Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
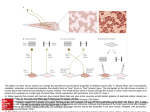
CAPS 423 Gastrointestinal Motility • Dr. Eric Accili • Department of Cellular & Physiological Sciences • University of British Columbia • [email protected] • Life Sciences Building, Rm 2320, (2nd floor west tower) • www.canalionique.wordpress.com Teaching 2016 Password = Fisiology Objectives • Functional Anatomy – GI tract, smooth muscle cells • Smooth Muscle Properties – slow waves, contraction • Innervation of the GI Tract – parasympathetic, sympathetic, enteric – sensory neurons, interneurons, motor neurons • Passage of Food – peristalsis, migrating myoelectric complex • GI Motility Disorders – symptoms "The alimentary canal is a musculo-membrane tube, about 30 ft! in length, extending from the mouth to the anus." Gray's Anatomy. Pennsylvania: Running Press, 1974 30 feet! Anatomy of the GI Tract Structure of the GI Tract Submucosal Plexus Myenteric Plexus GI Smooth Muscle Cells Longitudinal Muscle • • • • • Thin muscle coat Contraction shortens intestine and expands radius Innervated by excitatory motor neurons Few gap junctions to adjacent fibres Ca2+ influx from outside important in excitation-contraction coupling Circular Muscle • • • • • Thick muscle coat Contraction lengthens intestine and shortens radius Innervated by excitatory and inhibitory motor neurons Many gap junctions to adjacent fibres Intracellular Ca2+ release important in excitation-contraction coupling GI Smooth Muscle Cells • • • • ~ 500 M long, 5 to 20 M across Resting membrane potential -40 to -80 mV Circular layer better electrically coupled than longitudinal layer via frequent gap junctions Exhibit slow waves – – – – – – – – oscillating membrane potential triggered by influx of Ca2+ ~3/min in stomach to ~12/min in duodenum generated by interstitial cells located between longitudinal and circular layers of muscularis externa spread through each segment of GI tract amplitude can be modulated by intrinsic and extrinsic nerves and hormones sympathetic decreases and parasympathetic increases amplitude action potentials triggered if threshold reached, enhance contractile force Smooth Muscle Cells • • • • Spontaneously active (myogenic) Stretch induces active tension Myogenic activity modulated by nerves No structured neuromuscular junctions • • • • Not spontaneously active Not activated by stretch Activated by multiple motor neurons Structured neuromuscular junctions Motor Axon Varicosities There are no structured nerve-muscle junctions, transmitter release is diffuse. Action potentials do not trigger release of transmitter from every varicosity Varicosities can migrate along nerve fibres Different Wave Frequencies • Frequency of electrical activity determines the frequency of contractions. -~3/min in the antrum, ~12/min in the duodenum. ~6-10/min in the colon Slow Waves and Contraction 10-20 msec long 1 - 10 per sec • Extent of depolarization and frequency can be altered by hormones and nerves. Slow Waves Without APs • Contractions are small or nonexistent in the absence of action potentials. Slow Waves With APs • Phasic contractions occur when action potentials appear on slow waves. Santiago Ramon y Cajal Physician, Pathologist (1 May 1852 – 17 October 1934) Interstitial Cells of Cajal Martínez et al Nature Reviews Cancer 5, 904-909 (November 2005) Interstitial Cells of Cajal • • • Interstitial cell networks are the pacemakers for intestinal electrical slow waves. Interstitial cells of Cajal are non-neuronal cells of mesenchymal origin. Excitatory and inhibitory neurotransmitters spread diffusely from axonal varicosities to the interstitial cell networks. Gap Junctions Connect Cells • Gap junctions transfer electrical current from cell-to-cell in smooth muscle, generating a functional electrical syncytium. Information Transfer Routes Neurocrine Synaptic transmission, paracrine signalling and hormonal signalling are forms of chemical information transfer in the digestive tract. Regulation of GI Functions • Much of the hormonal and neural regulation is intrinsic to the GI tract. • Some