Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
Chronic
Hemolytic
Agglutinins:
A 20-Year
Gammopathy
With
By Robert
A male,
anemia
Anemia
47, developed
in association
S.
Response
Evans, Elizabeth
chronic
hemolytic
with hi9h titers
of
developed
globulins.
chronic
macroglobulin
serum
titer
of cold
hemolytic
cil with
and
of the
in
complement
of
(C)
Cessation
of
HRONIC
titer
agglutination
agglutinin
agglutinin.
and
Istered
There
since.
a return
has
have
was
ANEMIA
is
been
cyanosis
reason
to
From
the
Veterans
Robert
98108.
Division,
Seattle,
©
Blood,
/0.
Chief
Medical
Service,
of Washington
C. Gilliland,
Department
School
General
of
Medical
M .D.:
Laboratory
studies
tentative
of the
Seattle,
January
Technologist,
Bruce
Hospital,
revised
M.D.:
University
Medical
Wash.
ogy
1 , /972;
S. Evans,
ofMedicine,
B.S.:
Administration
June
his
ab-
and
to
as
cold
a relatively
red cell
mucous
mem-
episodes
of
patients
deof a warm
studies
of a middle-aged
male
with
a 20-yr
history
of sympagglutinin
syndrome
are presented.
The slow
progression
of
be attributed
to both
a gradual
increase
in cold
agglutinin
titer and its thermal
amplitude.
Recent
glutinins
and complement
permit
some
his hemolytic
disease,
though
obscurities
Submitted
a
production
due
skin
of
classify
in which
intravascular
the
been sponsymptoms,
has de-
having
kappa
agglutinin
ac-
acrocyanosis
in
cold
levels.
appearance
immunoglobulin
with
anemia
and
branes.
Hemoglobinuria
from acute
red cell destruction
may follow
chilling
although
this is not a uniform
occurrence.
Finally,
some
velop
a chronic
hemolytic
anemia
that persists
despite
maintenance
environment.
In this report,
toms
of the cold
his disorder
can
remissions
pretreatment
the
of macroglobulinemia
protein
can
produce
was
admin-
hemolytic
macroglobulin
and with
cold
there
normal
benign.
reduced
been
macroglobulin
Despite
monoclonal
light chain
tivity,
and
not
of the
of the
following
the
Chlorambucil
toward
creased.
titer
stasis
occurred
despite
During the past 2 yr there has
taneous
improvement
in his
and the level of macroglobulin
Serum
toward
is a manifestation
in the abnormal
to
cold
discontinued
and
in
chlorambucil
leading
of
anemia
infection,
and exacerbations
and a
HEMOLYTIC
agglutinins
increase
small
cold
hemolytic
h#{216} agglutinins
appeared
macroglobulin.
values
returned
by relapse.
There was a second
to chlorambucil,
but reactivation
respiratory
protein
electrophoresis.
The
agglutinins
was 1 :64,000.
The
anemia responded
to chlorambulevel
normal.
I 966,
anemie
component
a decrease
the
C
hemolytic
M
the
In
and Bruce C. Gilliland
followed
response
agglutinins
in 1 966. His symptpm
of
cold
agglutinin
syndrome
began
in
1 951 with cyanosis
of the extremities
nd
face after exposure
to cold. In 1 956, hemoglobinuna
was first noted after chilling.
In
1 962,
the
cold
agglutinin
titer
was
1 : 1 6,000,
and
his
red
cells were
coated
of Benign
to Chlorambucil
Baxter,
cold
complement
to Cold
History
the
with
Due
1973:
Wash.
of the interaction
of cold
agexplanations
of the course
of
mechanism
remain.’
Response
98018.
accepted
February
Veterans
Administration
of edicine.
Research,
Seattle,
Veterans
Associate
Professor
Medicine.
Universi;y
9. 1973.
Wash.
Hospital.
98108.
Administration
of
of
Medicine
Washington
and
and
Professor
Elizabeth
Baxter,
Hospital,
Seattle.
Director,
School
Immunolof
Medicine,
Wash.
1973
Vol.
by Grune
42.
