Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
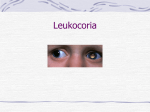
Retinoblastoma Retinoblastoma Mario Cotton Kristin Gartman Kristen Ryan Stephen F. Austin State University 1 Retinoblastoma 2 RETINOBLASTOMA What Is Retinoblastoma? Retinoblastoma (reh-tin-oh-blast-oma) is a childhood cancer arising from immature retinal cells in one or both eyes and can strike from the time a child is in the womb up to 5 years of age. This cancer is curable if caught early enough. However, 87% of the children stricken with this disease worldwide die, mostly in developing countries. In developed countries, 97% of those who do live have moderate to severe visual impairment. Retinoblastoma is a relatively uncommon tumor of childhood that accounts for about 3% of the cancers in children under the age of 15. The tumors originate in the retina, the light sensitive layer of the eye, which enables the eye to see. When the tumors are present in one eye, it is referred to as unilateral retinoblastoma, and when it occurs in both eyes it is referred to as bilateral retinoblastoma. 60% of the cases involve only one eye (unilateral); the rest affect both eyes (bilateral). 90% of retinoblastoma patients have no family history of the disease and only 10% of newly diagnosed patients have other family members with retinoblastoma. Early diagnosis and intervention is critical to the successful treatment of this disease. Common signs of retinoblastoma include: a white "glow" or "glint" in the pupil of one or both eyes in dim lighting white pupil in a color photo crossed or misaligned eyes Retinoblastoma 3 If you notice a white glow in any of your children’s photos, please contact your pediatrician or ophthalmologist immediately and have their eyes examined. Request pupil dilation of both eyes. If your physician is unable or unwilling to do the pupil dilation, please insist on a referral. Although it is rare, retinoblastoma can spread or metastasize outside of the eye to the brain, the central nervous system (brain and spinal cord), and the bones. In these cases, chemotherapy is prescribed by a pediatric oncologist and is administered through the peripheral blood vessels or into the brain for months to years after initial diagnosis of metastatic disease. Symptoms The white reflection often picked up in photographs is called leukokoria; when a tumor is present in the eye it prevents the lights of a camera's flash from reaching the back of the eye for processing by the retina. The flash can create a white eye effect due to the tumour or tumors instead of the familiar red eye effect that we often see in a healthy eye. Leukocoria (white pupil) and misaligned eyes (strabismus) are the most common signs of retinoblastoma. In other cases, the child may have developed neovascular glaucoma and may be in pain. Longstanding glaucoma can cause enlargement of the eye (buphthalmos). Children with neovascular glaucoma and enlargement of the eye are at greater risk for extraocular spread of their retinoblastoma. Retinoblastoma 4 A family history of retinoblastoma can be very important. Retinoblastoma was the first cancer to be directly associated with a genetic abnormality (Deletions or mutation of the q14 band of chromosome 13). Retinoblastoma can occur sporadically (without a family history) or it can be inherited (with a family history). If a genetic mutation is found there is a 45-50% chance that the parents will have another child with retinoblastoma. If there is no family history and no mutation is found, the risk of having a second child with retinoblastoma is 2-5%. The average age of children first diagnosed with retinoblastoma is 18 months. Treatment of Retinoblastoma The treatment of retinoblastoma is customized for each patient. Almost all parents choose some form of treatment for their child. No treatment may mean that the child would die. Goals of treatment from most to least important ranking are: saving life, maintaining the eye and vision, and preserving cosmetic appearance. Enucleation (ee-nuke-lee-a-shon) is the most common form of treatment for retinoblastoma. During an enucleation, the eye is surgically removed. This is necessary because it is the only way to remove the cancer completely. The removal of the eye is done under general anesthesia (the child is asleep). A parent may accompany the child to the operating room on the day of surgery and may be present until the child is