Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
A mathematical formulation of intraocular pressure
as dependent on secretion, ultrafiltration, bulk
outflow, and osmotic reabsorption of fluid
V
Ernst H. Bdrdny
An equation has been derived under simplified assumptions showing how the steady-state
value of intraocular pressure depends on rate of secretion of aqueous, episcleral venous
pressure, outflow facility at the chamber angle, colloid-osmotic pressure of the blood, systemic
arterial blood pressure, pressure distribution over the vascular tree of the eye, and filtration
properties of the vasculature in different intraocular regions.
It is shown that intraocular fluid formation will be reduced by increased intraocular pressure
in such a manner that the presence of a facility is simulated. In the conscious rabbit, this
pseudofacility is estimated to account for about 10 per cent of the measured tonographic
facility. Its absolute magnitude can be expected to rise with arteriolar vasodilatation (as
might be caused by miotics) and to drop with arteriolar vasoconstriction.
A method is outlined which should allow pseudofacility to be measured in the glaucomatous
human eye.
If intraocular pressure is not excessively high, changes in arteriolar tone will tend to cause
parallel changes in pressure and pseudofacility simulating homeostatic adjustment of facility
to pressure.
of major importance in most cases: secretion, episcleral venous pressure, and outflow facility.2 The following is an attempt
to deal simultaneously with all these factors
determining the steady state pressure of
the eye. The treatment is only a first approximation and undoubtedly will have to
be refined. Even at this stage, however, it
helps to clarify the interactions between
the many different factors.
The mathematics employed are the simplest possible. To keep them so, it has
been necessary to introduce a few unfamiliar concepts. A list of symbols appears
at the end of the paper.
JLhe possibility that filtration from the
vascular tree can contribute to formation
of the intraocular fluid and that colloid
osmotic forces can contribute to its removal
has been recognized a long time. Equations
governing an eye where these factors are
the only important ones were published in
1946.1 In later years, interest has mainly
been focused on the other factors in intraocular pressure, which almost certainly are
From the Department of Pharmacology, University
of Uppsala, Sweden.
This study was supported by Research Grant B
3060 from the Institute of Neurological Diseases
and Blindness, United States Public Health
Service, Bethesda, Md.
This paper was read in part at the Glaucoma
Research Conference, Hot Springs, Va., MayJune 1963.
I. The concept "pressure index"
Fig. 1 is a schematic drawing of the
vascular system of the eye. The main feature distinguishing it from other vascular
584
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017
V
-y-
V
Mathematical formulation of intraocular pressure 5S5
•n-
-v
territories is that the tissue pressure or
intraocular pressure, p i( under the conditions dealt with here determines and is
equal to the lateral pressure, p v , of the
veins at their point of exit from the ocular
cavity. (Note that p v here is pressure justinside the globe, not just outside.) The
arterial pressure, pn, is the mean lateral
pressure in the arterial tree outside the eye.
The exact point where it is measured is
immaterial, as long as it is central enough
not to be appreciably influenced by the
amount of blood flowing through the eye.
The ophthalmic artery may qualify.
As a start, consider p a and p v as constant.
Take a certain pressure p x between p,, and
p v ; with the exception of values of p x very
close to p,, or p v , there will as a rule be a
great many vessels on which there is one
point (or rather cross section) in which the
lateral pressure is p*. These points which
have p x in common will still have a common pressure if p,, or p v changes a little,
because their similarity in pressure depends
on their position on the scale of resistance
between vein and artery. This position can
be expressed by a "pressure index" x which
is defined as
„ - P* " Pv
(1)
The formula implies that for instance all
points with x = 0.333 are one-third of the
way between vein and artery, pressurewise.
Moderate changes in p,, or p v will not alter
this fact, which depends on the distribution
of flow resistance throughout the tree. As
long as the calibers of the vascular tree are
unchanged, a certain pressure index
identifies a certain group of points on a
number of vessels. The same group will,
however, acquire a different pressure index
if for instance arteriolar vasodilatation redistributes and changes the resistance in
the vascular tree.
It is evident that the range of variation
of pressure index is between 0 and 1, the
lower value characterizing the veins at their
point of exit, the upper one the arterial
branch in which p., is measured.
