11-62)
50
ASAT and ALAT
(N 11-60)
Month
M9
M8
M7
M6
M5
M4
M3
M2
M1
M9
M8
M7
M6
M5
M4
M1
M3
0
M2
Viremia (HCV-RNA, kUIml)
200
Etanercept
Month
Etanercept
Liver enzyme parameters
HCV viremia
700
600
500
400
300
200
100
0
M9
M8
M7
M6
M5
M4
M3
M2
35
30
25
20
15
10
5
0
M1
PASI
PASI
Month
Etanercept
Patient 1: Progressive control of the psoriasis with achievement of PASI 75; liver enzyme parameters and HCV viremia remained stable.
HCV viremia
1x25 2x25
Etanercept
2x50
Month
Etanercept
M16
M16
M14
M12
M10
M8
M6
M4
M16
M14
M12
M10
M8
M6
M4
Month
2x25
Pal (N 36-108)
gGT (N 11-62)
0
0
M2
Etanercept
(mg/w)
50
5000
M14
2
0
M12
4
M10
6
ASAT et ALAT
(N 11-60)
100
10000
M8
8
150
15000
M6
10
200
20000
M2
PASI
14
12
25000
M4
16
M2
18
Liver enzyme parameters
Units/l
Viremia (HCV-RNA, kUIml)
PASI
Month
2x25
Patient 2: Good initial psoriasis control with PASI 90 achievement (M3). After reducing etanercept doses to 25 mg/w (M8) a rapid relapse was observed.
Etanercept was augmented to 2x25 mg/w (M9) and then 2x50 mg/w (M10) to control again the psoriasis, and then reduced again to 2x25 mg/w (M13)
without any relapse. Liver enzyme parameters remained stable, HCV viremia fluctuation can be explained by the natural evolution of the disease.
COMMENTS
The association chronic active C hepatitis and psoriasis is a real therapeutic challenge. The hepatitis contra-indicates the use of
methotrexate or ciclosporine, the psoriasis may be worsen by interferon and ribavirin. In our two cases, the psoriasis was controlled and
the hepatitis remain stable.
Almost thirty cases of inflammatory rheumatic or digestive diseases treated by anti-TNF agents (etanercept or infliximab) in patients
with chronic C hepatitis have been reported (1). Inhibition of TNF is a recognized therapeutic option for psoriasis and does not seem to
be deleterious for chronic C hepatitis (and could even be beneficial for some authors). The situation seems to be different for B hepatitis,
since several cases of HBV reactivation with a case of fulminant hepatitis were reported under infliximab (2).
Thus, etanercept is an interesting therapeutic option in patients with severe psoriasis and chronic active C hepatitis.
REFERENCES
1- Peterson JR, Hsu FC, Simkin PA, Wener MH. Effect of tumour necrosis factor alpha antagonists on serum transaminases and viraemia in patients with
rheumatoid arthritis and chronic hepatitis C infection. Ann Rheum Dis 2003;62:1078-82.
2- Michel M et al. Fulminant hepatitis after infliximab in a patient with hepatitis B virus treated for an adult onset still's disease. J Rheumatol 2003;30:1624-5.
108
Appendix 8
Laffitte E, Janssens JP, Roux-Lombard P, Thielen AM, Barde C, Marazza G,
Panizzon RG, Saurat JH. Tuberculosis screening in patients with psoriasis
before antitumour necrosis factor therapy: comparison of an interferon-gamma
release assay vs. tuberculin skin test. Br J Dermatol 2009;161:797-800.
109
110
C L I N I C A L A N D LA B O R A T O R Y I N V E S T I G A T I O N S
BJD
British Journal of Dermatology
Tuberculosis screening in patients with psoriasis before
antitumour necrosis factor therapy: comparison of an
interferon-c release assay vs. tuberculin skin test
E. Laffitte, J.P. Janssens,* P. Roux-Lombard, A.M. Thielen, C. Barde, G. Marazza, R.G. Panizzon and
J.-H. Saurat
Clinic of Dermatology, and Divisions of *Pulmonary Diseases and Immunology and Allergy, University Medical Hospital, CH-1211 Geneva, Switzerland
Clinic of Dermatology, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland
Summary
Correspondence
Emmanuel Laffitte.
E-mail: [email protected]
Accepted for publication
25 May 2009
Key words
adalimumab, etanercept, infliximab, psoriasis,
T-SPOT.TB, tuberculosis
Conflicts of interest
None declared.
Presented at the 5th International
Congress Psoriasis from Gene to Clinic, London,
U.K., 4–6 December 2008 and awarded the
poster prize.
DOI 10.1111/j.1365-2133.2009.09331.x
Background Antitumour necrosis factor (anti-TNF) treatments may reactivate latent
tuberculosis infection (LTBI). For detecting LTBI, the tuberculin skin test (TST)
has low sensitivity and specificity. Interferon-c release assays (IGRA) have been
shown to be more sensitive and specific than TST.
Objective To compare the TST and the T-SPOT.TB IGRA for identifying LTBI in
patients with psoriasis before anti-TNF treatment.
Methods A retrospective study was carried out over a 4-year period on patients
with psoriasis requiring anti-TNF treatment. All were subjected to the TST,
T-SPOT.TB and chest X-ray. Risk factors for LTBI and history of bacillus
Calmette–Guérin (BCG) vaccination were recorded. The association of T-SPOT.TB
and TST results with risk factors for LTBI was tested through univariate logistic
regression models. Agreement between tests was quantified using kappa statistics.
Treatment for LTBI was started 1 month before anti-TNF therapy when indicated.
Results Fifty patients were included; 90% had prior BCG vaccination. A positive
T-SPOT.TB was strongly associated with a presumptive diagnosis of LTBI (odds
ratio 7Æ43; 95% confidence interval 1Æ38–39Æ9), which was not the case for the
TST. Agreement between the T-SPOT.TB and TST was poor, j = 0Æ33 (SD 0Æ13).
LTBI was detected and treated in 20% of the patients. In 20% of the cases, LTBI
was not retained in spite of a positive TST but a negative T-SPOT.TB. All patients
received an anti-TNF agent for a median of 56 weeks (range 20–188); among
patients with a positive TST ⁄negative T-SPOT.TB, no tuberculosis was detected
with a median follow-up of 64 weeks (44–188). One case of disseminated
tuberculosis occurred after 28 weeks of adalimumab treatment in a patient with
LTBI in spite of treatment with rifampicin.
