Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Practice Concepts.
Nancy L Wilson, MA, Editor
Copyright 7997 by
The Cerontological Society of America
The Cerontologist
Vol. 37, No. 5,675-682
Disruptive vocalization (DV) is a common problem in the management of cognitively and
physically impaired older people. This article reports the results of a consensus meeting
convened to provide guidelines for clinicians and recommendations for researchers in this
difficult and little-studied behavioral problem. DV arises largely in people with cognitive
impairment and generally reflects an underlying need or discomfort. A variety of factors can
precipitate and aggravate DV; the key to management is appropriate identification of all
possible factors and development of an individualized treatment plan.
Key Words: Disruptive vocalization, Screaming, Behavioral problems, Dementia, Nursing homes
Management of the Patient
With Disruptive Vocalization1
Philip D. Sloane, MD, MPH,2 Susan Davidson, RNC, MA,3
Kathleen Buckwalter, PhD, RN,4 B. Anthony Lindsey, MD,3
Susan Ayers, MA,5 Vonda Lenker,5 and Louis D. Burgio, PhD6
Disruptive vocalization (DV) consists of excessively
loud and/or repetitive verbal utterances, such as single words or phrases, nonsensical sounds, screaming, moaning, and constant requests for attention
(Cariaga, Burgio, Flynn, & Martin, 1991; Cohen-Mansfield, Werner, & Marx, 1990; Ryan, Tainsh, Kolodny,
Lendrum, & Fisher, 1988). DV generally occurs in cognitively impaired older persons; indeed, Alois
Alzheimer's original patient was noted to "scream
loudly" (Alzheimer, 1906). However, these behaviors
are occasionally found in other populations, such as
those with mental retardation, personality disorders,
and acute psychoses. These vocalizations are often
considered aberrant because of inappropriate intensity, frequency, duration, and/or the setting in which
'This work was supported by a grant from Manor HealthCare, Inc., Silver
Spring, Maryland, and is based on a conference held February 2-3,1996, in
Chapel Hill, North Carolina. The authors thank Ceri Hall for contributing
cases and ideas for the conference.
department of Family Medicine, School of Medicine, University of North
Carolina at Chapel Hill, NC 27599-7595. Address correspondence to Philip
D. Sloane, MD.
'Department of Psychiatry, School of Medicine, University of North Carolina at Chapel Hill.
'College of Nursing, the University of Iowa.
5
Manor HealthCare Corporation, Silver Spring, MD.
'Center for Aging, University of Alabama, Birmingham.
Vol. 37, No. 5,1997
675
they occur. Differentiation is sometimes made between verbal agitation and verbally aggressive behavior (Cohen-Mansfield, Marx, & Rosenthal, 1989). Verbally agitated behaviors include complaining;
screaming; yelling; constant requests for attention;
and repetitious noises, words, or phrases. Verbal aggression is hostile or accusatory in nature and often
threatens harm (e.g., "Get away or I'm going to hit
you," "I'm going to knock your block off"). Most disruptive vocalizations are of the verbally agitated type;
verbal aggression is generally a time-limited response to a perceived threat such as bathing and
dressing (Beck, Baldwin, Modlin, & Lewis, 1990;
Rosby, Beck, & Heacock, 1992).
Disruptive vocalization is especially problematic in
nursing homes, where even one loud, persistent vocalizer can cause distress among caregivers, visitors,
and other residents. DV can complicate the delivery
of quality care in several ways: by causing staff caregivers to feel stressed, to withdraw attention, and/or
to request reassignment to other residents; by leading to isolation of the resident from others; by resulting in excessive use of physical and/or pharmacologic
restraint; and by leading to resident transfer to a more
restrictive level of care (Rosby et al., 1992). Family
members may find the vocalizations stressful and, as
a consequence, visit less frequently or criticize staff
for their inability to maintain quiet or address needs.
Other residents may become annoyed or concerned
that someone is hurt, or may themselves become agitated and vocalize loudly in response.
