Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
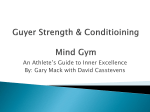
SportXXII, Science vol. 405 XXII, No. 5-6, December 2013 Sport Science Review, vol. no.Review, 5-6, 2013, - 415 DOI: 10.2478/ssr-2013-0020 Pre Participation Examination: Tool for Cardiovascular Screening of Competitive Athletes Kulroop KAUR BADWAL1 T he heart of an athlete has instilled inquisitiveness in many researchers, clinicians since a century. It is now well established that tedious physical training results in significant changes in cardiac structure and function. The recent increases in the number of people participating in recreational exercises and sports competitions have led to growing number of people exhibiting such changes. So the pre-participation screening becomes an important tool for non invasive examination and for diagnostic purposes. The main purpose of this consensus document is to reinforce the principle of the need for pre-participation medical clearance of all competitive athletes involved in organized sports programs, on the basis of (i) systematic screening by 12-lead ECG (in addition to history and physical examination) to identify hypertrophic cardiomyopathy - the leading cause of sportsrelated sudden death - and to prevent athletic field fatalities; (ii) transthoracic echocardiography with the potential ability of screening ability in detecting other lethal cardiovascular diseases. Keywords: Cardiovascular screening, sudden death, athletes 1 Department of Sports Medicine & Physiotherapy, Guru Nanak Dev University, Amritsar, Punjab, India ISSN: (print) 2066-8732/(online) 2069-7244 © 2013 • National Institute for Sport Research • Bucharest, Romania Unauthenticated Download Date | 6/18/17 3:05 AM 405 Tool for Cardiovascular Screening of Competitive Athletes Introduction Competitive athlete dying on a field is a tragedy having a great impact on the lay and medical personnel (Maron, 1993). Sudden deaths in competitive athletes are usually as a result of undiagnosed cardiovascular disease (Burke, 1991; Maron, 1996; Van Camp, 1995). Such events generally assume a high media and public profile because athletes are presumed to be healthy community. And they are also subject to practical and ethical issues related to the sports. This article is constituted to (1) increase the awareness of cardiovascular pre participation screening, (2) to assess the benefits and limitations of screening process, (3) to give effective recommendations and guidelines for practical, discreet and effective screening strategies. It is an endeavour which is seemingly important and relevant given the increasing number of competitive athletes taking part in sports worldwide, recent public health initiatives taken up by government on physical activity and exercise. Considerable interest has been raised regarding the role of pre-participation screening for early identification of those cardiovascular diseases which are responsible for athletic field deaths and for disqualification of athletes at risk, with the expectation that such a strategy may eventually prevent sudden death (Maron, 1987). Background The competitive athlete has been described as one who participates in an organized team or individual sport requiring systematic training and regular competition against others while placing a high premium on athletic excellence and achievement (Maron, 1994). The aim of pre participation screening is provide medical clearance or no objection certification for participation in competitive sports through routine and systematic evaluations anticipated to identify clinically relevant and preexisting cardiovascular abnormalities and thereby decrease the risks linked with sports. However, detection of a cardiac abnormality on screening examination is only the first step of recognition; follow up and referral to a cardiologist for further diagnostic investigations is sometimes required. From literature we can conclude that consensus panel guidelines of the 26th Bethesda Conference (Maron, 1994) should be used to formulate recommendations for continued participation or disqualification from competitive sports. The current guidelines primarily focus on population based screening of high school and collegiate, university level athlete’s rather individual assessments of athletes to elite level players and players of all ages and gender. These recommendations are particular important for participants of professional career based sports. Athletic training is likely to increase the risk for sudden cardiac death or disease progression in trained athletes is the formal base of these recommendations. The vast majority of athletes dying suddenly 406 Unauthenticated Download Date | 6/18/17 3:05 AM Sport Science Review, vol. XXII, No. 5-6, December 2013 on field or during training can be to extent controlled by the pre participation screening, by early detection of clinically significant diseases and allow timely therapeutic interventions that can decrease the incidence of such events. Causes of Sudden Death