Conclusion This study is the first to underline the frequency of LTBI in patients
with psoriasis (20%), and to support the use of IGRA instead of the TST for its
detection. Nevertheless, there is still a risk of tuberculosis under anti-TNF therapy, even if LTBI is correctly diagnosed and treated.
Antitumour necrosis factor (anti-TNF)-a agents are approved
for the treatment of psoriasis or other inflammatory diseases.
However, they may reactivate latent tuberculosis infection
(LTBI).1,2 Thus, screening for LTBI is mandatory and preventive treatment should be given to all patients with evidence of
LTBI before starting any anti-TNF-a therapy,3 even if it does
not offer complete protection.4 Screening for LTBI is traditionally based on history, chest X-ray and the tuberculin skin test
(TST).5–7 However, the TST has disadvantages: a low specific-
ity with false-positive results in bacillus Calmette–Guérin
(BCG)-vaccinated subjects. This leads to unnecessary treatments for LTBI with a significant risk of drug toxicity, and
lower sensitivity in immunosuppressed patients compared
with healthy subjects resulting in false-negative results and a
subsequent risk of tuberculosis reactivation with anti-TNF
therapy. Finally, the limit above which the TST is considered
positive (i.e. indicative of latent infection) differs according to
countries and guidelines (5–10 mm).
2009 The Authors
Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2009 161, pp797–800
797
798 Tuberculosis screening in psoriasis patients, E. Laffitte et al.
Since the early 2000s, in vitro blood tests measuring production of interferon (IFN)-c by T cells exposed to antigens
highly specific for Mycobacterium tuberculosis have been developed.
These tests (T-SPOT.TB; Oxford Immunotec, Oxford, U.K. and
QuantiFERON-TB Gold; Cellestis, Carnegie, Australia), collectively referred to as IFN-c release assays (IGRAs), are not
affected by prior BCG vaccination, thus offering increased
specificity compared with the TST.8 Their sensitivity, extrapolated from studies in patients with active tuberculosis, is probably at least as good as that of the TST in the detection of
LTBI. Recent guidelines have integrated the use of IGRAs in
screening strategies for subjects exposed to tuberculosis. The
U.S. Centers for Disease Control and Prevention guidelines9
state that the QuantiFERON-TB Gold test can be used in all
circumstances in which the TST is used and can be used in
place of the TST. The U.K. National Institute for Health and
Clinical Excellence 2006 guidelines10 and the 2007 Swiss
national guidelines11 both recommend, for immunocompetent
adults, a two-step procedure, i.e. confirmation of positive TST
results using an IGRA.
However, there are few data on LTBI detection and use of
IGRAs in patients with psoriasis. The aim of this study was
(i) to determine the frequency of LTBI in a population of
patients with psoriasis before anti-TNF treatment, (ii) to compare the TST with T-SPOT.TB for detecting LTBI, and (iii) to
evaluate the tolerance and effectiveness of treatment for LTBI
under anti-TNF therapy in our patients.
Materials and methods
This retrospective study was conducted in two academic dermatological centres (University Hospital, Geneva and CHUV,
Lausanne). All patients seen between November 2004 and
March 2008 with moderate to severe psoriasis qualifying for
anti-TNF-a therapy were screened for LTBI with a chest X-ray,
a TST and a T-SPOT.TB IGRA. The TST was considered positive
if the induration diameter was ‡ 5 mm. As there is no ‘gold
standard’ test for the diagnosis of LTBI, we aimed to evaluate
the risk factors for LTBI by recording the following data: age;
country of origin and tuberculosis incidence in the country of
origin according to World Health Organization data; history
of tuberculosis exposure (family or work); history of prolonged stay in a high-incidence area; BCG vaccination; and
prior immunosuppressive therapy (methotrexate, ciclosporin
or efalizumab).
In the absence of a ‘gold standard’ for the diagnosis of
LTBI, we analysed results of the T-SPOT.TB and the TST in
relation to the risk factors for LTBI, BCG-vaccination status,
and to a composite variable defining a probable diagnosis of
LTBI (‘probable LTBI’) defined as having a history of definite
exposure to a case of active tuberculosis and ⁄or having a chest
X-ray suggestive of prior tuberculosis infection (granulomas,
calcified adenopathy) and ⁄or originating from a high-incidence country (defined as > 40 cases in 100 000 per year).
The association of either T-SPOT.TB or TST results with risk
factors for LTBI or BCG-vaccination status was tested through
univariate logistic regression models. Agreement between tests
was quantified using kappa statistics. All statistical analyses
were performed with SPSS version 14.0, 2006 (Statistical Package for Social Sciences Inc., Chicago, IL, U.S.A.).
If LTBI was diagnosed, treatment with either rifampicin
(10 mg kg)1, max. 600 mg daily) for 4 months or isoniazid
(5 mg kg)1, max. 300 mg daily) for 9 months was started
1 month before introducing anti-TNF-a therapy, according to
the Swiss guidelines.11
Results
Fifty patients were analysed (Table 1). Ten patients (20%) came
from or had lived in a country with a high incidence of tuberculosis. Forty-five patients (90%) had prior BCG vaccination.
Comparative results of tuberculin skin test and
T-SPOT.TB
In 28 patients (56%), the TST and T-SPOT.TB were both negative. In eight patients (16%) both the T-SPOT.TB and TST
(‡ 5 mm) were positive. Two cases had a negative TST but a
positive T-SPOT.TB with a chest X-ray suggestive of LTBI (granuloma). In 12 cases (24%) the TST was positive and the
T-SPOT.TB was negative; all had prior BCG vaccination and a
normal chest X-ray. Agreement between both tests was poor for
TST ‡ 5 vs. T-SPOT.TB: 36 ⁄50 (72%), j = 0Æ33 (SD 0Æ13).
Probability of having a positive interferon-c release
assay or tuberculin skin test according to specific risk
factors
Table 2 shows the association between the presence of risk
factors for LTBI and results of an IGRA and TST based on univariate logistic regression analyses. Significant associations
were found between having a positive T-SPOT.TB and probable LTBI, a chest X-ray suggestive of LTBI or a history of
exposure to active tuberculosis. There was no association with
age, previous immunosuppressive therapy or country of origin
with a high incidence of tuberculosis. Conversely, none of the
above-mentioned variables was associated with having a TST
either ‡ 5 or 10. Association with BCG-vaccination status
could not be tested, because of the high rate of patients vaccinated (90%). Results from the multivariable analysis (not
shown) were not significant.