The reported prevalence of disruptive vocalization
in nursing homes varies depending on the definition
and the manner of assessment. Ryan et al. (1988) defined noise-making as any chronic pattern of verbal
behavior ranging from whispers to screams; they
identified a prevalence of 29% in one facility and 31%
in another. Cohen-Mansfield et al. (1990) narrowed
the definition to include only people who emitted
loud, shrill, or piercing sounds (shouts, screams, or
howls) at least once a day; they found that 15% of residents in one large facility were verbally disruptive in
that manner. Christie and Ferguson (1988) and Hallberg, Norberg, and Erikson (1990) limited their definitions to persons who were frequently loud and disruptive, either using sounds or words; their
identified prevalences were 12.5% and 15.2% of nursing home residents, respectively. Cariaga et al. (1991)
found that 11% of nursing home residents had disruptive vocalization identified as a target behavior in
their care plan; of these, 88.2% exhibited the behavior at least one time per shift, and 25% displayed it
more than 20 times per shift.
This article reports guidelines and recommendations for the care of disruptive vocalizers. They were
developed primarily for staff of residential long-term
care settings but should be applicable to home and
hospital care. These recommendations arose from a
conference on disruptive vocalization held in Chapel
Hill, North Carolina, in February, 1996. Invited participants included researchers in the field, educators,
and practitioners. Conference participants began by
reviewing cases that had been prepared by the participants; they proceeded with a review of current literature and then worked to develop a consensus on
current standards of care.
Why Do Disruptive Vocalizations Occur?
Most disruptive vocalization has multiple etiologies.
Nearly all disruptive vocalizers have some form of
brain injury; most have severe dementia due to
Alzheimer's disease or cerebrovascular disease
(Cariaga et al., 1991; Cohen-Mansfield et al., 1990; Halberg et al., 1990). Most are physically impaired because
of their dementia, are dependent in ambulation, transfer, and toileting, and have urinary incontinence
(Cariaga et al., 1991; Cohen-Mansfield et al., 1990; Halberg et al.,1990; Teri, Borson, Kiyak, & Yamagishi, 1989).
Nelson (1995) postulated that vocalizations arise because either (a) environmental stimuli exceed the individual's stress threshold, (b) an individual with low
deprivation tolerance has unmet needs, or (c) an individual is reacting to a perceived threat to personal
freedom. Halberg et al. (1990) found a high prevalence
of delusions, hallucinations, disorientation, anxiety,
and restlessness among disruptive vocalizers; they
suggested that environmental factors, sensory deprivation, and brain damage interact to potentiate this
behavior. Cohen-Mansfield et al. (1990) found signifi-
cant relationships between disruptive vocalization and
poor social networks, sleep disruption, restraint use,
past exposure to a life-threatening experience, falls,
being alone, being touched, depressed affect, perceived pain levels, and other agitated behaviors. Thus,
a variety of factors appear capable of provoking or aggravating disruptive vocalizations.
In clinical practice, it is useful to consider that most
disruptive vocalization reflects either an unmet need
or a response to physical or environmental stimuli
(Algase et al., 1996; Lawton & Nahemow, 1973). The
vocalizer is incapable of fully understanding or of responding to stimuli in a normal manner and therefore communicates in this socially disruptive manner. Diffuse brain disease is the underlying factor,
because (a) damage to orbitofrontal structures leads
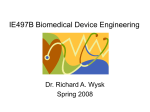
to disinhibition and (b) injury to dorsolateral prefrontal structures leads to deficits in decision making. In susceptible persons, DV can be triggered by a
variety of stimuli, including the physical environment, characteristics of the resident, and caregiver
behaviors (see Figure 1).
Environmental overstimulation often triggers the
vocalizations. An important element of overstimulation is inability to understand what is happening, for
example, in caregiving situations. Often, vocal patterns indicate that the resident feels stressed; "go
away" or "leave me alone" are common vocalizations
of such persons. Overstimulation should be suspected in residents who vocalize during personal
care (especially bathing or dressing), activities (especially congregate meals), and other situations in
which they are around other people. Vocalization in
the late afternoon, between 3 and 5 p.m., is often attributed to "sundowning"; however, commotion associated with shift change is often the trigger (Burgio
et al., 1994; Burgio, Scilley, Hardin, Hsu, & Yancey,
1996).
At times, environmental understimulation may be
responsible for the genesis of DV. This is particularly
likely if the resident has hearing loss, visual impairment, or other sensory deprivation; these conditions
in turn lead to isolation, loneliness, and misinterpretation of the environment. Vocal self-stimulation can
result, often characterized by moans or repetitious
676
Neurologic/cognitive
impairment
•Language problems
•Perceptual problems
•Impaired problem
solving/coping
•Disinhibition
Other internal factors
•Sensory deprivation
•Psychological distress
•Discomfort/pain
•Fatigue
•Psychotic disorders/
symptoms
External factors
•Environmental
•overstlmulatlon
•undtntlmulitlon
•mlspcrctptlon of
stimuli
•Caregiver behaviors
•ptrctlvtd as threat
•dtmMnorfapproach
•restriction of freedom
1
I
I Disruptive vocalization |
Figure 1. Genesis of disruptive vocalization (DV). DV generally
arises in individuals with cognitive or other neurologic impairment when subjected to certain internal and/or external factors.