No.
& Stratton,
3 (September).
Inc.
1973
463
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
464
EVANS.
to administration
of chlorambucil
acerbations
while
occurred
was
he was
observed
receiving
CASE
D.P.,
a 47-yr-old
man,
withexposuretocool
air
red or coffee
colored
and cleared
The
He was
larged,
When
first
seen
urinalyses
The
with
patient’s
red
except
normal,
Fourteen
He was
cord
was
bone
marrow
gamma
He was
was
began
The
6 mg
Fig.
the
next
6 wk,
titer
of cold
42,
but
was
the
titer
patient’s
cells
that
for
lymphoma,
were
was
not
en-
was
and
continued
to
The
antiserums
cells
cells
also
at
50,
with
were
normal.
or
had
margin.
Leukocytes
an
Titration
been
IE
values
had
red
cells.
platelets
3 mo.
were
normal.
increase
band
C showed
was
Hemolysis
cell
M-component
for
hematocrit
plasma
of serum
The
for
present
The
the
or
1:120
laboratory
and
lymphoid
and
normal.
was normal.
costal
of
5’C
of
specificity
electrophoresis
fatigue
of
in
in
the
fast
no CH5O units
anticomplementary.
dose
daily.
reticulocyte
The
counts
stationary
3 mo
were
had
not
decreased
After
red
values
the
chloride.
red
were
demonstrated.
spherocytosis
1:64,000.
2#{176}c.
The
easy
below
evidence
in a single
in acrocyanosis.
for
2 wk
to 2.5#{176},,.
At
the
of cholorambucil
be agglutinated
chlorambucil
titer
of cold
during
and
agglutinins,
the
then
same
ensuing
rose
time,
anti-C
discontinued,
to
there
medication,
by
was
the
serum
and
serum
30
mo
normal
was
are
levels
a gradual
hematocrit
in
high
during
was
dilution.
the
next
/
\
i;
atmosphere
nodes
platelets
(C)
Serum
electrophoresis
serum
reticulocytes
red
no
were
symptomatology
significant
remained
agglutinins.
patient’s
in his
4 cm
was
hematocrit
hematocrit
while
a decrease
and feet
had been
cool
negative
I positive
by
he reported
but
of chlorambucil
I. The
in the
the
The
and
fall
in
lymph
and
not
0,
C levels.
palpable
Serum
agglutinin
were
agglutinated
0.65#{176}cof sodium
in
smears.
cold
values,
in
1966,
there
The
reticulocytes
complement
in serum
hyperplasia,
examinations.
given
was
leukocytes
group
no change
now
l5#{176},and
aspiration
complement
presented
1965,
in March
The
with
were
decrease
later,
region.
history
43#{176}()
and
Serum
37’C
at
normoblastic
on repeated
family
granules
1:16,000
cells.
the spleen
solution
There
There
red
a further
were
was
hemosiderin
and
in hypotonic
of face, hands,
6 yr, his urine
developed
abnormalities.
content.
was
months
pale,
reticulocytes
during
and
washed
for
ex-
palpable.
hematocrit
c,A(C3)(l:S000-l:lO,0O0).
years later, in January
occurred,
29,;
cells
acrocyanosis
The
physical
not
hemoglobin
agglutinins
0, i positive
group
The
health.
notable
were
the
and
of cold
1962 because
of cyanosis
occasions
during
the past
many
chilling.
good
spleen
1962,
were
titer
(C4)and
Three
in
though
therapy.
warming.
without
and
morphology
in
of
occasions,
maintenance
GILLILAND
REPORT
during
On
two
AND
disorders.
male
the liver
1951.
had
blood
a robust
twice
episodes
after
always
other
and
normal
Two
had
and
seen
since
after
completely
patient
anemia,
was
on
BAXTER.
1
.
I00
80
60
t.t.
,
CH,0U,.t.
---
,.-.-1-,,-w
.-.
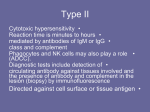
Fig. 1 .
Response
of chronic
hemolytic
anemia
due to cold
agglutinins
to the administration of chlorambucil.