anesthetized. The eyebrow, lids, and muscles of the eye are all left in place. Blinking, tearing, and movement of the brow are not affected from this surgery. The operation takes less than an hour and is not painful. Children go home the same day and are usually examined in the office on the following day when post-operative instructions and care are explained. A ball of plastic, rubber, or coral is placed where the eye had been so there is no cavity or hole. When both eyes are involved, sometimes the more involved or "worse" eye is enucleated, while the other eye may be treated with one of the vision-preserving treatments, such as external-beam radiation, plaque therapy, cryotherapy, laser treatment, and chemoreduction which are described below. External beam radiation has been used since the early 1900's as a way to save the eye(s) and vision. The radiation treatment is performed on an outpatient basis five times Retinoblastoma 5 per week over a 3 to 4 week stretch. Immediately after treatment, the skin may be sunburned or a small patch of hair may be lost in the back of the head from the beam exit position. Following external beam radiation, long-term effects can include cataracts, radiation retinopathy (bleeding and exudates of the retina), impaired vision, and temporal bone suppression (bones on the side of the head which do not grow normally). Radioactive plaques are disks of radioactive material that were developed in the 1930's to radiate retinoblastoma. The child must be hospitalized for this procedure, and undergoes two separate operations (one to insert the plaque and one to remove it) over 3 to 7 days. No pregnant visitors or health care professionals may visit or care for the child, and children under twelve years old are not permitted to visit. Following the plaque, long-term effects including cataracts, radiation retinopathy, and impaired vision may occur. Laser therapy, sometimes called photocoagulation or laser hyperthermia (which are two different techniques), is a non-invasive treatment for retinoblastoma. Lasers vey effectively destroy smaller retinoblastoma tumors. This type of treatment is usually done by focusing light through the pupil onto and surrounding the cancers in the eye. Laser treatment is done under local or general anesthesia, usually does not have any post-operative pain associated with it, and does not require any post-operative medications. Cryotherapy is another treatment which is performed under local or general anesthesia and freezes smaller retinoblastoma tumors. Cryotherapy usually has to be repeated many times to successfully destroy all of the cancer cells. Cryotherapy causes the lids and eye to swell for 1 to 5 days; sometimes the swelling is so much that the children are unable to open their lids for a few days. Eye drops or ointment can be given to reduce the swelling. Chemoreduction is the treatment of retinoblastoma with chemotherapy. Chemotherapy is given intravenously to your child, passes through the blood stream, and causes the tumors to shrink within a few weeks if successful. Children may require as many as twenty treatments with re-examinations of the eye under anesthesia every 3 weeks. Frequency United States Retinoblastoma 6 It is estimated that around 250-500 new cases of retinoblastoma occur in the United States yearly. International Worldwide, the incidence of retinoblastoma is recorded to be about 11 cases per million children younger than 5 years. A more commonly used estimate is 1 case of retinoblastoma per 18,000-30,000 live births, depending on the country. In the Philippines, unpublished reports have estimated the incidence to be greater than 1 case of retinoblastoma per 18,000 live births. Mortality/Morbidity Survival rates for patients with retinoblastoma range from a reported 86-92%. However, this must be kept in the context of the retinoblastoma cancers. In actuality, the survival rate drops with each decade of life for patients with the genomic mutation. The genomic mutation is a gene mutation within every cell of the individual's body. These patients typically present with either bilateral disease or unilateral-multifocal (one eye with multiple distinctly separate tumor foci) disease. These individuals have a predisposition for developing second cancers later in life. Mortality in these individuals is consequently much higher than those with somatic mutations (ie, affecting one retinal cell only and