The Gerontologist
noises such as "na-na-na-na-na-na." That problem
can be aggravated by the fact that people with hearing impairment are unable to appreciate the loudness of their vocalizations.
Immobility and restriction of movement also appear to underlie some disruptive vocalizations. All individuals desire to have some mastery of their environment; being able to move about on one's own
provides an energy outlet and a sense of control. Immobility resulting from severe physical impairment
or the use of restraining devices can leave the individual feeling isolated and unable to express needs.
Thus, "girlie," "nurse, nurse," and "get me up" are
expressions by persons with impaired mobility.
Pain and discomfort frequently trigger disruptive
vocalizations. Cariaga et al. (1991) noted that nursing
home residents who display DV receive pain medication significantly less often than a comparison population of residents who do not display DV; this may
be because cognitive impairment prevented the disruptive vocalizers from using words to articulate their
discomfort. Contractures, arthritis, fecal impaction,
bladder distention, urinary tract infection, undiagnosed pathological fractures, uncomfortable clothing, reflux esophagitis, ingrown toenails, ill-fitting
dentures, poor dentition, food wads in the palate,
sinus headaches, skin irritation (especially when accompanied by wetness), and full incontinence products are some of the sources of discomfort that have
been identified as precipitants of DV. Sounds particularly suggestive of pain or discomfort include
moans, growls, "ouch," and nonspecific increases in
the loudness of existing vocalizations. Nonverbal
signs such as tears, grimacing, splinting of a limb, or
reluctance to transfer may help identify the disruptive vocalizer with underlying pain.
Many persons with dementia have psychotic symptoms and vocalize because their delusional system
misinterprets the environment, or they have hallucinations. Fear, anxiety, and death generally characterize the vocalizations of such individuals: "You're
gonna kill me," "they're trying to kill my babies," and
"they're coming to get me" are examples of phrases
repeated by individuals with underlying psychotic
symptoms. A clue that helps identify such persons is
that they generally are not comforted by being
around others; even one-on-one interventions can
backfire when delusions are present.
Psychological distress (without psychosis), as manifested by depression, anxiety, and loneliness, can
Table 1. Assessment of the Disruptive Vocalizer
1. Describe the behavior
• who, what, where, when
• loudness, frequency, timing
• nonverbal accompaniment
• how staff and other residents respond
2. Listen carefully to the vocalizations and try to understand the message they are attempting to convey
• listen to content and tone
• try to identify desires and emotions expressed (e.g., pain, loneliness, fear)
• pay attention to nonverbal clues (e.g., grimacing, reaching out)
• try to identify if delusions are present
3. Identify situations that bring on or worsen the vocalization ("triggers")
• environmental ("external") factors such as caregiver behavior, noise, or isolation
• physiological ("internal") factors such as pain on movement, hunger, constipation, or uncomfortable positioning
4. Conduct a medical/physical evaluation
• cognitive status (most persons with DV have dementia; in the cognitively intact look for depression or personality disorder)
• physical examination for:
— new neurologic disease (e.g., stroke)
— new medical problems (e.g., urinary tract infection)
— sensory impairment (especially hearing)
— sources of pain and discomfort (e.g., constipation, arthritis, undetected fractures, toenails, teeth)
— mobility status and complications of immobility (contractures, skin breakdown)
— body positioning if immobile
5. Interview the family
• past history of losses, abuse, stress
• explanation for any names or events contained in vocalizations
• prior psychiatric disease (e.g., psychosis, depression or personality disorder), absence of a severe dementia
6. Identify interventions that appear to stop or reduce the vocalization
• think of the vocalizer as distressed rather than distressing
• assume that the vocalizations occur for a reason, and seek to understand the vocalizer's "internal reality"
• talk with all staff and family about what seems to aggravate and improve the vocalizations (a group brainstorming session can be helpful)
7. Synthesize and develop a management plan
• hold a regular interdisciplinary conference which includes primary caregivers
• identify all possible causes and contributing factors, and agree on the most promising management strategies for each
• try out potential interventions in brief, structured sessions during which DV response to intervention use and withdrawal is monitored
• communicate and consistently implement your management plan
• reevaluate frequently
Vol. 37, No. 5,1997
677
both underlie and trigger DV. Interviews with families of DV patients often reveal prior unhappy experiences, abusive situations, or other unfinished business. For example, one resident hollered, "my father
got me pregnant" for hours every day; in fact, this
had happened in her past. The vocalizations themselves can give clues to psychic distress; crying or expressions such as "let me die" suggest depression;
"help me" or "oh my God" suggest anxiety; calling
out "nurse" or a family member's name suggests
loneliness. In advanced dementia, specific psychological symptomatology may be difficult to understand or interpret; persons who are less cognitively
impaired should be evaluated using DSM-IV criteria
(American Psychiatric Association, 1994).