Levels
of
macroglobulin.
cold agglutinin,
20
10
‘
0
6
rAFAyAjtY4s:
3
4
5
6
7
1966
8
9i011i2
12
34
i967
Chi,,.b.,i
5
67234
S
968
6
7
S
910
and serum
hemolytic
complement are depicted
in relation
to hematocnt
and hemoglobin.
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
CHRONIC
6 mo
HEMOLYTIC
there
was
agglutinin
a gradual
titer
had
Chlorambucil
rise in hematocrit.
patient
acute
was
upper
fall
and
ambucil
discontinued
3 mo
later
serum
C.
Since
and
1968,
between
hematocrit
and
red
between
after
were
cells,
and
discontinuing
During
The
past
3 yr.
greater
100 ml:
the
of
due
to
and
and
reinstituted.
7#{176},,
.
During
episodes
an
to
were
normal.
The
rose
levels
than
The
to
gradually
detectable
have
generally
in
which
with
decreased
900
the
respiratory
formation
agglutinin
to
the
developed
weeks
cold
chlor-
35#{176},,
as
of
associated
rather
increased
to
bronchitis
several
were
ensuing
hematocrit
with
of
elevated.
1gM
the
to
in the
Hematocrit
destruction
serum
During
a disappearance
periods
These
remained
cold
with
a
The
fall
hematocrit
in hematocrit
increased
the
counts
The
three
daily.
rapid
infection
l8%-2l,.
have
was
differential
been
8#{176},,
.
The
remission
detectable.
in reticulocytes
there
request.
been
have
counts
the
patient
endurance.
cold
direct
level
1:32,000,
not
there
to 4 mg
of respiratory
a fall
to
titer
mg/l00
varied
ml
6 mo
chlorambucil.
the
and
nosis
to the
reticulocyte
1:16,000
patient’s
has
40#{176},but
and
episode
with
chlorambucil
apparently
since
the
associated
30#{176}c
and
has dropped
infections
at
reduced
1968,
leukocyte
reticulocytes
entered
a second
C again
became
an increase
in February
A second
again
was
to 35#{176},,
and
the
in
measurable.
The patient
and serum
Chlorambucil
and
cleared.
was
March
varied
of
then
l0,,
a rise
not
in the same dose.
titers
decreased,
infection
were
infection
C was again
in hematocrit
tract
to 28#{176},,
and
serum
free ofsymptoms.
a decrease
25#{176}c.
Reticulocytes
was
in hematocrit
increased,
respiratory
respiratory
465
was again
given
Cold
agglutinin
was again
6 mo there
ANEMIA
agglutinin
reports
general
A determination
of
titer
antiglobulin
was
reaction
1:4000,
was
improvement
macroglobulin
the
hematocrit
unchanged.
Since
was
then
in symptoms
with
in December
1970
and
4#{216}0.,
the
less
acrocya-
was
300
reticulocytes
patient
has
mg/
were
refused
6#{176}c.
additional
determination.
MATERIALS
The
method
scribed,
and
of titration
as well
as the
of the
methods
cold
AND
agglutinins
used
METHODS
and
in preparation
the
of
serum
the
complement
antiserums
levels
for
has
been
C globulins,
de-
(fi,)
C4
C3 (lc-,A).2
The
cells
hemolytic
ofa
mixed
with
HCI.
of
red
cells
normal
concentration
cells
residual
anti-C
globulin
was
with
milliliters
Fractions
were also
of
were
tested
phoresis.
The
serum
were
concentration
Buglio
patient’s
washed
red cells
and
patient’s
red
the
agglutination
out
light
in our
For
detection
distilled
water
tration
cells
of
100
of Kabat
The
the
red
addition
was
of 0.1
N
ml of a 20#{176}c
suspension
incubated
for
of
with
were
patient’s
remaining
red
serum
temperature
compared
and
0, 1 positive
patient’s
by the
0.25
and
at
37’C
of the
cells.
on
Sephadex
was
leukocytes
30
with
for
red
cells
to
were
tested
mm
at
incubation,
a control
tested
cells
Dr.
with
of
l00O
agglutination
hemolysis
by cold
for
coating
buffer
at
by
Tris-HCI
1 positive
analysis,
red
and
(Hyland
the
pH
Laboratories).
formation
8.
cells.