in Athletes A variety of cardiovascular abnormalities represent most common causes of sudden death in the competitive athletes (Corrado, 1990; Thiene, 1988; Tsung, 1982). The precise abnormalities of cardiac morphology leading to sudden death differ with age. The younger athletes show main cause of such incidence to be congenital abnormalities and malformations. About one third of cases show hypertrophic cardiomyopathy to be the predominant cause. The next most common seen are the congenital coronary anomalies like anomalous origin of left main coronary artery from the right sinus of valsalva (Cheitlin, 1974; Roberts, 1987). Coronary abnormalities have been found to be predominant cause of sudden death in team sports such as football and basketball which are considered to be high impact sports. Older athletes (35 years and above) represent an altogether different group as they usually participate in recreational sports rather than organized team sports. Atherosclerotic coronary artery disease has been found to be the major cause in this age group. Other causes such as cerebral aneurysm, nonpenetrating blunt chest impact (Maron, 1995) sickle cell trait, (Kark, 1987) and bronchial asthma are not considered here as this review focuses on athlete population. 407 Unauthenticated Download Date | 6/18/17 3:05 AM Tool for Cardiovascular Screening of Competitive Athletes Figure 1. Causes of sudden cardiac death in young competitive athletes (age 17), based on systematic tracking of 158 athletes in the United States, primarily from 1985 to 1995. Ao indicates aorta; LAD, left anterior descending coronary artery; AS, aortic stenosis; C-M, cardiomyopathy; ARVD, arrhythmogenic right ventricular dysplasia; MVP, mitral valve prolapse; CAD, coronary artery disease; HCM, hypertrophic cardiomyopathy; as shown in Maron et al . The precise abnormalities of cardiac morphology leading to sudden death differ with age. The younger athletes show main cause of such incidence to be congenital abnormalities and malformations. About one third of cases show hypertrophic cardiomyopathy to be the predominant cause. The next most common seen are the congenital coronary anomalies like anomalous origin of left main coronary artery from the right sinus of valsalva (Cheitlin, 1974; Roberts, 1987). Coronary abnormalities have been found to be predominant cause of sudden death in team sports such as football and basketball which are considered to be high impact sports. Older athletes (35 years and above) represent an altogether different group as they usually participate in recreational sports rather than organized team sports. atherosclerotic coronary artery disease has been found to be the major cause in this age group. Other causes such as cerebral aneurysm, nonpenetrating blunt chest impact (Maron, 1995) sickle cell trait, (Kark, 1987) and bronchial asthma are not considered here as this review focuses on athlete population. 408 Unauthenticated Download Date | 6/18/17 3:05 AM Sport Science Review, vol. XXII, No. 5-6, December 2013 Scope of the Problem Though sudden cardiac deaths are an infrequent event in sports tournaments but still screening has been found to be a useful precaution for same. And diseases like arrhythmogenic right ventricular dysplasia, long QT syndrome, or Marfan syndrome are rarely seen in population otherwise and so the reliable estimation techniques are lacking. The main obstacle to the screening process is the large number of athletes taking part in all the sports tournaments. From athletes to unspecified youth and children who take part in sports raise the number of participants to be increased to an alarmingly high level. The prevalence of the athletic field deaths reported are though less in number, the intense interest and increased awareness in sudden death in athletes is often fuelled by the media which gives a disproportionate augment to the actual numerical impact of sudden death being a public health problem. Legal considerations The educational institutions and professional sport tournaments and organizations are instructed to use reasonable care during conducting athletic programs. But still there is no clear legal model regarding duties or conduction of preparticipation screening of athletes to detect medical problems. And in the absence of strict abiding of rules and regulations established by law or by athletic governing bodies most institutions, academies rely on team physician or other medical personnel to determine appropriate screening procedures. A team physician who has medically cleared an athlete to participate in competitive sports is not necessary legally liable for an injury or death caused by an undiscovered cardiovascular condition. Failure to ascertain a latent asymptomatic cardiovascular condition by a physician due to malpractice requires a proof that the physician was deviated from the customary medical practice in his or her speciality in performing the screening of athletes and that the use of an established diagnostic criteria and methods which would