extrinsic regulation, mediated by non resident endocrine cells and neurons. • Overlap allows for subtle and precise control of GI functions. Gastrointestinal Hormones Location of endocrine cells Hormone that produce the hormone Stomach Gastrin Somatostatin Duodenum or jejunum Secretin Cholecystokinin (CCK) Motilin Gastric inhibitory polypeptide (GIP) Somatostatin Pancreatic islets Pancreatic polypeptide Amylin Ileum or colon Glucagon-like peptide-1 (GLP-1) Peptide YY Somatostatin Gut Hormone Communication Routes Enteroendocrine cells are 1-2% of epithelial cell lining. Sense sigals in lumen and release peptide hormone. Innervation of the GI Tract Autonomic Nervous System Parasympathetic Typically stimulates motor and secretory activity. Vagus control to level of transverse colon, remainder from pelvic nerves. Sympathetic Typically inhibits motor and secretory activity, induces contraction of muscularis mucosae and some sphincters. Celiac, Superior and inferior mesenteric Sympathetic input shunts blood away from gut during exercise or stress ~20% CO The Enteric Nervous System • • • • Contains about 108 neurons, ~ same as in spinal cord. Includes motor neurons, sensory receptors, and interneurons. Can coordinate activity in the absence of extrinsic innervation (reflex arcs). Receives extrinsic innervation from sympathetic and parasympathetic. Neuronal cell bodies of the myenteric plexus encricled by sympathetic postganglionic nerves Blue – “auto-fluorescence” of myenteric neuronal cell bodies Green – fluorescence of antibody for tyrosine hydroxylase ‘en passant’ terminals –release neurotransmitter along their length ‘en passant’ terminals release neurotransmitter along their length Enteric nerves of the human myenteric plexus Groups of cell bodies = “Ganglion” Connections of ENS Neurons • • • • • • • • • Control by ENS, modulation by ANS Plexuses consist of ganglia interconnected by tracts of fine unmyelinated nerve fibres Effector neurons to muscle cells, secretory cells, blood vessels Interneurons to integrate sensory input and formulate output Extensive branching in ENS, each axon may innervate many muscle cells Afferent fibres are abundant, carry signals from chemosensitive and mechanosensitive nerve endings Most myenteric neurons are motor, submucosal regulate secretion Multiple neurotransmitters like CNS Excitatory motor neurons release Ach or Sub. P, inhibitory release VIP, NO Integrated Circuits • The brain and the enteric nervous system have integrated circuits. Microcircuits of the ENS • Gut behavior is programmed by the enteric microcircuits. Local and Central Reflexes Intestine and Colon Reflexes • Law of the intestine – a bolus in the intestine causes contraction behind and relaxation ahead. • Intestinointestinal reflex, colonocolonic reflex – over distension of one segment causes intestinal relaxation. • Gastroileal reflex, gastrocolic reflex – elevated stomach secretory and motor function increase ileal and colonic motility. Intrinsic Reflexes Excitatory potentials are mediated by substance P or acetylcholine release from motor neurons Localized mechanical or chemical stimulation of the intestinal mucosa elicits contraction above and relaxation below Inhibitory potentials are mediated by nitric oxide or vasoactive intestinal peptide release from motor neurons Intestine Reflex Pathway • • Sympathetic prevertebral ganglia are pathways for rapid transfer of signals between separated regions of bowel. The transganglionic pathways bypass synaptic delays inherent in the enteric nervous system in signal transfer over long distances. Gastric Reflexes GASTRIC RECEPTIVE RELAXATION NODOSE GANGLION DORSAL INTEGRATIVE MOTOR PATHWAYS NUCLEUS ACCOMMODATION OF PROXIMAL STOMACH NODOSE GANGLION DORSAL INTEGRATIVE MOTOR PATHWAYS NUCLEUS VAGUS VAGUS VAGUS VAGUS MECHANORECEPTOR MECHANORECEPTOR INHIBITORY NEURON FOOD BOLUS ESOPHAGUS CIRCULAR SMOOTH MUSCLE INTERNEURON VIP/NO PROXIMAL STOMACH FOOD BOLUS STOMACH CIRCULAR SMOOTH MUSCLE INHIBITORY NEURON VIP/NO PROXIMAL STOMACH Inhibitory Motor Neurons • • • Activity of a subpopulation of inhibitory motor neurons