Fractions
immunoelectro-
of rosettes
The
with
the
subjects.3
complement-fixing
concentrations
G antibodies.4
Harboe.5
using
diffusion
to demonstrate
the
low
G-200
group
0,
Ouchterlony
by radial
used
of normal
tested
by antigamma
by
with
was determined
et al.
or absence
originally
antibody
of
Typing
Cold
agglutinins
24-hr
urine
gamma
of light
from
G
chains
later
consumption
globulin
test
to
insufficient
of the
bleedings
to
cold
agglutinin
were
typed
for
laboratory.
of Bence
and
then
mg/mI
munoelectrophoresis.
method
was
the
7.2 or 6.8
mixture
at
group
of
of 37’C,
sedimented
times
with
milliliter
to
serum
supernatant
three
fractionated
were
presence
was carried
chains
the
were
susceptibility
of 1gM
by Lo
produce
adjusted
tested
for cold agglutinin
activity
by cellulose
acetate
electrophoresis,
described
The
of
the
red
agglutinin
half
serum.
method
demonstrate
was
cells
in
The
cold
One
to temperature
washed
to normal
anti-C
pH
I .0 ml
blood
were
serum.
compared
C components
to
red
The
The
equilibrated
added
The
ofthe
as follows:
serum.
had been
was
activity
determined
hemoglobin
agglutinin
Two
of
temperature.
hemolysis.
in the
ml
was
all reagents
normal
the
complement-fixing
subject
0.5
After
the desired
and
and
normal
Jones
and
Serum
and
proteinuria,
lyophilized.
Mayer,6
then
The
lyophilized
examined
hemolytic
in which
for
Bence
specimen
urine
Jones
C determinations
normal
values
was
protein
were
ranged
was
from
thoroughly
dissolved
in
by
done
dialyzed
water
at
electrophoresis
by
a modification
80 to 160 CH
U/mI.
against
a concenand
of
imthe
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
466
EVANS.
SI
Cr tagging
patient
and
was
used
to observe
the survival
the
survival
of
ofcomplement-coated
autologous
red cells
and
ofthe
patient
BAXTER.
AND
GILLILAND
homologous
red
cells
in a normal
subject.7
the
in
RESULTS
The
G-200
cold agglutinin
activity
separation.
This
material
was
found
produced
in the first peak
a homogeneous
electrophoresis.
Ouchterlony
analysis
of isolated
repeated
adsorption
and elution
from
red cells
antibody
but not with anti-A.
Bence
Jones
protein
in urine
that had been highly
concentrated.
To
determine
what
per
cent
of the
patient’s
of the Sephadex
spike
on protein
cold
agglutinin
showed
reaction
could
not be
serum
1gM
was
participating
cold agglutinins,
an aliquot
of serum
was absorbed
repeatedly
prepared
from
group
0, I positive
red cells.
The
concentration
measured
by radial
diffusion,
and the cold agglutinin
titer was
lowing
each
absorption.
moval
of cold agglutinin
the patient’s
serum
1gM
Seven
activity.
at this
absorptions
were
Cold
agglutinin
particular
bleeding
using a control
activity,
showed
serum
with 2 g of macroglobulin,
less than 20
nonspecific
absorption
The patient’s
throughout
the
washed
period
hemolysis
by cold
less than
hemolysis
The
red cells
of study.
agglutinins
hemolysis
of normal
red
cells
of the
when
agglutinated
red cells
patient
washed
but
were
compared
of the patient’s
cells under
the
c;
red
were
His
necessary
activity
(Table
prepared
by
with
anti-K
demonstrated
for complete
rerepresented
84
of
1). Repeat
studies
without
cold
of macroglobulin.
agglutinin
by anticomplement
relatively
resistant
to normal
red cells,
as
same conditions.
red
cells.2
compared
at 37#{176}C
formed
as
with
stroma
of 1gM was
determined
fol-
There
to
rcsettes
serums
to C
was
20%-50%
with
monocytes
and polymorphonuclear
leukocytes
from
a normal
donor
when
incubated
at
25#{176}C.The adherence
of red cells to leukocytes
appeared
to be due to C components,
since the amount
of ‘y G globulin
detectable
on the red cell surface
was not increased
above
that found
on normal
red cells.4
Both
polymorphonuclear neutrophils
and mononuclear
cells formed
rosettes
with the complementcoated
red cells ofthe
patient.