Certain caregiver behaviors can both trigger and
perpetuate DV. Activities such as bathing and dressing are often misinterpreted or misunderstood by
persons with dementia, and the activities themselves
can be demeaning and uncomfortable. For these reasons, agitated behaviors often occur during personal
care activities (Beck et al, 1990). One study of DV
(Cohen-Mansfield et al., 1990), found that the majority of "screamers" do so only for short periods of
time, generally during caregiving, but that in some
individuals DV can persist for hours.
Appropriate caregiver attention, which will be discussed further under the management of DV, can reduce the frequency or duration of vocalizations (Burgio et al., 1994). Certain caregiver responses, however, such as intermittently providing attention to
residents while they are vocally disruptive and ignoring them when they are not, can aggravate DV. Indeed, some "disruptive" vocalization can be considered an adaptive response, for example, when a
resident needs to be taken to the bathroom, calls out
repeatedly, and staff are not immediately available.
Other factors that may be involved in the genesis
of disruptive vocalizations include fatigue and vocal
tics. Any existing behavioral disturbance tends to be
worsened by fatigue; this is also true of many disruptive vocalizers. Vocal tics have been suggested as a
neurological basis underlying DV in some patients
(Rabins, 1994); thus, in some individuals the vocalizations may represent an irresistible compulsion simi-
lar to the vocal expressions of some persons with
Tourette's syndrome.
Finally, we should mention two diagnoses that can
occasionally lead to repetitive vocalization in the absence of cognitive impairment: personality disorders
and psychotic depression. Individuals with these conditions are relatively rare in nursing facilities. Persons
with Axis II Cluster B personality disorders (e.g., borderline, histrionic, antisocial, narcissistic) generally
have a long history of personality pathology; their vocalizations usually reflect an underlying difficulty with
being alone and often constitute an attention-getting
device. Typically, such individuals use critical or sarcastic words and are not excessively loud. They are
often skilled at detecting weak spots or vulnerabilities
in staff members and, therefore, get under their skin
using expressions such as "I know you're not taking
care of me." People with psychotic depression will
scream, moan, or cry out with expressions such as
"I'm going to die" because their profound depression
is accompanied by morbid delusions.
Assessment. — Assessment of the person with DV
should be multidisciplinary. It should include obtaining a careful description of the vocalization and the
setting in which it occurs; an attempt to identify the
meaning, antecedents, and consequences of the vocalization; assessment of the cognitive and physical
status of the vocalizer; inquiry into past events and
health problems that may be relevant; and synthesis
of information to formulate a treatment plan. Table 1
outlines the recommended assessment process.
Management. — Persons who produce only occasional disruptive vocalizations often have one or two
causes that can be directly addressed, such as overstimulation. Frequent vocalizers are more complex;
they generally have multiple problems that must be
addressed simultaneously (Lindgren, Hallberg, &
Norberg, 1992). In managing such persons, trial and
error are often involved, and staff often need to be
both ingenious and persistent. Improvement is frequently temporary, and new treatment approaches
then have to be tried.
Table 2. General Principles of Management of Disruptive Vocalization
Consider a variety of approaches. One single approach rarely "cures" a problem vocalizer.
Assess the problem carefully. Look for a variety of factors and solutions.
Agree on a plan of care for all to follow. Disseminate the plan to staff over all shifts.
Remember that DV rarely places anyone in imminent danger. Often, the vocalizations are more disturbing to staff, other residents, and
family members than to the vocalizer.
