Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
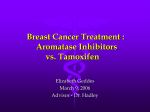
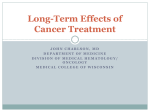
Annals of Oncology 11: 1017-1022. 2000. © 2000 Kluwer Academic Publishers. Printed in the Netherlands Original article Tumor response and estrogen suppression in breast cancer patients treated with aromatase inhibitors E. Bajetta,1 N. Zilembo,1 E. Bichisao,2 A. Martinetti,1 R. Buzzoni,1 P. Pozzi,1 P. Bidoli,1 L. Ferrari1 & L. Celio1 'Division of Medical Oncology Unit B, Istituto Nazionale per lo Studio e la Cura det Tumori; 2Italian Trials in Medical Oncology (1TM0) Group, Milan, Italy levels, with a decrease in the levels of both hormones irrespective of any antitumor response. In particular, the degree of Background: The rationale for the hormonal treatment of breast plasma estrogen suppression was similar in the patients who cancer (BC) is based on depriving tumor cells of estrogenic experienced a complete remission and those with progressive stimulation. Aromatase inhibitors (AIs) block the conversion disease (PD). of peripheral tissue androgens to estrogens with different levels Conclusions: The plasma estrogen suppression induced by of potency. In an attempt to investigate the relationship be- aromatase inhibition is not the only mechanism accounting for tween tumor response and estrogen suppression, we reviewed its clinical activity. Many clinical trials have demonstrated that the hormonal and clinical data of two previous studies with all AIs induce a similar antitumor response regardless of their formestane (250 and 500 mg i.m. fortnightly) in advanced BC potency, and further investigations are warranted in order to patients. improve our understanding as to why the patients with PD also Patients and methods: Two hundred four BC patients were show a significant plasma estrogen suppression. It is possible selected on the basis of the availability of records concerning that intratumoral aromatase activity may be a marker for their plasma estrone (El) and estradiol (E2) levels assessed at selecting the BC patients most likely to respond to AI treatscheduled times. The degree of estrogen suppression and the ment. best clinical response of each patient during the trials were considered. Results: There was a positive and significant (P < 0.05) Key words: aromatase inhibitors, tumour response, plasma correlation between baseline and post-formestane El and E2 estrogen suppression Summary Introduction Although the ovarian production of steroids declines in postmenopausal women, the peripheral synthesis of estrogens increases in fat, muscle and liver tissues, and thus becomes the major contributor to circulating estrogen levels. It is widely accepted that at least one-third of breast cancer tumors in women is induced and sustained by estrogens, and so the rationale for hormonal treatment is based on depriving tumor cells of estrogenic stimulation. There are currently two main pharmacological approaches towards reducing the effects of estrogens on tumor cells: the administration of antiestrogens (such as tamoxifen) that interact with estrogen receptors inside the tumor, or the use of aromatase inhibitors that block the conversion of androgens to estrogens in peripheral tissues [1, 2]. The aromatase inhibitors have varying degrees of potency in inhibiting in vivo aromatisation [3, 4]. Jones et al. [5] demonstrated that formestane inhibits peripheral aromatase activity by 85%-92%, but Geisier et al. [6] have more recently shown that exemestane suppresses aromatisation by 98%, which is the same level of suppression induced by anastrozole and letrozole [7, 8]. Furthermore, it is known that there is a consistency between the degree of aromatisation and plasma estrogen suppression, although the detection limits of the assay make it difficult to assess plasma estrogen levels in postmenopausal women [9]. In any case, no direct relationship between clinical response and plasma estrogen levels during aromatase inhibitor treatment has yet been demonstrated [4], and there is no evidence that greater potency leads to a better clinical response in breast cancer patients. In fact, the clinical results of recent multicentre clinical trials of steroidal and non-steroidal aromatase inhibitors have shown that both are more active than megestrol acetate, but there is no difference