Latent tuberculosis infection diagnosis and treatment
A diagnosis of LTBI was considered in the 10 cases (20%)
with a positive T-SPOT.TB. In 28 patients with both a negative
TST and T-SPOT.TB, LTBI was considered as reasonably
excluded. In 12 cases (24%) with a TST ‡ 5 but a negative
T-SPOT.TB, all with a prior BCG vaccination and a normal
X-ray, a diagnosis of LTBI was not considered.
A total of 12 patients were treated for LTBI (nine with rifampicin and three with isoniazid): the 10 patients with LTBI,
2009 The Authors
Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2009 161, pp797–800
Tuberculosis screening in psoriasis patients, E. Laffitte et al. 799
Table 1 Characteristics of the 50 patients analysed
TST ‡ 5 mm
T-SPOT.TB
Characteristic
All (n = 50) Pos (n = 10)
Age (years), mean (range)
Male, n (%)
Prior immunosuppressive
therapya, n (%)
BCG vaccination, n (%)
Risk factors for LTBI, n (%)
High TB incidence in country
of origin
Contact with TB patient
(family or work)
Chest X-ray suggestive of TB
Probable LTBIb
48 (17–74)
35 (70)
34 (68)
Neg (n = 40) Pos (n = 20)
TST ‡ 10 mm
Neg (n = 30) Pos (n = 18)
Neg (n = 32)
54Æ3 (25–63) 46Æ4 (17–75) 47Æ5 (17–64) 48Æ3 (25–74) 49Æ2 (25–64) 47Æ3 (17–75)
6 (60)
29 (72)
12 (60)
23 (77)
11 (61)
24 (75)
8 (80)
26 (65)
12 (60)
22 (73)
10 (55Æ5)
24 (75)
45 (90)
9 (90)
36 (90)
19 (95)
26 (87)
17 (94)
28 (87Æ5)
10 (20)
3 (30)
7 (17)
6 (30)
4 (13)
5 (27Æ8)
5 (15Æ6)
11 (22)
5 (50)
6 (15)
6 (30)
5 (17)
5 (27)
6 (18Æ75)
4 (8)
21 (42)
4 (40)
8 (80)
0 (0)
14 (35)
2 (10)
11 (55)
2 (7)
11 (37)
2 (11Æ1)
12 (66Æ6)
2 (6Æ25)
10 (31Æ2)
BCG, bacillus Calmette–Guérin; LTBI, latent tuberculosis infection; TST, tuberculin skin test; Pos, positive; Neg, negative. aMethotrexate,
ciclosporin or efalizumab. bProbable LTBI was defined as having a history of definite exposure to a case of active TB and ⁄ or having a chest
X-ray suggestive of prior TB infection (granulomas, calcified adenopathy) and ⁄ or originating from a country with a high incidence (defined
as > 40 in 100 000 per year).
Table 2 Association of either T-SPOT.TB or the tuberculin skin test (TST) results with risk factors for latent tuberculosis infection (LTBI):
univariate logistic regression models
Characteristics
Age
Prior immunosuppressive therapya
Risk factor for LTBI
High TB incidence in country of origin
Contact with TB patient (family or work)
Chest X-ray suggestive of TB
Probable LTBIb
T-SPOT.TB
TST ‡ 5 mm
Odds ratio (95% CI)
TST ‡ 10 mm
Odds ratio (95% CI)
Odds ratio (95% CI)
1Æ05 (0Æ99–1Æ11)
1Æ71 (0Æ31–9Æ3)
0Æ99 (0Æ95–1Æ0)
0Æ85 (0Æ24–2Æ97)
1Æ01 (0Æ99–1Æ11)
0Æ66 (0Æ18–2Æ36)
2Æ02 (0Æ42–9Æ8)
5Æ67 (1Æ25–25Æ7)
25Æ3 (2Æ41–267)
7Æ43 (1Æ38–39Æ9)
2Æ78 (0Æ67–11Æ7)
2Æ14 (0Æ55–8Æ3)
2Æ6 (0Æ39–17Æ4)
3 (0Æ93–9Æ7)
2Æ07 (0Æ51–8Æ47)
1Æ67 (0Æ43–6Æ5)
3Æ21(0Æ48–21Æ4)
2Æ08 (0Æ64–6Æ73)
CI, confidence interval. aPrior immunosuppressive therapy: methotrexate, ciclosporin or efalizumab. bProbable LTBI defined as having a
history of definite exposure to a case of active TB and ⁄ or having a chest X-ray suggestive of prior TB infection (granulomas, calcified
adenopathy) and ⁄ or originating from a country with a high incidence (defined as > 40 in 100 000 per year). Bold text: significant association (P < 0Æ01)
and two patients with a positive TST (‡ 5 mm) and a negative
T-SPOT.TB but included in a clinical trial which did not accept
the validity of T-SPOT.TB. There were no serious adverse
effects with the LTBI treatment; two patients had an elevation
of transaminase less than five times the normal limit, which
did not required the interruption of therapy.
Antitumour necrosis factor therapy
Patients received anti-TNF-a therapy (etanercept, infliximab or
adalimumab) for a median of 56 weeks (range 20–188). No
case of tuberculosis occurred in the 10 patients with a positive
TST ⁄negative T-SPOT.TB who were not treated for LTBI, after
a median duration of 64 weeks of anti-TNF therapy (range
44–188). A disseminated tuberculosis occurred after 28 weeks
of adalimumab in a patient with LTBI treated with rifampicin
for 4 months.
Discussion
The present study is to our knowledge the first to show that,
in a population of patients treated for psoriasis, a positive
T-SPOT.TB IGRA is strongly associated with the presence of
risk factors for LTBI. This association was not found for the
TST, and agreement between the T-SPOT.TB and TST was
poor, probably because of a high rate of BCG-vaccinated
patients (90%) acting as a confounding factor. As there is no
gold standard for the diagnosis of LTBI, it was impossible to
estimate the true sensitivity and specificity of either test in this
setting.
2009 The Authors
Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2009 161, pp797–800
800 Tuberculosis screening in psoriasis patients, E. Laffitte et al.
There are very few data concerning LTBI and the use of
IGRAs in patients with psoriasis. In a recent report of 11
patients, Desai et al.12 studied the utility of another IGRA
(QuantiFERON) in screening for LTBI before anti-TNF therapy. They suggest that QuantiFERON should replace the TST
for LTBI screening because its validity is well documented in
rheumatological disorders, but there was no evaluation of risk
factors for LTBI in the patients assessed.