Do not overreact to acute episodes. Often, the risk of forcibly administering medication or other treatment outweighs the benefit. A mild
sedative such as diphenhydramine or lorazepam is acceptable on a very short-term basis (i.e., for a few days), while assessment takes
place.
Behavioral and environmental interventions are preferable to medication in the initial management of DV unless there is clear evidence of
depression or psychotic symptoms.
Persons who are less cognitively impaired are more likely to respond to behavioral interventions such as activities; persons with advanced
dementia respond better to comfort measures and environmental measures.
Remind staff not to take the behavior personally, even if it appears to be directed at them. Most vocalizers are too cognitively impaired to
understand what they are doing. It helps to think of the vocalizer as suffering in some way.
678
The Gerontologist
Table 3. Managing Specific Causes of Disruptive Vocalization
Cause or Trigger of Vocalization
Recommended Strategies
Overstimulation
Avoid large group activities and congregate dining
Reduce noise and commotion
Create a more homelike environment
Use a calm, quiet, slow, and consistent caregiving approach
Provide one-on-one caregiving and activities
Provide diffuse, nonglare lighting
Understimulation/Sensory deprivation
Involve resident in social activities
Maximize hearing and vision
Locate resident near activities and traffic
Use microphone and earphones to feed back own sounds (Leverett,
1991)
Introduce environmental sounds by using a loud machine, such as a
hair dryer, or by using audiotape and earphones (Burgio et al., 1994)
Provide high-intensity light therapy (Mishima et al., 1994; Satlin, Vo
licer, Ross, Herz, & Campbell, 1992; Lovell, Ancoli-lsrael, & Gevirtz,
1995)
Provide vibrating or rocking chair
Provide aroma therapy
Provide dolls, stuffed animals, Spinoza bear
Pain/Discomfort
Check skin, toenails, and positioning; look for urine or fecal soiling
Treat underlying diseases and conditions, including constipation
Treat hunger and thirst, if present
Give adequate pain medication as standing dose (not PRN)
Provide appropriate exercise and positioning
Provide massage
Immobility/Restriction of freedom
Provide ambulation or wheeling
Escort resident out doors
Reduce use of restraints
Position person in an area he or she would choose
Provide choices
Delusions and other psychotic symptoms
Maximize hearing and vision
Trial of low-dose, high-potency antipsychotic medication using
standing (not PRN) schedule
Depression
Provide antidepressant medication
Provide reassurance, reminiscence, and other one-on-one activities
Psychological distress without psychosis or major depression
Reduce overstimulation
Provide comforting touch, massage
Instruct staff to verbally reassure resident that he/she is safe
Have one familiar caregiver work with resident one-on-one
Routinize caregiving schedule
Play taped voice of loved one
Plan spiritual activities such as hymn singing, taped rosary, visit from a
clergyman, or attendance at a church service where quiet is
socially expected
Play audiotape of heartbeat
Provide music, especially if associated with pleasant memories
Provide doll, stuffed animal, or Spinoza bear
Provide hot water bottle
Fatigue
Reduce overstimulation
Control length of activities and family visits
Schedule naps
General/Nonspecific treatments
Behavior Therapy (e.g., differential reinforcement)
One-on-one with staff or family member
High intensity light therapy (Mishima et al., 1994; Satlin et al., 1992;
Lovely etal., 1995)
Spiritual activities (see under Psychological Distress)
Sedating, antidepressant, or anticonvulsant medication (Devanand &
Levy, 1995)
Reduce impact of noise on others
Staff education (e.g., that noise-making is often not volitional)
Quiet room; soundproof selected bedrooms
Ear plugs for staff who must provide direct care
Position near hearing impaired
Vol. 37, No. 5,1997
679
General Principles
Each disruptive vocalizer should be approached individually, with the goal of identifying and addressing underlying problems or unmet needs (White,
Kaas, & Richie, 1996). There are, however, some generalizations that are helpful in approaching most vocalizers. These are outlined in Table 2.
Behavioral and environmental treatments are the
mainstay of DV management (White et al., 1996).
