Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Stroke
محمد محمود الشيخ عيسى.د
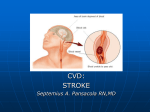
Stroke is a rapid appearance of focal neurologic deficit that attributable to a focal vascular cause.
This definition is a clinical and need brain imaging to support the diagnosis.
It is the third most common cause of death.
It causes death and disability by either ischemia and infarction or by hemorrhage.
Stroke according to it’s pathology divided into:Ischemic stroke
Thrombotic
Embolic
Hemorrhagic stroke
Intracerebral Hemorrhage
Subarachnoid Hemorrhage
84%
53%
31%
16%
10%
6%
Ischemic stroke
Acute stroke: focal neurological deficit due to occlusive vascular lesion. It is of rapid onset lasting
longer than 24 hours.
Risk factor for Ischemic stroke:A-Non- modifiable
▪ Age: risk double for each decade after 55 years of age.
▪ Gender: male > female , except in very young and very old .
▪ Race: more common in black.
▪ Heredity: The risk is 2.4 for paternal history.
The risk is 1.4 for maternal history.
▪ Previous vascular event, e.g M.I., stroke or peripheral embolism.
▪ Fibromuscular dysplasia.
B-Modifiable risk factors
1-Hypertention: the risk is 2-5time greater than non hypertensive patients.
2- Cardiac disease: acute MI, AF, Rhumatiod heart disease, endocarditis , patent foramen ovule
3- Diabetes mellitus .
4- Dyslipidemia: ↓HDL and ↑LDL .
5- TIA: the risk 10 - 15%.
6- Tobacco use and smoking.
7- Hyper viscosity (polycythemia).
8- Contraceptive pills.
9- Excessive alcoholic consumption .
10-Homocystinuria.
13- Carotid artery stenosis.
11- Antiphospholipid antibody syndrome.
14-Physical inactivity and obesity.
12- Vasculitis.
15-Social deprivation .
1
Pathophysiology of ischemic stroke
1. Thrombosis:- produce stroke by
◘ Occluding large cerebral arteries (especially the internal carotid, middle cerebral, or basilar), or
small penetrating arteries (as in lacunar stroke), or cerebral veins and venous sinuses.
◘ Symptoms typically evolve over minutes to hours.
◘ Thrombotic strokes are often preceded by TIAs , which tend to produce similar symptoms
because they affect the same territory recurrently.
2. Embolism:- produce stroke when
◘ Cerebral arteries are occluded by distal passage of emboli from the heart, aortic arch, carotid
arteries or cerebral arteries.
◘ Emboli in the anterior cerebral circulation most often occlude the middle cerebral artery or its
branches.
◘ Emboli in the posterior cerebral circulation usually lodge at the apex of the basilar artery or in the
posterior cerebral arteries.
◘ Embolic stroke characteristically produce neurologic deficit that maximal at onset.
◘ Cardiac emboli produce symptoms vary between attacks since different vascular territories are
affected..
Clinical evidence of embolus source
1- Carotid bruit (stenosis).
2- Atrial fibrillation or other arrhythmias.
3- Valvular heart diseases.
4- Recent M.I.
Ischemia
● Acute occlusion of an intracranial vessel causes reduction in blood flow to the brain region is
supplies.
● The magnitude of flow reduction is a function of collateral blood flow and this depends on
individual vascular anatomy and the site of occlusion.
● A fall in cerebral blood flow to zero causes death of brain tissue within 4 to 10 min.
● If blood flow is restored prior to a significant amount of cell death, the patient may experience
only transient symptoms, i.e. a TIA.
● Tissue surrounding the core region of infarction is ischemic but reversibly dysfunctional and is
referred to as the ischemic penumbra .
● The ischemic penumbra will eventually infarct if no change in flow occurs and hence saving the
ischemic penumbra is the goal of thrombolytic therapy and newer therapies.
2
Clinical feature:
I-Anterior circulation
(internal carotid artery and it's branches: ophthalmic artery which supplies the retina, Anterior
cerebral artery and middle cerebral artery )
1.Anterior cerebral artery:
Occlusion of the anterior cerebral artery leads to a paralysis and sensory loss affecting the contra
lateral leg.
Voluntary control of micturition may be impaired.
2.Middle cerebral artery
MCD is the vessel most commonly involved in ischemic stroke.
A- Superior branch of middle cerebral artery occlusion of it result in
■ Contralateral hemiparesis and hemisensory deficit involving the face and arm and hand more
than the leg.
