Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gene therapy of the human retina wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Herpes simplex research wikipedia , lookup
Antimicrobial resistance wikipedia , lookup
Gene therapy wikipedia , lookup
Public health genomics wikipedia , lookup
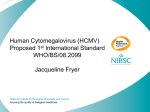
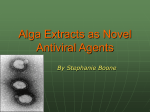
Journal of Antimicrobial Chemotherapy (2003) 52, 324–330 DOI: 10.1093/jac/dkg354 Advance Access publication 29 July 2003 Human cytomegalovirus resistance to antiviral drugs: diagnosis, monitoring and clinical impact Fausto Baldanti1,2 and Giuseppe Gerna1* 1Servizio di Virologia, 2Laboratori Sperimentali di Ricerca, IRCCS Policlinico San Matteo, 27100 Pavia, Italy The incidence of human cytomegalovirus (HCMV) disease in AIDS patients decreased dramatically after the introduction, a few years ago, of highly active antiretroviral combination therapy. As a consequence, the emergence of drug-resistant HCMV strains is no longer a major problem in HIV-infected individuals. However, HCMV resistance to antiviral drugs is presently recognized as an emerging problem in transplantation settings. The mechanisms of HCMV drug resistance will be analysed along with the clinical features relevant to the emergence of drug-resistant HCMV strains during antiviral treatment of patients receiving either solid organ or haematopoietic stem cell transplantation. Keywords: HCMV, antivirals, drug resistance Introduction Until very recently, the large majority of immunocompromised patients receiving antiviral treatment for human cytomegalovirus (HCMV) infection or disease was represented by patients with AIDS. Thus, it is not surprising that emergence of drug-resistant HCMV strains was mostly reported in this patient population.1–18 The striking clinical benefit of the recently introduced highly active antiretroviral combination therapies (HAART) in HIV-infected individuals is demonstrated by the sharp decrease in the incidence of HCMV infections as well as other opportunistic infections.19–23 Consequently, from an epidemiological standpoint, HCMV drug resistance has become a less dramatic problem. However, a substantial number of drug-resistant HCMV strains has now been recovered from either transplant recipients24–37 or other immunosuppressed patient populations.1,38,39 Thus, physicians and clinical virologists are still facing the need for a timely identification of drug-resistant HCMV strains when in the presence of virological failure of antiHCMV treatment. In addition, the development of new antivirals with different mechanisms of action is still recognized as a major priority for the effective treatment of immunocompromised patients. This report will describe the mechanism of action of anti-HCMV drugs and the molecular basis of HCMV drug resistance. In addition, techniques for monitoring HCMV infection and response to antiviral treatment and for detecting the emergence of drug-resistant HCMV strains will be reviewed. Special attention will be paid to discuss the advantages and drawbacks of the techniques for phenotypic and genotypic drug resistance determination and to highlight the peculiar clinical features relevant to the emergence of drug-resistant HCMV strains in transplantation settings. Assays for diagnosis and monitoring of HCMV infection Viral parameters currently utilized for monitoring of HCMV infection and evaluation of the response to antiviral treatment are: (i) viraemia, (ii) antigenaemia, (iii) circulating cytomegalic endothelial cells (CCEC), (iv) DNAaemia and (v) RNAaemia. Viraemia consists of a rapid virus isolation technique based on 16–24 h co-cultivation of 2 × 105 peripheral blood leucocytes (PBL) with human fibroblast monolayers grown in shell vials, followed by counting of infected fibroblasts after nuclear staining with a monoclonal antibody (MAb) directed to the major HCMV immediateearly (IE) antigen p72.40 Antigenaemia consists of quantitative determination of HCMV pp65-positive cells in 2 × 105 PBL examined in a cytospin preparation.41 The number of HCMV-infected CCEC is determined in the cytospin preparations used for antigenaemia quantification after staining with pp65-specific MAbs.42 DNAaemia can be determined by quantitative PCR either in PBLs,43 plasma43,44 or whole blood45 and is expressed as HCMV DNA genome equivalents (or copy number) per 2 × 105 PBL, or a determined volume of whole blood or plasma, respectively. Other methods, such as the branched DNA (bDNA) technique, have been used for HCMV DNA quantification in immunocompromised patients.46 RNAaemia consists of qualitative or quantitative determination of IE- or late-mRNAs in blood by RT–PCR47 or NASBA (nucleic acid sequence based amplification).48,49 .................................................................................................................................................................................................................................................................. *Corresponding author. Tel: +39-0382-502644; Fax: +39-0382-502599; E-mail [email protected] ................................................................................................................................................................................................................................................................... 