Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
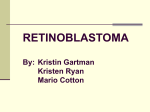
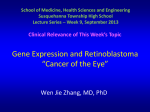
Atlas of Genetics and Cytogenetics in Oncology and Haematology INIST-CNRS OPEN ACCESS JOURNAL Solid Tumour Section Short Communication Head and Neck: Retinoma Helen Dimaras Division of Hematology and Oncology, The Hospital for Sick Children, Toronto, ON, Canada (HD) Published in Atlas Database: March 2012 Online updated version : http://AtlasGeneticsOncology.org/Tumors/RetinomaID5049.html DOI: 10.4267/2042/47543 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2012 Atlas of Genetics and Cytogenetics in Oncology and Haematology Identity Clinics and pathology Other names Retinocytoma Note Retinoma is the benign precursor to the childhood eye tumor, retinoblastoma. In rare cases, it remains benign for the lifetime of the individual, never progressing to retinoblastoma. Retinoma has three (3) characteristic clinical features: a grey, translucent mass in the retina; cottage cheese-like calcification; and a hyperplastic retinal epithelium/chorioretinal scar (Gallie et al., 1982). Vitreous seeds have also been observed associated with retinoma (Lueder et al., 1995). Note The diagnosis of retinoma is made by clinical observation. Evidence of retinoma in eyes removed for retinoblastoma is often observed by histology (Dimaras et al., 2008; Eagle, 2009), and sometimes clinically after treatment of the overlying retinoblastoma tumor (Dimaras et al., 2009). Epidemiology Retinoma has been observed clinically in 1.8% (Gallie et al., 1982) to 3.2% (Abouzeid et al., 2012) of retinoblastoma cases and by pathology in 15.6% (Dimaras et al., 2008) to 20.4% (Eagle, 2009) of enucleated retinoblastoma specimens. Retinoma showing classic features of chorioretinal scar, translucent retinal mass and calcification. Atlas Genet Cytogenet Oncol Haematol. 2012; 16(9) 680 Head and Neck: Retinoma Dimaras H Retinoma histology showing abundant fleurettes and sparse cells with eosinophilic cytoplasm. Pathology Prognosis Retinoma is histologically distinct from its malignant counterpart, retinoblastoma. Retinoma displays abundant fleurettes, eosinophilic cytoplasm, foci of calcification and non-proliferative cells (Margo et al., 1983; Dimaras et al., 2008). Retinoma lacks the typical features of retinoblastoma (Homer Wright and Flexner-Wintersteiner rosettes, nuclear molding, abundant mitoses and necroses), and is often observed adjacent to retinoblastoma tumor in enucleated specimens (Dimaras et al., 2008). Retinoma is by definition benign and does not pose any threat to life, thought it may interfere with vision. Regular examination of rare individuals with retinoma is necessary to spot any sign of malignant transformation to retinoblastoma. Cytogenetics Note Retinomas identified histologically adjacent to retinoblastomas have been studied by FISH. Retinomas display low level genomic copy number changes in several genes altered to a higher degree in adjacent retinoblastoma tumors (Gain: KIF14, DEK, E2F3, MYCN; Loss: CDH11), suggesting a shared origin (Dimaras et al., 2008). The altered copy number changes in retinoma are not manifested at the expression level as in retinoblastoma. Treatment Frequent ophthalmic examination monitors for potential malignant progression. Malignant progression is more common in children with retinoma than in adults. In a child, the physician may opt to treat retinoma as retinoblastoma if there is even a minor suspicion of malignant progression. Evolution Genes involved and proteins Because retinomas share the same genetic origin as retinoblastoma and are frequently observed adjacent to retinoblastoma in pathological specimens, it is hypothesized that every retinoblastoma passes through a retinoma stage. However, rare retinomas do not ever progress to retinoblastoma. The difference between the retinomas that progress to malignancy and those that do not is unknown. Benign cystic growth has also been observed in some retinomas (Sampieri et al., 2008; Abouzeid et al., 2012). Atlas Genet Cytogenet Oncol Haematol. 2012; 16(9) Note Like retinoblastoma, retinoma is initiated by the loss of both copies of the RB1 tumor suppressor gene. RB1 (Retinoblastoma tumor supressor gene) Location 13q14.2 681 Head and Neck: Retinoma Dimaras H Note Retinoma is initiated by the loss of both copies of the RB1 gene. Adjacent specimens of retinoblastoma and retinoma display the same mutation(s) in RB1 (Dimaras et al., 2008). DNA / RNA DNA: 27 exons, 180 kb genomic DNA; RNA: 4840 bp mRNA transcript. Protein 928 amino acid phosphoprotein. References Gallie BL, Ellsworth RM, Abramson DH, Phillips RA. Retinoma: spontaneous regression of retinoblastoma or benign manifestation of the mutation? Br J Cancer. 1982 Apr;45(4):513-21 Margo C, Hidayat A, Kopelman J, Zimmerman LE. Retinocytoma. A benign variant of retinoblastoma. Arch Ophthalmol. 1983 Oct;101(10):1519-31 Lueder GT, Héon E, Gallie BL. Retinoma associated with vitreous seeding. Am J Ophthalmol. 1995 Apr;119(4):522-3 Dimaras H, Khetan V, Halliday W, Orlic M, Prigoda NL, Piovesan B, Marrano P, Corson TW, Eagle RC Jr, Squire JA, Gallie BL. Loss of RB1 induces non-proliferative retinoma: increasing genomic instability correlates with progression to retinoblastoma. Hum Mol Genet. 2008 May 15;17(10):1363-72 CDKN2A (p16INK4A) Location 9p21.3 Note Retinoma is marked by upregulation of p16INK4A mRNA and protein, which is not observed in retinoblastoma. The upregulation of the senescence-associated protein may account for the non-proliferative nature of retinoma (Dimaras et al., 2008). DNA / RNA DNA: 3 exons, 6.6 kb genomic DNA; RNA: 471 bp mRNA transcript. Protein 156 amino acid protein. Sampieri K, Mencarelli MA, Epistolato MC, Toti P, Lazzi S, Bruttini M, De Francesco S, Longo I, Meloni I, Mari F, Acquaviva A, Hadjistilianou T, Renieri A, Ariani F. Genomic differences between retinoma and retinoblastoma. Acta Oncol. 2008;47(8):1483-92 Dimaras H, Khetan V, Halliday W, Héon E, Chan HS, Gallie BL. Retinoma underlying retinoblastoma revealed after tumor response to 1 cycle of chemotherapy. Arch Ophthalmol. 2009 Aug;127(8):1066-8 Eagle RC Jr. High-risk features and tumor differentiation in retinoblastoma: a retrospective histopathologic study. Arch Pathol Lab Med. 2009 Aug;133(8):1203-9 Abouzeid H, Balmer A, Moulin AP, Mataftsi A, Zografos L, Munier FL. Phenotypic variability of retinocytomas: preregression and postregression growth patterns. Br J Ophthalmol. 2012 Jun;96(6):884-9 This article should be referenced as such: Dimaras H. Head and Neck: Retinoma. Atlas Genet Cytogenet Oncol Haematol. 2012; 16(9):680-682. Atlas Genet Cytogenet Oncol Haematol. 2012; 16(9) 682