between them in terms of antitumor activity and tolerability [10-14]; consequently no aromatase inhibitor can be considered the drug of choice [15, 16]. There are no published data directly comparing the activity of the new aromatase inhibitors with each other, and only letrozole [17] and vorozole [18] 1018 have been shown to be more active than aminoglutethimide (AG). No difference in the response rate between letrozole and AG or in the overall response rate between vorozole and AG has been observed, and it is difficult to understand whether the more powerful effects of letrozole on time to progression, time to treatment failure or overall survival, or of vorozole in terms of clinical benefit, are actually due to the fact that they are more potent than AG. In an attempt to investigate the relationship between tumor response and plasma estrogen suppression, we reviewed the hormonal and clinical data of two previous studies with formestane in breast cancer patients. Table 1. Antitumor response rates to aromatase inhibitors observed in trials versus megestrol acetate (patients unassessable for antitumor response have not been considered in this table). CR, Non-steroidal aromatase inhibitors 11(4) Anastrozole 1 mg Letrozole 2.5 mg 12(7) Vorozole 2.5 mg 5(2) Steroidal aromatase inhibitors Formestane 250 mg 5(6) 8(2) Exemestane 25 mg PR, SD, PD. 22(8) 29(17) 15(7) 79(30) 151(58) 19(11) 93(53) 40(19) 130(63) 10(11) 47(13) 41(45) 149(41) 34(37) 128(35) Abbreviations: CR - complete response; PR - partial response; SD stable disease; PD - progressive disease. Patients and methods In 1994 and 1997, we published two papers reporting the endocnnological and clinical results of two formestane doses (250 and 500 mg i.m. fortnightly) randomly given to postmenopausal advanced breast cancer patients. Patient selection The first study [19] involved 143 patients pre-treated for advanced disease (72 receiving 250 mg; and 71 receiving 500 mg), and the second study [20] 152 patients at first relapse (73 on 250 mg and 79 on 500 mg) Briefly, the eligibility criteria of each study were an age of < 80 years, postmenopausal status, measurable disease, a positive or unknown estrogen receptor status (in the latter case, a disease-free interval of more than 2 years was required), and a performance status <2 (ECOG scale). In agreement with the guidelines of the local Bio-Ethics Committee, all of the patients gave their informed consent before starting treatment according to the rules in force at the time. Detailed information concerning all of the patients is available in the original publications. For the present analysis, the patients were selected on the following basis: • clinical response (patients were not considered if they had progressed before the first evaluation); • the availability of estrogen values (E2 levels in the first study; E2 and El levels in the second). Hormonal measurements The plasma estrogen levels were considered separately and not pooled, because each study used a different analytical method. In the first study, plasma E2 levels were measured by means of RI A, in the second plasma E2 and El levels were evaluated using a new method consisting of solid phase extraction followed by RIA. The estrogen assays in each study were repeated in order to confirm the results. Detailed information concerning the analytical methods is available in the original publications. As both studies demonstrated that the maximum suppression of plasma estrogens induced by formestane was reached after an average of 15 days of treatment, and that there was no significant decrease thereafter, we have here considered only the baseline levels and those measured after 12 (first study) or 10 weeks (second study), when the first tumor response evaluations were made. Tumor response Tumor response was evaluated in both trials according to UICC criteria by means of physical examinations, bone scans, chest and skeletal X-rays, and liver echography or computed tomography. These examinations were performed at the beginning of each study, after 12 (first study) or 10 weeks (second study), and then every 12 weeks. Statistical analysis Spearman's correlation coefficient (r) between the baseline and posttreatment plasma E2 and El levels was calculated. The plasma estrogen suppression and best clinical response of each patient during the trials