324 © The British Society for Antimicrobial Chemotherapy 2003; all rights reserved. HCMV drug resistance Figure 1. Chemical structures of ganciclovir, foscarnet and cidofovir. Anti-HCMV drugs available clinical practice Ganciclovir is a nucleoside analogue inhibitor of HCMV DNA polymerase (encoded by UL54). In order to be active, the drug requires a triple phosphorylation, the first being carried out by a viral phosphotransferase (encoded by UL97), whereas the second and third phosphorylations are carried out by cellular enzymes.3,50 Ganciclovir is usually administered at the dosage of 5 mg/kg body weight twice a day for induction treatment, whereas primary or secondary prophylaxis treatments (see below) are usually carried out with half this dosage. Ganciclovir is currently administered intravenously (iv), although an oral formulation of the drug is available. Valganciclovir is a recently developed oral prodrug of ganciclovir with improved pharmacokinetic characteristics.51 In a recent study, it was shown that using valganciclovir at a dosage of 900 mg twice a day for induction treatment and 900 mg once a day for maintenance treatment, systemic exposure to ganciclovir was similar to that obtained following iv administration of ganciclovir, eventually leading to a comparable efficacy of the two drugs.51 Foscarnet is a DNA polymerase inhibitor acting as a competitor of pyrophosphate. Foscarnet does not require metabolic activation and is administered at a dosage of 90 mg/kg body weight twice a day for induction treatment and at half that dosage for primary or secondary prophylaxis. The administration is iv. Cidofovir is a nucleotide analogue inhibiting the viral DNA polymerase. Being already phosphorylated, it does not require activation by UL97. A peculiar characteristic of cidofovir is its extended halflife in vivo allowing weekly or bi-weekly administration. The drug is administered iv at a dosage of 5 mg/kg once a week during induction and 5 mg/kg once every other week during maintenance treatment. A schematic of the chemical structures of ganciclovir, foscarnet and cidofovir is shown in Figure 1. ment was usually administered at a reduced dosage lifelong. However, in the absence of effective control of HIV replication with concomitant decay of the immune system, HCMV recurrences were not prevented, eventually leading to the emergence of HCMV drugresistant strains.1–18 Moreover, in these highly immunocompromised patients, sequential treatments with different anti-HCMV drugs led in many cases to the accumulation of multiple genetic alterations with the final emergence of multidrug-resistant strains.5,9,52,53 Following the introduction of HAART, the incidence of HCMV disease in HIVinfected individuals dropped sharply.19–23 In parallel, the emergence of drug-resistant HCMV strains in this clinical setting appears to be a memory of the past. However, the number of patients failing HAART for multiple reasons (drug-related toxicity, intolerance, poor adhernce to treatment, emergence of HIV drug-resistant strains) is increasing. Thus, in the future, detection of HCMV drug-resistant strains in HAART-treated individuals might not remain just an anecdote.54 In solid organ (SOTR) or haematopoietic stem cell (HSCTR) transplant recipients, pre-symptomatic treatment approaches are usually adopted. In particular, both primary prophylaxis and pre-emptive therapy of HCMV infections have been utilized. Primary prophylaxis is based on the administration of ganciclovir to SOTR for several weeks after transplantation in order to suppress viral replication during a period of time when the patient is considered to be at high risk for development of HCMV infection. In contrast, pre-emptive therapy is based on virological monitoring of patients in the posttransplant period in order to identify and treat only those actually at risk for HCMV disease since reaching threshold values of viral load. The latter approach was proven to be able to prevent development of HCMV-related symptoms with the advantage of avoiding unnecessary treatment and related drug toxicity. Although pre-emptive therapy is now widely utilized, no consensus on standardized treatment protocols has been reached. The major reason for this is the fact that different viral parameters have been used in different laboratories to monitor HCMV infection. The most utilized viral parameters have been antigenaemia and DNAaemia. However, these techniques still lack standardization and patients at risk for HCMV disease are thus far defined mostly on the basis of locally established threshold values. In addition, different patient populations are treated on the basis of different threshold values of viral load. In this respect, it is common to treat HSCTR at the first confirmed appearance of HCMV in blood,55 whereas in SOTR higher viral load levels have been set as a threshold for treatment initiation. An exception is represented by treatment of donor-positive, recipient-negative (D+/R–) SOTR which is treated upon the first appearance of HCMV in blood.55 Monitoring of HCMV infection and response to antiviral treatment Approaches to treatment of HCMV infection in immunocompromised patients Different treatment approaches have been applied to different populations of immunocompromised patients. In the pre-HAART era, given the very high prevalence of HIV-infected individuals with low CD4 cell counts showing positivity for HCMV in blood and the unfeasibility of weekly monitoring of HCMV infections in asymptomatic individuals, specific treatment was administered in the presence of overt HCMV disease (symptomatic treatment). Response to treatment was monitored both clinically and virologically. However, the high risk of HCMV disease relapse prompted the introduction of secondary prophylaxis or maintenance treatment. Maintenance treat- In immunocompromised patients, correct monitoring of the response to antiviral treatment of HCMV infections may be the most powerful tool for detecting the emergence of drug-resistant HCMV strains. In fact, following treatment initiation, a sharp decrease in level of viral parameters is consistently observed in patients infected by drugsusceptible HCMV strains. In contrast, the emergence of drug-resistant strains