Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
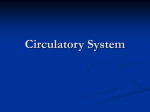
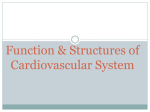
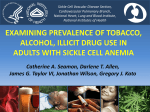
The NHLBI Page Cardiovascular Tissue Engineering Research Support at the National Heart, Lung, and Blood Institute Martha S. Lundberg Abstract: Tissue engineering aims at building 3-dimensional living substitutes that are equal to or better than the damaged tissue to be replaced. The development of such a tissue replacement requires a multidisciplinary approach and careful attention to the optimal cell source, the interactions of growth factors and extracellular milieu, and the scaffolding design. This article is a review of the tissue engineering programs of the National Heart, Lung, and Blood Institute, which support research efforts to translate novel approaches for the treatment of cardiovascular disease. Recent progress is discussed, which highlights some major questions relevant to cardiovascular tissue engineering. The National Heart, Lung, and Blood Institute has a strong interest in tissue engineering and will continue to foster the practical, clinical, and commercial development of research discoveries in this emerging field. (Circ Res. 2013;112:1097-1103.) Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Key Words: biomaterials ■ cardiovascular ■ regenerative medicine O ver the last 40 years, death rates from cardiovascular diseases (CVD) have declined significantly because of advances in medical treatment options and improved healthcare. Americans are living longer, healthier lives with CVD but along with this reality comes additional consequences. For example, the total economic cost of CVD in the United States rose to ≈$298 billion in 20081,2; CVD is becoming a chronic and expensive ailment, which is compounded by an aging population. Our ability to achieve alternative and more cost-effective therapies is an urgent need, especially for the treatment of atherosclerosis, peripheral arterial disease, and congestive heart failure. Recently, improved understanding of cells, tissue properties, and specialized biomaterials has enabled teams of scientists and engineers to create tissue substitutes destined for heart valve repair, reduction of scarring after myocardial infarction, blood vessel replacement, and correction of pediatric heart malformations. Development of novel tissue engineering strategies for heart failure and vascular disease is a research priority for the National Heart, Lung, and Blood Institute ([NHLBI], http://www.nhlbi.nih.gov/about/ strategicplan/documents/StrategicPlan_Plain.pdf). The Multi-Agency for Tissue Engineering Science (MATES) Interagency Working Group defines tissue engineering and science as the use of physical, chemical, biological, and engineering processes to control and direct the aggregate behavior of cells (http://www.tissueengineering. gov/advancing_tissue_science_&_engineering.pdf). At the ■ stem cells ■ tissue engineering core of tissue engineering is the construction of 3-dimensional (3D) tissues using biomaterials. These materials provide overall mechanical support and cell-instructive cues to guide cell growth and tissue construct stability. Tissue engineering, often used synonymously with regenerative medicine, endeavors to combine the use of cells, engineering, and biomaterials to empower the body’s own repair mechanisms to heal damaged tissues or organs. Since Weinberg and Bell3 first described the idea of growing a living blood vessel in 1986, the field of tissue engineering has grown tremendously. For example, healthcare is already being changed by tissue engineering approaches; a search on tissue engineering in ClinicalTrials.gov brings up almost 50 trials, primarily in the eye, bone, cartilage, and dental fields (http://clinicaltrials.gov/). Clinical studies are also beginning to emerge in the cardiovascular, liver, kidney, and endocrine areas. At the National Institutes of Health, a survey of NHLBIspecific projects in tissue engineering was conducted using the electronic research administration system. Overall, this survey showed that NHLBI supports >200 projects in tissue engineering and regenerative medicine, which represents ≈$96.9 million in funding for fiscal year 2012. The NHLBI portfolio is spread over a number of mechanisms, including Small Business Innovation Research (R42, R44) but >50% fall in the R01 category. There is a sizeable training component in the F, K, and T mechanisms. Comparable data can also be obtained using the Original received November 28, 2012; revision received February 4, 2013; accepted March 6, 2013. In February 2013, the average time from submission to first decision for all original research papers submitted to Circulation Research was 11.98 days. The views expressed herein are those of the author and do not reflect those of the NHLBI, NIH, HHS or Federal Government. From the Division of Cardiovascular Sciences (DCVS), National Heart, Lung and Blood Institute (NHLBI), Bethesda, MD. Correspondence to Martha S. Lundberg, PhD, DCVS, NHLBI, Rockledge II, Rm 8210, 6701 Rockledge Dr, Bethesda, MD 20892. E-mail lundberm@ nhlbi.nih.gov © 2013 American Heart Association, Inc. Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.112.300638 1097 1098 Circulation Research April 12, 2013 Nonstandard Abbreviations and Acronyms CVD ECM hESCs MATES NHLBI 3D cardiovascular disease extracellular matrix human embryonic stem cells Multi-Agency for Tissue Engineering Science National Heart, Lung, and Blood Institute 3-dimensional public domain National Institutes of Health Research Portfolio Reporting Tools system (http://www.projectreporter.nih.gov/ reporter.cfm). The purpose of this article is to describe NHLBI– supported cardiovascular tissue engineering research programs, discuss recent advances made possible by federal-wide collaboration through the MATES interagency working group (http:// www.tissueengineering.gov/), and summarize some of the major questions that may impact the future directions of this field. Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Innovative Technologies for Engineering Small Blood Vessels Demand for alternative vascular conduits has been driven by the poor clinical efficacy of existing synthetic grafts for small diameter artery applications in patients who lack adequate saphenous veins. To address this demand, NHLBI released a targeted initiative, Innovative Technologies for Engineering Small Blood Vessels. Four R01 grants were funded for a total of $13.7 million for 5 years in 2006 (http://grants.nih.gov/grants/ guide/rfa-files/rfa-hl-05-013.html). The major objective of this program was to apply a broad range of multidisciplinary approaches to conduct research, and to design, fabricate, and engineer small (<5.0 mm) blood vessel substitutes with improved biocompatibility and durability. The anticipated outcome was to create an environment for establishing optimal conditions (eg, cell types, protocols, animal models, and assessment tools) for vessel replacement therapy in humans. Investigators who were funded under this program have accomplished significant preclinical proof of principle studies in animals, and these novel technologies are being further explored for translation into human use by industry. As of October 2012, this program has stimulated the tissue engineering area by producing 72 publications in peer-reviewed journals, which have been cited >860 times by others (excluding review articles). Enabling Technologies for Tissue Engineering and Regenerative Medicine One ultimate application of tissue engineering is to develop strategies for in vivo regeneration to permanently restore function to compromised tissues in humans but a more near-term application is to develop in vitro disease models for drug testing. However, a critical roadblock is the difficulty in unifying a broad array of disciplines and applying focused tools from developmental and cell biologists, geneticists, clinicians, engineers, materials scientists, and mathematicians to better understand tissue formation. In particular, there is a critical need for multidisciplinary teams to work together to identify the mechanisms of cellular behavior that affect tissue dynamics. In collaboration with the MATES working group, NHLBI cosponsored another program, Enabling Technologies for Tissue Engineering and Regenerative Medicine, and solicited for grant applications (http://grants.nih.gov/grants/guide/pafiles/par-06-504.html) in an effort to cross-fertilize the field with other scientific disciplines. In 2007, funding support for 7 R01 multidisciplinary research projects began, and our commitment totals $14.1 million. Active support continues through 2014. The overall outcome for this transagency effort was to promote collaborative development of new technologies, tools, methods, and devices that enable the engineering of functional tissues. As of October 2012, the NHLBI-funded investigators supported by this program have published ≈122 articles since 2007 on their findings, often in high-impact journals. New Strategies for Growing 3D Tissues Although the long-term goal of tissue engineering is to enhance in vivo regeneration, a short-term opportunity is to improve our understanding of how cells respond structurally to the features of their environment, and to develop accurate approaches that may