Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
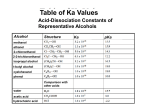
48, 255–263 (1999) Copyright © 1999 by the Society of Toxicology TOXICOLOGICAL SCIENCES Uptake of 10 Polar Organic Solvents during Short-Term Respiration Shinji Kumagai, 1 Hajime Oda, Ichiro Matsunaga, Hiroshi Kosaka, and Susumu Akasaka Department of Occupational Health, Osaka Prefectural Institute of Public Health, 1–3– 69, Nakamichi, Higashinari-ku, Osaka, 537 Japan Received April 1, 1997; accepted August 12, 1998 Respiratory uptake was investigated for 10 polar organic solvents with high blood/air partition coefficients (l blood/air): ethyl acetate (l blood/air, 77), methyl iso-butyl ketone (90), methyl acetate (90), methyl propyl ketone (150), acetone (245), iso-pentyl alcohol (381), iso-propyl alcohol (848), methyl alcohol (2590), ethylene glycol monobutyl ether (EGBE, 7970), and propylene glycol monomethyl ether (PGME, 12380). Test-air concentrations (C inh) were 25 to 200 ppm. Four healthy male volunteers inhaled the test air for 10 min at rest and then room air for 5 min. The percentage of solvent in the end-exhaled air and in the mixed-exhaled air increased after the start of the test-air respiration, and reached a quasi-steady-state level within a few min. The speeds of these increases at the start of the test-air respiration became lower as # ) for the last five min of the l blood/air increased. The mean uptakes (U test air respiration were 67.3, 52.9, 60.4, 53.0, 52.6, 63.0, 60.3, 60.8, 79.7, and 81.3%, respectively, for ethyl acetate, methyl iso-butyl ketone, methyl acetate, methyl propyl ketone, acetone, iso-pentyl alcohol, iso-propyl alcohol, methyl alcohol, EGBE and PGME. # values of the alcohols were higher than those of the Thus, U ketones and lower than the glycol ethers. The overall view, except # increased with l water/air increases. This for esters, showed that U tendency can be explained by a hypothesis that solvent absorbed in the mucus layer of the respiratory tract is removed by the bron# values of ethyl acetate and methyl chial blood circulation. U acetate were higher than those of methyl iso-butyl ketone and methyl propyl ketone, though the l blood/air values of these esters were nearly equal to those of the ketones. For the respiration of the esters, their metabolites, ethyl alcohol and methyl alcohol, were detected in the exhaled air. The exhalation percentage of the metabolites increased after the start of test-air respiration and reached a quasi-steady-state level of 2 and 3%, respectively, by the 5th min. These data suggest that removal of the solvent via metabolism in the wall tissue of the respiratory tract plays an important role for the esters. Key Words: polar organic solvents; blood/air partition coefficient; respiratory metabolism, respiratory uptake. The respiratory uptake (denoted by U) of a chemical is defined as follows: U5 1 Cinh 2 Cmix exh 3 100 ~%! Cinh (1) To whom correspondence should be addressed. Fax: 181– 6 – 6972–2393. where C inh and C mix-exh are the chemical concentrations in inhaled air and in mixed exhaled air, respectively. For nonreactive vaporous chemicals such as organic solvents, U must be related to the blood-air partition coefficient of the chemical (l blood/air), because the chemical is considered to be transferred from air to blood in the alveolar region, according to Henry9s law (Fiserova-Bergerova, 1983). Consequently, U of a chemical with high l blood/air is predicted to be high. However, in a human respiration study, Wigaeus et al. (1981) found that though the l blood/air value of acetone is higher than 200, U is around 45%. Åstrand (1983) noted that because of the high water-solubility, acetone is partly absorbed in the mucus layer during inhalation and is released from the layer during exhalation, so that the U is low. This phenomenon is called “washin/wash-out behavior.” Johanson (1991) proposed a model of the respiratory tract, from trachea to terminal bronchioles, considering the wash-in/wash-out behavior of polar solvents. Based on an assumption that l blood/air is the same as the water/air partition coefficient (l water/air), the model predicted that as the blood/air partition coefficient (l blood/air) increased from 10 to 10,000, U decreased from 55 to 35% at rest