is associated with an increase in viral load or the lack of decrease in level of different viral parameters.4,5,9,11,12,26–28,33–35,54,56–61 The most reliable parameter for the identification of the emergence of drug-resistant strains appears to be viraemia. In fact, positive viraemia levels during treatment document active viral replication 325 F. Baldanti and G. Gerna and may anticipate the increase in viral load as determined by quantitative determination of viral components (pp65, DNA).3,4,8,12,28 However, increase in levels of viral parameters can also be documented following short (few days) interruptions of treatment or when therapy is administered at a reduced dosage because of drug toxicity or intolerance. Thus, results of the virological response to treatment should always be interpreted for each patient with great caution and within the clinical context. In addition, the emergence of drug-resistant HCMV strains should always be proven before shifting to an alternative treatment. Thus, several assays (either phenotypic or genotypic) have been developed in recent years to rapidly detect the presence of drug-resistant HCMV strains directly in biological specimens (see below). A clinical situation stressing this warning is represented by the peculiar behaviour of antigenaemia during treatment of primary HCMV infection in SOTR. In this subset of patients, a dissociation between increasing antigenaemia and decreasing DNAaemia and viraemia levels is often observed.55 This phenomenon appears to be restricted to patients treated with ganciclovir, and the reasons for this event occurring are still unclear. Considering that D+/R– is also the subset of SOTR in whom almost all reported drugresistant HCMV strains have been detected,25–28,33,36,37 it appears evident that separating an abnormal rise of antigenaemia alone from a true increase in viral load during therapy is of critical importance for correct diagnosis of drug resistance. In this respect, the concomitant determination of DNAaemia and viraemia is of crucial help: emergence of drug-resistant strains in these patients is associated with a concomitant increase in all viral parameters, which, in contrast, are shown to decrease in parallel when an effective treatment is administered.28 Molecular basis for drug resistance Ganciclovir Acquisition of mutations in UL97 phosphotransferase (Figure 2) appears to be a crucial step in the selection of ganciclovir-resistant HCMV strains. HCMV strains with mutation in key regions (domains VIII, VI and IX) of the viral enzyme have been proven to be highly resistant to ganciclovir.6–8,14,17,18,25–28,31,56,62–68 In addition to UL97, mutations in UL54 impact ganciclovir susceptibility.13,15,53,56,69,70 However, mutations in UL54 are less common and have been reported only in patients harbouring ganciclovir-resistant UL97mutant strains maintained on ganciclovir treatment.53 The isolates with mutations in both UL97 and UL54 showed very high levels of resistance to ganciclovir and simultaneous cross-resistance to cidofovir,53 but retained foscarnet susceptibility. Finally, it is worth mentioning that, according to the limited data so far available, valganciclovir does not appear to select for an increased number of ganciclovir-resistant strains.71 Foscarnet Mutations in domains II, III and VI of HCMV DNA polymerase (Figure 2) are responsible for foscarnet resistance.5,57,66,69,70 Interestingly, no cross resistance to either ganciclovir or cidofovir is associated with foscarnet-induced UL54 mutations.66,69,70 Thus, the reported emergence of double ganciclovir- and foscarnet-resistant HCMV strains was due to the accumulation of specific mutations in the two viral genes induced by sequential treatment with the two drugs.9,5,66 However, mutations in domain III have been proven to induce simultaneous resistance to foscarnet, ganciclovir and cidofovir.56 Cidofovir Mutations in the HCMV DNA polymerase are responsible for simultaneous resistance to cidofovir and ganciclovir.66,70 Because of its high renal toxicity, cidofovir is not widely utilized for treatment of HCMV infection. Thus, selection of cidofovir-resistant strains is an extremely rare event and it appears mostly driven by sustained ganciclovir administration.53 Methods for phenotypic determination of antiviral drug resistance Reduction of HCMV replication in the presence of increasing drug concentrations can be determined by several methods. Plaque reduction assay (PRA) This assay measures the reduction in number of cytopathic effect foci following infection of fibroblast monolayers with titrated virus isolates (CPE-PRA).72 Alternatively, the number of IE antigen or late antigen plaques can be determined (IEA- or LA-PRA).4,73 This assay is regarded as the reference method for HCMV drug susceptibility determination and, following titration of the virus isolate, requires 4–10 days to be completed. In detail, IEA-PRA provides results in 4 days, LA-PRA is completed in 6–7 days and CPE-PRA takes longer. Although PRA has been known for several years and widely utilized, it is not yet standardized and comparison of results from different laboratories appears sometimes difficult. The lack of standardization is primarily related to:(i) the use of different fibroblast strains, (ii) the use of cell-free virus as inoculum versus cell-associated virus, (iii) the virus plaque staining technique; (iv) the use of laboratory adapted HCMV strains (AD169, Towne) versus clinical isolates as controls, (v) the subjectivity in reading test results. Consensus is lacking in the definition of drug resistance: some authors indicate 6 µM ganciclovir and 400 µM foscarnet as ID50 cut-off values for ganciclovir- and foscarnet-sensitive HCMV strains, respectively. In our laboratory we define as drug-resistant the HCMV