■ If the dominant hemisphere is involved there will be also brocas (expressive) aphasia.
3
B- Inferior branch of middle cerebral artery
Occlusion of this branch result in
■ Contralateral homonymous hemianopia.
■ Marked impairment of cortical sensory functions.
■ If the dominant hemisphere is involved, Wernicke (receptive) aphasia occur.
If the non dominant hemisphere is involved.
■ Lack of awareness that a deficit exists (anosognosia).
■ Neglect and failure to recognize the contralateral limbs.
■ Neglect of the contralateral side of external space.
■ dressing apraxia and constructional apraxia.
C- lenticulostriate branch of middle cerebral artery:
Occlusion of this artery produce small vessel lacunar stroke within the internal capsule, this
produce
1- Pure motor stroke or sensory motor stroke contralateral to the lesion.
2- Ischemia within the genu of the internal capsule causes facial weakness followed by arm then leg
weakness.
3- clumsy hand, dysarthria lacunar syndrome.
D- Occlusion at the bifurcation of middle cerebral artery
This will produce severe stroke syndrome combines the features of superior and inferior division
stroke. Its clinical features include:◙ Contralateral hemiparesis and hemisensory deficit involving the face and arm and hand more
than the leg.
◙ Homonymous hemianopia.
◙ If the dominant hemisphere is affected, global (combined expressive and receptive) aphasia.
E- Occlusion of the stem of the middle cerebral artery
The result clinical syndrome is similar to that seen following occlusion at the bifurcation except
that, in addition, infarction of the motor fibers in the internal capsule causes paralysis of the
contralateral leg. The result is contralateral hemiplegia and sensory loss affecting the face, hand,
arm, and leg.
Internal carotid artery:
Occlusion of the internal carotid artery is
☼ Preceded by TIAs or by transient monocular blindness
caused by ipsilateral ophthalmic artery ischemia.
☼ Symptomatic occlusion result in contralateral hemiplegia,
hemisensory deficit, and homonymous hemianopia.
☼ Aphasia is present with dominant hemisphere involved.
4
II- Posterior circulation (vertebro basilar artery and it's branches)
1- posterior cerebral artery
The paired posterior cerebral arteries arise from the tip of the basilar artery
and supply the occipital cerebral cortex, medial temporal lobes, thalamus,
and rostral midbrain.
Occlusion of a posterior cerebral artery produce homonymous hemianopia
affecting the contralateral visual filed.
Macular vision may be spared, because of the dual (middle and posterior cerebral artery) blood
supply to the portion of the visual cortex representing the macula.
Occlusion near the origin of the posterior cerebral artery at the level of the midbrain causes vertical
gaze palsy, oculomotor (III) nerve palsy, internuclear ophthalmoplegia.
Bilaterl posterior cerebral artery infarction may result in cortical blindness, memory impairment
(from temporal lobe involvement) and inability to recognize familiar face (prosopagnosia).
2- Long circumferential vertebrobasilar branches
The long circumferential branches arising from the vertebral and basilar arteries are the posterior
inferior cerebellar, the anterior inferior cerebellar and the superior cerebellar arteries.
A- Posterior inferior cerebellar artery
Occlusion of PICA leads to ipsilateral cerebellar ataxia, Horner syndrome and facial sensory deficit,
and nystagmus, vertigo, nausea, vomiting, dysphagia, dysarthria and hiccup. Contralateral impaired
pain and temperature sensation in the limbs.
B- Anterior inferior cerebellar artery
Occlusion affect lateral portion of the caudal pons and produce ipsilateral cerebellar ataxia
ipsilateral facial weakness, facial sensory deficit, nystagmus, vertigo, nausea and vomiting.
Gaze palsy, deafness, tinnitus are common findings.
Contralateral impaired pain and temperature sensation in the limbs.
C- Superior cerebellar artery
Occlusion of this artery there will be resembles that associated with anterior inferior cerebellar
artery lesions but there will be skew division of the eyes.
Auditory function is unaffected.
Contralateral loss of touch, vibration, position, pain and temperature sense.
3-Vertebrobasilar penetrating branches :
Occlusion of this branches causes brainstem infarction lead to complex pattern of dysfunction
depending on the site of the lesion and its relationship to the cranial nerve nuclei, long tracts and
brainstem connection.
5
Lacunar infarction:
1- Small infarct less than 1.5 cm3.
2- Single lacunar infarction typically cause minor stroke; pure motor or sensory stroke, sudden
unilateral ataxic hemiparesis or dysarthria-clumsy hand syndrome.