condition. In human respiration studies of high water-soluble organic solvents, the observed U values at rest condition were reported to be 43, 56 or 57% for acetone (l blood/air, 245) (Landahl and Herrmann, 1950; Sato and Nakajima, 1979; Schrikker et al., 1985; Wigaeus et al., 1981), 47% for n-butyl alcohol (l blood/air, 677) (Åstrand et al., 1976; Kaneko et al., 1994), 64% for ethyl alcohol (l blood/air, 1440) (Kaneko et al., 1994; Landahl and Herrmann, 1950), 58% for methyl alcohol (l blood/air, 2590) (Kaneko et al., 1994; Sedivec et al., 1981), 67% for ethylene glycol monobutyl ether (l blood/air, 7970) (Johanson, 1984; Johanson and Dynesius, 1988), 62% for ethylene glycol monoethyl ether (l blood/air, 22090) (Groeseneken et al., 1986; Johanson and Dynesius, 1988) and 76% for ethylene glycol monomethyl ether (l blood/air, 32840) (Groeseneken et al., 1989; Johanson and Dynesius, 1988). Thus, there was a large discrepancy between the estimated and observed U values for methyl and ethyl alcohols and glycol ethers, so that the washin/wash-out behavior could not completely explain the respiratory behavior of these solvents. Because the observed U values above were obtained under various experimental conditions and by various investigators, these values may not be comparable. In this study, we determined U values for 10 polar 255 256 KUMAGAI ET AL. TABLE 1 Partition Coefficients of Solvents Partition coefficient Solvent l water/air l oil/air l blood/air Ethyl acetate a Methyl iso-butyl ketone b Methyl acetate a Methyl propyl ketone b Acetone b iso-Pentyl alcohol a iso-Propyl alcohol a Methyl alcohol a Ethylene glycol monobutyl ether c Propylene glycol monomethyl ether c 72 79 108 166 395 850 1500 3330 176 926 86 626 86 1010 154 83 77 90 90 150 245 381 848 2590 7050 5450 7970 12280 696 12380 a Kaneko et al. (1994), Sato and Nakajima (1979), c Johanson and Dynesius (1988) b organic solvents under the same experimental conditions. We also observed the time course of chemical concentration in the exhaled air during short-term respiration MATERIALS AND METHODS Subjects. Four healthy male volunteers (among the authors) participated in this study after a full explanation and their written consent. The means (SDs) of age, weight, and height were 46.5 years (3.2), 60.5 kg (13.5), and 167.0 cm (8.8), respectively. Three of the subjects were smokers but avoided smoking from 3 h before the experiment. All subjects avoided alcohol consumption from 15 h before the experiment. After the experiment, hematological tests (blood cell count, hematocrit, hemoglobin), and liver tests (GOT, GPT, g-GTP) were done, and no significant disorder was found in any of the subjects. Chemicals. Respiratory uptakes were investigated for 10 organic solvents: ethyl acetate, methyl iso-butyl ketone, methyl acetate, methyl propyl ketone, acetone, iso-pentyl alcohol, iso-propyl alcohol, methyl alcohol, ethylene glycol monobutyl ether (EGBE), and propylene glycol monomethyl ether (PGME). All of the chemicals were special or first grade, obtained from Wako Pure Chemical Industries, Ltd. (Osaka, Japan). The partition coefficients of these solvents are summarized in Table 1. Experimental conditions and solvent analysis. The schematic diagram of the experimental set-up is shown in Figure 1. It is similar to the apparatus described by Schrikker et al. (1985). During the experiments, the subjects breathed through a mouthpiece with one-way valves. The inlet of this mouthpiece was connected to the test air in a 100-L Tedlart bag or room air. The outlet of the mouthpiece was connected to a 10-L Tedlart bag for collection of the mixed exhaled air. To avoid loss of the exhaled solvent vapor in condensed water, the connecting metal tubes, the mouthpiece and the three-way valves were kept at a constant temperature of 40°C by means of a heating coil. For determination of the solvent concentration in the inhaled and exhaled air, a portion of air in the mouthpiece was continuously transferred to a flame ionization detector (FID of HP5890 Series II, Hewlett Packard, U.S.) through a fused silica capillary (0.53 mm ID) using a suction pump connected to the outlet of the FID. Sampling rate was 7 ml/min. The capillary was kept at 100°C in order to avoid loss of the exhaled solvent vapor in