They are preferred because, although effectiveness
data are relatively lacking in all treatment areas, behavioral management carries a lower risk of toxicity
than medication. Many behavioral treatment options
are available, so it is important to identify which of
several suggested interventions is most promising
before making it part of a formal care plan. One
method of evaluation is to conduct structured sessions composed of four 5-minute segments during
which a proposed intervention is introduced, removed, re-introduced, and again removed. During
the session, a staff member or volunteer with a watch
and notepad is unobtrusively positioned in a corner
or adjacent room, recording the frequency and duration of DV episodes during each segment. If one or
more of these sessions is conducted for each proposed intervention, the results will constitute data by
which the response to each proposed intervention
can be objectively evaluated and compared (Burgio
et al., 1996). After the effectiveness of the interventions is determined, the amount of time and energy
necessary to train staff in their consistent application
is justified. Staff consistency and training are critical
to successful treatment programs. Interventions that
rely on nursing assistants are likely to fail unless accompanied by a staff management system that involves ongoing performance monitoring and feedback (Burgio & Scilley, 1994).
Treatment strategies for specific causes are presented in Table 3. Management of environmental
overstimulation generally involves reducing or eliminating excessive or troubling stimuli (e.g., replacing
daytime television with selected videotapes; serving
one food item at a time; using one staff member
rather than several for caregiving). Relief of pain and
discomfort involves treating underlying diseases and
specifically addressing the vocalizer's pain; helpful
consultative advice can be obtained from physical
therapy (for mobilization, relief of contractures, and
advice on range of motion) and occupational therapy
(about positioning and feeding). Immobility can be
addressed by relieving associated discomfort and by
providing the resident with opportunities to be active and to make choices.
Sensory deprivation responds to sensory stimulation either through improvement of hearing and vision, through the introduction of pleasant stimuli
(such as aromas, music, and/or a vibrating chair), direct sensory feedback about the vocalization (e.g.,
through a microphone attached to earphones). Fatigue is addressed by ensuring that the vocalizer has
adequate rest and is not overstimulated, and by
scheduling stressful activities (such as a trip to the
dentist) in the morning, when the resident is likely to
be less tired.
Medications are often of limited value in the management of DV; therefore, they are generally used as
an adjunct to behavioral management techniques.
There are, however, several situations in which medication has been specifically shown to be effective and
where early use of pharmacotherapy is indicated:
delusions and psychotic symptoms, major depression, and pseudobulbar affect secondary to bilateral
frontal lobe disease (Schiffer et al., 1985). Medication
is often tried in recalcitrant cases of DV even when
the indications cited above are absent; in these situations, reports on medication effectiveness are largely
anecdotal, and therapy often must be approached as
trial and error (Teri et al., 1992). Indeed, dementia has
been shown to affect the dopaminergic, cholinergic,
and seratoninergic systems, and a variety of medications theoretically could be effective. Table 4 provides
general empiric guidelines for medication use in DV.
One-on-one attention from staff and families is a
commonly used intervention; it reduces vocalizing in
many persons with DV. One-on-one attention is
quite time-intensive; therefore, its major usefulness
is in aborting episodes in intermittent vocalizers.
When noisemaking is more persistent, family and
volunteers should augment staff time when possible.
Unless consistently employed as part of a behavior
therapy program, however, one-on-one attention will
not have lasting effects on frequent vocalizers and
may even increase DV frequency by reinforcing the
Table 4. Guidelines for Medication Use in Disruptive Vocalization
Medications are of limited effectiveness and run a significant risk of adverse effects in the management of DV. In some individuals, however, they provide a valuable adjunct to behavioral management techniques.
Drugs that have low adverse effect profiles should be used. Begin with low doses and increase slowly.
Effects are cumulative; therefore, trials should use standing doses, not PRN.
Antipsychotics should be prescribed for most vocalizers with psychotic symptoms; those with fewest anticholinergic effects (e.g., risperidone, haloperidol, thiothixene) are preferred.
Benzodiazepines should be prescribed with great caution; there are no objective data of effectiveness, and side effects are common.
The fact that low serotonin has been associated with impulsivity provides a rationale for use of medications with serotonergic properties
(e.g., buspirone, trazodone, and selective serotonin re-uptake inhibitors).
Persons with sudden unexplained vocalizations or crying spells (pseudobulbar affect) often respond to antidepressants.
In resistant cases, especially if physical violence is also present, anticonvulsants (e.g., valproic acid or carbamazepine) may be considered
Psychostimulants (methyphenidate or dextroamphetamine) may be considered in persons with depressive symptoms who fail to respond
to traditional antidepressants
680
The Gerontologist
undesired behavior. Activities that help calm vocalizers include sitting with them, walking or wheeling
with them, and talking at an audible level for the vocalizer. Some (but not all) vocalizers respond favorably to touch; try stroking the hair, holding a hand,
and massaging hand, foot, or back.