Note:
Coma: when bilateral brainstem infarction damages the reticular formation system.
Pseudobulber palsy: bilateral supranuclear palsy (UMN) lesion of the lower cranial nuclei.
Clinical subtypes of stroke
-Transient Ischemic Attack ((T.I.A)): Focal neurological deficit reach peak within seconds and
lasting for minutes or hours with complete recovery within 24 hours, it is a warning sign of
complete stroke (( 10-15% )) within 3 months.
-Reversible Ischemic neurological deficit ((R.I.N.D)): The neurological deficit last longer than 24
hours but resolve completely or mostly complete within few days.
-Progressing stroke ( or Stroke in evolution ): The neurological deficit progress in stepwise manner
over 6hours of onset to few days.
-Complete stroke: Focal neurological deficit that persist with no further worsening
-Multi-infarct dementia (MID): MID caused by multiple small or large infarctions and the patient
present with loss of short term memory, getting lost in familiar place , walking with rapid
shuffling steps , loss of bladder and bowel control with crying or laughing
inappropriately
Investigation:
CT scan :-CT will be normal in early infarction (less than 6 hours).
CT very sensitive for acute hemorrhage.
MRI: Diffusion weighted imaging highly sensitive and specific for stroke.
MRA to see the circle willis and neck vessels.
F.B.S, CBC , ESR
B urea, S.creatinine
S. lipid profile
Prothrombine time and partial thromboplastine time
ECG, Echocardiography
Doppler U/S of carotid artery
Cerebral angiography
6
Management of stroke
The time is brain
Mean that treatment of stroke should be considered as an emergency , thus avoiding of
delay should be the major aim in management of acute stroke and all patients with stroke should
be admitted to the hospital.
Initial examination should include
1-Observation of breathing and pulmonary function, pulse, Bp, temp and arterial oxygen saturation
using pulse oximetery
2-Evaluation of concomitant heart disease
3- Venous line inserted and samples of blood taken for RBS , B urea and creatinine
4-ECG
5-Brain imaging ((CT or MRI)) for patient with TIA or stroke
Management at emergency service
1-Oxygen should be administered if the oxygen saturation below 95%
2- Patient have large infarction with massive oedema may benefit from anti – oedema agents
such as mannitol or artificial ventilation , surgical decompression to reduce the intracranial
pressure .
3- The blood pressure is usually acutely raised after a stroke and should not be lowered in the acute
stage, since it will always return towards the patient’s normal level within 24-48 hours because the
ischemic penumbra depend upon the raised perfusion pressure and the blood pressure lowering if
there is :•Bp < 220 / 120mm Hg on repeated measurement .
•Patient with severe cardiac failure or renal failure
•Patient with aortic dissection
•Patient with hypertensive encephalopathy
•Patient with intracranial hemorrhage
Low Bp secondary to hypovolemia are associated with neurological deterioration in acute stroke
and should be treated with volume expanders, normal saline ((0.9%)) is recommended for fluid
replacement during the first 24 hours after stroke
4-Treatment serum glucose < 200mg / dl
( < 11.1 mmol / l ) with soluble insulin .
Severe hypoglycemia {< 50mg/dl (<2.8mmol/l)} should be treated with intravenous dextrose
or infusion of 10-20 % glucose
5-Pyrexia (temperature < 37.5Cº ) treated by paracetamol and fanning with a search for
concurrent infections
7
Treatment of ischemic stroke
I- Thrombolytic therapy: recombinant tissue plasminogen activator (rtPA) for acute ischemic
stroke. Indication: Clinical diagnosis of stroke.
Onset of symptoms to the time of the drug administration is 3 hours.
CT scan of >1/3 of the MCA territor.y (ischemia no hemorrhage ) .
Age ≥18years .
Contraindication: Sustained BP> 185/110 despite treatment.
Platelets < 100000, HCT< 25%.
Glucose < 50 or > 400mg/dL.
Use of heparin within 48h and prolonged PTT, or elevated INR.
rapidly improving symptoms.
Prior stroke or head injury within 3months.
Prior intracranial hemorrhage.
Major surgery in preceding 14days.
Minor stroke symptoms.
Gastrointestinal bleeding in preceding 21days.
Recent myocardial infarction.
Coma or stupor.
Administration of rtPA:Intravenous access with two peripheral IV lines (avoid arterial or central line placement).
for rtPA administer 0.9 mg / kg intravenously (maximum 90mg) IV as 10 % of total dose by
bolus , followed by remainder of total dose over 1h with frequent cuff blood pressure monitoring.