condensed water. The FID temperature was 200°C. The signal level of the FID increased proportionally to the solvent concentration in the mouthpiece at less than 100 ppm, but increased non-linearly at 100 ppm or more. Consequently, the calibration curve prepared for each solvent was used to determine the solvent concentration in the mouthpiece. Test air was prepared by mixing dry air and vapors of given amounts of liquid organic solvent and water in the 100-L Tedlart bag. Solvent concentrations of the test air were 50, 100, and 200 ppm for ethyl acetate, acetone, and iso-propyl alcohol; 25, 50, and 100 ppm for PGME; 25 ppm for iso-pentyl alcohol and EGBE; 50 ppm for methyl iso-butyl ketone; and 100 ppm for methyl acetate, methyl propyl ketone, and methyl alcohol. All of the concentrations were equal to or less than the Occupational Exposure Limits (OELs) recommended by the Japan Society for Occupational Health (1996) and the threshold limit values (TLVs) by the American Conference on Governmental Industrial Hygienists (1995). The relative humidity of the test air was 50% at 20°C. The subjects inhaled the room air for at least 3 min until the concentration of FID-detectable endogenous substances in the exhaled air became stable. Next, they inhaled the test air for 10 min, and finally the room air for 5 min. They sat on a chair at rest during the experiment. The signal level of the FID was recorded as shown in Figure 2. The mixed exhaled air was collected in 10-L Tedlar t bags for 1 min before, as well as during, the 10-min respiration of test air. The bag was exchanged for another every 1 min. After the experiment, the bags were heated to 50°C in order to vaporize the condensed water and solvent, and 1 ml of the mixed exhaled air was injected into a gas chromatograph equipped with an FID (HP5890 Series II,, Hewlett Packard, USA). To analyze the test air under the same conditions, a portion (about 10 L) of the test air was transferred to a 10-L Tedlar t bag and heated to 50°C, then 1 ml was injected into the gas chromatograph. The columns used were a DB-WAX (30 m 3 0.53 mm ID, J & W, USA) for acetone, iso-propyl alcohol, and methyl alcohol, and a DB-1 (30 m 3 0.53 mm ID, J & W, USA) for the other solvents. The oven temperatures were 40°C for methyl acetate and acetone, 50°C for ethyl acetate, iso-propyl alcohol and methyl alcohol, 80°C for PGME and 120°C for methyl iso-butyl ketone, methyl propyl ketone, iso-pentyl alcohol and EGBE. The injector and detector temperatures were 150 and 180°C, respectively. The flow rate of the helium carrier gas was 12 ml/min. Finally, the solvent concentration in the mixed exhaled air (C mix-exh) was calculated by correcting for 14-ml dead space of the mouthpiece. During respiration of iso-pentyl alcohol, the 3 subjects complained of irritation of the throat, despite the fact that the level was only one-fourth of the OEL and the TLV. Consequently, the test was not done for the last subject, and data were obtained from only 3 subjects. Calculations of exhalation percentages in mixed exhaled air. The exhalation percentage of parent solvent to the mixed exhaled air (denoted by E mix) in each minute was defined as C mix-exh/C inh 3 100 (%). U was calculated as FIG. 1. Schematic diagram of the experiment. 257 UPTAKE OF 10 POLAR ORGANIC SOLVENTS the mean of C end-exh/C inh 3 100 during each 20-s period. The mean of E end for the last 5 min of the test-air respiration (denoted by E# end) is calculated. As stated above, metabolites were detected in mixed exhaled air for the respirations of ethyl acetate, methyl acetate, and iso-propyl alcohol. Because the parent solvent concentrations in the end-exhaled air were not determined separately by chromatography, the FID signal of the above metabolites had to be added to that of their parent solvents. Ratios of FID sensitivity (signal level per ppm in our analytical system) of metabolite to parent were 0.6, 0.4, and 0.9, respectively, for ethyl alcohol/ethyl acetate, methyl alcohol/methyl acetate, and acetone/iso-propyl alcohol. Because the E meta values were 2, 3, and 0.9 –3%, respectively, for the respiration of ethyl acetate, methyl acetate, and iso-propyl alcohol, the E end values were overestimated by about 1.2, 1.2, and 0.8 –2.7%, respectively, which can be considered