We chose to base our diagnosis of LTBI on the results of
the T-SPOT.TB rather than on the TST. Several points suggest
that patients with LTBI were correctly identified: patients with
a positive T-SPOT.TB had a significant association with risk
factors for LTBI; and in 10 of 12 patients with a positive TST
and a negative T-SPOT.TB, no treatment was given and no
tuberculosis occurred under anti-TNF therapy with a mean
follow-up of 76 weeks. According to the literature, most cases
of tuberculosis in patients receiving anti-TNF therapy are
detected within 12 months of the beginning of anti-TNF treatment.13 Treatment for LTBI was administered in 12 cases, and
was avoided in 10 patients, whereas it would have been given
to 22 patients if we have followed the guidelines based on the
TST alone. Treatment for LTBI was relatively well tolerated,
with a slight elevation of transaminases in two patients.
Twenty per cent of our patients had a probable LTBI which
we consider to be a high rate; however, we were unable to
compare our results with those from other studies, as published data only report the frequency of tuberculosis in
patients under an anti-TNF agent for moderate to severe
plaque psoriasis.6 In these studies, the patients were screened
for LTBI and treated if necessary before the anti-TNF treatment, but the actual number diagnosed with LTBI, and the
tolerance of its therapy are not reported.
An important message from our observations is that the risk
of active tuberculosis under anti-TNF therapy persists even if
LTBI is diagnosed and treated. Indeed, a case of disseminated
tuberculosis occurred in a patient adequately treated for LTBI.
Even if screening of LTBI reduces the occurrence of active
tuberculosis under anti-TNF therapy,14 a residual risk remains,
with atypical and disseminated presentations that dermatologists should be aware of.
Our study had a few limitations. It was retrospective in
design, but as all patients seen in both institutions were analysed, the risk of selection bias was limited. Also, we included a
relatively low number of patients, which may have limited the
feasibility of certain statistical computations (i.e. multivariate
logistic regression). However, the data presented are the first
to show in this population highly significant univariate results
between risk factors for LTBI and the T-SPOT.TB, and support
the use of IGRAs instead of the TST.
References
1 Keane J, Bresnihan B. Tuberculosis reactivation during immunosuppressive therapy in rheumatic diseases: diagnostic and therapeutic strategies. Curr Opin Rheumatol 2008; 20:443–9.
2 Gardam MA, Keystone EC, Menzies R et al. Antitumour necrosis
factor agents and tuberculosis risk: mechanisms of action and clinical management. Lancet Infect Dis 2003; 3:148–55.
3 Lin J, Ziring D, Desai S et al. TNFalpha blockade in human diseases:
an overview of efficacy and safety. Clin Immunol 2008; 126:13–30.
4 Sichletidis L, Settas L, Spyratos D et al. Tuberculosis in patients
receiving anti-TNF agents despite chemoprophylaxis. Int J Tuberc
Lung Dis 2006; 10:1127–32.
5 British Thoracic Society Standards of Care Committee. BTS recommendations for assessing risk and for managing Mycobacterium tuberculosis infection and disease in patients due to start anti-TNF-alpha
treatment. Thorax 2005; 60:800–5.
6 Doherty SD, Van Voorhees A, Lebwohl MG et al. National Psoriasis
Foundation consensus statement on screening for latent tuberculosis infection in patients with psoriasis treated with systemic and
biologic agents. J Am Acad Dermatol 2008; 59:209–17.
7 Centers for Disease Control and Prevention. Guide for primary health
care providers: targeted tuberculin testing and treatment of latent tuberculosis infection. Available at: http://www.cdc.gov/tb/publications/LTBI/pdf/
TargetedLTBI05.pdf (last accessed 10 June 2009).
8 Menzies D, Pai M, Comstock G. Meta-analysis: new tests for the
diagnosis of latent tuberculosis infection: areas of uncertainty and
recommendations for research. Ann Intern Med 2007; 146:340–54.
9 Mazurek GH, Jereb J, Lobue P et al. Guidelines for using the
QuantiFERON-TB Gold test for detecting Mycobacterium tuberculosis
infection, United States. MMWR Recomm Rep 2005; 54:49–55.
10 National Institute for Health and Clinical Excellence. Tuberculosis.
Clinical Diagnosis and Management of tuberculosis, and measures for
its prevention and control. Available at: http://www.nice.org.uk/
CG033. Last updated March 2006 (last accessed 10 June 2009).
11 Beglinger C, Dudler J, Mottet C et al. Screening for tuberculosis
infection before the initiation of an anti-TNF-alpha therapy. Swiss
Med Wkly 2007; 137:620–2.
12 Desai N, Raste Y, Cooke NT, Harland CC. QuantiFERON-TB Gold
testing for tuberculosis in psoriasis patients commencing antitumour necrosis factor alpha therapy. Br J Dermatol 2008;
158:1137–8.
13 Bieber J, Kavanaugh A. Tuberculosis and opportunistic infections:
relevance to biologic agents. Clin Exp Rheumatol 2004; 22:S126–33.
14 Gomez-Reino JJ, Carmona L, Angel Descalzo M. Risk of tuberculosis in patients treated with tumor necrosis factor antagonists due to
incomplete prevention of reactivation of latent infection. Arthritis
Rheum 2007; 57:756–61.
2009 The Authors
Journal Compilation 2009 British Association of Dermatologists • British Journal of Dermatology 2009 161, pp797–800
Appendix 9
Dumont-Berset M, Laffitte E, Gerber C, Dudler J, Panizzon RG. Eczematous
drug eruption after infliximab. Br J Dermatol 2004;151:1272-3.
115
116
British Journal of Dermatology 2004; 151: 1272–1288.
CORRESPONDENCE
Eczematous drug eruption after infliximab
DOI: 10.1111/j.1365-2133.2004.06282.x
SIR, Infliximab (Remicade, Schering-Plough), a humanized
antitumour necrosis factor (TNF)-a monoclonal antibody, has
been associated with several cutaneous side-effects.1–4 We
report a patient with an eczematous eruption that appeared
after the administration of infliximab.