At intermediate points, the pressure in-
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017
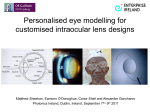
Fig. 1. Schematic diagram of the vascular tree
of the eye, to illustrate the concept "pressure index." Vessels with low pressure index are close
to the veins on the pressure scale and mainly affected by venous pressure, since p.< = .vp« +
(1 " x)-pT.
dex decides in which proportions p,, and p v
contribute to p.v (Fig. 1). From now on,
"point x" on a vessel means the point where
pressure index is x.
II. The forces involved in filtration
Rearrangement of equation (1) gives
the filtering hydrostatic pressure head acting from die lumen of the vessel at point x
Px - pi = p* - p,- = x(p. - pv)
(2)
Osmotic forces will be disregarded except
for the colloid-osmotic pressure, po,,n. This
is assumed to be constant, and fully active
throughout the vascular territory. Thus,
Pressure head for filtration = x(pn - pv) - peon
In assuming constancy of pc0n one assumes that the colloid-osmotic pressure of
the aqueous is negligible and in disregarding all other osmotic forces one assumes
that the permeability of the blood-aqueous
barrier is large enough to minimize the influence of crystalloid-osmotic differences.
Where this is not true, for instance in die
ciliary processes, the mobility of water
under crystalloid-osmotic pressure is not
impressive.3 Anyhow, the assumption of one
and only one pcoii is an approximation.
III. The concept "conductivity coefficient
for filtration"
A conventional measure of conductivity
for filtration across a membrane would be
(3)
Investigator2 Ophthalmology
December 1963
586 Bdrdny
Y
Conductivity coefficient
for filtration
individual segments (determined by Ax)
and to a composite proportionality factor
Y, which will be termed "conductivity
coefficient for filtration." This coefficient Y
embraces all the remaining local factors,
such as number of vessels, their circumference, wall properties, location, etc. The
conductivity coefficient so defined is evidently not constant all the way from artery
to vein but is a function of x, Y(x).
Thus we have
AF = Y(x)-Ax- pressure head for filtration
t
t
Pi=Pv
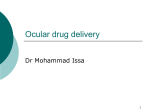
Fig. 2. Conductivity coefficient for filtration of the
vascular wall as a function of pressure index. The
black dot indicates the center of gravity of the
area A under the curve. Its pressure index is xc.
milliliters per minute per unit area and
millimeters of mercury pressure difference.
Since position along the vessel is not measured in length but in pressure index, a
special measure for conductivity has to
be used in the present treatment.
Consider the part of the vascular tree
located between pressure index x and pressure index x + Ax. It consists of a number
of short segments of vessels, all of which
carry the same lateral pressure. Some of
the vessels may have very permeable walls,
others may be thick walled. Some of them
will be located superficially in the iris,
others may be deeply embedded between
double layers of epithelium in the ciliary
processes. Some are retinal or choroidal,
even if their contribution to the filtrate
must be negligible. Some of the vessel
segments are shorter than the others, because they are narrow and the pressure
drops fast along them. In all of them the
pressure drops by the amount Ax- (p a - p v )
from one end to the other.
The contribution of filtrate per unit
time from this aggregate is AF. It is proportional to the pressure head for filtration
(determined by x), to the lengths of the
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017
The detailed distribution of Y(x) over
the vascular tree is not known. It is evident,
however, that Y is very close to zero when
x is zero, at the point of exit of the large
veins, and when x is close to 1, in the thickwalled arteries outside the eye. If filtration
occurred here it would not be counted anyhow.
Fig. 2 shows a diagram of Y as a function
of pressure index x. It is possible but not
proved that the maximum corresponds to
the anatomic capillaries. The shape of the
curve between x = 0 and 1 is pure guesswork and not essential to the argument.
The total area below the Y-curve will be
called A and represents the total conductivity for filtration or for colloid-osmotic
reabsorption of the vascular tree. Its dimension is volume per unit time and unit
pressure difference, similar to facility.
Vasomotor changes in the eye, which affect
pressure distribution over the vascular tree
(without shutting off circulation in certain
regions) will change the shape of the Ycurve but not affect A to any large extent.