unilateral-unifocal disease). The greatest predictor of death is extraocular extension, either directly through the sclera or via extension along the optic nerve. Several of these topics are discussed further in later sections of this article. Race There seems to be no racial predilection for retinoblastoma. No difference in incidence exists among blacks and whites. Sex Age Studies show that there appears to be no significant difference in the incidence of retinoblastoma by sex for children aged 0-14 years. The estimated boys-to-girls ratio is reportedly 1.12:1. Retinoblastoma 7 Retinoblastoma is diagnosed at an average of 18 months with 90% diagnosed before patients reach age 5 years. Children who are affected bilaterally are diagnosed at an average age of 13 months, while patients with unilateral retinoblastoma are diagnosed at an average age of 24 months. When a known family history of retinoblastoma exists, patients with bilateral retinoblastoma are diagnosed at an average age of 11 months. A few cases of retinoblastoma in adults (aged 20 y and older) have been reported in the literature. Some theorize that these lesions arise from a previously existing retinocytoma that underwent malignant transformation. Good info for Parents Side Effects of Cancer and Cancer Treatment Cancer and cancer treatment can cause a variety of side effects; some are easily controlled and others require specialized care. Below are some of the side effects that are more common to retinoblastoma and its treatments. Fatigue. Fatigue is extreme exhaustion or tiredness, and is the most common problem that people with cancer experience. More than half of patients experience fatigue during chemotherapy or radiation therapy, and up to 70% of patients with advanced cancer experience fatigue. Patients who feel fatigue often say that even a small effort, such as walking across a room, can seem like too much. Fatigue can seriously impact family and other daily activities, can make patients avoid or skip cancer treatments, and may even impact the will to live. Nausea and vomiting. Vomiting, also called emesis or throwing up, is the act of expelling the contents of the stomach through the mouth. It is a natural way for the body to rid itself of harmful substances. Nausea is the urge to vomit. Nausea and vomiting are common in patients receiving chemotherapy for cancer and in some patients receiving radiation therapy. Many patients with cancer say they fear nausea and vomiting more than any other side effects of treatment. When it is minor and treated quickly, nausea and vomiting can be quite uncomfortable but cause no serious problems. Persistent vomiting can cause dehydration, electrolyte imbalance, weight loss, depression, and avoidance of chemotherapy. After Treatment Retinoblastoma 8 All children cured of cancer, including those with retinoblastoma, require lifelong, follow-up care. Once a child has been free of retinoblastoma for two to four years following treatment, and is considered cured, the emphasis during periodic follow-up visits changes. Pediatric oncologists will focus on the quality of the child's life, including developmental and emotional concerns. Most young children adapt well to the loss of one eye if enucleation took place. Rarely, both eyes will require removal to save the child's life. If both eyes are removed, the local educational system is required to provide special services. Parents are encouraged to investigate the school's services and advocate on their child's behalf. Based on the therapy the child received and whether the child has the genetic form of retinoblastoma, the doctor will determine what evaluations are needed to check for long-term effects. This may include imaging studies (CT scan or MRI) and blood tests. Counseling will also be provided in the case of children who have an increased risk of additional tumors later in life, such as those with retinoblastoma in both eyes and those with one eye affected and who have a family history of the disease. Annual visits to specialized ophthalmologic and medical oncologists are necessary in order to fully monitor the child's recovery and to increase the probability that a second cancer will be detected in its earliest stages. Children who have had cancer can also enhance the quality of their future by following established guidelines for good health into and through adulthood, including not smoking, maintaining a healthy