negligible. Accordingly, correction of E end values is not done. Determination of respiratory rate and tidal volume. The respiratory rate was determined from the protocol of the FID signal level (Fig. 2). The total respiratory ventilation volume was determined by subtracting the remaining test-air volume from the prepared volume, and minute ventilation was calculated. Tidal volume was calculated from the respiratory rate and minute ventilation. Statistical analysis. Statistical testing of the mean values of E end and E mix among the three test-air concentrations was performed by analysis of variance. # between two solvents was performed by t-test. Statistical testing of E# end and U Regression analysis of the time course of E end was performed by Newton’s method (Statistica, StatSoft, Inc.). The equations used were E end 5 a(1 2 exp[2bt]) and E end 5 aexp(2bt), respectively, during and after the test-air respiration, where t is the time in minutes. After the E end value estimated by the regression equation reaches 95% of a value, the condition is defined as “quasi-steady-state” in this study. The time courses of E mix and E meta were also analyzed similarly. RESULTS Respiratory Rate and Tidal Volume FIG. 2. FID signal time courses for respiration of methyl alcohol. 100-E mix (%). The means of E mix and U for the last five min of the test-air # ) were also calculated. respiration (denoted by E# mix and U For the respirations of ethyl acetate, methyl acetate, and iso-propyl alcohol, the peaks of ethyl alcohol, methyl alcohol, and acetone, respectively, were detected on the gas chromatograms of the mixed-exhaled-air samples. Because no alcohol peaks were detected in these samples collected before the respiration of the esters, the alcohols were considered to be ester metabolites. Though a peak of endogenous acetone was found on the chromatograms of the mixed-exhaled-air samples collected before the respiration of iso-propyl alcohol, acetone concentration increased after the start of respiration, so the added acetone was considered to be a metabolite of the alcohol. The concentration of metabolite in the mixed exhaled air is denoted by C meta, and the exhalation percentage of metabolite, E meta, is defined as C meta/C inh 3 100 (%) (ppm of metabolite/ppm of parent solvent 3 100). The means of C meta and E meta during # meta and E# meta) were calculated. the last 5 min (denoted by C Calculations of exhalation percentages in end-exhaled air. Parent solvent concentration in the end-exhaled air (denoted by C end-exh) was determined from the experimental protocol as shown in Figure 2. Because the exhaled air includes FID-detectable endogenous substances, the bottom level during the exhalation following inhalation of the test air minus the top level during the exhalation following inhalation of the room air, was considered to be the signal level of C end-exh. Consequently, C end-exh was determined from this signal level for each exhalation, then C end-exh/C inh 3 100 (%) was computed. The exhalation percentage of solvent to the end-exhaled air (denoted by E end) was defined as The mean respiratory rate of each solvent was from 12.1 to 14.0 min –1, except for iso-pentyl alcohol. The value for isopentyl alcohol was 15.3 min –1, which was slightly higher than those for the other solvents, probably due to the throat irritation. The mean tidal volume in each solvent was from 470 to 530 ml, and no significant difference was found among the solvents. Exhalation Percentages of Parent Solvents For acetone and iso-propyl alcohol, no differences were found in either E end or E mix among the three inhaled concentrations. For ethyl acetate and PGME, although there were no differences in E mix among the inhaled concentrations, there were statistically significancant differences in E end in 7 and 3, respectively, out of 45 20-s periods. However, as no statistical significance in E end was found in the other periods, it was not clear whether or not there was a true difference of E end among the inhaled concentrations. Figure 3 shows the time courses of E end and E mix in the 10 solvents. For ethyl acetate, acetone, iso-propyl alcohol, and PGME, the mean values among the three inhaled concentrations were used. For ethyl acetate, which is the solvent with the lowest l blood/air, the E end rose very rapidly at the start of the 258 KUMAGAI ET AL. FIG. 3. Time courses of exhalation percentage in end-exhaled air (E end) and in mixed exhaled air (E mix) for respiration of ten organic solvents. EGBE, ethylene glycol monobutyl ether; PGME, propylene glycol monomethyl ether. 