A 36-year-old man presented with a diffuse pruritic rash of
1 week’s duration. He had been receiving treatment for
3 months with oral leflunomide 20 mg daily and intravenous
infliximab 3 mg kg)1 at weeks 0, 2 and 6 for a palmoplantar
pustular psoriasis with severe arthritis. Four days after the
third infusion of infliximab he developed a pruriginous
maculopapulovesicular erythematosquamous eruption of
the limbs and trunk (Fig. 1a). There was no history of allergy
or eczema. Abnormal laboratory results included elevated
erythrocyte sedimentation rate at 35 mm in the first hour
(normal < 10), white blood cell count of 15Æ1 · 109 L)1 with
71% neutrophils and 1% eosinophils, and C-reactive protein
at 49 mg L)1 (normal < 10). Human immunodeficiency
virus, syphilis and Chlamydia serology were negative and
there was no evidence for any viral disease. Skin biopsy
showed spongiform dermatitis with oedema in the epidermis
between keratinocytes and the upper dermis, associated with
keratinocyte necrosis, and a lymphocytic infiltrate in the
upper dermis (Fig. 1b). The skin condition improved within
2 weeks after stopping the two drugs and the use of topical
steroids. One month later, patch tests to leflunomide and
infliximab were negative. As infliximab had been proving
beneficial for the arthritic condition in this patient, rechallenge with a perfusion of 50 mg of infliximab was attempted.
Two days later, the eczematous rash reappeared with an
identical histological pattern. Thereafter, infliximab was
switched to subcutaneous etanercept (Enbrel, Wyeth),
another TNF-a inhibitor, without recurrence of the rash.
TNF-a inhibitors are highly effective in the treatment of
early and chronic rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, Crohn’s disease and psoriatic skin
lesions.5 In clinical studies with infliximab, a humanized
mouse monoclonal antibody against human TNF-a, adverse
drug reactions were most frequently reported in the respiratory system (upper and lower respiratory tract infections),
and in the skin and appendages.1 The most frequently
described skin side-effects are mainly delayed hypersensitivity
reactions: erythema multiforme, leucocytoclastic vasculitis,
annular lichenoid eruption, lupus-like syndrome, bullous skin
lesions4 and eczematide-like purpura.1–4,6 Several eczematous skin eruptions following infliximab have been reported
previously.5,7 Skin reactions typically arise after one or
several repeated treatments, and at 1–14 days after the
injection.
In arthritic conditions, infliximab is classically given with
methotrexate to reduce the incidence of human antichimeric
1272
Figure 1. (a) First eczematous rash 4 days after the third infusion of
infliximab in combination with leflunomide. (b) Histopathology confirmed a spongiform dermatitis associated with keratinocyte necrosis
and a lymphocytic infiltrate in the upper dermis (haematoxylin and
eosin; original magnification · 100).
2004 British Association of Dermatologists
CORRESPONDENCE
antibodies. Methotrexate may be replaced by leflunomide in
patients intolerant to methotrexate, but the combination of
infliximab and leflunomide has been associated with a high
frequency of adverse events.6 Kiely and Johnson6 reported a
pruriginous rash in 14 of 20 rheumatoid arthritis patients
treated with this combination. The skin reactions were
characterized by eczematous patches with excoriations, and
in some cases with lichenoid features.
Despite the fact that the molecule is well absorbed
percutaneously,3 patch tests were negative in our patient,
and only the rechallenge during a perfusion allowed us to
confirm that infliximab was the cause of the eczematous rash.
This led to discontinuation of infliximab. In one similar case,
the dermatitis flared after each infliximab infusion, but
responded to therapy with topical steroids and topical
0Æ03% tacrolimus.7
Finally, we did not observe cross-reactivity between infliximab and etanercept. No eczematous eruption developed
under etanercept therapy. Thus, this adverse effect appears to
be related to the molecular structure of infliximab rather than
being a consequence of TNF-a blockade, as both drugs share
the similar purpose of TNF-a blockade, but have different
structures, one being a humanized antibody and the other a
fusion protein between the p75 human TNF-a receptor and
a human immunoglobulin. However, an eruption with a
pattern of erythema multiforme has been observed in
a patient following treatment with both infliximab and
etanercept, and this could be related to TNF-a blockade in
this case.3
Departments of Dermatology and
*Rheumatology, Centre Hospitalier
Universitaire Vaudois, CH-1011
Lausanne, Switzerland
Correspondence: E. Laffitte,
E-mail: [email protected]
M.Dumont-Berset
E.Laffitte
C.Gerber
J.Dudler*
R.G.Panizzon
References
1 Devos SA, van den Bossche N, de Vos M, Naeyaert JM. Adverse
skin reactions to anti-TNF-alpha monoclonal antibody therapy.
Dermatology 2003; 206: 388–90.
2 Kent PD, Davis JM III, Davis MD, Matteson EL. Bullous skin
lesions following infliximab infusion in a patient with rheumatoid arthritis. Arthritis Rheum 2002; 46: 2257–8; author reply
2259.
3 Vergara G, Silvestre JF, Betlloch I et al. Cutaneous drug eruption to
infliximab: report of 4 cases with an interface dermatitis pattern.
Arch Dermatol 2002; 138: 1258–9.
4 Wang LC, Medenica MM, Shea CR, Busbey S. Infliximab-induced
eczematid-like purpura of Doucas and Kapetenakis. J Am Acad
Dermatol 2003; 49: 157–8.
5 Gottlieb AB. Infliximab for psoriasis. J Am Acad Dermatol 2003; 49:
S112–17.
6 Kiely PD, Johnson DM. Infliximab and leflunomide combination
therapy in rheumatoid arthritis: an open-label study. Rheumatology
(Oxford) 2002; 41: 631–7.
7 Wright RC. Atopic dermatitis-like eruption precipitated by infliximab. J Am Acad Dermatol 2003; 49: 160–1.
1273
Endothelin-1 could be one of the targets of psoriasis
therapy
DOI: 10.1111/j.1365-2133.2004.06277.x
SIR, All current treatments for psoriasis have limitations,
particularly for severely affected patients. The pathogenesis of
this inflammatory skin disorder that may affect about 1–3%
of the world population1 is still under debate. One of the
principal clinical aspects of psoriasis is the hyperproliferation
of keratinocytes in some skin areas via the action of
inflammatory mediators. Controlling this upregulated growth
would be a very attractive therapy even if the causative
agent(s) of the disease cannot be blocked. The active vitamin
D3 analogues tacalcitol, calcipotriol and maxacalcitol are
examples of an effective treatment which addresses keratinocyte hyperproliferation2 without affecting the underlying
cause of the disease.