No other antithrombotic treatment for 24 h.
For decline in neurologic status or uncontrolled blood pressure, give cryoprecipitate, and reimage
brain emergently.
• Avoid urethral catheterization for 2h.
• Intra- arteiral thrombolysis is recommended for treatment of acute MCA or basilar artery
occlusion within 6 hours from the onset of symptoms
II-Endovascular mechanical thrombectomy
This accomplished by inserting a catheter into femoral artery, directing it into the cerebral
circulation and deploying a cork screw-like device to ensnare the clot, which is then withdrawn
from the body. This used in
*Patient whom unable to receive thrombolytic drugs
*Patient not respond to thrombolytic agent
*Can be done within 8 hours from the onset of symptoms
8
Anticoagulant therapy
Indications of anticoagulants:•Unstable TIA
•Stroke in-evolution
•Stroke associated with AF
•Stroke in patient with valvular heart disease
•Stroke in patient with acute anterior Q -wave myocardial in faction
•Stroke patient with prosthetic heart valve (For imbolic stroke )
Unfractionated heparin 1000-2000 IU/hr intravenous infusion (APTT 1.5-2.5 times the control time
of the test ).
Low- molecular- weight heparin: used in patient to switch from IV heparin to warfarin and used in
patient at high risk of recurrent thromboembolism on temporary interruption of warfarin therapy
for invasive procedures.
Warfarin (curamins ):- oral anticoagulant the usual maintenance dose is 5-15mg/d orally, can be
started at the same time with heparin and about two days after the prothrombin time (PT) reaches
international normalized ratio (INR) =2.0-3.0 .heparin can be discontinued.
The PT or INR should be measured at lest every two weeks.
-Non valvular AF (INR 2-3) in patient < 75 years and younger but has risk factors
-Valvular heart disease (INR 2.5-3)
-Bio-prosthetic valves, warfarin (INR 2.5) for 3 months followed by long term aspirin alone (75 –
1oo mg/day)
-Mechanical valve (INR 3 -3.5)
Anticoagulant given for small and medium but not for acute large size
embolic ischemic
infarction .
Antiplatelet therapy
For thrombotic stroke or TIA
1- Aspirin: 300 mg at once then 75 mg daily.
Adverse effect include dyspepsia, nausea, abdominal pain, diarrhea, skin rash, peptic
ulcer, gastritis and gastrointestinal bleeding.
2- Clopidogrel: (75mg orally daily) Slightly more effective than aspirin in preventing vascular events
in high risk patient ((i.e. patients with previous stroke, peripheral artery disease, symptomatic
coronary disease, or Dm)).
Adverse effect diarrhea, skin rash, neutropenia, thrombocytopenia and thrombotic
thombocytopenic purpura.
9
3- Dipyridomole:MR 200 mg 12 – hourly if
event whilst on aspirin .
4- Clopidogrel plus aspirin : use in stroke patient with unstable angina with ECG or enzyme
changes . major bleeding were increased with this combination
Carotid endarterectomy
CEA is recommended in patents with 70-99% stenosis and only performed in centers with
perioperative complication ((all strokes and death)) of less than 6% and ideally within 2weeks after
last ischemic stroke.
The benefit is more in patients >75years, and men appear to benefit more than women
CEA is indicated for patients with stenosis 50- 69% with very recent hemispheric stroke and
only performed in centers with a perioperative complication rate of less than 3%.
The patient should remain on antiplatelet therapy before and after CEA
Prevention and management of complication
1-Treatment of brain oedema and elevated ICP.
2-Treatment and prevention of aspiration pneumonia, DVT and pulmonary embolism
3-Treatment of post stroke seizure .
4-Prevention and treatment of UTI .
5- Prevention and treatment of pressure sore .
Primary prevention of stroke
1-Blood pressure, sugar, cholesterol should be checked regularly
2-Cigarette smoking, heavy use of alcohol should discouraged
3-Regular physical activity is recommended
4-Diet low in salt and saturated fat, high in fruit and vegetable is recommend.
5-antioxidant vitamin supplement not recommended
6-Elevated body mass index is recommended to take weight reducing diet
7-Hormonal replacement to post menopausal women is not recommended
Secondary prevention of stroke
1-Treatment of hypertension, diabetes mellitus and hyperlipidema .
2-Cigarette smoking should discouraged
3-Diet rich in fruit and vegetable
4-Over weight should reduced
10