weight, and avoiding drinking alcohol in excess. Questions to Ask the Doctor Regular communication with your child's doctor is important in making informed decisions about his or her health care. Consider asking the following questions of your child's doctor: Does my child have the genetic form of retinoblastoma? What is the stage of the disease? What are the treatment options? What clinical trials are open for my child? What treatment do you recommend? Why? What is the likelihood that the recommended treatment can save my child's vision? What can I expect chemotherapy to accomplish in the treatment of my child's cancer? Retinoblastoma What are the relative benefits and risks of radiation treatment in treating my child? What are the common side effects of each treatment, in the short term and long term? What follow-up tests will my child need, and when will they be needed? Retinoblastoma Tidbits Cancer Facts: Cancerous growths have been discovered in dinosaurs! Retinoblastoma was documented in children more than 2,000 years ago Retinoblastoma Facts: More than 95% of patients treated for retinoblastoma in the U.S. are cured More than 90% of patients retain at least one eye More than 80% of the children keep 20/20 vision Complete blindness is unusual in children who have been successfully treated for retinoblastoma Did you Know? Retinoblastoma is a cancer Retinoblastoma is the most common eye cancer in children Retinoblastoma is about as common as hemophilia Retinoblastoma affects boys as commonly as girls The average age for diagnosis of retinoblastoma when one eye is involved is 2.5 years There are 350 new cases of retinoblastoma per year in the U.S. and about 5,000 worldwide Retinoblastoma affects all races equally Diagnostic Facts: Retinoblastoma is diagnosed with the indirect ophthalmoscope, ultrasound, CT/MRI scans Biopsies are rarely necessary Anesthesia for examination and treatment may be necessary as often as every 2 weeks Examination of the parents may help in the diagnosis of the child 9 Retinoblastoma Patient Information Resources Candlelighters Childhood Cancer Foundation P.O. Box 498 Kensington, MD 20895 Toll Free: 800-366-2223 Phone: 301-962-3520 www.candlelighters.org Children's Hospice International 901 N. Pitt St., Ste. 230 Alexandria, VA 22314 Toll Free: 800-24-CHILD (800-242-4453) Phone: 703-684-0330 www.chionline.org The Eye Cancer Network Eye Care Foundation 115 E. 61st Street New York, NY 10021 Phone: 212-832-8170 www.eyecancer.com Make-A-Wish Foundation 3550 N Central Ave., Ste. 300 Phoenix, AZ 85012 Toll Free: 800-722-9474 www.wish.org National Childhood Cancer Foundation 440 E Huntington Dr. P.O. Box 60012 Arcadia, CA 91006-6012 Toll Free: 800-458-6223 (US and Canada only) Phone: 626-447-1674 www.nccf.org www.CureSearch.org National Children's Cancer Society 1015 Locust, Ste. 600 10 Retinoblastoma St. Louis, MO 63101 Toll Free: 800-532-6459 www.nationalchildrenscancersociety.org Outlook: Life Beyond Childhood Cancer www.outlook-life.org The Children's Cause for Cancer Advocacy 1010 Wayne Ave., Ste. 770 Silver Spring, MD 20910 Phone: 301-562-2765 www.childrenscause.org The Starlight Starbright Foundation 1850 Sawtelle Blvd., Ste. 450 Los Angeles, CA 90064 Phone: 310-479-1212 www.slsb.org National Organization for Rare Disorders (NORD) 55 Kenosia Ave. P.O. Box 1968 Danbury, CT 06813-1968 Phone: 203-744-0100 www.rarediseases.org Rare Cancer Alliance 1649 N. Pacana Way Green Valley, AZ 85614 Phone: 206-600-5327 www.rare-cancer.org 11 Retinoblastoma 12 References About Retinoblastoma. (n.d.). Retrieved July 30, 2008, from www.chect.org.uk Abramson, David H., MD, FACS & Servodidio, Camille, RN, MPH. (1997-2002). A Parent’s Guide to Understanding Retinoblastoma. Retrieved July 30, 2008, from www.retinoblastoma.com Adventura, Marichelle L., MD, Roque, Manolette R., MD, MBA, DPBO, FPAO, Aaberg, Thomas M., Jr, MD & Roque, Barbara, L., MD. (2006, February 16). Retinoblastoma. Retrieved July 30, 2008, from www.emedicine.com/oph/topic346.htm Finger, Paul T., MD. (1998-2008). Retinoblastoma. Retrieved July 30, 2008, from http://www.eyecancer.com/Patient/Condition.aspx?nID=53&Category=Retinal+T umors&Condition=Retinoblastoma Retinoblastoma – Childhood. (2006-2008). Retrieved July 30, 2008, from http://www.cancer.net/patient/Cancer+Types/Retinoblastoma+-+Childhood What is retinoblastoma? (n.d.). Retrieved July 30, 2008, from http://www.retinoblastoma.net/whatisrb.html