guide the creation of 3D engineered cellular aggregates. Consistent with this short-term goal, the NHLBI initiated a new program in 2011 entitled, New Strategies for Growing 3D Tissues (http://grants.nih.gov/grants/guide/rfa-files/RFAHL-11–025.html, and http://grants.nih.gov/grants/guide/rfafiles/RFA-HL-11–026.html). The anticipated outcome for this program is to demonstrate reproducible recapitulation in the laboratory for events, such as differentiation, proliferation, migration, and maturation. This program is jointly funded with the National Institute of Arthritis and Musculoskeletal and Skin Diseases, and the National Institute of Biomedical Imaging and Bioengineering. Total support for 12 projects shared between the 3 institutes is $18.4 million. Of the 12 projects funded, key multidisciplinary research questions being addressed include how cells form a 3D structural response to the dynamic elements of humanized heart (7), lung (3), blood (1), and musculo-skeletal (1) biomatrices, as well as the design of bioreactors that will sustain the growth, development, and vascularization of functional human tissues. Funding support for the R01 projects continues through 2015 and is expected to make significant advancements in this area. NHLBI Support for Federal-wide Efforts in Tissue Engineering Research Parallel to efforts at the NHLBI, a federal-wide strategic plan was developed by the MATES Interagency Working Group regarding tissue science and engineering. Since the term tissue engineering was initially defined in 1988,4 several fundamental questions about how cells work within engineered matrices still remain unsolved. The MATES plan laid out the priorities and implementation steps for Federal Government agencies to focus their activities to have the greatest impact in advancing tissue science and engineering. New innovations that address understanding the cellular response, formulating biomaterial scaffolds and the tissue matrix environment, and developing enabling tools are recognized needs to launch tissue engineering applications into an increasingly sophisticated medical marketplace. An explosion of interest and research in tissue engineering has occurred during the last 10 years, and the NHLBI has Lundberg Cardiovascular Tissue Engineering Support at NHLBI 1099 played a critical role in accelerating our understanding of the field. First generation tissue-engineered products have been designed as simplified model systems to answer fundamental cell biology and engineering questions needed for moving to the next level of functional organ complexity. Additionally, stem cell research has contributed much toward the scientific underpinnings of cell biology and engineering, as well as providing reliable, robust sources of characterized cells. Many near-term challenges and opportunities for integrating current knowledge and best practices are now being sought, so that gap areas can be rapidly identified and addressed. Recent examples of where the NHLBI has funded the growth of federal-wide strategic research areas, as described in the MATES plan, are provided in 3 broadly defined categories below. Understanding the Cellular Response Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 An important challenge for the field of tissue engineering and science is to model the normal process by which cells self-assemble into tissues and then organs; in general, the cell is considered the central functional unit within a given organ system. Cells receive messages from physical, chemical, and electric sources, each of which begins a cascade of internal cellular events that ultimately determines phenotypic change. Cells also share information by releasing molecular signals that regulate their own behavior and that of nearby or even distant cells. In the cardiac regeneration field, the biological complexity of the tissue has driven researchers to focus efforts toward that of in vivo repair as opposed to replacement. Animal studies are in progress to understand the ability of human embryonic stem cells (hESCs)–derived cardiomyocytes to repair injured hearts. Shiba et al5 used a guinea-pig model to show that transplanted heart cells, grown from human stem cells and delivered with a prosurvival cocktail of Matrigel, insulin-like growth factor-1, and multiple cell death pathway inhibitors, electrically couple and beat in sync with the own muscle of the heart. More surprising is that with transplantation of the cells, the overall incidence of arrhythmia was lower, an effect that may be clinically useful if shown successful in larger animals (Figure 1). Furthermore, matrices that promote differentiation and proliferation of stem cells for use in