Survival
of the patient’s
5’Cr-tagged
red cells in his own circulation
was
served
during
treatment
with chlorambucil.
The t survival
was 1 1 days at
beginning
ofchlorambucil
3 mo
sion
tient’s
later.
circulation
Table
The
was
treatment
survival
t
13 days.
1 . Relation
15 days
group
The
of Serum
No of
Absorptions
and
of normal
initial
1M
Concentration
0,
he was
lmg/100
in partial
I positive
of rapid
to Cold
cells
Agglutinin
Titer
of
Cold Agglutinin
Titer
650
25,600
1
510
12.800
2
390
6.400
3
315
3.200
4
245
1.600
5
120
400
6
118
7
100
milliliters
of se rum were
absorbed
with
stroma
10
0
from
2 ml of red blood
cells.
pa-
of normal
Reciprocal
ml)
remis-
in the
destruction
‘yM
Before
‘Three
phase
when
obthe
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
CHRONIC
cells
tinins
HEMOLYTIC
ANEMIA
467
seen in other
patients
was not observed.’
showed
the first
with
chronic
The patient’s
a biphasic
curve
with
90 mm. The remaining
an
hemolytic
red cells
initial
red cells
period
were
anemia
due to cold
injected
into a normal
of rapid
removed
agglusubject
removal
of 30%
at a gradual
rate
during
with a
of 24 days.
DISCUSSION
The
history
ofcold
ofacrocyanosis
agglutinin
hemolytic
had
anemia.
component
titer
ofcold
agglutinins
in the
serum
protein
duced
complement
coating
red cells were heavily
coated
to C hemolysis
has been
shown
ment
at
through
the
by in vitro
components
onstrated
above
that
process
due
the
action
studies
to repeated
of cold
to be
C3)
that
fixation
1951
at least
on
required
ofC
reactions
had
rather
than
a partial
red
agglutination.2
cells,
in
vitro
were
introduced
own
brane
red cells,
damage
consumed
red cells.
phonuclear
existence
to
the
his
leukocytes
ofsuch
The concept
that
in chronic
hemolytic
has
been
a process
whose
and C4
reported.8’9
of
that
Further
red
cell’s
pro-
resistance
comple-
takes
place
studies
dem-
is a continuing
agglutinin
and
hemolytic
red
noted
the
disease
for
cells
circulation.
as it was
Transfused
cells
no
result
at
furof
released
red
It
was
is reasonable
by a steady
cells, as the
and the acute
the circulation
active.
the absence
of
susceptible
to C
to
deposipatient’s
form
of memdid not occur.’
cells with
the C components
by cold
has been enhanced
by observations
red cells of this patient
subject.
Furthermore,
both
macrophages
and
those
seen
in patients
of receptor
sites for C3
M
serum
resistance
of his circulating
cells
our group
of patients
with
this
total
serum
hemolytic
comple-
when
The significance
of the coating
of red
agglutinin
as a cause
of red cell destruction
similar
existence
cold
acquired
C components
gradually,
that results
in rapid
removal
from
that 30% of51Cr-tagged
circulation
of a normal
formed
rosettes
with
detectable
This abnormal
accumulation
probable
explanation
when
normal
red
into
levels
of chronic
his
hemolytic
anemia,
the patient
This
change
may
have
been
depletion
postulate
that complement
was
tion on the surface
of circulating
until
and
to circulating
the
abnormal
onset
at 37#{176}C.The
patient’s
own
and were
relatively
resistant
for
between
of serum
complement
is the
period
of rapid
destruction
hemolysis
increased
agglutinin.
due to the
depletion
of serum
C, as well as the acquired
to complement
hemolysis.