have revealed the medical abnormality. To develop reliable diagnostic procedures in lieu of cost benefit and feasibility factors to establish the nature and scope of screening is a collective judgement of medical personnel. Ethical considerations A general accord in the society is that it is a responsibility of the physician to initiate appropriate efforts to identify the life threatening conditions in the athletes to minimize cardiovascular risk associated with participation in sports. There also appears an ethical obligation on behalf of educational institutions to conduct cost effective strategies to ensure that athletes are not at risk for 409 Unauthenticated Download Date | 6/18/17 3:05 AM Tool for Cardiovascular Screening of Competitive Athletes medical risks. Despite sufficient resources, it has been recognised that there is not high motivation among coaches, athletes or institutions to implement the screening procedures probably due to the economic pressures inherent in the sports environment. The extent to which the screening procedures can be supported at any level of cost efficiency considerations, awareness and practical limitations; it is not possible to attain a zero risk circumstance in sports. In a game or match, the athlete is prone to some kind of injury which cannot be avoided due to type of games and training involved, for e.g. in hockey and football, in which serious injuries can be a problem to athlete during the match. So it makes important to acknowledge limitations associated with the screening procedure in order to inform public which might otherwise harbor misconcepts about screening principles and its efficacy; and to offer guidance to physicians and medical personnel responsible for the process. Current Position of Pre-participation Screening There are no universally accepted and established standards for the screening procedures in schools, colleges, sports organizations and sports tournaments. There is also lack of certified health professionals who can perform the screening procedures. Some form of medical clearance by a physician by history and physical examination is necessary for the sportspersons participating regularly in sports. Some appropriate models of the preparticipation examination have been developed by a number of medical organizations and investigators (Dyment, 1991; Hulse, 1987; Durant, 1985). Prospects of Pre-participation Screening History and physical examination alone is not sufficient to guarantee detection of critical medical and cardiovascular conditions in large populations of competitive athletes. Heart murmur produced during aortic stenosis or hypertrophic cardiomyopathy can be detected during routine screening (Wigle, 1985; Maron, 1987a,b). Besides athletes with hypertrophic cardiomyopathy do not have family history of premature sudden death or syncope episode due to the disease. The standard procedure of history conveys low specificity for detection of cardiovascular diseases that might lead to sudden cardiac death during vigorous training or during field match. In older athletes personal history about coronary risk factors and family history of cardiac disease can be useful for identifying those athletes who are at risk. 410 Unauthenticated Download Date | 6/18/17 3:05 AM Sport Science Review, vol. XXII, No. 5-6, December 2013 Benefits and Precincts of Noninvasive Screening Tests The two-dimensional echocardiogram is the principal diagnostic tool for clinical recognition of hypertrophic cardiomyopathy, demonstrating otherwise unexplained asymmetric left ventricular wall thickening, the outcome of this disease (Maron, 1987a,b; Louie, 1994; Wigle, 1985). Echocardiography can also detect some other relevant abnormalities associated with sudden death in young athletes, such as valvular heart disease, left ventricular dysfunction (with myocarditis and dilated cardiomyopathy) and aortic root dilatation. However, even such diagnostic testing cannot guarantee identification of all important lesions. Another important limitation of screening with 2D echocardiography is the false positive or false negative results. Screening for hypertrophic cardiomyopathy with DNA testing for mutations in genes encoding proteins of the sarcomere is not yet practical or feasible for large populations, given the substantial genetic heterogeneity of the disease (Geisterfer, 1990; Tierfelder, 1994; Watkins, 1995). Arrhythmogenic right ventricular dysplasia (ARVD) usually cannot be reliably diagnosed solely with echocardiography and electrocardiography; the best available noninvasive test for this disease is magnetic resonance imaging, which is both expensive and not universally available (Ricci, 1992; McKenna, 1994). Electrocardiography has been found to be a useful tool for mass screening of cardiovascular abnormalities due to cost efficiency and non invasiveness. It is more practical and is used as an alternative to echocardiography in population based screening. In hypertrophic cardiomyopathy, the ECG has been found to be abnormal in 95% of