Keratinocytes can produce cytokines and growth factors,
and some of these can stimulate cell proliferation through an
autocrine loop. Several years ago it was reported by our
group that endothelin (ET)-1 is produced in keratinocytes and
acts through the ETA receptor as an autocrine growth factor
for these cells.3 ETs are a family of three vasoactive peptides,
termed ET-1, ET-2 and ET-3, which induce their biological
actions through at least two major receptor subtypes that
belong to the family of G-protein coupled receptors: a selective
ETA receptor, which binds ET-1 and ET-2 with high affinity
and ET-3 with low affinity, and a nonselective ETB receptor
which binds all ET isopeptides with equal affinity. It has
recently been reported that compounds that antagonize the
action of ET-1 by blocking the ETA receptor may control the
growth of tumour cells in which the ET-1 autocrine loop is
upregulated.4,5 High levels of ET-1 have been found in
psoriatic skin and in the serum of patients with psoriasis.6,7
Inflammatory cytokines such as interleukin-1a increase the
production of ET-1 that in turn may lead to the chronic
stimulation of keratinocyte proliferation. Other growth factors and cytokines can also regulate the homeostasis of
epidermal differentiation and proliferation, but nevertheless
ET-1 seems to play an important role in these processes. To
verify this hypothesis and in an attempt to evaluate possible
new therapies for controlling skin proliferation in psoriasis,
an ET-1 antagonist was administered to primary keratinocytes isolated from psoriatic patients as already reported.8
Briefly, keratinocytes were isolated on a lethally irradiated
feeder layer of 3T3-J2 cells; for serial propagation, cells were
cultivated in a serum-free keratinocyte medium and utilized
for the experiments at the second passage.
Keratinocyte cultures were derived from punch biopsies of
lesional and normal-appearing skin of 11 patients with
psoriasis, and from three nonpsoriatic control individuals
undergoing plastic surgery. All the patients had discontinued
local (steroids and keratolytic compounds) and ⁄ or systemic
(mostly ciclosporin) therapy 1 month before the biopsy.
No difference was seen in the presence and expression level
of ET-1 receptors as measured by a semiquantitative reverse
2004 British Association of Dermatologists, British Journal of Dermatology, 151, 1272–1288
Appendix 10
Thielen AM, Barde C, Saurat JH, Laffitte E. Refractory chronic cutaneous
sarcoidosis responsive to dose escalation of TNF-alpha antagonists. Dermatology
2009;219:59-62.
119
120
Rapid Communication/Hot Topics
Dermatology 2009;219:59–62
DOI: 10.1159/000221005
Received: March 30, 2009
Accepted: April 17, 2009
Published online: May 25, 2009
Refractory Chronic Cutaneous Sarcoidosis
Responsive to Dose Escalation of TNF-Alpha
Antagonists
A.-M. Thielen C. Barde J.-H. Saurat E. Laffitte
Dermatology Department, Hôpitaux Universitaires de Genève, Geneva, Switzerland
Key Words
Sarcoidosis ⴢ Tumor necrosis factor antagonists ⴢ
Infliximab ⴢ Adalimumab ⴢ Dose escalation
Abstract
Cutaneous sarcoidosis may be a chronic disease with important morbidity requiring aggressive therapy. The efficacy of
different anti-tumor necrosis factor (anti-TNF- ) treatments in refractory cutaneous and systemic sarcoidosis has
been reported previously. We report the first patient with
chronic cutaneous sarcoidosis who responded to dose escalation of anti-TNF- agents that have been ineffective at the
standard dosage, illustrating that the optimal dosing regimen has still to be defined for this indication before considering difficult-to-treat patients as nonresponders. Our case
report also illustrates that the fusion protein etanercept,
even used at a high dosage, may be less effective for the
treatment of cutaneous sarcoidosis than the monoclonal antibodies infliximab and adalimumab.
Copyright © 2009 S. Karger AG, Basel
Cutaneous sarcoidosis is a dermatosis characterized
by noncaseating granulomatous infiltration. Standard
therapeutic options include corticoids, antimalarials,
methotrexate (monotherapy or combination) and newer
therapies including pentoxifylline, tetracyclines, isotretinoin, leflunomide, thalidomide, chlorambucil, melatonin, cyclosporine A, allopurinol, laser surgery [1] and
medium-dose UVA1 phototherapy [2]. Nevertheless, cutaneous sarcoidosis is often a refractory chronic disease
and aggressive therapy may be required. The mechanisms underlying the formation, maintenance, and spontaneous resolution of the sarcoid granuloma are not well
understood but there are several pieces of evidence that
tumor necrosis factor (TNF-) plays a crucial role [3].
Several case reports and small series have reported the
efficacy of different anti-TNF- agents in refractory cutaneous and systemic sarcoidosis [4–9]. The optimal dosing regimen has still to be defined for this indication
before considering difficult-to-treat patients as nonresponders when on standard doses. We report the case of
a patient with refractory cutaneous sarcoidosis in whom
anti-TNF agents were ineffective at the standard dosage,
but who responded to dose escalation.
Case Report
Dr. Anne-Marie Thielen, Caroline Barde, Jean-Hilaire Saurat and
Emmanuel Laffitte acted as paid consultants for Wyeth (Enbrel쏐),
Schering-Plough (Remicade쏐) and Abbott (Humira쏐).
© 2009 S. Karger AG, Basel
1018–8665/09/2191–0059$26.00/0
Fax +41 61 306 12 34
E-Mail [email protected]
www.karger.com
Accessible online at:
www.karger.com/drm
A 37-year-old woman was suffering from stage 1 pulmonary
and cutaneous sarcoidosis for 5 years. She developed a maculopapular erythematous plaque on the left cheek extending to the
Dr. Anne-Marie Thielen
Dermatology Department
24, rue Micheli-du-Crest
CH–1211 Genève 14 (Switzerland)
Tel. +41 22 372 94 23, Fax +41 22 372 94 70, E-Mail [email protected]
Fig. 1. Maculopapular erythematous plaque of the left cheek extending to the paranasal canthus.
Fig. 2. Insufficient response after 5 infusions at a standard dosage
Fig. 3. Excellent treatment response with a regression of the ery-
Fig. 4. Excellent evolution 7 months after adalimumab treatment
thema and the infiltration after 7 months of infliximab with a
dose escalation to 7.5 mg/kg every month.
initiation at a dosage of 80 mg every other week.
paranasal canthus (fig. 1), two erythematous nodules on the chin
and the right cheek and multiple nodular lesions on both arms.