were considered, strictly following the response criteria used in each trial. The data are reported as median or mean values (±SD or SEM), together with their 95% confidence limits (95% CI). A /"-value of 0.05 was considered significant for evaluating differences. Results This analysis involved a total 204 breast cancer patients. Ninety-one patients with a median age offifty-nineyears (range 45-75) were selected from the first study on the basis of the availability of plasma E2 levels: forty-eight patients received formestane 250 mg and forty-three formestane 500 mg. In the case of the second study, 113 patients with a median age of 62 years (range 38-80), were selected on the basis of the availability of plasma E2 levels (51 patients received formestane 250 mg and 62 formestane 500 mg), and 110 patients with a median age of 62 years (range 38-80) were selected on the basis of the availability of plasma El levels (53 patients received formestane 250 mg and 57 formestane 500 mg). Plasma estrogen suppression A significant (P < 0.05) positive correlation was found between the baseline and post-treatment El and E2 levels (first study: E2 r - 0.73 and 0.62 for 250 and 500 mg, respectively; second study: E2 r - 0.34 and 0.54 for 250 and 500 mg, respectively, El /• = 0.40 and 0.69). Although the correlation coefficients are not very high, they confirm the pharmacological efficacy of formestane and are in agreement with the previously reported results analysed by means of ANOVA for repeated measure- 1019 Table 2 First study: E2 (pg/ml) suppression (mean values ± SD and 95% CI) and clinical response, by formestane dose. 500 mg 250 mg No. CR 6 PR 8 SD 4 PD 30 Baseline 250 mg group Twelve weeks 7.3 ±3.5 4.3 ± 2.4 (4.4-10.1) (2.4-6.2) 5.7 ± 1.7 2.8 ±0.9 (4.5-6.8) (2.2-3.4) 4.3 ±0.8 2.5 ±0.9 (3.5-5.1) (1 6-3 4) 5.6 ± 1.8 3.6 ± 1.3 (4.9-6.3) (3.2-4.1) No. Baseline a Twelve weeks 8 7.2 ±3.6 13 (4.7-9.7) 6.1 ±2.4 (4.8-7.3) 3.3 ±0.9 (2.6-4.0) 3.5± 1.1 (2.9-4.1) 2.6 (-) 3 (-) 5.9 ±1.9 (5.0-6.7) 2.9 + 0.9 (2.5-3.2) 1 21 7 _J 6 1. 3 2 500 mg group Table 3. Second study: E2 (pg/ml) suppression (mean values ± SD and 95% Cl) and clinical response, by formestane dose. 250 mg No. Baseline 500 mg Ten No. Baseline weeks CR 8 PR 7 SD 23 PD 13 7.7 ±3.4 (5.3-10 0) 5.8 ± 1.6 (4.6-7-0) 6.2 ±3.1 (4.9-7.5) 6.4 ± 1 9 (5.3-7.4) 5.1 ±5.2 (1.5-8.7) 3.3 ± 1.8 (1.9-4.7) 3 6±2.8 (2.4-4.7) 2.8 ±0.8 (2.4-3 3) Ten weeks 11 15 23 13 6.3 ±2.5 (4.8-7.8) 9.4 ± 6.4 (6.1-12.6) 6.4 + 2.7 (5.3-7.5) 5.2 ± 2.4 (3.8-6.5) 2.6±1.2 (1 9-3.4) 3.713.0 (2.2-5 2) 2.2 ±0.8 (1.8-2.5) 2.1 ±0.7 (1.7-2.4) Table 4 Second study: El (pg/ml) suppression (mean values ± SD and 95% CI) and clinical response, by formestane dose. 250 mg 500 mg weeks - Complete Response - Progression Figure 1. First study: E2 suppression in patients with CR and PD (mean 1 SEM). more effective than the 250 mg dose, but this difference was not statistically significant. No. Baseline Ten weeks No. Baseline Ten weeks Table 3 shows the mean E2 values after 10 weeks of CR 8 41.4 ± 14.9 27.3 1 17.9 10 33.0 ±11.0 19.2 ±4.3 treatment with formestane 250 mg in patients achieving (31.0-51.8) (14.9-39.8) (22.0-44.0) (16.3-22.0) a complete response (CR), and deserves some comments. PR 7 35.2 ± 11.4 20 6 ±4.9 15 42.4 ±23.9 25.71 13.6 The mean values at baseline and after 10 weeks were (26.7-43.6) (16.9-24.3) (30.2-54.4) (18.9-32.6) respectively 7.7(± 3.4) and 5.1(±5.2) pg/ml: the high SD 24 33.8 ± 13.9 22.218.7 20 36.9113.5 21.618.2 (30.9-42.8) (17.9-25.1) standard deviation is due to the fact that one patient (28.3-39.4) (18.7-25.7) PD 14 36.6 ±8.9 19.3 ±7.3 12 28.3 112.2 17.717.6 (aged 63 years) had 6.6 pg/ml at baseline and 17.5 pg/ml (21.3-35.2) (13.4-22.1) after treatment. Similarly, a 53-year-old patient with (31.9-41.3) (15.5-23.1) stable disease experienced an increase from 8.3 pg/ml to 13.8 pg/ml. Table 4 shows the mean (± SD and 95% CI) El levels ments. It is likely that between-patient variability accounts for this low correlation rate, which suggests that observed in the second study; there was a significant baseline estrogen values are poor predictors of plasma suppression of plasma El levels in both treatment groups, and the formestane doses seem to be equally estrogen suppression. effective. Figures 1 and 2 show the direct comparison between Clinical response according to plasma estrogen suppression the degree of plasma E2 suppression in the patients achieving CR and in those experiencing progressive Tables 2 and 3 show the clinical response according to disease (PD), which was chosen because CR and PD the mean E2 levels (±SD and 95% CI) observed at should be the most reliable antitumor responses. The baseline and after 12 (first study) and 10 weeks (second degree and trend of plasma estrogen suppression in these study). Plasma estrogen suppression was significant in two groups of patients was similar regardless of the all of the treatment groups; the 500 mg dose seems to be response. 