isolates showing ID50 values ≥5-fold the mean ID50 values determined on a series of HCMV isolates from untreated patients.4,9,12,28,74 Other authors consider as resistant HCMV isolates with ID50 values increased by ≥2 S.D. of the mean ID50 values determined on a series of HCMV control field isolates.6 Recently, a rapid drug susceptibility screening assay has been developed based on the concept of PRA.58 This assay measures the reduction in IEA-plaques following inoculation onto fibroblast monolayers of a predetermined number of PBL and incubation of cell cultures for 4–6 days in the presence of a single drug concentration (ganciclovir, 20 µM; foscarnet, 400 µM). A decrease of ≤50% in the number of IEA-plaques with respect to the no-drug control is considered as associated with the presence of drug resistance.74 A similar approach has been described by Pepin et al.75 In situ ELISA This technique measures the reduction in LA production in fibroblast cultures infected with cell-free HCMV, which reflects the number of cells undergoing a complete virus replication cycle. The assay is carried out in 96-well microtitre plates and viral titration can be carried out in the context of the assay by simultaneously challenging increasing virus dilutions with decreasing drug concentrations in the same plate. After 4–6 days of incubation, the amount of viral antigen in each well is determined by immunoenzymic staining followed by 326 HCMV drug resistance Figure 2. Schematic of HCMV DNA polymerase (encoded by UL54) and phosphotransferase (encoded by UL97). DNA polymerase codons mutated in ganciclovirand cidofovir-cross-resistant, foscarnet-resistant and multidrug-resistant HCMV strains are indicated by solid, dashed, and dotted vertical bars, respectively. UL97 codons mutated in ganciclovir-resistant HCMV strains are shown by vertical solid bars. spectrophotometric determination of absorbance. The assay is completed in 4–6 days.76,77 Virus yield reduction assay The effect of antiviral drugs on viral replication can also be determined by quantifying the reduction in infectious viral titres, measured either as cell-free or cell-associated virus.78 This technique is cumbersome and extremely time-consuming and is currently utilized for research in drug development. Flow cytometry-based assays The reduction in viral antigen production can also be determined using flow cytometry by counting the number of trypsinized fibroblasts expressing late viral proteins.79,80 DNA reduction assay This assay measures the reduction in viral DNA synthesis in fibroblast cultures in the presence of increasing drug concentrations.81 Quantification of HCMV DNA is obtained by hybridization of the viral genome with a 125I-labelled probe followed by counting the γ-emission by the bound probe. Following preparation of a titrated virus stock, results are available in 1 week. However, this assay is not widespread, primarily because of the need for dedicated facilities and expensive equipment (γ-counter). Methods for genotypic determination of antiviral drug resistance The presence of drug-resistant HCMV strains can be determined by identifying specific mutations in the viral phosphotransferase (UL97) or DNA polymerase (UL54) coding sequences. Sequencing Analysis of UL97 and UL54 genes is usually carried out following amplification of gene fragments from viral isolates or directly from clinical samples by PCR. When using an automated sequencer, results are available in a couple of days. This assay is the reference technique for the identification of mutations emerging during treatment failure. However, despite its powerful diagnostic potential, sequence analysis is currently restricted to specialized laboratories, requiring expensive equipment and personnel with specific expertise. Restriction fragment length polymorphism (RFLP) This assay allows detection of specific mutations associated with drug resistance by evaluating the restriction pattern of PCR products digested with endonucleases, in which restriction sites have been modified (suppressed or generated) by single mutations.28,63 In addition, deletions modifying the size of digested fragments can be readily detected.64 Thus far, this technique has been widely applied for identification of UL97 mutations conferring ganciclovir resistance. Probe-specific hybridization or primer-specific amplification Probes discriminating single nucleotide substitutions can be used for hybridization of PCR products. Alternatively, primers can be designed to anneal only with the wild-type or the mutant sequence, thus allowing specific amplification by PCR or ligase chain reaction (LCR).82,83 Advantages and disadvantages of phenotypic testing for drug resistance Methods determining the level of inhibition of viral replication in vitro in the presence of a drug provide direct evidence of susceptibility or resistance to antiviral compounds. However, ‘susceptibility’ or ‘resistance’ are not absolute concepts, but indicate levels of inhibition of viral replication which are comparable or significantly lower than those observed using reference strains, respectively. Indeed, the selection of appropriate controls represents one of the most debated issues, and lack of consensus on this topic represents the major obstacle for the standardization of phenotypic assays 327 F. Baldanti and G. Gerna for HCMV drug resistance determination. AD169 or Towne strains, which most laboratories use as drug-sensitive reference strains, appear to be different from clinical HCMV isolates in different aspects. In fact, the replication and spread in cell culture of AD169 and Towne strains are different from those of clinical isolates, as shown by the faster viral kinetics and the higher release of cell-free virus in cell culture supernatant, which contrasts with the slower