(4)
h
h
IV. Filtration as a function of vascular
and intraocular pressures
Inserting the value for filtering pressure
head from (3) into (4) one obtains
A F
=
Y(x)-Ax-[x(p. - p v ) - pcull]
(5)
Passing to the limit and rearranging gives
dF _
Total filtration rate F is obtained by
integration from x = 0 to x = 1,
+A
Mathematical formulation of intraocular pressure 587
Thus, a possible interpretation of xc is
F = (p. - Pv)Jx-Y(x)dx - pcoll J Y ( X )
(7)
The secoiid integral is the total area
under the Y-curve, A. The first integral is
the moment of the area under the Y-curve
around the Y-axis. Hence it is equal to the
area A times the x-coordinate xc of the
center of gravity of the area (Fig. 2). Thus,
filtration rate F can be expressed as
F =
( p . - pv)-A-xc - p co ,,-A
(8)
Here, the first term represents outward
filtration from the vessels as it would appear in the absence of colloid-osmotic
pressure and the second term expresses
total colloid-osmotic reabsorption to the
vascular tree.
V. The pressure at the center of gravity
of the area under the Y-curve: A measure
of capillary pressure
-A
The pressure index xc of the center of
gravity of the area under the Y-curve is
hard to visualize. It can be translated,
albeit somewhat loosely, into more common physiologic concepts, however.
Making use of equations (1) and (8)
one obtains
F =
A(po -
Pv
(9)
- pen,,)
Here, p 0 is the absolute pressure corresponding to the center of gravity. What is
its physiologic meaning?
Consider the statement: No net transfer
of fluid into or out of the vascular tree
will occur by hydrostatic forces if the
excess of capillary pressure over intraocular pressure equals the colloid-osmotic
pressure of the blood.
This statement, which is a reformulation
of Starling's hypothesis, is loose insofar
as capillary pressure is ill defined; capillary
pressure is a pressure region, not a pressure. However, if capillary pressure is
defined as p c , the pressure at the center of
gravity of the Y-curve, the statement becomes exact, as equation 9 shows:
Whe
= peon, F =
0
Jl
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017
x,. = the pressure index of the capillaries
A word of caution is necessary. The Ycurve embraces all vessels contributing to
intraocular fluid production or removal. It
is quite possible that the several capillary
beds present in the eye occupy different
pressure regions. The idealized capillary
with pressure p c may not exist at all and
be only a mathematical construct, an
"equivalent capillary" summarizing and
averaging the properties of all the real
capillaries.
VI. Pseudofacility
Since, according to the assumptions, p v
= p i ; equation (8) shows that if intraocular and venous pressures are increased,
for instance as a result of a tonometer
being put onto the eye, F decreases. The
rate of change of F with pressure is
dpv
dpi
dpi
Since p., has been defined as the pressure
in a vessel where blood flow through the
eye has no influence, changes in intraocular pressure will also leave p., unaffected. Therefore,
dp,,
-r±- = 0 and equation 10 simplifies into
dF
(ID
dp,
Axc thus represents a rate of decrease in
filtration with increasing intraocular pressure. Its dimension is volume per unit time
and unit pressure rise, exactly as facility.
Axc can be termed "pseudofacility" if one
considers secretion to be pressure independent as is done in tonography or it can
be termed "ease of suppression of formation" or "ease of increase in reabsorption."
The possible existence of such a pressureproportional decrease in fluid formation
was discussed by Grant4 in his exposition
of tonography at the Third Macy Glaucoma
Conference.
It is interesting to note that pseudofacility increases with xc, the pressure index
Investigative Ophthalmology
December 1963
588 Bdrdny
of the capillaries. Since miotics are vasodilators, they can be expected to increase
xc. Moreover, it is conceivable that unfolding of the iris somewhat increases total
conductivity for filtration, A. It is therefore
possible that one component in the facilityincreasing action of miotics is their effect
on pseudofacility. Conversely, vasoconstrictor catecholamines should cause a drop in
pseudofacility.
Another special case is that of the patient with arterial hypertension. It is well
known that his intraocular pressure is
normal. Because of the diffuse increase in
arteriolar resistance he can be expected to
have a low xc and (assuming a normal A)
a low pseudofacility.
It is evidently important to know how
large pseudofacility is under various conditions. Direct experiments are still lacking.
An estimate for the rabbit eye is made
in Section VIII.