259 UPTAKE OF 10 POLAR ORGANIC SOLVENTS Exhalation of Metabolites Figure 6 shows the time courses of E meta in the respiration of ethyl acetate, methyl acetate, and iso-propyl alcohol. For the respiration of ethyl acetate and methyl acetate, we detected ethyl alcohol and methyl alcohol, respectively, at the 1st min, and the E meta values were 1.1 and 1.3%. Thereafter, the E meta increased to 2 and 3%, respectively, and reached quasi-steadystate levels at the 5th min. For the respiration of ethyl acetate, the C# meta increased linearly to the test-air concentrations, so that the E# meta almost never changed among the 3 respiration levels. For the respiration of iso-propyl alcohol, the peak of endogenous acetone was found on the chromatogram before the respiration of test air, but the concentrations were less than 0.5 ppm. At the 1st min, C meta increased to 1.0, 0.9, and 1.0 ppm, respectively, for the respirations of 50, 100, and 200 ppm. Thereafter, C meta increased to 1.5, 1.6, and 1.8 ppm, respectively, and reached quasi-steady-state at the 5th min, which shows that C meta almost never changed among the 3 respiration levels. These C meta values correspond to E meta of 3.0, 1.6, and 0.9 %, respectively. FIG. 4. b values estimated by regression analysis for time courses of exhalation percentage in end-exhaled air (E end) against the reciprocal of blood/ air partition coefficient. The equations used were E end 5 a(1 2 exp(2bt)) and E end 5 aexp(2bt), respectively, during and after the test-air respiration, where t is time in minutes. F, b for E end during the test-air respiration; E, b for E end after the end of the test-air respiration. test-air respiration, reached a quasi-steady-state level in the second 20-s period, and fell very rapidly at the end of the test-air respiration. The E mix also rose rapidly and reached a quasi-steady-state level in the 2nd min. Conversely, for PGME, which is the solvent with the highest l blood/air, the E end increased slowly during the first five min of the test-air respiration, reached a quasi-steady-state level at the 6th min, and decreased slowly after the end of the test-air respiration. The E mix also increased slowly during the first three min and reached a quasi-steady-state level at the 4th min. Figure 4 shows the estimated b values against 1/l blood/air. Overall view shows that as the l blood/air is higher, the b value becomes lower. # values plotted against Figure 5 shows the E# end, E# mix and U l blood/air. The overall view, except for the esters, shows that E# end values increased with increasing l blood/air from 90 to 150 (p , 0.01), did not change with l blood/air of 150 to 2500, and there# values of the alcohols were after decreased (p , 0.01). The U higher than those of the ketones (p , 0.05 or 0.01) and lower than the glycol ethers (p , 0.01). Thus, the overall view shows # values # values increased with increasing l blood/air. The U that U of ethyl acetate and methyl acetate were higher than those of methyl iso-butyl ketone and methyl propyl ketone (p , 0.05 or p , 0.01), though the l blood/air values of these esters were nearly equal to those of the ketones. DISCUSSION Highly water-soluble solvent is considered to be partly absorbed in the mucus layer lining the wall of the respiratory tract during inhalation and is released from the layer to the exhaled air during exhalation. This leads us to a hypothesis that the observed C end-exh is not in equilibrium with the solvent concentration in arterial blood but is with that in the mucus layer. The present study found that C end-exh reached a quasi-steady-state level within a few min, and that both the speed of increase of C end-exh at the start of test-air respiration and that of decrease at the end of test-air respiration became lower with increasing l water/air or l blood/air. These findings suggest that C end-exh is in equilibrium with the solvent concentration in a small, waterfilled compartment, which is not inconsistent