to the intestinal circular muscle tonically inhibits contraction. Neural blockade or inhibition of NO synthase removes inhibition. Provides added level of control over muscle tone. Inhibitory Motor Neurons • Strength of circular muscle contraction evoked by each slow wave cycle is a function of the number of inhibitory motor neurons in an inactive state. Inhibitory Motor Neurons • Inhibitory innervation of gastrointestinal sphincters is transiently activated for timed opening and passage of luminal contents. Inhibitory Motor Neurons • Inhibitory motor innervation of the intestinal circular muscle is continuously active and is transiently inactivated to permit muscle contraction. Gut Sensory Receptors • Mechanoreceptors – muscle (stretch, tension, length) – mucosal • Chemoreceptors – – – – – acid osmotic amino acid lipid glucose • Thermoreceptors Enterochromaffin Cells • Release of serotonin (5-HT) from enterochromaffin cells is an early step in transduction of sensory information. Enteroendocrine Cells • Enteroendocrine cells are the first step in the transduction of chemoreceptive sensory information. Acid Chemoreceptors • Chemoreceptors for acid in the gastric or duodenal mucosa evoke firing in vagal afferents. Distension Response • Distension of the esphagus evokes firing in vagal afferent fibres. Abdominal Pain • • • Distension is the principal stimulus for pain and discomfort in the digestive tract. Balloon distension in the colon evokes pain in specific regions Most noxious stimuli (burning, cutting, caustic substances) do not evoke painful sensations in the GI tract Irritable Bowel Syndrome • • • Individuals with irritable bowel syndrome have increased sensitivity to balloon distension in the large intestine. A similar phenomenon occurs in the small intestine. Mechanism unclear Chewing (Mastication) • • • • Both voluntary and reflex. Lubricates food with salivary mucus. Amylase breaks down starch. Mechanically chops food into smaller pieces. Swallowing • 1) Oral – • 2) Pharyngeal – – – – – – • voluntary phase, tongue moves food up and back into the pharynx, where it stimulates receptors that initiate a reflex controlled by the swallowing centre in the medulla and lower pons in less than 1 sec, soft palate moves to open a narrow passage to the pharynx. the larynx is moved against the epiglottis to prevent food entering the trachea. the upper esophageal sphincter relaxes. the pharynx contracts to force the bolus deeply into the pharynx. a peristaltic wave is initiated to force the bolus through the UES. During this phase, respiration is inhibited. 3) Esophageal – – – the UES constricts. a primary peristalsis travels at 3 to 5 cm/sec down the entire esophagus in less than 10 sec. secondary peristalsis occurs if food remains. pharynx larynx Pressures During Swallowing Note resting pressure at the sphincters Esophageal Function • A conduit to move food from the pharynx to stomach. • The UES and LES prevent entry of air and gastric contents, respectively. • In the absence of peristalsis the LES remains tightly closed to prevent esophagitis (heartburn). • Failure to relax during swallowing = achalasia. Esophageal Peristalsis Lower Esophageal Sphincter • The lower esophageal sphincter is innervated by both vagal excitatory fibers (VEF) and vagal inhibitory fibers (VIF). Gastric Motility • 1) Allows the stomach to serve as a reservoir. – – – • 2) Breaks food into smaller particles and mixes food with gastric secretions. – – • can accommodate volumes of up to 1.5L without a great increase in intragastric pressure = receptive relaxation. contents may remain unmixed for 1 hr after eating. fats gather at the top and are last to be emptied. contractions are vigorous in the antrum. generates ‘chyme’. 