1020 250 mg group weeks 500 mg group weeks - Complete Response - Progression Figure 2 Second study: E2 suppression in patients with CR and PD (mean ± SEM). It is worth noting that (as shown in Table 2), the baseline E2 levels are lower in the CR than in the PD patients. However, the number of patients with CR is smaller, and so no direct comparison can be made; when the number of patients with CR and PD increases (as shown in Table 3), the E2 levels become more similar. Furthermore, given the range of SEM in Figures 1 and 2, it is clear that baseline estrogen levels are not different between the two patient groups. Discussion Our analysis shows that the suppression of plasma estrogens is not the only mechanism responsible for the antitumor response induced by formestane, a finding that is in line with the clinical evidence that all aromatase inhibitors are equally useful in the treatment of advanced breast cancer patients (Table 1), regardless of their suppressive potency. A comparison of the endocrine effects of formestane (steroidal) and anastrozole (non-steroidal) has recently been made in 60 postmenopausal advanced breast cancer patients [21]. Anastrozole led to a significantly greater mean suppression of E2 levels (P - 0.0001) than formestane (79% vs. 58%), and a similar result was observed in the case of El and E1S. The curve of estrogen suppression induced by formestane was similar to that previously reported in the literature [5,19, 22], and there are still some concerns as to the optimal dose to be used in clinical practice. The antitumor response rate was no different between the two treatment groups (17% and 10%, P = 0.482 ns), and clearly demonstrates that both agents are effective despite the difference in the degree of plasma estrogen suppression, as the authors themselves pointed out: "The clinical significance of these differences in total oestrogen suppression remains to be established." The baseline estrogen levels considered in our analysis do not appear to predict clinical response, as is also clearly demonstrated by the results of two clinical trials designed to identify the optimal dose of exemestane [23, 24]. The key problem is why some breast cancer patients do not respond to treatment with aromatase inhibitors, despite a significant reduction in estrogen levels, and the presence of all of the standard requirements for hormonal treatment. It is likely that this resistance is due to some still unidentified specific characteristics of the tumour, and biological reasons may account for the absence of any relationship between clinical response and estrogen suppression. Experimental models have demonstrated [25] that tumor cells can adapt themselves to very low estrogen levels, and so even a high degree of estrogen suppression may be inadequate because the stimulation induced by the residual low levels could lead to resistance over time. Furthermore, peripheral tissues are not the only source of estrogens in postmenopausal women because breast cancer tissue itself is an endocrine organ. The cell concentrations of El, E2 and estrone sulphate (E1S) may be higher than those in the circulation as a result of local production factors, including aromatisation [26, 27], and the synthesis of El via the estrone sulphatase and estradiol dehydrogenase pathways may be the major supply route of estrogen to the tumor [28]. A number of investigations concerning intratumoral aromatase activity are currently ongoing [29], some of which have found that formestane [30] and vorozole [31] are capable of significantly suppressing intratumoral aromatase activity in breast cancer patients (by an average of 80%); however, little information is available in the case of anastrozole [32] and letrozole [33]. It is also worth noting that a correlation between tumor aromatase activity and the response to AG was observed in a study of 29 advanced breast cancer patients [34]. The tumor aromatase values in the responders were significantly higher than in the non-responders, with 10 of 14 patients (71%) having values of more than 0.5 pmol ER produced/mg protein/h responding to the therapy as against 0 of 15 patients with lower values. These results have been confirmed by another trial in which none of the five patients with aromatase-negative tumors responded, as against 11 of 18 patients (61%) with aromatase-positive cancers [35]. The real significance of intratumoral aro- 1021 matase activity in breast cancer patients is still unclear, as is the role played by aromatase inhibitors in suppressing or modulating this activity. An assay evaluating intratumoral aromatase activity in surgically excised breast tissue could lead to the identification of a marker for targetting patients suitable for treatment with aromatase inhibitors (as is routinely done in the case of estrogen receptors) especially in an adjuvant setting, and may also help to differentiate these drugs from each other. In conclusion, there is evidence indicating that plasma estrogen suppression per se is not the only mechanism accounting for the antitumor activity of aromatase inhibitors, and that it is not associated with tumor response. There is a need to be able to target responsive breast cancer patients in order to ensure a higher rate of disease control, and avoid the use of aromatase inhibitors in unsuitable patients. The routine assessment of intratumoral aromatase activity by means of a specific assay could be an interesting challenge for the future. 12. 13. 14. 15. 16. 17. Acknowledgements 18. The authors would like to thank the Scientific Service of the Italian Trials in Medical Oncology (ITMO) Group for its editorial assistance. 19. 20. References 1. Brodie AMH, Njar VCO. Aromatase inhibitors and breast cancer. Semin Oncol 1996; 23: 10-20. 2. Buzdar AU, Plourde PV. Hortobagyi GN. Aromatase inhibitors in metastatic breast cancer. Semin Oncol 1996; 23: 28-32. 3. Lonning PE. Aromatase inhibition for breast cancer treatment. Acta Oncol 1996; 35: 38-43. 4. Dowsett M. Biological background to aromatase inhibition. Breast 1996; 5: 196-201. 5. Jones AL. Mac Neill F, Jacobs S et al. The influence of intramuscular 4-hydroxyandrostenedione on peripheral aromatisation in breast cancer patients. Eur J Cancer 1992; 28A: 1712-6. 6. Geisler J, King N, Anker G et al. In vivo inhibition of aromatization by exemestane, a novel irreversible aromatase inhibitor, in postmenopausal breast cancer patients. Clin Cancer Res 1998; 4: 2089-93. 7 Geisler J, King N. Dowsett M et al. Influence of anastrozole (Arimidex), a selective, non-steroidal aromatase inhibitor, on in vivo aromatisation and plasma oestrogen levels in post-menopausal women with breast cancer. Br J Cancer 1996; 74: 1286-91. 8. Dowsett M, Jones A, Johnston SRD et al. In vivo measurement of aromatase inhibition by letrozole (CGS 20267) in postmenopausal patients with breast cancer. Clin Cancer Res 1995; 1: 1511-5. 9. Lonning PE. Pharmacology of new aromatase inhibitors. Breast 1996; 5: 202-8. 10. Buzdar A, Jonat W, Howell A et al. Anastrozole, a potent and selective aromatase inhibitor, versus megestrol acetate in postmenopausal women with advanced breast cancer: Results of an overview analysis of two phase III trials. J Clin Oncol 1996; 14: 2000-11. 11. Dombernowsky P, Smith I, Falkson G et al. Letrozole, a new oral aromatase inhibitor for advanced breast cancer: Double-blind randomized trial showing a dose effect and improved efficacy and 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. tolerability compared with megestrol acetate. J Clin Oncol 1998. 16: 453-61. Thurlimann B, Castiglione M, Hsu-Schmitz SF et al. Formestane versus megestrol acetate in postmenopausal breast cancer patients after failure of tamoxifen: A phase III prospective randomised cross over trial of second-line hormonal treatment (SAKK 20/90), Eur J Cancer 1997; 33: 1017-24. Goss PE, Winer EP, Tannock IF. Schwartz LH. Randomized phase III trial comparing the new potent and selective thirdgeneration aromatase inhibitor vorozole with megestrol acetate in postmenopausal advanced breast cancer patients. North America Vorozole Study Group. J Clin Oncol 1999: 17: 52-63. Kaufmann M, Bajetta E, Dirix LYet al. Exemestane is superior to megestrol acetate after tamoxifen failure in postmenopausal women with advanced breast cancer: Results of a phase III randomized double blind trial. J Clin Oncol 2000; 18. 