with the above hypothesis. As stated in the introduction section, Johanson’s respiratory tract model, considering the wash-in/wash-out behavior, predicts that the respiratory uptake will decrease from 55 to 35% as l blood/air increases from 10 to 10,000. This study showed that # inas l blood/air increased from 80 to 12,000, the observed U creased from 53 to 81%, except for ethyl acetate and methyl acetate (Figure 5). This discrepancy suggests that the wash-in/ wash-out behavior cannot completely explain the actual respiratory behavior of these solvents. Morris and Cavanagh (1986, 1987), Morris et al. (1986), and Aharonson et al. (1974) found that organic solvents, including acetone, iso-propyl alcohol, and ethyl alcohol, were taken into the body through the nasal wall tissue of animals. Dahl et al. (1991) quantitatively determined nasal uptake amounts of 2,4dimethylpentane, propyl ether, butanone, 1,3-dioxolane, and ethyl alcohol in dogs, and Gerde and Dahl (1991) proposed a 260 KUMAGAI ET AL. # ) of ten organic solvents against the blood/air FIG. 5. Exhalation percentage in end-exhaled air (E# end) and in mixed exhaled air (E# mix) and respiratory uptake (U # . The values were averaged partition coefficient. EGBE, ethylene glycol monobutyl ether; PGME, propylene glycol monomethyl ether; F, E# end; E, E# mix; 1, U during the last 5 min. model describing nasal uptake. The model includes wash-in/ wash-out behavior in the nasal cavity as well as removal of solvent from the nasal wall tissue by the nasal capillary blood circulation, and it can appropriately predict the observed nasal uptake for the solvents with l blood/air of 1 to 3000. Because our examination uses mouth respiration rather than nasal, the solvents cannot be removed in the nasal wall. However, because bronchial capillary blood flows in the wall tissue of the respiratory tract to nourish the ciliated columnar epithelium and supply the mucus and serosal glands (Deffebach et al., 1987), the circulation must play a similar role. Thus, the solvent accumulated in the wall tissue may be removed by the bronchial capillary blood flow, and it is distributed to the whole body. Breitenbucher et al. (1994) and Onorato et al. (1994) reported that dimethyl ether was taken into the bronchial bloodstream of the respiratory tract in human respiration studies. As alcohols and glycol ethers are much more water-soluble and blood-soluble solvents than dimethyl ether, their concentrations in the mucus layer and wall tissue are predicted to be much higher. Consequently, the amount of alcohols and glycol ethers taken into the bronchial circulation may be considerably # values larger. This can explain the result of the observed U being higher with l blood/air. For the respiration of ethyl acetate and methyl acetate, ethyl alcohol and methyl alcohol were found in the mixed exhaled air. We can try to explain the appearance of the alcohols using the following two hypotheses. The first is that the esters were metabolized to the alcohols in the wall tissue of the respiratory tract, then the alcohols diffused to the tissue surface and released in the exhaled air. The second hypothesis is that the esters were transferred to the arterial blood of the alveolar region and metabolized in the body, and the alcohols were released via the alveolar air. However, if all of the esters taken into the body (about 60 L) were metabolized and the metabolites were distributed in the whole body, the ethyl alcohol and methyl alcohol concentrations in blood could not be higher than 0.15 and 0.09 mg/l, respectively, which corresponds to the exhaled air levels of 0.06 ppm and 0.03 ppm, based on the equilibrium between the blood and alveolar air. This denies the second hypothesis. Because the wall tissue of the respiratory tract is the first to be exposed to the solvent vapor in inhaled air, and the tissue volume is small, the solvent concentration must become high. Consequently, if the esters are metabolized in the wall tissue, it would be reasonable that their metabolite concentrations in the tissue are enough high to be detected in the exhaled air. These considerations support the first hypothesis. Morris (1990) and Morris and Cavanagh (1987) found metabolism of organic solvents, including ethyl acetate and iso-propyl