cases; also changes are observed in coronary abnormalities. But it lacks imaging capability for recognition of cardiac morphological structural defects. It has low specificity as a screening test in athletic groups because of high frequency of ECG alterations in the trained competitive athletes due to physiological adaptation of the athlete’s heart to the sports training. Recommendations Noninvasive testing can enhance the diagnostic power accompanied by history and physical examination but it is unwise to recommend such tests like electrocardiography, echocardiography as routine advice. False positive results due to non invasive tests can cause anxiety in athletes, their peers and families. Hence it is recommended to take history and perform physical examination to identify cardiovascular abnormalities which are known to cause sudden cardiac death or disease progression with exercise training. It should be done from school and college level so as to have a longitudinal history of every athlete. It is recommended to follow one standard procedure for screening procedures that is officially recommended by all the governing sports organizations. A national standard procedure should be formed and followed considering nature and 411 Unauthenticated Download Date | 6/18/17 3:05 AM Tool for Cardiovascular Screening of Competitive Athletes scope of preparticipation medical evaluations. Coronary risk factors recognition in older athletes and their family history should be taken with immense care and without negligence to identify disease with screening. Exercise stress testing can be performed before initiating competitive or contact sports. Preparticipation sports examinations are performed by physicians or non-physician healthcare workers with different training and experience which can be unethical. It is recommended that athletic preparticipation screening should be performed by a physician having requisite training, medical skills to reliably obtain a detailed history, perform examination and recognize the underlying cardiac abnormalities. Blood pressure measurement should also be included in the screening procedure. The cardiovascular history should include questions designed to establish the (1) prior occurrence of exertional chest pain/discomfort or syncope/near-syncope, unexplained shortness of breath or fatigue associated with exercise; (2) past detection of a heart murmur or increased systemic blood pressure; and (3) family history of premature death (sudden or otherwise), or noteworthy disability from cardiovascular disease in close relative younger than 50 years old or specific knowledge of the occurrence of certain conditions (eg, hypertrophic or dilated cardiomyopathy). The cardiovascular physical examination should accentuate (1) precordial auscultation in both supine and standing positions to identify heart murmurs consistent with dynamic left ventricular outflow obstruction; (2) brachial blood pressure measurement in the sitting position; (3) recognition of the physical stigmata of Marfan syndrome; and (4) assessment of the femoral artery pulses to exclude coarctation of the aorta. As mentioned above, when cardiovascular morphological diseases or abnormalities are suspected or identified, the athlete has to be referred to a cardiovascular specialist for further testing procedures done by expert for evaluation and confirmation. The identified cardiovascular abnormalities should be judged with respect to the 26th Bethesda Conference consensus panel guidelines for the final recommendation of eligibility for future athletic competition (Maron, 1994). References Burke, A. P., Farb, A., Virmani, R., Goodin, J. & Smialek, J. E. (1991). Sportsrelated and non-sports-related sudden cardiac death in young adults. Am Heart J., 121, 568-575. Cheitlin, M. D., De Castro, C. M., & McAllister, H. A. (1974). Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva: a not-so-minor congenital anomaly. Circulation, 50, 780-787. 412 Unauthenticated Download Date | 6/18/17 3:05 AM Sport Science Review, vol. XXII, No. 5-6, December 2013 Corrado, D., Thiene, G., Nava, A., Rossi, L., & Pennelli, N. (1990). Sudden death in young competitive athletes: clinicopathologic correlations in 22 cases. Am J Med., 89, 588-596. Durant R. H., Seymore, C., Linder, C. W., & Jay, S. (1985). The preparticipation examination of athletes: comparison of single and multiple examiners. Am J Dis Child, 139, 657-661. Dyment P. G. (1991). Sports Medicine: Health Care for Young Athletes (2nd ed.) Elk Grove Village, Ill: American Academy of Pediatrics. Geisterfer-Lowrance, A. A., Kass, S., Tanigawa, G., Vosberg, H. P., McKenna, W., Seidman, C. E., & Seidman, J. G. (1990). A molecular basis for familial hypertrophic cardiomyopathy: a β-cardiac myosin heavy chain gene missense mutation. Cell., 62, 999-1006. Hulse, E., & Strong, W. B. (1987). Preparticipation evaluation for athletes. Pediatr Rev., 9, 173-182. Kark, J. A., Posey, D. M., Schumacher, H. R., & Ruehle, C. J. (1987). Sickle-cell trait as a risk factor for sudden death in physical training. N Engl J Med, 317, 781-787. Louie, E. K., & Edwards, L. C. (1994). Hypertrophic cardiomyopathy. Prog Cardiovasc Dis, 36, 275-308. Maron, B. J., Bonow, R. O, Cannon, R. O. III, Leon, M. B., & Epstein, S. E. (1987). Hypertrophic cardiomyopathy: interrelations of clinical manifestations, pathophysiology, and therapy, 1. N Engl J Med, 316, 780-789 Maron, B. J., Bonow, R. O, Cannon, R. O. III, Leon, M. B., & Epstein, S. E. (1987). Hypertrophic cardiomyopathy: interrelations of clinical manifestations, pathophysiology, and therapy, 2. N Engl J Med, 316, 844-852. Maron, B. J., & Garson, A. (1994). Arrhythmias and sudden cardiac death in elite athletes. Cardiol Rev, 2, 26-32. Maron, B. J., Isner, J. M., & McKenna, W. J. (1994). 