The localization on the face was causing important psychological
morbidity. She had previously been treated by topical and systemic steroids, tacrolimus 0.1% ointment (Protopic쏐), methotrexate, chloroquine, thalidomide, and pentoxifylline with poor results. Thus infliximab (Remicade쏐) treatment was initiated (induction therapy by an infusion of 5 mg/kg for a body weight of 85
kg at weeks 0, 2, and 6 followed by a maintenance therapy every
other month for 5 infusions) which revealed insufficient efficacy
(fig. 2), the patient presenting an extension and new lesions at the
fourth infusion although stage 1 pulmonary sarcoidosis regressed
during this therapy. Intralesional infliximab injections were per-
formed in 4 lesions on the arm (6 mg total dose for 4 injections)
with the hypothesis of a better local bioavailability, but this treatment was ineffective. The dosage and the frequency of infliximab
infusions were increased (7.5 mg/kg every month) with an excellent clinical improvement maintained for 7 infusions (fig. 3). The
treatment was interrupted at this moment on the patient’s request.
After 4 months, the lesions relapsed and subcutaneous injections
of etanercept (Enbrel쏐), 50 mg twice weekly, were started for 3
months, without any clinical response. Adalimumab (Humira쏐)
was then introduced at a dosage of 40 mg every other week, combined with UVA1 therapy twice weekly for 3 months (23 sessions;
total dose 595 J/cm2). The clinical response was incomplete after
5 months and adalimumab was then increased to 80 mg every
60
Dermatology 2009;219:59–62
of infliximab (5 mg/kg at weeks 0, 2, and 6 followed by an infusion every other month) – persistence of an inflammatory plaque
surrounded by an infiltrated border.
Thielen/Barde/Saurat/Laffitte
other week. Clinical evolution was excellent with a clear reduction of the existing lesions and the absence of development of new
sites persisting for 7 months under maintenance therapy (fig. 4).
Discussion
TNF- plays a major role in infectious and noninfectious granuloma formation. Its implication has been
studied in various systemic granulomatous diseases such
as tuberculosis, sarcoidosis and Crohn’s disease [3]. In
sarcoidosis, high levels of TNF- are correlated with disease activity and progression [3]. Logically, the efficacy of
TNF- antagonists for the treatment of systemic and cutaneous sarcoidosis has been reported [4–9]. Infliximab
and adalimumab are monoclonal antibodies directed
against TNF- that bind to free and cell surface TNF- ,
while etanercept is a recombinant human TNF receptor
fusion protein that antagonizes the effects of endogenous
TNF- by competitively inhibiting its interaction with
cell surface receptors. Adalimumab and infliximab induce apoptosis of cells presenting the bound form of
TNF- [10], whereas etanercept does not. These data suggest that adalimumab and infliximab have a better ability to disrupt granuloma than etanercept. There are clinical pieces of evidence to support this hypothesis, with a
better activity of adalimumab and infliximab than etanercept in granulomatous disorders such as sarcoidosis
and Crohn’s disease. Moreover, paradoxical development
of noncaseating granuloma has been documented under
anti-TNF agents and more frequently with etanercept,
raising the hypothesis that TNF inhibitors may sometimes leave sufficient cytokine activation to support
granuloma formation [11–14].
Our patient did not respond to standard doses of the
three TNF inhibitors and a high dosage of etanercept, but
she responded to high dosages of infliximab and adalimumab. There are no clear recommendations of anti-TNF
use in cutaneous sarcoidosis. In several studies and reports, infliximab and adalimumab were administered
based upon the conventional dose regimen for psoriasis.
For example, in 54 patients suffering from lupus pernio,
a dose regimen of 5 mg/kg infliximab at weeks 0, 2, and
6 followed by an infusion every other month appeared
superior to systemic corticosteroids with or without additional agents [7]. In contrast to previous reports, our
patient illustrates that the conventional anti-TNF dose
regimen may not be sufficient in some patients with cutaneous sarcoidosis. The first treatment, infliximab, was
administered at a weight-dependent dosage of 5 mg/kg
based upon the conventional dose regimen for psoriasis.
Major clinical effectiveness could nevertheless only be
observed after a notable increase of the dosage to 7.5 mg/
kg every month. We observed the same phenomenon
with adalimumab, which was effective at the double dosage (80 mg every other week) of the conventional one
used for psoriasis patients (40 mg every other week).
This concept of dose escalation with TNF- inhibitors
has been validated in several diseases such as rheumatoid
arthritis, Crohn’s disease or uveitis [15–17] for patients
unresponsive to conventional doses. The optimal dosage,
duration of therapy, and long-term toxicity of TNF antagonists in patients with refractory sarcoidosis are yet to
be determined. To our knowledge, our patient is the first
case report illustrating the effectiveness of dose escalation of anti-TNF drugs for the treatment of refractory cutaneous sarcoidosis.
References
1 Badgwell C, Rosen T: Cutaneous sarcoidosis
therapy updated. J Am Acad Dermatol 2007;
56:69–83.
2 Mahnke N, Medve-Koenigs K, Megahed M,
Neumann NJ: Medium-dose UV-A1 phototherapy. Successful treatment of cutaneous
sarcoidosis. Hautarzt 2003;54:364–366.
3 Sweiss NJ, Curran J, Baughman RP: Sarcoidosis, role of tumor necrosis factor inhibitors
and other biologic agents, past, present, and
future concepts. Clin Dermatol 2007; 25:
341–346.
Refractory Chronic Cutaneous Sarcoidosis
Responsive to Dose Escalation
4 Mallbris L, Ljungberg A, Hedblad MA, et al:
Progressive cutaneous sarcoidosis responding to anti-tumor necrosis factor- therapy.
J Am Acad Dermatol 2003;48:290–293.
5 Callejas-Rubio JL, Ortego-Centeno N, Lopez-Perez L, Benticuaga MN: Treatment of
therapy-resistant sarcoidosis with adalimumab. Clin Rheumatol 2006;25:596–597.
6 Heffernan M, Anadkat MJ: Recalcitrant cutaneous sarcoidosis responding to infliximab. Arch Dermatol 2005;141:910–911.
7 Stagaki E, Mountford WK, Lackland DT,
Judson MA: The treatment of lupus pernio:
the results of 116 treatment courses in 54 patients. Chest 2009;135:468–476.
8 Heffernan MP, Smith DI: Adalimumab for
treatment of cutaneous sarcoidosis. Arch
Dermatol 2006;142:17–19.
9 Philips MA, Lynch J, Azmi FH: Ulcerative
cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol 2005;53:917.