alcohol, in the nasal cavity in rat studies. Because our examination used mouth respiration, not nasal respiration, the present finding suggests that the metabolism occurs in the lower respiratory tract tissue in humans. For the respiration of ethyl acetate and methyl acetate at 100 ppm, based on the simple assumptions that the esters equilibrated between the wall tissue and end-exhaled air and that the tissue-air partition coefficient (l tissue/air ) is the same as the l blood/air , the ester concentrations in the wall tissue are estimated to be 3.0 and 4.1 mg/l, respectively. Based on similar assumptions that the alcohols (metabolites of the esters) are equilibrated between the wall tissue and exhaled UPTAKE OF 10 POLAR ORGANIC SOLVENTS 261 FIG. 6. Time courses of metabolite concentrations (C meta) and their percentage in test air concentration (E meta); 25, 50, 100, and 200 are the test air concentrations in ppm. 262 KUMAGAI ET AL. air and that the tissue-air partition coefficient (l tissue/air ) is the same as the l blood/air , ethyl alcohol and methyl alcohol concentrations in the wall tissue are estimated to be 5.4 and 10.2 mg/l, respectively. These values are higher than the above estimated ester concentrations. The alcohols produced in the wall tissue must be taken into the bronchial circulation and distributed to the whole body as well as being are released into the exhaled air. Considering the alcohols taken into the bronchial bloodstream, the total amounts of esters removed by metabolism in the wall tissue are predicted to be very large, though the alcohols released into the exhaled air were only 2 and 3% of the inhaled esters. The present study # values of the esters were higher by 7 to showed that the U 14% than those of methyl iso-butyl ketone and methyl propyl ketone, though the l blood/air values of the esters are # nearly equal to those of the ketones. Such discrepancy in U may be caused by a difference in the metabolic clearance in the wall tissue. In the respirations of iso-propyl alcohol of 50, 100, and 200 ppm, the E meta of acetone were 3.0, 1.6, and 0.9%, respectively. The above-mentioned consideration leads to a hypothesis that iso-propyl alcohol was metabolized in the wall tissue of the lower respiratory tract. The concentrations of iso-propyl alcohol and acetone in the wall tissue are estimated to be 58.7 and 0.9 mg/l, respectively, for respiration at 100 ppm. Comparing the respiration of iso-propyl alcohol with that of the esters shows that the concentration of the parent solvents is much higher, and that of the metabolites is much lower. Consequently, the amount of acetone (metabolite of iso-propyl alcohol) taken into the bronchial bloodstream is predicted to be much smaller. When the inhaled concentration of iso-propyl alcohol increased from 50 to 200 ppm, C meta in ppm hardly changed, which suggests that the metabolism in the wall tissue was saturated. Thus, the metabolic clearance in the wall tissue is considered to be low, so that the metabolism plays only a small role in the respiratory uptake of iso-propyl alcohol. For the other seven solvents, their metabolites were not observed in the exhaled air. But this does not necessarily demonstrate that there is no metabolism of these solvents in the wall tissue. For example, methyl alcohol and glycol ethers are metabolized to acids in the human body. Because vapor pressures of these metabolites are very low, even if the metabolism occurs in the wall tissue, the metabolites cannot be detected in the exhaled air by our analytical system. Determinants of uptake of high water- or blood-soluble solvents are considered to be the wash-in/wash-out behavior of the respiratory tract, the removal by the bronchial and alveolar circulation, and the metabolism in the wall tissue. Though the amount of uptake caused by the first and second functions relate to the water- or blood-solubility of the solvent, metabolic clearance relates to the enzymatic capacity as well as the wateror blood-solubility, resulting in a more complex contribution to respiratory uptake. REFERENCES Aharonson, E. F., Menkes, H., Gurtner, G., Swift, D. L., and Proctor, D. F. (1974). Effect of respiratory airflow rate on removal of soluble vapors by the nose. J. Appl. Physiol. 