He is unique
in
syndrome
in having
an absence
of measurable
ment,
that
to the
electrophoresis,
the
globulins
body
temperature.’
Following
the onset
of chronic
ther episodes
of hemoglobinuria.
The lack
an initial
indicates
15 yr prior
of normal
red cells
with C components
(primarily
temperatures
in
present
The
appeared
beginning
been
were removed
it was shown
polymorphonuclear
red cells
on human
Others
rapidly
that
his
from
the
red cells
leukocytes
are coated
monocytes
with
and
IgG.
The
polymor-
have
to
failed
confirm
the
sites.’#{176}
the
C components
on the surface
anemia
due to cold agglutinins
(C4 and C3) has been challenged
by Engelfriet
that a2D
globulin
(C3d),
an enzymatic
cleavage
fragment
that remains
on the red cells in vivo.
of the circulating
are /lE and
red cells
globulins
et al.” They
presented
evidence
product
of C3, is the only
C
Regardless
of the nature
of the
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
468
EVANS.
adherent
complement
fraction
or
fractions,
the
BAXTER.
destruction
chronic
form
of the disease
is usually
accompanied
cytosis,
suggesting
loss of membrane
as a result
phagocytic
cells as is postulated
to occur
with IgG
of
by some
of surface
antibodies.3
of rosettes
by this patient’s
red cells and leukocytes
for biologically
active
C components,
probably
C3b,
culating
red cells.
Chronic
hemolytic
anemia
due to cold agglutinins
AND
red
cells
in the
degree
of spherointeraction
with
The formation
is interpreted
on the surface
is an
GILLILAND
as evidence
of the cir-
uncommon
disorder,
and so far, there
are few descriptions
of treatment
by measures
other
than
maintaining
a warm
environment.
Unlike
hemolytic
anemia
due
to warmreacting
autoantibodies
of the lgG
variety,
hemolytic
anemia
due
to cold
agglutinins
appears
to be resistant
to steroids.
Splenectomy
may
reduce
the
hemolytic
activity
been
established.’2
glutinin
in vitro
these
agents
glutinins
has
favorable
in some
patients,
but
its value
as a general
Penicillamine
and
other
mercaptanes
by splitting
disulfide
bonds
of the 1gM
in the treatment
not been established
response
in two
of
hemolytic
the decade
has
not
agof
anemia
due to cold
since the initial
report
agof
patients.’3”4
Several
reports
attesting
value
with alkylating
agents,
particularly
tration
of these
agents
provement
in anemia
in the marrow.
Olesen
with chlorambucil.’7
chronic
during
measure
inactivate
cold
molecule.
The value
of long-term
chlorambucil,
has caused
a decrease
along
with a decrease
has reported
treatment
The
concentration
of
treatment
have
in the M component
and an imin the number
of lymphoid
cells
of the cold agglutinin
syndrome
M component
was reduced,
and
the titer
of cold
agglutinins
was decreased.
Dacie
satisfactory
improvement
in three
of nine patients
while
three
others
had some
benefit.’8
Our
attempts
two other
patients
were not successful,
prior to any evidence
of improvement
since
in the
of macroglobulinemia
appeared.’5”6
Adminis-
and Worlledge
given
chlorambucil
with
alkylating
have
noted
therapy,
agents
in
bone
marrow
depression
hemolytic
process.
occurred
Administration
of chlorambucil
to the patient
reported
above
was followed
by significant
reduction
in levels
of 1gM and in the titer
of cold
agglutinins.
The hematocrit
rose, and reticulocytes
decreased.
Total
serum
complement
rose
from
undetectable
levels to approximately
50
of normal
during
each
remission.
Reticulocytes
were always
elevated
to 2%-3,
even when
the hematocrit
was within
the range
of normal.
The 51Cr t survival
of 15 days
during
the
partial
remission
was
not returned
ambucil
was
levels.
being
An
further
evidence
to normal.