Behavior therapy is a family of interventions that
has been shown to be effective in modifying a variety
of behaviors; it should be used only when there is no
unmet need that can be addressed more directly.
One behavior therapy technique is called differential
attention. Assuming that the vocalizer enjoys social
contact, he or she is provided with staff, family, or visitor attention as a reward for being quiet rather than
for being noisy. Other rewards can include food (e.g.,
ice cream), tobacco or snuff, and contact with animals or children. Even highly demented disruptive
vocalizers can respond; however, response is generally gradual, requiring a period of many weeks. Consistent implementation of the behavior management
program by all staff is crucial to success (Burgio et al.,
1995; Christie & Ferguson, 1988).
Reducing the Impact of DV on Others
Many problem vocalizers cannot be totally quieted
without an unhealthy degree of sedation. In such
cases, it is important to take steps to reduce the impact of the noise on staff and other residents. Staff
education and consistency are the most important issues; staff should realize that the vocalizations are
not willful or directed at caregivers. During periods
of high noise production, isolating the vocalizer for a
short period of time in a quiet room or soundproofed area (with frequent staff monitoring) can
provide relief to staff and other residents; units that
house behaviorally disruptive persons with late-stage
dementia should construct some rooms with extra
soundproofing for such residents. Placing a vocalizer
near hearing-impaired residents or other repetitive
vocalizers has been reported to help at times. Finally,
in rare cases, caregivers may be permitted to wear
earplugs when providing direct care to a severely disruptive vocalizer. When measures to reduce noise
impact are instituted, staff should understand that
care for the vocalizer must continue to be provided.
References
Algase, D. L, Beck, C , Kolanowski, A., Whall, A., Berent, S., Richards, K., &
Beattie, E. (1996). Need-driven dementia-compromised behavior: An alternative view of disruptive behavior. American Journal of Alzheimer's
Disease, 77(6), 10-19.
Alzheimer, A. (1906). A characteristic disease of the cerebral cortex. In: The
early story of Alzheimer's disease. New York: Raven Press.
American Psychiatric Association. (1994). Diagnostic and statistical manual of
mental disorders (4th ed.). Washington, DC: Author.
Beck, C, Baldwin, B., Modlin, T., & Lewis, S. (1990). Caregivers' perception of
aggressive behavior in cognitively impaired nursing home residents.
Journal of Neuroscience Nursing, 22,169-172.
Burgio, L D., Cotter, E. M., Stevens, A. B., Hardin, J. M., Sinnott, J., & Hohman,
M. J. (1995). Elders' acceptability rating of behavioral treatments and
pharmacotherapy for management of geriatric behavioral disturbances.
The Gerontologist, 35,630-636.
Burgio, L. D. & Scilley, K. (1994). Caregiver performance in the nursing home:
The use of staff training and management procedures. Seminars in
Speech and Language, 15, 313-322.
Burgio, L, Scilley, K., Hardin, J. M., Hsu, C, & Yancey, J. (1996). Environmental "white noise": An intervention for verbally agitated nursing home
residents. Journal of Gerontology: Psychological Sciences, 51B,
P364-P373.
Burgio, L. D., Scilley, K., Hardin, M., Janosky, J., Bonino, P., Slater, S. C, & Engberg, R. (1994). Studying disruptive vocalization and contextual factors
in the nursing home using computer-assisted real time observation.
Journal of Gerontology: Psychological Sciences, 49, P230-P239.
Cariaga, J., Burgio, L. D., Flynn, W., & Martin, D. (1991). A controlled study of
disruptive vocalization among geriatric residents in nursing homes. Journal of the American Geriatrics Society, 39,501-507.
Christie, M., & Ferguson, C. (1988). Can anyone stop that screaming? Canadian Nurse, 84 (October), 30-32.
Cohen-Mansfield, J., Marx, M., & Rosenthal, A. (1989). A description of agitation in a nursing home. Journal of Gerontology: Medical Sciences, 44,
M77-M84.
Cohen-Mansfield, J., Werner, P., & Marx, M. (1990). Screaming in nursing
home residents. Journal of the American Geriatrics Society, 38,785-792.
Devanand, D. P., & Levy, S. R. (1995). Neuroleptic treatment of agitation and
psychosis in dementia. Journal of Geriatric Psychiatry and Neurology,
8(SuppM),S18-S27.