3) empties gastric contents into duodenum at a controlled rate. – – several mechanisms adjust the rate of gastric emptying. liquids are emptied before solid foods. Gastric Emptying Rates Plastic spheres 7 mm Gastric Motility • • Gastric contractions usually start in the middle of the stomach and travel toward the pylorus. They increase in force and velocity as they approach the gastroduodenal junction. – • • • • thus the majority of mixing occurs in the antrum. As the peristaltic wave reaches the pylorus, a small amount of food exits before the pyloric sphincter closes. The rapid contraction of the antrum also propels chyme back = retropulsion. Fed contractions are ~3/min During fasting, quiescence periods of 75-90 min are followed by 5-10 min of strong antrum contractions with a relaxed pylorus. – part of the migrating myoelectric complex. pacemaker zone Gastric Motility • • • • • • Gastric peristaltic waves occur at about the frequency of the gastric slow waves that are generated by the pace-maker zone. They occur at ~3/min and travel towards the pylorus. Smooth muscle contracts when the depolarization during the slow wave exceeds the threshold for contraction. The greater the depolarization the greater the force of contraction. Acetylcholine and gastrin increase the amplitude and duration of contractions, norepinephrine does the opposite. Action potentials notable in antrum and pylorus Gastroduodenal Junction • The pylorus separates the gastric antrum from the duodenal bulb and functions as a sphincter. • The electrical rhythm of the duodenum is 10-12 slow waves per min. • Allows for regulated emptying of gastric contents at rate the duodenum can process the chyme. – too rapid can cause duodenal ulcers. • Prevents regurgitation of duodenal contents to stomach. – can cause gastric ulcers. • Is densely innervated by vagal and sympathetic fibers. – sympathetic fibers increase constriction, vagal may constrict or relax, depending upon the neurotransmitter. • CCK, GIP, and secretin all constrict the pylorus. Regulating Gastric Emptying -Rate at which fat empties doesn’t exceed rate at which it can be emulsified by bile -Acid is not dumped into the duodenum more rapidly than it can be neutralized Vomiting • The oral expulsion of gastric (and sometimes duodenal) contents. • Preceded by retching, in which gastric contents are forced into the esophagus, but do not enter the pharynx. • Reflex behavior coordinated by vomiting centre in medulla oblongata. • Stimulated by distension of stomach and duodenum, tickling back of throat, emetics (e.g. ipecac). • Wave of reverse intestinal peristalsis. • Pyloric sphincter and stomach relax to receive contents. • A forced inspiration occurs against a closed glottis along with contraction of abdominal muscles to elevate intra-abdominal pressure and drive gastric contents into the esophagus. • The LES relaxes, the stomach contracts, the UES relaxes, vomitus enters the mouth. • Closure of the glottis and inhibition of respiration prevent entry into the trachea. Small Intestine Motility • ~5 m in length, takes 2 - 4 hrs for chyme to transverse. • Duodenum, jejunum, ileum, where most digestion and absorption occurs. • Movements mix chyme with digestive secretions, bring chyme into contact with microvilli, propel to colon. • Most frequent movement is segmentation. • Peristalsis is the progressive contraction of circular smooth muscle in an orthograde direction. – timing determined by the slow waves. • Slow waves decline along length, 11-13/min to 8-9/min. – may or may not be accompanied by action potential spikes. – excitability is enhanced by parasympathetic nerves and inhibited by sympathetic nerves. Migrating Myoelectric Complex • The pattern of motility during fasting, stomach to colon. • Bursts of intense electrical and contractile activity separated by longer quiescent periods. • Repeats every 75 to 90 min in humans. – about the time that MMC reaches distal ileum, new one begins. • Sweep the small bowel clean and empty contents to colon. • Inhibits migration of colonic bacteria into the ileum. • Substances released by bacteria may stimulate secretion of NaCl & water by epithelium, causing diarrhea Migrating Myoelectric Complex feeding triggers a switch to a different pattern, with both segmental contractions & peristaltic contractions Muscularis Mucosae Contraction • Contract irregularly at ~3/min. • Alter pattern of ridges and folds of mucosa and mix luminal contents. • Villi