tissue engineering are of great interest. For example, hESCs have been used to promote neovascularization and myogenesis in the areas damaged by a heart attack; however, because of minimal cell-based retention, more suitable biomatrices are needed to improve survival and integration of cells transplanted into the host tissue. Duan et al6, funded under PAR-06-504, aim to further our understanding of hESCs in a 3D environment to determine whether native cardiac extracellular matrix (ECM) hydrogels can drive differentiation of hESCs into cardiac lineages, and whether the use of cardiac ECM hydrogels can alleviate the need for supplemental growth factors. The authors show that hydrogel with a high ECM content (75% EM, 25% collagen) increased the fraction of hESCs expressing cardiac marker troponin T, improved mature striation patterns, and improved overall contractile function. These results serve as the basis for future studies of the mechanisms by which the native ECM hydrogel regulates cardiomyocyte phenotype and the use of the native ECM hydrogel as a cell delivery vehicle for heart repair. Formulating Biomaterial Scaffolds and the Tissue Matrix Environment Because of advancements in materials science, there are a wide variety of synthetic and natural polymers that may be used for tissue scaffolds. Increasingly, materials are being selected based on the properties for a particular application. Scaffold porosity and matrix stiffness are both important considerations for structural integrity, cellular infiltration, and final maturation of the construct. Following up on studies that demonstrated the clinical feasibility of engineered vascular grafts in humans, Hibino et al7 developed a tissue-engineered vascular graft composed of a biodegradable, polyglycolic acid scaffold with autologous bonemarrow–derived mononuclear cells. The authors demonstrated in mice that bone marrow is not a significant source of endothelial or smooth muscle cells in the formation of neovessels, and further, that the adjacent vessel wall is the principal source of cells, making up 93% of the proximal neotissue. The authors conclude that in this setting, the tissue-engineered construct functions by mobilizing the innate healing capabilities of the body to regenerate neotissue from preexisting committed tissue cells. This technology is currently in clinical trial to evaluate the safety and growth potential in children undergoing surgery for congenital heart disease. A major limitation for use of tissue-engineered vascular grafts is that it often requires months-long processing to culture a functional and mechanically robust arterial prosthesis that are suitable for repair. Recently although, Quint et al8 funded under RFA-HL-05-013 showed that 1 mm decellularized human tissue–engineered vessels can be used as a biological graft that resists both clotting and intimal hyperplasia. Their results demonstrated that engineered vessels can be grown from banked cells, rendered acellular, and then be used for tissue regeneration in vivo. Even more remarkable was that the decellularized human tissue–engineered vessels were found to have recruited endogenous cells that included a confluent endothelium and coaxial subendothelial smooth muscle cells (Figure 2). Their results offer an inventive solution to the widespread scarcity of vessels available for revascularization procedures. Moreover, they show that engineered vessels can feasibly be produced offline, not requiring cells from the actual recipient, and thereby reducing the waiting time for the production of the vascular substitute. There are ≈80 000 heart valve replacements or repairs performed in the United States each year, however, mechanical or bioprosthetic devices for heart valve disease are associated with significant drawbacks, such as the fact that they cannot grow, remodel, or repair in vivo. The field of tissue engineering has emerged as an exciting alternative in the search for improved heart valve replacement structures, especially for those individuals who cannot receive conventional therapy. For example, studies by Tseng et al9 are exploring the fabrication of trilayer hydrogel quasilaminates. This novel approach looks at the challenge of layer-specific valve mechanical properties for the purpose of tailoring matrix-specific formulas for cell encapsulation. In another study, Tedder et al10 describe the development of 2 novel types of acellular collagen scaffolds, one scaffold was designed to mimic natural valve fibrous layers, and the other scaffold was developed to mimic the delicate and 1100 Circulation Research April 12, 2013 Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Figure 1. Transplanted