VII. Intraocular pressure as a function of
secretion, filtration, outflow facility, and
episcleral venous pressure
It is not known whether secretion from
the ciliary processes is markedly affected
by the hydrostatic pressure difference
across the epithelium. Certainly secretion
of fluid can go on without such a pressure
difference.5 If there is a dependence, it
would formally behave as filtration and
be taken care of by the composite conductivity coefficient Y. Hence, in the following, true secretion will be considered
pressure independent and its rate designated S. The symbol for episcleral venous
pressure will be p c and refers to vessels
so far downstream that their pressure is independent of aqueous flow.0 Conventional
outflow facility through the chamber angle
and associated veins is C. Filtration rate F
can be positive or negative, depending on
whether net production of aqueous or net
reabsorption occurs. With formula (8) a
positive sign means net production of
aqueous and one has
P.
=
(12)
P.
Inserting F from equation (8) into (12)
and rearranging gives equation (13) at the
bottom of the page.
This equation summarizes the influence
of all the factors taken into account in the
present treatment. It is seen that if the contribution of the vascular tree is neglected,
by putting A =0, the classical relation of
Goldmann2 between p^ pe, C, and S results.
VIII. Estimation of the size of pseudofacility
As a first approximation, one can consider episcleral venous pressure p 0 to be
independent of arterial pressure p,,. Secretion S and colloid-osmotic pressure p,:on
are also independent of this variable.
Hence, a change in arterial blood pressure
will act on intraocular pressure only
through the third term of equation (13)
and
iEL =
(14)
Simultaneous measurements in the conscious rabbit of changes in ophthalmic
artery pressure (by an indirect method)
and in intraocular pressure (by calibrated
tonometry) following unilateral carotid
ligation are available.1-7 The change in
steady state intraocular pressure was about
4 mm. Hg for a change in ophthalmic artery
blood pressure of 40 mm. Hg. Hence
0.1
C + Axe
Axc
C +
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017
(15)
Available tonographic measurements of
C embrace Axc and have given a value of
0.33 in the conscious rabbit.8 This then is
the denominator of expression (15) and
pseudofacility Axc in the rabbit under
physiologic conditions is of the order of
Axc
P< =
h
Axc
(13)
•y-
*y
Mathematical formulation of intraocular pressure 589
0.03 unit. Arteriolar dilatation could well
increase pseudofacility a few times, but
it is unlikely to become dominant as long
as the normal outflow channels at the angle
are patent.
No corresponding figures are available
for man. A study of the steady state effect
of an increase in episcleral venous pressure
on intraocular pressure should be possible
and would allow an estimate of pseudofacility to be made with the aid of the
second term of equation (13) which gives:
Ap,
_
(16)
Ap0 ~~ C
If the rise in p c in this experiment is
produced by a cuff around the neck or by
pressure breathing, it will be accompanied
by a rise in pressure in all the periocular
veins. It will then be necessary to limit the
change in venous pressure so that it keeps
well below resting intraocular pressure.
Too large a rise in venous pressure is transmitted to the intraocular veins and causes
a rise in intraocular pressure no longer
exclusively due to the rise in pc. Probably,
sufficient precision will be easier to obtain
in cases of glaucoma, where a considerable
venous pressure rise can be allowed, than
in normal subjects, in whom the permissible
rise is only a few millimeters of mercury.
IX. The pressure during angle-closure
While the factors determining filtration
(Pa, Pcoiij A, XC) perhaps play only a minor
role in an eye with normal C, they are
very important indeed in an eye with
blocked outflow at the chamber angle. If
C is made equal to zero in equation 13 one
obtains:
S - A'Proll
pi (with blocked angle) = p., +
Lx.
^—
(17)
The assumptions behind the derivation of
equation (13) certainly do not hold very
well for the large pressure changes in angle
closure, but equation (17) still should be
of interest. It indicates (not unexpectedly)
that even with a completely blocked angle,
the intraocular pressure will level off below
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017
mean arterial blood pressure, provided that
colloid-osmotic reabsorption Apcou exceeds
secretion S. If this is the case, the second
term of equation (17) is negative and decreases with increasing pseudofacility Axc.
If in this situation a vasodilating miotic is
given and does not succeed in freeing the
angle, the increase in pseudofacility will reduce the negative term and increase pressure, making the situation worse. This
seems to be in accord with clinical experience that strong miotics "add to the congestion."
X. Pressure effects of changes in arteriolar
tone
The pressure-increasing effect of vasodilatation just discussed makes it interesting to enquire under which conditions the
increase in pseudofacility Axc brought
about by vasodilatation outweighs the increased filtration of fluid. Does vasodilatation ever cause a decrease in pi?