growth rate and the preferential cell-to-cell transmission of recent clinical isolates. In addition, AD169 and Towne strains present important genetic alterations,84 which likely occurred during the fibroblast adaptation process and which might be accompanied by more subtle mutations in other genes. The characteristics of reference strains might also affect their susceptibility to antiviral drugs. Interestingly, AD169 recombinants carrying mutations from clinical isolates often show ID50 values substantially different from those of the parental drug-resistant strain.56,57,64,66,67,69,70 Besides other factors already mentioned above, other factors should be taken into account in an attempt to standardize the phenotypic drug resistance testing, i.e. the presence of multiple viral variants in the viral isolate, and the possible growth deficits of drug-resistant viral strains. The last two points have direct implications in the interpretation of results of drug susceptibility testing. In fact, in the presence of mixtures of wild-type and mutated virus strains, the isolation procedure may favour the recovery of a single viral variant, sometimes delaying the isolation of the resistant strain.12,28,64 In addition, when in the presence of a mixed viral population in vivo including drug-resistant strains with impaired growth in fibroblast cultures,4,8,9,60,61,66,69 the sensitive strains may overgrow the resistant ones in cell culture, thus hampering the reliability of the drug susceptibility testing. Advantages and disadvantages of genotypic testing for drug resistance The use of molecular biology techniques for detection of drug resistanceassociated mutations in UL97 and UL54 can greatly shorten the time required for the identification of HCMV drug-resistant strains. In addition, molecular techniques provide the opportunity to quantify the mutant (resistant) viral variants in the context of a mixed viral population. Finally, genotypic testing of drug susceptibility appears in need of better standardization. However, identification of HCMV strains with specific mutations in target gene products is only indirect evidence of drug resistance. In this respect, problems in result interpretation might arise in the face of new mutations or constellations of mutations. In these cases, great caution must be applied before labelling as resistant a strain with a new mutation in UL97 or UL54. In fact, although UL97 regions involved in ganciclovir recognition and processing appear to be well defined, confirmatory marker transfer experiments still appear to be mandatory in order to elucidate the role of new mutations in these regions in conferring ganciclovir resistance. As for UL54, although distinct patterns of mutations conferring resistance to foscarnet and cross-resistance between ganciclovir and cidofovir have been described, some amino acid changes appear to confer multiple drug resistance. Thus, the impact of new UL54 mutations in decreasing the susceptibility of clinically available anti-HCMV compounds is not a priori predictable, and marker transfer confirmation is needed. Conclusions In conclusion, as emerging from the above-reported considerations, no wonder tool is available at present for rapid detection of the emergence of drug-resistant HCMV strains in immunocompromised patients failing anti-HCMV treatment. On the contrary, an integrated programme including: (i) careful virological monitoring of HCMV infection and response to treatment, (ii) the use of rapid phenotypic screening assays for drug susceptibility testing and molecular techniques for detection of specific genetic mutations, and (iii) the application of confirmatory drug susceptibility assays on viral isolates obtained during virological follow-up, still appears to be the best approach for the timely detection of drug-resistant HCMV strains in the clinical setting. Acknowledgements This work was partially supported by Ministero della Salute, Istituto Superiore di Sanità, Programma Nazionale di Ricerca sull’AIDS (grant 50D.12), Ministero della Salute, Ricerca Finalizzata 2001 (convenzione 126). References 1. Erice, A., Chou, S., Biron, K. K. et al. (1989). Progressive disease due to ganciclovir-resistant cytomegalovirus in immunocompromised patients. New England Journal of Medicine 320, 289–93. 2. Jacobson, M. A., Drew, W. L., Feinberg, J. et al. (1991). Foscarnet therapy for ganciclovir-resistant cytomegalovirus retinitis in patients with AIDS. Journal of Infectious Diseases 163, 1348–51. 3. Stanat, S. C., Reardon, J. E., Erice, A. et al. (1991). Ganciclovirresistant cytomegalovirus clinical isolates: mode of resistance to ganciclovir. Antimicrobial Agents and Chemotherapy 35, 2191–7. 4. Gerna, G., Baldanti, F., Zavattoni, M. et al. (1992). Monitoring of ganciclovir sensitivity of multiple human cytomegalovirus strains coinfecting blood of an AIDS patient by an immediate-early antigen plaque assay. Antiviral Research 19, 333–45. 5. Baldanti, F., Sarasini, A., Silini, E. et al. (1995). Four dually resistant human cytomegalovirus strains from AIDS patients: single mutations in UL97 and UL54 open reading frames are responsible for ganciclovirand foscarnet-specific resistance, respectively. Scandinavian Journal of Infectious Diseases. Supplementum 99, 103–4. 6. Wolf, D. G., Smith, I. L., Lee, D. J. et al. (1995). Mutations in human cytomegalovirus UL97 gene confer clinical resistance to ganciclovir and can be detected directly in patient plasma. Journal of Clinical Investigation 95, 257–63. 7. Chou, S., Guentzel, S., Michels, K. R. et al. (1995). Frequency of UL97 phosphotransferase mutations related to ganciclovir resistance in clinical cytomegalovirus isolates. Journal of Infectious Diseases 172, 239–42. 