human embryonic stem cells–cardiomyocyte (hESC–CMs) partially remuscularize injured guinea-pig hearts, preserve mechanical function, and reduce arrhythmia susceptibility. To determine the arrhythmic potential of hESC–CM transplantation in an infarct model, guinea pigs were implanted with a telemetric ECG transmitter and subjected to cardiac cryoinjury. Ten days after cryoinjury, animals underwent a repeat thoracotomy and intracardiac injection of either hESC–CMs in pro-survival cocktail (PSC), non-CMs in PSC, or PSC vehicle only. End points included echocardiography, telemetric monitoring of spontaneous arrhythmias, and induced arrhythmias by programmed electric stimulation (PES) (performed on day +28 post-transplantation). A, Twenty-eight-day-old hESC–CM grafts in a cryoinjured heart stained with picrosirius red, and anti–β-myosin heavy chain (βMHC, red, higher magnification shown) plus human-specific in situ probe (HumCent, brown). Second row, confocal image of host–graft contact, dual-labeled for HumCent (white) and βMHC (red). Third row, destained and then immunostained for βMHC (red) and either connexin 43 (C×43) or cadherin (green). Fourth row, C×43 and cadherin shared between graft and host myocytes. B, Fractional shortening (FS) by echocardiography in uninjured and injured animals receiving hESC–CMs in PSC, non-CMs in PSC, or PSC vehicle only at 2 days before and 28 days after transplantation. C, Representative telemetric ECG traces showing episodes of spontaneous nonsustained and sustained ventricular tachycardia (VT). D, Percentage of animals by group that showed spontaneous VT during monitoring from days 3 to 28 after transplantation. E, Frequency of spontaneous VT by group. F, Representative ECG (red) and stimulation (blue) traces from a cryoinjured non-CM recipient induced to sustained VT by PES. G, Percentage of animals by group that showed induced VT by PES. All data are presented as mean±SEM; n≥13 per group. *P<0.05; **P<0.01. †P<0.05 vs day −2. Reprinted from Shiba et al5 with permission from Macmillan Publishers, Ltd. highly hydrated spongiosa layer. Human bone marrow stem cells were seeded onto both scaffolds. Trilayered constructs were created using a cell-seeded spongiosa scaffold sandwiched between 2 fibrous scaffolds using a protein-based glue and then placed into anatomically analogous 3D heart valve shapes. The valves were conditioned in bioreactors to induce cellular differentiation, and cell viability was assessed after 8 days. To evaluate biocompatibility, the structures were implanted subdermally in juvenile rats and showed good integration after 5 weeks.10 These examples are foundational toward the development of new approaches to reduce the burdens associated with conventional, mechanical, and bioprosthetic (animal or human) heart valve replacement therapies. Developing Enabling Tools Tissue development is the result of molecular and supramolecular interactions, and great progress has been made toward that understanding; yet additional research is needed to improve our appreciation between living and nonliving components of engineered tissues. Reliable protocols and tests, as well as improved real-time imaging, are required for collecting data that are comparable, and to inform predictive models for assessing the state of engineered tissues. Currently, studies of engineered tissues often are conducted by implantation of the construct into an animal; however, this approach can be inefficient because of inadequate vascularization. Vascularization is a limiting factor because of Lundberg Cardiovascular Tissue Engineering Support at NHLBI 1101 Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Figure 2. Explant immunohistochemistry of decellularized human tissue–engineered vessel at 6 weeks. Stained with (A) hematoxylin and eosin stain (H&E; red and blue), (B) smooth muscle α-actin (brown), (C) von Willebrand Factor (brown), and (D) elastin Van Gieson (black stain near lumen). By H&E (A), explanted grafts were negative for evidence of graft dilation, with relatively uniform graft wall architecture. Although there was no significant dilation within each segment of the explanted vessels, only one time point at 6 weeks was obtained for histology. The decellularized human tissue–engineered graft exhibited host cell infiltration on the luminal and abluminal side of the matrix. Host cells did not completely infiltrate through the entire wall of the graft by 6 weeks, and there was a remaining acellular matrix. The neotissue investing and adjacent to the grafts was characterized by immunohistochemistry for smooth muscle and endothelial cell markers. The cells on the outer side of the engineered vessels