10 Mitoma H, Horiuchi T, Tsukamoto H, et al:
Mechanisms for cytotoxic effects of antitumor necrosis factor agents on transmembrane tumor necrosis factor alpha-expressing cells. Arthritis Rheum 2008; 58:
1248–1257.
Dermatology 2009;219:59–62
61
11 Metyas SK, Tadros RM, Arkfeld DG: Adalimumab-induced noncaseating granuloma
in the bone marrow of a patient being treated
for rheumatoid arthritis. Rheumatol Int
2009;29:437–439.
12 Toussirot E, Pertuiset E, Kantelip B,
Wendling D: Sarcoidosis occurring during
anti-TNF-alpha treatment for inflammatory
rheumatic diseases: report of two cases. Clin
Exp Rheumatol 2008;26:471–475.
62
13 Ishiguro T, Takayanagi N, Kurashima K, et
al: Development of sarcoidosis during etanercept therapy. Intern Med 2008; 47: 1021–
1025.
14 González-López MA, Blanco R, GonzálezVela MC, et al: Development of sarcoidosis
during etanercept therapy. Arthritis Rheum
2006;55:817–820.
15 Kristensen LE, Geborek P, Saxne T: Dose escalation of infliximab therapy in arthritis
patients is related to diagnosis and concomitant methotrexate treatment: observational
results from the South Swedish Arthritis
Treatment Group register. Rheumatology
2009;48:243–245.
Dermatology 2009;219:59–62
16 Lutt JR, Deodhar A: Rheumatoid arthritis:
strategies in the management of patients
showing an inadequate response to TNFalpha antagonists. Drugs 2008;68:591–606.
17 Kaplan GG, Hur C, Korzenik J, Sands BE: Infliximab dose escalation vs initiation of
adalimumab for loss of response in Crohn’s
disease: a cost-effectiveness analysis. Aliment Pharmacol Ther 2007;26:1509–1520.
Thielen/Barde/Saurat/Laffitte
Appendix 11
Laffitte E, Fontao L, Kaya G, Khelifa E, Lubbe J, Saurat J-H. Infliximab for
Netherton syndrome: Sustained clinical improvement correlated with a
reduction of thymic stromal lymphopoietin levels in skin. J Invest Dermatol
2009;129:S22, and presented as a poster in 39th Annual ESDR Meeting, 9-12
September 2009, Budapest, Hungary
125
126
Infliximab for Netherton syndrome: Sustained clinical improvement correlated with a
reduction of thymic stromal lymphopoietin levels in skin
E Laffitte, L Fontao, G Kaya, E Khelifa, J Lubbe, J-H Saurat
Clinic of Dermatology, University Medical Hospital, CH-1211 Geneva, Switzerland
INTRODUCTION
Netherton syndrome (NS) is a skin disease caused by mutations in the gene SPINK5, a gene encoding a protein called protease inhibitor LEKTI
(lymphoepithelial Kazal-type-related inhibitor). Recent experimental data in vitro and in vivo have reported overexpression of TSLP (thymic stromal
lymphopoietin), a cytokine pro-Th2 and pro-inflammatory cytokines such as TNF alpha in the epidermis of patients deficient in protein LEKTI (1).
We report a case of Netherton's syndrome with a cutaneous expression of high TSLP and TNF alpha, who presented a dramatic clinical
improvement with the anti TNF monoclonal antibody infliximab.
OBSERVATION
We report the case of a 25-year old woman with a typical clinical NS, confirmed by the absence of LEKTI expression in the epidermis. She
presented with recurrent severe inflammatory vesiculopustular cutaneous flares, unresponsive to therapy with systemic dapsone, topical steroids,
tacrolimus and pimecrolimus. Thus, we initiated infliximab (monoclonal antibody against TNF-α) infusions at 5mg/kg with an induction therapy
(week 0-2-6), followed by a maintenance therapy every other month. After the second infusion, a dramatic improvement was observed and after
one year of therapy the skin was nearly clear of inflammatory lesion; however the ichtiosis was not improved.
Positive control
Patient
Vesiculopustular eruption with typical ichtiosis circonflex; histology showing a
epidermal superficial neutrophilic infiltrate and a polymorphic dermal infiltrate
Lekti immunostaining showing a complete
deficient epidermis.
Dr S. Fraitag, Necker Hospital, Paris, France
Evolution after one year of infliximab therapy:
nearly complete clinical remission
TSLP expression was assessed by ELISA and quantitative RT-PCR in skin biopsies obtained before and after infliximab therapy from inflammatory
and non inflammatory lesions. ELISA performed on skin protein extracts revealed an elevated TSLP production in inflammatory skin lesion before
and after infliximab therapy. Of note, after one year of anti-TNF, a reduction by 4 of TSLP production was observed both in inflammatory and non
inflammatory skin lesions. Quantitative RT-PCR performed on total RNA isolated from skin biopsies gave similar results for TSLP and reveals a
strong expression of TNF-a in both lesional and non lesional skin that was not modulated by infliximab therapy.
2.5
2008
2009
75
50
25
0
Uninvolved skin
Uninvolved skin 2008
Lesional skin 2008
relative expression of RNA transcipts
TSLP ng/mg skin proteins
100
2
Uninvolved skin 2009
Lesional skin 2009
1.5
1
0.5
0
Lesional skin
IFNg
TSLP expression assessed by ELISA in skin biopsies before (2008) and after (2009) antiTNF
IL10
IL17
IL23
IL6
IL8
TGFb
TNFa
TSLP
Expression of various inflammatory cytokines assessed by quantitative RT-PCR in skin
biopsies before (2008) and after (2009) antiTNF therapy
CONCLUSION
In our observation, high levels of TSLP skin were correlated with inflammatory activity of the disease, which is consistent with recent data (2) and
indicates that this cytokine seems important in NS. Moreover, our data suggest that TNF may play a crucial role in NS and in the inflammatory
cascade driven by TSLP, and that an anti-TNF should be considered as a therapeutic approach for NS.
1-Liu YJ. Thymic stromal lymphopoietin: master switch for allergic inflammation. J Exp Med. 2006;203:269-73.
2- Briot A, Deraison C, Lacroix M, Bonnart C, Robin A, Besson C, Dubus P, Hovnanian A. Kallikrein 5 induces atopic dermatitis-like lesions through PAR2-mediated thymic stromal lymphopoietin expression in Netherton syndrome. J Exp Med
2009;206:1135-47.