8. Wolf, D. G., Lee, D. J. & Spector, S. A. (1995). Detection of human cytomegalovirus mutations associated with ganciclovir resistance in cerebrospinal fluid of AIDS patients with central nervous system disease. Antimicrobial Agents and Chemotherapy 39, 2552–4. 9. Sarasini, A., Baldanti, F., Furione, M. et al. (1995). Double resistance to ganciclovir and foscarnet of four human cytomegalovirus strains recovered from AIDS patients. Journal of Medical Virology 47, 237–44. 10. Smith, I. L., Shinkai, M., Freeman, W. R. et al. (1996). Polyradiculopathy associated with ganciclovir-resistant cytomegalovirus in an AIDS patient: phenotypic and genotypic characterization of sequential virus isolates. Journal of Infectious Diseases 173, 1481–4. 11. Boivin, G., Gilbert, C., Morissette, M. et al. (1997). A case of ganciclovir-resistant cytomegalovirus (CMV) retinitis in a patient with AIDS: longitudinal molecular analysis of the CMV viral load and viral mutations in blood compartments. AIDS 11, 867–73. 328 HCMV drug resistance 12. Baldanti, F., Simoncini, L., Talarico, C. L. et al. (1998). Emergence of a ganciclovir-resistant human cytomegalovirus strain with a new UL97 mutation in an AIDS patient. AIDS 12, 816–8. 13. Smith, I. L., Taskintuna, I., Rahhal, F. M. et al. (1998). Clinical failure of CMV retinitis with intravitreal cidofovir is associated with antiviral resistance. Archives of Ophthalmology 116, 178–85. 14. Gilbert, C., Handfield, J., Toma, E. et al. (1998). Emergence and prevalence of cytomegalovirus UL97 mutations associated with ganciclovir resistance in AIDS patients. AIDS 12, 125–9. 15. Jabs, D. A., Enger, C., Forman, M. et al. (1998). Incidence of foscarnet resistance and cidofovir resistance in patients treated for cytomegalovirus retinitis. The Cytomegalovirus Retinitis and Viral Resistance Study Group. Antimicrobial Agents and Chemotherapy 42, 2240–4. 16. Drew, W. L., Stempien, M. J., Andrews, J. et al. (1999). Cytomegalovirus (CMV) resistance in patients with CMV retinitis and AIDS treated with oral or intravenous ganciclovir. Journal of Infectious Diseases 179, 1352–5. 17. Abraham, B., Lastere, S., Reynes, J. et al. (1999). Ganciclovir resistance and UL97 gene mutations in cytomegalovirus blood isolates from patients with AIDS treated with ganciclovir. Journal of Clinical Virology 13, 141–8. 18. Jabs, D. A., Martin, B. K., Forman, M. S. et al. (2001). Mutations conferring ganciclovir resistance in a cohort of patients with acquired immunodeficiency syndrome and cytomegalovirus retinitis. Journal of Infectious Diseases 183, 333–7. 19. Gerna, G., d’Arminio Monforte, A., Zavattoni, M. et al. (1998). Sharp drop in the prevalence of human cytomegalovirus leuko-DNAemia in HIV-infected patients following highly active antiretroviral therapy. AIDS 12, 118–20. 20. O’Sullivan, C. E., Drew, W. L., McMullen, D. J. et al. (1999). Decrease of cytomegalovirus replication in human immunodeficiency virus infected-patients after treatment with highly active antiretroviral therapy. Journal of Infectious Diseases 180, 847–9. 21. Deayton, J., Mocroft, A., Wilson, P. et al. (1999). Loss of cytomegalovirus (CMV) viraemia following highly active antiretroviral therapy in the absence of specific anti-CMV therapy. AIDS 13, 1203–6. 22. Soriano, V., Dona, C., Rodriguez-Rosado, R. et al. (2000). Discontinuation of secondary prophylaxis for opportunistic infections in HIVinfected patients receiving highly active antiretroviral therapy. AIDS 14, 383–6. 23. Deayton, J. R., Wilson, P., Sabin, C. A. et al. (2000). Changes in the natural history of cytomegalovirus retinitis following the introduction of highly active antiretroviral therapy. AIDS 14, 1163–70. 24. Knox, K. K., Drobyski, W. R. & Carrigan, D. R. (1991). Cytomegalovirus isolate resistant to ganciclovir and foscarnet from a marrow transplant patient. Lancet 337, 1292–3. 25. Lurain, N. S., Ammons, H. C., Kapell, K. S. et al. (1996). Molecular analysis of human cytomegalovirus strains from two lung transplant recipients with the same donor. Transplantation 62, 497–502. 26. Rosen, H. R., Benner, K. G., Flora, K. D. et al. (1997). Development of ganciclovir resistance during treatment of primary cytomegalovirus infection after liver transplantation. Transplantation 63, 476–8. 27. Alain, S., Honderlick, P., Grenet, D. et al. (1997). Failure of ganciclovir treatment associated with selection of a ganciclovir-resistant cytomegalovirus strain in a lung transplant recipient. Transplantation 63, 1533–6. 28. Baldanti, F., Simoncini, L., Sarasini, A. et al. (1998). Ganciclovir resistance as a result of oral ganciclovir in a heart transplant recipient with multiple human cytomegalovirus strains in blood. Transplantation 66, 324–9. 29. Kruger, R. M., Shannon, W. D., Arens, M. Q. et al. (1999). The impact of ganciclovir-resistant cytomegalovirus infection after lung transplantation. Transplantation 68, 1272–9. 30. Manso, J. V., Lambert, J. L., Ona, M. et al. (1999). Ganciclovir resistance in a heart transplant recipient infected by cytomegalovirus. International Journal of Cardiology 71, 97–8. 31. Mendez, J. C., Sia, I. G., Tau, K. R. et al. (1999). Novel mutation in the CMV UL97 gene associated with resistance to ganciclovir therapy. Transplantation 67, 755–7. 32. Bienvenu, B., Thervet, E., Bedrossian, J. et al. (2000). Development of cytomegalovirus resistance to ganciclovir after oral maintenance treatment in a renal transplant recipient. Transplantation 69, 182–4. 33. Limaye, A. P., Corey, L., Koelle, D. M. et al. (2000). Emergence of ganciclovir disease among recipients of solid-organ transplants. Lancet 356, 609–10. 34. Eckle, T., Prix, L., Jahn, G. et al. (2000). Drug-resistant human cytomegalovirus infection in children after allogeneic stem cell transplantation may have different clinical outcomes. Blood 96, 3286–9. 