Hallberg, I. R., Norberg, A., & Erikson, S. (1990). Functional impairment and
behavioral disturbances in vocally disruptive patients in psychogeriatric
wards compared with controls. International Journal of Geriatric Psychiat/y, 5,53-61.
Lawton, M. P., & Nahemow, L. (1973). Ecology and the aging process. In C.
Eisdorfer & M. P. Lawton (Eds.), The psychology of adult development
and aging. Washington, DC: American Psychological Association.
Leverett, M. (1991). Approaches to problem behaviors in dementia. Physical
and Occupational Therapy in Geriatrics, 9,93-105.
Lindgren, C , Hallberg, I. R., & Norberg, A. (1992). Diagnostic reasoning in
the care of a vocally disruptive severely demented patient. Scandinavian
Journal of Caring Science, 6,97-103.
Lovell, B. B., Ancoli-lsrael, S., & Cevirtz, R. (1995). Effect of bright light treatment on agitated behavior in institutionalized elderly subjects. Psychiatry Research, 57, 7-12.
Mishima, K., Okawa, M., Hishikawa, Y., Hozumi, S., Hori, H., & Takahashi, K.
(1994). Morning bright light therapy for sleep and behavior disorders in
elderly patients with dementia. Acta Psychiatrica Scandinavica, 89,1-7.
Nelson, J. (1995). The influence of environmental factors in incidents of disruptive behavior. Journal of Gerontological Nursing, 27(5), 19-24.
Rabins, P. V. (1994). Noncognitive symptoms in Alzheimer's disease. In R. D.
Terry (Ed.), Alzheimer's disease. New York: Raven Press.
Rosby, L., Beck, C , & Heacock, P. (1992). Disruptive behaviors of a cogni-
Unanswered Questions
So much is unknown about repetitive vocalizers
that the list of unanswered questions would be
lengthy indeed. Studies of the epidemiology and
natural history of DV are needed; the following are
some of the unanswered questions: Do certain behaviors (e.g., motor agitation) predate and constitute a risk for DV? If so, stopping the first link in the
chain of behavior might constitute effective prevention. Is DV a predictor of other, more dangerous,
behaviors, such as physical aggression? Is it a predictor of impending death? Do women tend to vocalize more than men? Is DV more common in vascular dementia? The extent to which such
vocalizations have neuroanatomic correlates (e.g.,
frontal lobe lesions have been associated with disVol. 37, No. 5,1997
inhibition, basal ganglia lesions with impulsive vocalization) is also unknown.
Few systematic data exist concerning the management of DV. We know that no single intervention
works for all, and that the effectiveness of interventions changes over time in the same individual; thus,
we need to learn how to target interventions to certain individuals and subgroups. Very few treatments
have been subjected to randomized trials, but even
in these cases we do not know whether the interventions can be effectively carried out in nonresearch
settings. Whether the effects of interventions are
durable is also unstudied. Finally, the role and effectiveness of medications in these problem patients is
a largely unstudied issue.
681
cognitive dysfunction, and functional skill. Journal of the American Geriatrics Society, 37,109-116.
Teri, L, Rabins, P., Whitehouse, P., Berg, L, Reisberg, B., Sunderland, T.,
Eichelman, B., & Phelps, C. (1992). Management of behavior disturbance
in Alzheimer disease: Current knowledge and future directions.
Alzheimer Disease and Associated Disorders, 6, 77-88.
White, M. K., Kaas, M. J., & Richie, M. F. (1996). Vocally disruptive behavior.
Journal of Gerontological Nursing, 22(11), 23-29.
tively impaired nursing home resident. Archives of Psychiatric Nursing,
6, 98-107.
Ryan, D. P., Tainsh, S. M. M., Kolodny, V., Lendrum, B. L, & Fisher, R. H.
(1988). Noise making amongst the elderly in long term care. The Cerontologist, 28,369-371.
Satlin, A., Volicer, L, Ross, V., Herz, L, & Campbell, S. (1992). Bright light
treatment of behavioral and sleep disturbances in patients with
Alzheimer's disease. American Journal of Psychiatry, 149,1028-1032.
Schiffer, R. B., Herndon, R. M., & Rudick, R. A. (1985). Treatment of pathologic laughing and weeping with amitriptyline. New England Journal of
Medicine, 312,1480-1482.
Teri, L, Borson, S., Kiyak, A., & Yamagishi, M. (1989). Behavioral disturbance,
Received July 15, 7996
Accepted April 25,1997
682
The Gerontologist