37, 654 – 657. American Conference of Govermental Industrial Hygienists. (1995). Threshold limit values for chemical substances and physical agents and biological exposure indices for 1995–1996. ACGIH, Cincinnati, OH. Åstrand, I. (1983). Effect of physical exercise on uptake, distribution, and elimination of vapors in man. In Modeling of Inhalation Exposure to Vapors: Uptake, Distribution, and Elimination, Vol. 2 (Fiserova-Bergerova, V., Ed.), pp.107–130. CRC Press, Boca Raton, FL. Åstrand, I., Ovrum, P., Lindqvist, T., Hultengren, M. (1976). Exposure to butyl alcohol: Uptake and distribution in man. Scand. J. Work Environ. Health. 3, 165–175. Breitenbucher, A., Chediak, A. D., and Wanner, A. (1994). Effect of lung volume and intrathoracic pressure on airway mucosal blood flow in man. Respir. Physiol. 96, 249 –258. Dahl, A. R., Snipes, M. B., Gerde, P. (1991). Sites for uptake of inhaled vapors in Beagle dogs. Toxicol. Appl. Pharmacol. 109, 263–275. Deffebach, M. E., Charan, N. B., Lakshminarayan, S., and Butler, J. (1987). The bronchial circulation: Small, but a vital attribute of the lung. Am. Rev. Respir. Dis. 135, 463– 481. Fiserova-Bergerova, V. (1983). Introduction to mathematical model. In Modeling of Inhalation Exposure to Vapors: Uuptake, Distribution, and Elimination, Vol. 1 (Fiserova-Bergerova, V., Ed.), pp. 51–70. CRC Press, Boca Raton, FL. Gerde, P., and Dahl, A. R. (1991). A model for the uptake of inhaled vapors in the nose of the dog during cyclic breathing. Toxicol. Appl. Pharmacol. 109, 276 –288. Groeseneken, D., Veulemans, H., and Masschelein, R. (1986). Respiratory uptake and elimination of ethylene glycol monoethyl ether after experimental human exposure. Br. J. Ind. Med. 43, 544 –549. Groeseneken, D., Veulemans, H., Masschelein, R., and Van Vlem, E. (1989). Experimental human exposure to ethylene glycol monomethyl ether. Int. Arch. Occup. Environ. Health 61, 243–247. Japan Society for Occupational Health (1996). Recommendation of the occupational exposure limits. J. Occup. Health 37, 259 –282. Johanson, G. (1984). Toxicokinetic studies of 2-butoxyethanol. Undersokningsrapport 39 (English abstract). Arbetarskyddsstyrelsen, Stockholm, Sweden. Johanson, G. (1991). Modelling of respiratory exchange of polar solvents. Ann. Occup. Hyg. 35, 323–339. Johanson, G., and Dynesius, B. (1988). Liquid/air partition coefficients of six commonly used glycol ethers. Br. J. Ind. Med. 45, 561–564. Kaneko, T., Wang, P. Y., Sato, A. (1994). Partition coefficients of some acetate esters and alcohols in water, blood, olive oil, and rat tissues. Occup. Environ. Med. 51, 68 –72. Landahl, H. D., and Herrmann, R. G. (1950). Retention of vapors and gases in the human nose and lung. Archs. Ind. Hyg. Occup. Med. 1, 36 – 45. Morris, J. B. (1990). First-pass metabolism of inspired ethyl acetate in the upper respiratory tracts of the F344 rat and Syrian hamster. Toxicol. Appl. Pharmacol. 102, 331–345. Morris, J. B., and Cavanagh, D. G. (1986). Deposition of ethanol and acetone vapors in the upper respiratory tract of the rat. Fundam. Appl. Toxicol. 6, 78 – 88. Morris, J. B., and Cavanagh, D. G. (1987). Metabolism and deposition of propanol and acetone vapors in the upper respiratory tract of the hamster. Fundam. Appl. Toxicol. 9, 34 – 40. Morris, J. B., Clay, R. J., and Cavanagh, D. G. (1986). Species differences in UPTAKE OF 10 POLAR ORGANIC SOLVENTS upper respiratory tract deposition of acetone and ethanol vapors. Fundam. Appl. Toxicol. 7, 671– 680. Onorato, D. J., Demirozu, M. C., Breitenbucher, A., Atkins, N. D., Chediak, A. D., and Wanner, A. (1994). Airway mucosal blood flow in humans. Am. J. Respir. Crit. Care. Med. 149, 1132–1137. Sato, A., and Nakajima, T. (1979). Partition coefficients of some aromatic hydrocarbons and ketones in water, blood and oil. Br. J. Ind. Med. 36, 231–234. 263 Schrikker, A. C. M., de Vries, W. R., Zwart, A., and Luijendijk, S. C. M. (1985). Uptake of highly soluble gases in the epithelium of the conducting airways. Pflugers Arch. 405, 389 –394. Sedivec, V., Mraz, M., and Flek, J. (1981). Biological monitoring of persons exposed to methanol vapors. Int. Archs. Occup. Environ. Health 48, 257– 271. Wigaeus, E., Holm, S., and Åstrand, I. (1981). Exposure to acetone: uptake and elimination in man. Scand. J. Work Environ. Health 7, 84 –94.