26th Bethesda Conference: recommendations for determining eligibility for competition in athletes with cardiovascular abnormalities. Task Force 3: hypertrophic cardiomyopathy, myocarditis and other myopericardial diseases and mitral valve prolapse. J Am Coll Cardiol, 24, 880-885. 413 Unauthenticated Download Date | 6/18/17 3:05 AM Tool for Cardiovascular Screening of Competitive Athletes Maron, B. J., Poliac, L., Kaplan, J. A., & Mueller, F. O. (1995). Blunt impact to the chest leading to sudden death from cardiac arrest during sports activities. N Engl J Med, 333, 337-342. Maron, B. J., Roberts, W. C., McAllister, H. A., Rosing, D. R., & Epstein, S. E. (1980). Sudden death in young athletes. Circulation, 62, 218-229. Maron, B. J., Shirani, J., Poliac, L. C., Mathenge, R., Roberts, W. C., & Mueller, F. O. (1996). Sudden death in young competitive athletes: clinical, demographic and pathological profiles. JAMA, 276, 199-204. Maron, B. J. (1993). Sudden death in young athletes: lessons from the Hank Gaithers affair. N Engl J Med, 329, 55-57. Maron, B. J., Bodison, S. A., Wesley, Y. E., Tucker, E. & Green, K. J. (1987) Results of screening a large group of intercollegiate competitive athletes for cardiovascular disease. J Am Coll Cardiol, 10, 1214–1221. McKenna, W. J., Thiene, G., Nava, A., Fontaliran, R., Blomstrom-Lundqvist, C., Fontaine, G., & Camerini, F. (1994). On behalf of the Task Force of the Working Group for the Myocardial and Pericardial Disease of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the International Society and Federation of Cardiology. Diagnosis of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Br Heart J, 71, 215-218. Ricci, C., Longo, R., Pagnan, L., Dalla Palma, L., Pinamonti, B., Camerini, F., Bussani, R., & Silvestri, F. (1992). Magnetic resonance imaging in right ventricular dysplasia. Am J Cardiol, 70, 1589-1595. Roberts, W. C. (1987). Congenital coronary arterial anomalies unassociated with major anomalies of the heart or great vessels. In: Adult Congenital Heart Disease (p. 583). Philadelphia, Pa: FA Davis Co. Thiene, G., Nava, A., Corrado, D., Rossi, L., & Pennelli, N. (1988). Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med, 318, 129-133. Thierfelder, L., Watkins, H., MacRae, C., Lamas, R., McKenna, W., Vosberg, H. P., Seidman, J. G., & Seidman, C. E. (1994). α-Tropomyosin and cardiac troponin T mutations cause familial hypertrophic cardiomyopathy: a disease of the sarcomere. Cell, 77, 701-712. 414 Unauthenticated Download Date | 6/18/17 3:05 AM Sport Science Review, vol. XXII, No. 5-6, December 2013 Van Camp, S. P., Bloor, C. M., Mueller, F. O., Cantu, R. C., & Olson, H. G. (1995). Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc, 27, 641-647. Watkins, H., Conner, D., Thierfelder, L., Jarcho, J. A., MacRae, C., McKenna, W. J., Maron, B. J., Seidman, J. G., & Seidman, C. E. (1995). Mutations in the cardiac myosin binding protein-C gene on chromosome 11 cause familial hypertrophic cardiomyopathy. Nat Genet, 11, 434-437. Wigle, E. D., Sasson, Z., Henderson, M. A., Ruddy, T. D., Fulop, J., Rakowski, H., & Williams, W. G. (1985). Hypertrophic cardiomyopathy: the importance of the site and extent of hypertrophy—a review. Prog Cardiovasc Dis, 28, 1-83. Kulroop KAUR BADWAL, M.B.B.S., is working as final junior resident of M.D. Sports Medicine in the Department of Sports Medicine and Physiotherapy at Guru Nanak Dev University, Amritsar, Punjab, India. She received her Bachelor’s degree in M.B.B.S. (Bachelor of Medicine & Bachelor of Surgery) from Baba Farid University of Health and Medical Sciences, Faridkot, Punjab, India. Her area of interest is Sports Medicine, Cardiology, Sports injury and Research Education. Currently she is working on research project titled “Association of Body Composition and Heart Structural Changes in Endurance, Strength and Combined Trained Athletes”. Dr. Kulroop Kaur Badwal is also working on a variety of projects in both the sports and community health fields. Corresponding address: Kulroop KAUR BADWAL Guru Nanak Dev University, Faculty Of Sports Medicine And Physiotherapy GT Road, Amritsar, Punjab, India - 143005 Phone: 09781500976 Email: [email protected] 415 Unauthenticated Download Date | 6/18/17 3:05 AM Unauthenticated Download Date | 6/18/17 3:05 AM