The
stopped,
as the
exacerbation
administered
of
equal
in February
that
the
rate
of red
hemolytic
anemia
recurred
cold
agglutinin
titer
returned
severity
1968,
following
occurred
while
a respiratory
cell
destruction
had
3 mo after
chlorto pretreatment
chlorambucil
infection
cold agglutinin
titer was at a relatively
low level (1:2000).
Reactivation
hemolytic
anemia
occurred
again
4 mo later
in June
1968,
following
was
when
the
of the
another
respiratory
infection
when
cold agglutinin
titers
were still relatively
low. Such
exacerbations
may
be related
to an increase
in complement
formation
and
activation,
as well as greater
activity
by phagocytic
cells.
Both
factors
are probably
dependent
on the thermal
amplitude
of the cold
agglutinin,
including
complement
deposition
on
red
cells
at
normal
body
temperature.
It is signifi-
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
CHRONIC
HEMOLYTIC
cant that,
complement
despite
the
components
Furthermore,
serums
with
The
ANEMIA
depression
were
of the cold
agglutinin
still bound
to normal
agglutinin
isolated
from
patient
resistance
to hemolysis
to normal
cells.
was
a homogeneous
by
immuno-
1gM with
kappa
light
chains
only.
The M component
observed
acetate
electrophoresis
appears
to have
been
nearly
all cold
since
it disappeared
with
repeated
absorption
of the serum
with
cell stroma
in the cold.
after
removal
of all cold
Measurement
agglutinin
of the patient’s
activity
showed
an
The identity
of the M component
tivity
has been
well documented
been
observed
globulin
with
other
(rheumatoid
While
toms,
tions
the
cold
been
depressed.
tion.
Finally,
the
failure
of our
can
to detect
there
is evidence
that
followed
the
E, Bingham
M:
the
and
1gM.
agglutinin
activity
achas
anti--y
antilipoprotein
patient’s
G
activities.20
M component
led
to symp-
be classed
as benign.
Serum
concentranormal,
and bone
marrow
function
has
Bence
Jones
protein
benign
for the
mechanism
questions
M component
cessation
in a concentrated
evidence
for
responsible
protein
and the homeostatic
at present
but pose important
2 yr that
cold
antibody
on
agred
before
of
including
0, and
has also been
considered
The nature
of the stimulus
ofthe
abnormal
tion are unknown
during
activity
gammopathy
have
remained
The
24-hr urine
sample
malignant
disease2’
with
immunoglobulins,
antistreptolysin
agglutinin
serum
1gM
84
reduction
on electrophoresis
by others.’9
Similarly,
monoclonal
factor),
his monoclonal
of IgG and IgA
not
our
level by chlorambucil,
cells at 31 and 37#{176}C.
red
the patient’s
red cells had
not lost
high titers ofcold
agglutinin
as compared
cold
globulin
cellulose
glutinin,
469
rather
than
production
limiting
its producfor future
investigadecreased
of the cytotoxic
spontaneously
drug.
REFERENCES
I
.
Evans
RS, Turner
hemolytic
The
anemia
role
due
of complement
Evans
anemia
mechanism
ment
due
3.
Lo
cells
coated
and
sphering
by
4. Gilliland
detection
ment-coated
5.
of
in
RS,
J
Jandi
JH:
G:
mononuclear
cells
in
JP, Vaughan
M,
Schubothe
Red
human
Huber
RS:
1961,
Furth,
R,
Exclusive
cold
EA,
occurrence
hemagglutinins.
sensitized
Haematol
19:19,
FS:
of
Scand
II.
&
G,
MM:
2).
Experimental
Springfield,
Ill.,
162
Kr
Motulsky
AG,
Giblett
ER,
The
Br
Linscott
J
WD,
monocytes:
for
the
for
immunoglobulin
third
component
G.
Receptor
sites
complement:
by cold
on
Binding
of
autoantibodies.
Br J
970
N,
Gelfand
EW,
interaction
and
and
red
lgG
Jandl
between
cells.
Specificity
fragments.