were predominately positive for smooth muscle α-actin (B), indicating a smooth muscle or myofibroblast phenotype. The neointima also had a thin layer of smooth muscle cells. The luminal surface displayed a confluent lining of endothelial cells on all samples, which were positive for von Willebrand factor (C). Because the decellularized graft was acellular at the time of implantation, the endothelial cells were host derived. The endothelialized neointima likely aided in preventing graft thrombosis and was thin and did not cause narrowing of the lumen. The decellularized human tissue–engineered vessels provided a matrix that supported the host cellular infiltration and stimulated a functional neointima. Elastin formation within the neointima was shown on elastic van Gieson staining (D). Scale bar, 100 µm. Reproduced from Quint et al8 with permission of MOSBY, Inc and Elsevier. the role of oxygen and nutrient diffusion limitations within bulk engineered tissues, which underlies the importance of preformed vasculature. In engineered tissues with preformed vascular networks, this is attributable to the inability of preassembled vascular networks to connect with the host’s microcirculation. To overcome this limitation, Kang et al11 has developed a technology for generating vascularized tissue–engineered constructs. In this study, the authors designed a transplantation model in immunodeficient mice, which consisted of human endothelial colony forming cells and mesenchymal progenitor cells in Matrigel. The cellcontaining Matrigel implants were harvested for microvessel density analysis or transplanted into secondary mice at day 7. In vivo labeling of human-specific cells with fluorescently conjugated lectins allowed for the visualization of functional connections between bioengineered and host vessels. Importantly, their results show that prebuilt perfused human vessels are transplantable from one in vivo site to another (Figure 3).11 Kang’s work extends the range of applications of cell-based technology for transplantable tissue–engineered constructs. NHLBI looks forward to the expansion of this field using new approaches for scaffold design. One advantage of studying cell behavior at the microscale level is to identify mechanisms of in vivo multicellular migration.12,13 Hydrogels represent a mostly biocompatible class of materials that are capable of mimicking the basic, 3D properties of native tissues. Their properties can be tailored to enable precise control of surface features to study cell behavior mechanisms in vitro. For example, Du et al14 developed a clever method using hydrophilic microgels (20% [wt/wt] poly(ethylene glycol)-diacrylate) mixed with a photo-initiator and applied to a glass slide as a way to study cells discretely. Specifically, a drop of photocrosslinkable polyethylene glycol diacrylate prepolymer was pipetted onto a glass slide. A cover glass slide was applied on top of the solution drop, which formed an evenly distributed film of prepolymer solution. A photomask was put on top of the cover slide, and microgels were formed by exposing the prepolymer solution to ultraviolet Table. Some Major Questions in Cardiovascular Tissue Engineering Domain Question Soft tissues What is the best way to establish a blood supply to a tissueengineered construct, such as a cardiac patch? Cells How do very few hESC–CMs surviving in the heart affect ventricular arrhythmia? Are patient-specific (autologous) approaches best, or can we address issues with allogenic donors? Imaging What approaches and methods are best to assess viability and function of an engineered tissue in vivo? hESC–CM indicates human embryonic stem cells–cardiomyocytes. 1102 Circulation Research April 12, 2013 Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Figure 3. Microvessel density analysis before and after transplantation of Matrigel implants containing 2×106 cells at a ratio of 2 endothelial colony forming cells: 3 mesenchymal progenitor cells. Matrigel implants were harvested at multiple time points before and after transplantation. A, Diagram of transplantation model. B–E, Perfused human and murine vessels were identified by tail-vein injection of a mixture of rhodamine (red)–conjugated ulex europaeus agglutinin-I and fluorescein isothiocyanate (FITC; green)–conjugated GS-IB4. B, Representative confocal images of 3 distinct patterns of lectin-labeled vessels in the implants at pretransplantation day 7. White arrowheads indicate human, murine, and chimeric vessels. C, Representative confocal images of lectin-labeled vessels in the implants at multiple time points. White dotted line in the day 3 panel of pretransplantation indicates the border of