35. Eckle, T., Lang, P., Prix, L. et al. (2002). Rapid development of ganciclovir-resistant cytomegalovirus infection in children after allogeneic stem cell transplantation in the early phase of immune recovery. Bone Marrow Transplantation 30, 433–9. 36. Lurain, N. S., Bhorade, S. M., Pursell, K. J. et al. (2002). Analysis and characterization of antiviral drug-resistant cytomegalovirus isolates from solid organ transplant recipients. Journal of Infectious Diseases 186, 760–8. 37. Bhorade, S. M., Lurain, N. S., Jordan, A. et al. (2002). Emergence of ganciclovir-resistant cytomegalovirus in lung transplant recipients. Journal of Heart and Lung Transplantation 21, 1274–82. 38. Sasaki, T., Okayama, A., Eizuru, Y. et al. (1997). Progressive retinitis-encephalitis due to ganciclovir-resistant cytomegalovirus associated with aplastic anemia. Internal Medicine 36, 375–9. 39. Wolf, D. G., Yaniv, I., Honigman, A. et al. (1998). Early emergence of ganciclovir-resistant human cytomegalovirus strains in children with primary combined immunodeficiency. Journal of Infectious Diseases 178, 535–8. 40. Gerna, G., Revello, M. G., Percivalle, E. et al. (1990). Quantification of human cytomegalovirus viremia by using monoclonal antibodies to different viral proteins. Journal of Clinical Microbiology 28, 2681–8. 41. Gerna, G., Revello, M. G., Percivalle, E. et al. (1992). Comparison of different immunostaining techniques and monoclonal antibodies to the lower matrix phosphoprotein (pp65) for optimal quantitation of human cytomegalovirus antigenemia. Journal of Clinical Microbiology 30, 1232–7. 42. Percivalle, E., Revello, M. G., Vago, L. et al. (1993). Circulating endothelial giant cells permissive for human cytomegalovirus (HCMV) are detected in disseminated HCMV infections with organ involvement. Journal of Clinical Investigation 92, 663–70. 43. Gerna, G., Furione, M., Baldanti, F. et al. (1994). Comparative quantitation of human cytomegalovirus DNA in blood leukocytes and plasma of transplant and AIDS patients. Journal of Clinical Microbiology 32, 2709–17. 44. Spector, S. A., Wong, R., Hsia, K. et al. (1998). Plasma cytomegalovirus (CMV) DNA load predicts CMV disease and survival in AIDS patients. Journal of Clinical Investigation 116, 178–85. 45. Cope, A. V., Sabin, C., Burroughs, A. et al. (1997). Interrelationship among quantity of human cytomegalovirus (HCMV) DNA in blood, donor-recipient serostatus, and administration of methylprednisolone as risk factor for HCMV disease following liver transplantation. Journal of Infectious Diseases 176, 1484–90. 46. Chernoff, D. N., Miner, R. C., Hoo, B. S. et al. (1997). Quantification of cytomegalovirus DNA in peripheral blood leukocytes by a branched-DNA signal amplification assay. Journal of Clinical Microbiology 35, 2740–4. 47. Bitsch, A., Kirchner, H., Dupke, R. et al. (1993). Cytomegalovirus transcripts in peripheral blood leukocytes of actively infected transplant patients detected by reverse transcription-polymerase chain reaction. Journal of Infectious Diseases 163, 740–3. 48. Gerna, G., Baldanti, F., Middeldorp, J. M. et al. (1999). Clinical significance of expression of human cytomegalovirus pp67 late transcript in heart, lung, and bone marrow transplant recipients as determined by nucleic acid sequence-based amplification. Journal of Clinical Microbiology 37, 902–11. 329 F. Baldanti and G. Gerna 49. Gerna, G., Baldanti, F., Lilleri, D. et al. (2000). Human cytomegalovirus immediate-early mRNA detection by nucleic acid sequence-based amplification as a new parameter for preemptive therapy in bone marrow transplant recipients. Journal of Clinical Microbiology 38, 1845–53. 50. Sullivan, V., Talarico, C. L., Stanat, S. C. et al. (1992). A protein kinase homologue controls phosphorylation of ganciclovir in human cytomegalovirus-infected cells. Nature 358, 162–4. 51. Martin, D. F., Sierra-Madero, J., Walmsley, S. et al. (2002). A controlled trial of valganciclovir as induction therapy for cytomegalovirus retinitis. New England Journal of Medicine 346, 1119–26. 52. Sullivan, V., Biron, K. K., Talarico, C. et al. (1993). A point mutation in the human cytomegalovirus DNA polymerase gene confers resistance to ganciclovir and phosphonylmethoxyalkyl derivatives. Antimicrobial Agents and Chemotherapy 37, 19–25. 53. Smith, I. L., Cherrington, J. M., Jiles, R. E. et al. (1997). High-level resistance of cytomegalovirus to ganciclovir is associated with alterations in both the UL97 and DNA polymerase genes. Journal of Infectious Diseases 176, 69–77. 54. Baldanti, F., Paolucci, S., Parisi, A. et al. (2002). Emergence of multiple drug-resistant human cytomegalovirus variants in two HIV-infected patients failing HAART. Clinical Infectious Diseases 34, 1146–9. 55. Gerna, G., Baldanti, F., Grossi, P. et al. (2001). Diagnosis and monitoring of human cytomegalovirus infection in transplant recipients. Reviews in Medical Microbiology 12, 155–75. 56. Chou, S., Marousek, G., Guentzel, S. et al. (1997). Evolution of mutations conferring multidrug resistance during prophylaxis and therapy for cytomegalovirus disease. Journal of Infectious Diseases 176, 786–9. 57. Chou, S., Marousek, G., Parenti, D. M. et al. (1998). Mutation in region III of the DNA polymerase gene conferring foscarnet resistance in cytomegalovirus isolates from 3 subjects receiving prolonged antiviral therapy. Journal of Infectious Diseases 178, 526–30. 58. Boivin, G., Gilbert, C., Morissette, M. et al. (1997). A case of ganciclovir-resistant cytomegalovirus (CMV) retinitis in a patient with AIDS: longitudinal molecular analysis of the CMV viral load and viral mutations in blood compartments. AIDS 11, 867–73. 59. Baldanti, F., Revello, M. G., Percivalle, E. et al. (1998). Use of the human cytomegalovirus (HCMV) antigenemia assay for diagnosis and monitoring of HCMV infections and detection of antiviral drug resistance in the immunocompromised. Journal of Clinical Virology 11, 51–60. 