J
JH,
human
for
Exp
lgG
Med
1970
CP,
von
dem
haemolytic
use
Pondman
Borne
G,
complement
Immunol
MJ,
SD:
for
The
examination
their
tag.
H uman
Douglas
Misset-Groenveld
and
CA:
cell
1968
Engelfriet
immune
Mayer
DM,
H,
red cells
H,
1965
(ed
sites
and
monocytes
monocytes
subclasses
on compleClin
Invest
Finch
red
HJ :
162:1281,
Rosen
The
V.
a
PolIcy
receptor
132:1207,
Van
H,
Eberhard
complement
Science
man.
JH:
J
2:259,
Donohue
Huber
Clin
Binding
as
10. Abramson
Leddy
Immunochemistry
7.
agglutinins.
Viranuvatti
1:249, 1955
Distinct
of
1967
isolated
Kabat
Thomas,
The
to comple-
cell-bound
antibody
human
red cells.
Evans
J Haematol
6.
cells
1970
K,
chains
cold
Cotran
BC,
Harboe
Lind
M ‘filler-
agglutinins:
of red
immunoglobulin
158:1582,
49:898,
M:
Chronic
G,
chromium
Haematol
9.
AF,
with
Biroli
of
destruction.
1967
Buglio
Science
Pirzio
use
II.
8.
to cold
by
lnvest46:l46l,
cell
E, Bingham
of resistance
hemolysis
agglutinins.
1968
RS, Turner
hemolytic
cold
in red
J Clin Invest 47:691,
2.
to
Chronic
Van
components
in
serological
6:721,
1970
Ill.
specific
Wolters
Beckers
Loghem
anaemias.
of
KW,
AEG,
JJ:
Preparation
antisera
and
studies.
D,
Auto-
against
products,
Clin
and
Exp
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
EVANS.
470
12.
Evans
immune
serological
NY
RS,
and
Sci 124:422,
Ritzmann
mercaptanes
Med
14.
SE,
in
cold
57:718,
therapy
in
Waldenstrom:
Turner
H:
disease
activity.
primary
it)
1963
the
Olesen
WC:
agglutinin
Effect
disease.
of
Dacie
hemolytic
19.
J Lab
cold
1966
cases.
macroglobulinemia.
of
Proc
Staff
to
JA MA
JV,
Worlledge
Christenson
WN,
Dacie
Charlwood
PA:
containing
Identification
of
Qf an abnormal
3:262,
20.
1957
Potter
Med284:831,
21.
Hobbs
malignant?
J
M:
Auto-immune
6:82,
JV,
1969
Croucher
Electrophoretic
high-litre
cause
with
in
Scand
SM:
Hematol
ponents)
Response
treatment
syndrome.
Prog
sera
tinins:
chlorambucil
macroglobulinemia
of four
on
hemagglutinin
GILLILAND
1964
anemias.
BEE,
The
1:116,
AND
Chlorambucil
agglutinin
Haematol
Ann
H:
cold
18.
Levin
Meet Mayo
Clin 36: 135, 1961
16. Clatanoff
DV,
Meyer
00:
183:126,
of
1965
Hematol
3:27,
ED:
Continuous
Report
chlorambucil
17.
E: Auto-
Observations
1961.
Schubothe
disease.
Semin
15. Bayrd
M,
disease:
reactions
Acad
13.
Clin
Bingham
hemolytic
BAXTER.
the
Myeloma
haemagglu-
antibody
peak.
antibody-like
studies
cold
Br
proteins
activity.
as
the
J Haematol
(M-comN
EngI
J
1971
JR:
Br Med
Paraproteins,
J 3:699,
1967
benign
or
From www.bloodjournal.org by guest on June 17, 2017. For personal use only.
1973 42: 463-470
Chronic Hemolytic Anemia Due to Cold Agglutinins: A 20-Year History of
Benign Gammopathy With Response to Chlorambucil
Robert S. Evans, Elizabeth Baxter and Bruce C. Gilliland
Updated information and services can be found at:
http://www.bloodjournal.org/content/42/3/463.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.