implant. D, Graph of microvessel density before and after transplantation (n=3–8; mean±SEM). *Significant difference (P≤0.05) between groups for total MVD. †Significant difference (P≤0.05) between groups for human MVD. E, Representative confocal images of green fluorescent protein (GFP)/ UEA-I (rhodamine)–positive vessels in the implants at day 7 after transplantation into GFP-transgenic mice. White dotted line indicates the border of implant. Scale bars represent 100 μm. Reproduced from Kang et al11 with permission of the American Society of Hematology. light through the photomask. The glass slide of prefabricated array of microgels was immersed in mineral oil, and the microgels were assembled into tubular structures by swiping a needle underneath them. The assembly was subsequently stabilized by a secondary crosslinking step. By varying the internal designs of each individual microgel, the sequential assembly allowed for the creation of vascular-like microchannels with a circular lumen and was interconnected in a network to model the bifurcating structure of native vasculature. This simple yet elegant design may be used as a powerful research tool for building biomimetic tissue models, such as for studying cardiac progenitor cells differentiated to mimic native muscle fibers. Future Directions The use of tissue engineering approaches for the treatment of CVD holds significant promise for new therapeutic approaches, especially given the growth of nanoscale approaches for biomaterial design. Further exploration of stem cell technologies, particularly the use of cells differentiated from hESCs and induced pluripotent stem cells, and the creation of a suitable microenvironment for long-term tissue formation are directions likely to advance our understanding of how tissues repair and regrow. These advancements should lead to improved options for arterial revascularization, heart valve repair, arrhythmias, and congenital malformations in pediatric populations. Lundberg Cardiovascular Tissue Engineering Support at NHLBI 1103 Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 However, the practicality of implementing clinicallyviable tissue–engineered constructs on a day-to-day level will require answers to some of the major questions and provocative issues facing this field (Table). Some of these concerns are hampered by research gaps, which include: (1) validated biomarkers to identify the intracellular machinery that guides cells to become functional tissues; they are also required to assess the immunologic requirements and fate of engineered tissues over time; (2) quantitative biological assays to improve the assessment of tissue-engineered construct safety, function, and stability that assist the development pathway and regulatory acceptance of these products; and (3) computationally efficient methods and models, to link gene and protein dynamics to cellular phenotypic outcomes. Additional constraints are universal standards and protocols for longterm storage of cells and tissue constructs, and standardized clinical and preclinical approaches consistent with regulatory requirements. Perhaps the greatest roadblock to therapeutic application is how to combine the vast number of parameters that influence 3D biological responses to produce the necessary outcome. In terms of NHLBI support for tissue engineering research, the RFA-HL-11–025, New Strategies for Growing 3D Tissues program has 3 more years to run. It is hoped that this program, together with other Agency efforts, will provide a robust scientific underpinning to aid tissue engineering approaches for heart, lung, and blood diseases. Leveraging both nano- and microsystem technologies will lead to innovations for the treatment of disease in vivo and may serve as a conduit to spur corporate growth activity in this area. For example, microsystems could be useful for the identification of regeneration-inducing ligand systems to treat chronic inflammation and ischemia or potentially enable the monitoring of real-time angiogenesis. Strategies that improve nondestructive assessment tools for regenerative medicine remain an important goal (http://www.nist.gov/mml/bbd/biomaterials/functional_imaging_regenerative_medicine_workshop.cfm). It is anticipated that these efforts will be highly interactive with discovery science and clinical research and thereby, provide design blueprints for realistic expectations and marketplace needs for tissue-based tools and approaches. Summary Considerable progress has been made in the field of tissue engineering, however the search for the best technologies to create functional cardiovascular tissues are still being investigated. The targeted research