The factors entering into the situation
become clearer on differentiation of pi in
equation (13) with respect to xc:
dp,
_
(C
- • [ C ( p » - p.) + A-p,.,, - S] (18)
With C in the normal range, about 0.3,
and p a - p c of the order of 10% the positive
terms inside the square brackets certainly
dominate by a wide margin, the differential
is positive, and intraocular pressure rises
with arteriolar vasodilatation. Only if C
becomes quite small and A-p,,,, is small
enough, the possibility arises for S to
dominate over the other terms. The expression then becomes negative and intraocular pressure drops with arteriolar vasodilatation. The conditions for this to happen
are the same as make for a very high
intraocular pressure and in fact it is easy to
show that the sign of the square bracket
changes from positive to negative only as
pt reaches and exceeds p.,.
Thus, changes in arteriolar tone occurring
in the normal or moderately high range of
intraocular pressures cause changes in pressure and in pseudofacility both in the same
estigntioe Ophthalmology
December 1983
590 Bdrdmj
direction. This simulates a homeostatic
adaptation with an increase in facility tending to counteract a rise in pressure.
Comments
Despite the simplifying assumptions on
which they are based, the relations derived
are probably not very far from the truth.
How important they are clinically is quite
another question, the answer to which will
have to wait until reliable estimates of A
and xc have been obtained for the human
eye under various conditions.
REFERENCES
1. Barany, E. H.: The influence of local arterial
blood pressure on aqueous humour and intraocular pressure. An experimental study of the
mechanisms maintaining intraocular pressure.
I. Intraocular pressure and local blood pressure
from seconds to hours after unilateral carotid
occlusion. A search for homeostatic reflexes
in the undisturbed eye, Acta ophth. 24: 337,
1946.
2. Coldmann, H.: Abflussdruck, Minutenvolumen
und Widerstand der Kammerwasserstromung
des Menschen, Docum. ophth. ('s. Grav.) 5-6:
278, 1951.
3. Auricchio, C , and Barany, E. H.: On the role
of osmotic water transport in the secretion of
the aqueous humour, Acta physiol. scandinav.
45: 190, 1959.
4. Grant, VV. M.: In Newell, F. W., editor:
Glaucoma, Tr. of the Third Conference, New
York, 1959, Josiah Macy, Jr. Foundation, pp.
19-20.
5. Berggren, L.: Unpublished, quoted by Barany,
E. H.: Pharmacology of aqueous humour
formation, in Uvniis, B., general editor: Proc.
First International Pharmacological Meeting,
Stockholm, 1961, vol. 4, p. 109, Oxford, 1963,
Pergamon Press, Inc.
6. Goldmann, H.: In Newell, F. W., editor:
Glaucoma, Tr. of the Second Conference, New
York, 1957, Josiah Macy, Jr. Foundation, pp.
207-210.
7. Barany, E. H.: The influence of local arterial
blood pressure on aqueous humour and intraocular pressure. An experimental study of the
mechanisms maintaining intraocular pressure.
II. The recovery of intraocular pressure, arterial
blood pressure, and heat dissipation by the
external ear after unilateral carotid ligation,
Acta ophth. 25: 81, 1947.
8. Becker, B., and Constant, M. A.: The facility
of aqueous outflow, A. M. A. Arch. Ophth.
56: 305, 1956.
Symbols
pOj
mean blood pressure in ophthalmic artery
or even more centrally
pc,
mean blood pressure corresponding to
center of gravity of area under Y-curve.
Loosely, capillary pressure
Pf.ni,
colloid-osmotic pressure of blood
pn,
episcleral venous pressure
pi,
intraocular pressure
pv,
pressure in intraocular veins at their
px,
a blood pressure between p,, and p v
x,
pressure index corresponding to p.*
point of exit from t h e ocular cavity
XK,
pressure- index of center of gravity of
area under Y-curve. Loosely, pressure
index of capillaries
Y,Y(x), conductivity coefficient for filtration of
the vascular wall
A,
C,
-V
total conductivity for filtration of the
vascular tree
facility of outflow through the chamber
angle and its associated veins
F,
S,
filtration
rate
secretion rate
V
Downloaded From: http://iovs.arvojournals.org/ on 06/17/2017