1399-411. Castiglione-Gertsch M. New aromatase inhibitors: More selectivity, less toxicity, unfortunately, the same activity. Eur J Cancer 1996, 32A: 393-5. Hamilton A, Piccart M. The third-generation non-steroidal aromatase inhibitors: A review of their clinical benefits in the secondline hormonal treatment of advanced breast cancer. Ann Oncol 1999; 10: 377-84. Gershanovich M, Chaudri HA, Campos D et al. Letrozole, a new oral aromatase inhibitor. Randomised trial comparing 2.5 mg daily, 0.5 mg daily and aminoglutethimide in postmenopausal women with advanced breast cancer. Ann Oncol 1998; 9: 639-45. Bergh J, Bonneterre J, Illiger HJ et al. Vorozole (Rivizor®) versus aminoglutethimide (AG) in the treatment of postmenopausal breast cancer relapsing after tamoxifen. Proc ASCO 1997; 16: 155a (Abstr 543). Bajetta E, Zilembo N, Buzzoni R et al. Endocrinological and clinical evaluation of two doses of formestane in advanced breast cancer. Br J Cancer 1994, 70: 145-50. Bajetta E, Zilembo N, Barni S et al. A multicentre, randomized, pharmacokinetic, endocrine and clinical study in breast cancer patients at first relapse: Endocrine and clinical results. Ann Oncol 1997; 8- 649-54. Vorobiof DA, Kleeberg UR, Perez-Carrion R et al. A randomized, open, parallel-group trial to compare the endocrine effects of oral anastrozole (Arimidex®) with intramuscular formestane in postmenopausal women with advanced breast cancer. Ann Oncol 1999; 10: 1219-25. Coombes RC, Huges SWM, Dowsett M. 4-hydroxyandrostenedione: A new treatment for postmenopausal patients with breast cancer. Eur J Cancer 1992, 28A: 1941-5. Zilembo N, Noberasco C, Bajetta E et al. Endocrinological and clinical evaluation of exemestane, a new steroidal aromatase inhibitor. Br J Cancer 1995; 72: 1007-12. Bajetta E, Zilembo N, Noberasco C ct al. The minimal effective exemestane dose for endocrine activity in advanced breast cancer. Eur J Cancer 1997; 33: 587-91. Masamura S, Santner SJ. Heitjan DF, Santen RJ. Estrogen deprivation causes estradiol hypersensitivity in human breast cancer cell. J Clin Endocrinol Metab 1995; 80: 2918-25. Pasqualini JR, Chetrite G, Blacker C. Feinstein MC et al. Concentrations of estrone, estradiol and estrone sulphate, and evaluation of sulphatase and aromatase activities in pre- and postmenopausal breast cancer patients. J Clin Endocrinol Metab 1996; 81; 1460-4. Blankenstein MA, van de Ven J, Maitimu-Smeele I, Donker GH et al. Intratumoral levels of estrogens in breast cancer. J Steroid Biochem Mol Biol 1999; 69: 293-7. Purhoit A, Wang DY, Ghilchik MW, Reed MJ. Regulation of aromatase sulphatase in breast tumor cells. J Endocrinol 1996; 150: S65-71. Miller WR, Mullen P, Telford J, Dixon JM. Clinical importance of intratumoral aromatase. Breast Cancer Res Treat 1998; 49: S27-32. Reed MJ, Aherne GW. Ghilchik MW et al. Concentrations of 1022 31. 32. 33. 34. estrone and 4-hydroxyandrostenedione in malignant and normal breast tissue. Int J Cancer 1991, 49: 562-5. de Jong PC, van de Ven J, Nortier HW et al. Inhibition of breast cancer tissue aromatase activity and estrogen concentrations by 1 b ' the third-generation aromatase inhibitor vorozole. Cancer Res 1997; 57: 2109-11. Geisler J, Bernsten H, Ottestad L et al. Neoadjuvant treatment with anastrozole (Anmidex) causes profound suppression of intra-tumor estrogen levels. ProcASCO 1999; 18: 82a (Abstr 311). Brodie A, Lu Q, Yue Wet al. Intratumoral aromatase model: The effects of letrozole (CGS 20 267). Breast Cancer Res Treat 1998; 49 (Suppl 1): S23-6. Bezwoda WR, Mansoor N, Dansey R. Correlation of breast tumor aromatase activity and response to aromatase inhibition with aminoglutethimide. Oncology 1987; 44: 345-9. 35. Miller WR, O'Neill J. The importance of local synthesis of estrogen within the breast. Steroids 1987; 50: 537-48. „ •.,-,., . -,r>™ , -.-• • ->n™ Received 17 March 2000: accepted 27 June 2000. Correspondence to. E. Bajetta, MD Division of Medical Oncology Unit B Istituto Nazionale per lo Studio e la Cura dei Tumori via Venezian 1 20133 Milano Italy E-mail' [email protected]