programs of the NHLBI are aimed toward improving the understanding of the physical, electric, and chemical factors that affect 3D cellular structures and transferring that knowledge into the testing and translation of novel CVD treatments. As a medical treatment concept, tissue engineering aims to control cell phenotype and direct tissue formation that is functionally equal to or better than the tissue to be replaced. The development of such a tissue replacement will require careful attention to the cell/growth factor/matrix interactions, optimal cell sources, and the design of biomimetic scaffolds. The NHLBI has a strong interest in tissue engineering and will continue to foster the practical, clinical, and commercial development of research discoveries in this emerging field. Future steps will be taken to identify opportunities for leveraging between the research priorities of the NHLBI and other Federal initiatives. Additional information regarding the research funded at the NHLBI can be found at www.nhlbi.nih.gov and by using the National Institutes of Health Research Portfolio Reporting Tools available at: http://www.projectreporter.nih.gov/reporter.cfm. Acknowledgments We thank Michael Laflamme for contributing to Figure 1, Laura Niklason for contributing to Figure 2, and Joyce Bischoff for contributing to Figure 3. Sources of Funding Dr Lundberg is a full-time employee in the Division of Cardiovascular Sciences of the National Heart, Lung, and Blood Institute (NHLBI), and Bioengineering Research Partnership Coordinator for the NHLBI. The NHLBI provided partial monetary support for the figures reused in this publication. Disclosures None. References 1.National Heart, Lung, and Blood Institute. Morbidity and Mortality: 2012 Chart Book on Cardiovascular, Lung, and Blood Diseases. Bethesda, MD: National Institutes of Health, National Heart, Lung, and Blood Institute, U.S. Department of Health and Human Services; 2012. 2. Roger VL, Go AS, Lloyd-Jones DM, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2012 update: a report from the American Heart Association. Circulation. 2012;125:e2–e220. 3. Weinberg CB, Bell E. A blood vessel model constructed from collagen and cultured vascular cells. Science. 1986;231:397–400. 4. Skalak R, Fox CF. Tissue engineering. In: Alan R. Liss, ed. Proceedings of a workshop held at Granlibakken, Lake Tahoe, CA, February 26–29, 1988. UCLA symposia on molecular and Cellular biology: new series #107. 5. Shiba Y, Fernandes S, Zhu WZ, et al. Human ES-cell-derived cardiomyocytes electrically couple and suppress arrhythmias in injured hearts. Nature. 2012;489:322–325. 6. Duan Y, Liu Z, O’Neill J, Wan LQ, Freytes DO, Vunjak-Novakovic G. Hybrid gel composed of native heart matrix and collagen induces cardiac differentiation of human embryonic stem cells without supplemental growth factors. J Cardiovasc Transl Res. 2011;4:605–615. 7. Hibino N, Villalona G, Pietris N, et al. Tissue-engineered vascular grafts form neovessels that arise from regeneration of the adjacent blood vessel. FASEB J. 2011;25:2731–2739. 8. Quint C, Arief M, Muto A, Dardik A, Niklason LE. Allogeneic human tissue-engineered blood vessel. J Vasc Surg. 2012;55:790–798. 9.Tseng H, Cuchiara ML, Durst CA, Cuchiara MP, Lin CJ, West JL, Grande-Allen KJ. Fabrication and mechanical evaluation of anatomically-inspired quasilaminate hydrogel structures with layer-specific formulations. Ann Biomed Eng. 2013;41:398–407. 10. Tedder ME, Simionescu A, Chen J, Liao J, Simionescu DT. Assembly and testing of stem cell-seeded layered collagen constructs for heart valve tissue engineering. Tissue Eng Part A. 2011;17:25–36. 11. Kang KT, Allen P, Bischoff J. Bioengineered human vascular networks transplanted into secondary mice reconnect with the host vasculature and re-establish perfusion. Blood. 2011;118:6718–6721. 12. Rørth P. Whence directionality: guidance mechanisms in solitary and collective cell migration. Dev Cell. 2011;20:9–18. 13. Eyckmans J, Boudou T, Yu X, Chen CS. A hitchhiker’s guide to mechanobiology. Dev Cell. 2011;21:35–47. 14.Du Y, Ghodousi M, Qi H, Haas N, Xiao W, Khademhosseini A. Sequential assembly of cell-laden hydrogel constructs to engineer vascular-like microchannels. Biotechnol Bioeng. 2011;108:1693–1703. Cardiovascular Tissue Engineering Research Support at the National Heart, Lung, and Blood Institute Martha S. Lundberg Downloaded from http://circres.ahajournals.org/ by guest on June 18, 2017 Circ Res. 2013;112:1097-1103 doi: 10.1161/CIRCRESAHA.112.300638 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2013 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/112/8/1097 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/