also contract irregularly to help empty central lacteals of villi and increase intestinal lymph flow. • Lacteals = intestinal lymphatic that takes up chyle and passes it to they lymph circulation, which passes to the blood Motility of the Colon • Receives 500 to 1500 ml chyme per day. • Most salts and water are absorbed. – feces normally contains only 50 to 100 ml water per day. • The progress of colonic contents is slow (5-10 cm/hr). • Mass movement occurs 1-3 times per day. – differs from peristalsis by prolonged contraction. – push contents within a significant length of colon. • Stimulation of sympathetic nerves stop movements, vagal nerves cause segmental contractions in proximal portion, pelvic nerves control distal colon. Gut Stress Response • Alterations in large intestinal motility and blood flow occur in response to acute stress in humans. Rectum and Defecation • The rectum is typically empty. • Mass movement of the sigmoid colon fills rectum. – causes reflex relaxation of the internal and constriction of the external anal sphincters, urge to defecate. • If defecation is postponed, the urge to defecate subsides. • May voluntarily relax external sphincter. • Descending and sigmoid colon contract. • Intra-abdominal pressure is elevated to aid expulsion of feces. GI Disorders That Impact Motility • Irritable Bowel Syndrome (IBS) – most common GI disorder - 10% to 20% of adults. – abnormal function of the colon – abdominal pain, bloating, constipation and diarrhea • Crohn’s Disease – inflammation of the small intestine – abdominal pain and diarrhea • Celiac Disease – intolerance to gluten (wheat, rye, barley) – immune mediated damage to small intestine – abdominal pain, diarrhea, weight loss, fatigue • Social and economic costs are enormous. • These disorders remain poorly understood and there are few effective treatments. GI Motility Disorders • Gastroesophageal Reflux Disease – ~15% of population – chronic but treatable, lifestyle, medication, surgical procedures • Constipation – infrequent bowel movements (<3/week) – decreased number of propagating contractions (slow transit) • Diarrhea – Frequent loose or watery stools – Excessive number of propagating contractions (rapid transit) • Gastroparesis – stomach takes too long to empty – nausea, vomiting, early feeling of fullness • Achalasia – lack of peristalsis in the esophagus, LES doesn’t relax – difficulty swallowing, chest discomfort, weight loss Hirschsprung's Disease Hirschsprung's Disease • Nerve cells in latter part of the colon are missing (both myenteric and submucous plexi). • Muscles in that region do not relax, hence contractions of muscle that normally push food through that part of the colon do not occur. • Region of intestine above the “aganglionic” region swells resulting in constipation, swollen belly etc. • 1 case per 5400-7200 newborns Hirschsprung's Disease In the absence of the enteric nervous system, how do the muscles of the colon end up contracted? Muscles themselves are naturally more contracted AND/OR Parasympathetic nervous system provides some basal input to contract muscles Enteric nervous system provides resting relaxation. May be due to the absence of a neurotransmitter; e.g. Vasoactive Intestinal Peptide (VIP) • peptide neurotransmitter found in neurons of the colon • when applied to colonic smooth muscle, causes relaxation VIP in the human myenteric plexus Groups of cell bodies = “Ganglion” Hirschsprung's Disease – current therapy • Corrected by surgery – but there can be issues, does not always work well. • Laxatives, high fibre diet to correct constipation Hirschsprung's Disease - research • Gene directed therapy – re-create enteric neurons. • Stem cell therapy – re-create enteric neurons. • Botulinum Toxin (Botox)! – decrease acetylcholine release at the neuromuscular junction, relax muscle in colon. Limited success. Enteric Nervous System of Mouse Normal EDN-3 (endothelin) mutant Enteric nervous system (ENS) phenotypes observed in various mouse mutant strains commonly used as models for Hirschsprung's disease Nature Reviews Neuroscience 8, 466-479, 2007