60. Bowen, E. F., Cherrington, J. M., Lamy, P. D. et al. (1999). Quantitative changes in cytomegalovirus DNAemia and genetic analysis of the UL97 and UL54 genes in AIDS patients receiving cidofovir following ganciclovir therapy. Journal of Medical Virology 58, 402–7. 61. Emery, V. C. & Griffiths, P. D. (2000). Prediction of cytomegalovirus load and resistance patterns after antiviral chemotherapy. Proceedings of the National Academy of Sciences, USA 97, 8039–44. 62. Lurain, N. S., Spafford, L. E. & Thompson, K. D. (1994). Mutation in the UL97 open reading frame of human cytomegalovirus strains resistant to ganciclovir. Journal of Virology 68, 4427–31. 63. Chou, S., Erice, A., Jordan, M. C. et al. (1995). Analysis of the UL97 phosphotransferase coding sequence in clinical cytomegalovirus isolates and identification of mutations conferring ganciclovir resistance. Journal of Infectious Diseases 171, 576–83. 64. Baldanti, F., Silini, E., Sarasini, A. et al. (1995). A three-nucleotide deletion in the UL97 open reading frame is responsible for the ganciclovir resistance of a human cytomegalovirus clinical isolate. Journal of Virology 69, 796–800. 65. Hanson, M. N., Preheim, L. C., Chou, S. et al. (1995). Novel mutation in the UL97 gene of a clinical cytomegalovirus strain conferring resistance to ganciclovir. Antimicrobial Agents and Chemotherapy 39, 1204–5. 66. Baldanti, F., Underwood, M. R., Stanat, S. C. et al. (1996). Single amino acid changes in the DNA polymerase confer foscarnet resistance and slow-growth phenotype, while mutations in the UL97-encoded phosphotransferase confer ganciclovir resistance in three double-resistant human cytomegalovirus strains recovered from patients with AIDS. Journal of Virology 70, 1390–5. 67. Baldanti, F., Underwood, M. R., Talarico, C. L. et al. (1998). The Cys607→Tyr change in the UL97 phosphotransferase confers ganciclovir resistance to two human cytomegalovirus strains recovered from two immunocompromised patients. Antimicrobial Agents and Chemotherapy 42, 444–6. 68. Chou, S. & Meichsner, C. L. (2000). A nine-codon deletion mutation in the cytomegalovirus UL97 phosphotransferase gene confers resistance to ganciclovir. Antimicrobial Agents and Chemotherapy 44, 183–5. 69. Cihlar, T., Fuller, M. D., Mulato, A. S. et al. (1998). A point mutation in the human cytomegalovirus DNA polymerase gene selected in vitro by cidofovir confers a slow replication phenotype in cell culture. Virology 248, 382–93. 70. Cihlar, T., Fuller, M. D. & Cherrington, J. M. (1998). Characterization of drug resistance-associated mutations in the human cytomegalovirus DNA polymerase gene by using recombinant mutant viruses generated from overlapping DNA fragments. Journal of Virology 72, 5927–36. 71. Boivin, G., Gilbert, C., Gaudreau, A. et al. (2001). Rate of emergence of cytomegalovirus (CMV) mutations in leukocytes of patients with acquired immunodeficiency syndrome who are receiving valganciclovir as induction and maintenance therapy for HCMV retinitis. Journal of Infectious Diseases 184, 1598–601. 72. Lang, D. J. & Cheung, K. S. (1982). Effectiveness of acycloguanosine and trifluorothymidine as inhibitors of cytomegalovirus infection in vitro. American Journal of Medicine 73, 49–53. 73. Prix, L., Maierl, J., Jahn, G. et al. (1998). A simplified assay for screening of drug resistance of cell-associated cytomegalovirus strains. Journal of Clinical Virology 11, 29–37. 74. Gerna, G., Sarasini, A., Percivalle, E. et al. (1995). Rapid screening for resistance to ganciclovir and foscarnet of primary isolates of human cytomegalovirus from culture-positive blood samples. Journal of Clinical Microbiology 33, 738–41. 75. Pepin, J. M., Simon, F., Dussault, A. et al. (1992). Rapid determination of human cytomegalovirus susceptibility to ganciclovir directly from clinical specimen primocultures. Journal of Clinical Microbiology 30, 2917–20. 76. Tatarowicz, W. A., Lurain, N. S. & Thompson, K. D. (1991). In situ ELISA for the evaluation of antiviral compounds effective against human cytomegalovirus. Journal of Virological Methods 35, 207–15. 77. Stahle, E. L., Schloss, L., Sundqvist, V. A. et al. (1998). Solid phase ELISA for determination of the virus dose dependent sensitivity of human cytomegalovirus to antiviral drugs in vitro. Antiviral Research 40, 105–12. 78. Wingard, J. R., Stuart, R. K., Saral, R. et al. (1981). Activity of trifluorothymidine against cytomegalovirus. Antimicrobial Agents and Chemotherapy 20, 286–90. 79. Kesson, A. M., Zeng, F., Cunningham, A. L. et al. (1998). The use of flow cytometry to detect antiviral resistance in human cytomegalovirus. Journal of Virological Methods 71, 177–86. 80. Lipson, S. M., Soni, M., Biondo, F. X. et al. (1997). Antiviral susceptibility testing-flow cytometric analysis (AST-FCA) for the detection of cytomegalovirus drug resistance. Diagnostic Microbiology and Infectious Disease 28, 123–9. 81. Lurain, N. S., Thompson, K. D., Holmes, E. W. et al. (1992). Point mutations in the DNA polymerase gene of human cytomegalovirus that result in resistance to antiviral agents. Journal of Virology 66, 7146–52. 82. Alain, S., Mazeron, M. C., Pepin, J. M. et al. (1993). Rapid detection of cytomegalovirus strains resistant to ganciclovir through mutations within the gene UL97. Molecular and Cellular Probes 7, 487–95. 83. Bourgeois, C., Sixt, N., Bour, J. B. et al. (1997). Value of a ligase chain reaction assay for detection of ganciclovir resistance-related mutation 594 in UL97 gene of human cytomegalovirus. Journal of Virological Methods 67, 167–75. 84. Cha, T. A., Tom, E., Kemble, G. W. et al. (1996). Human cytomegalovirus clinical isolates carry at least 19 genes not found in laboratory strains. Journal of Virology 70, 78–83. 330