Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
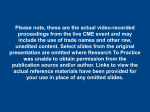
Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Can the Lung Cancer Pie Be Divided into Angiogenic Slices? Tina Cascone1 and John V. Heymach2,3 1 Division of Cancer Medicine, 2,3Departments of Thoracic, Head and Neck Medical Oncology and Cancer Biology. The University of Texas MD Anderson Cancer Center, Houston, Texas. Corresponding Author: John V. Heymach, Departments of Thoracic, Head and Neck Medical Oncology, and Cancer Biology, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Unit 432, Houston, TX 77030. Phone: 713-792-6363; Fax: 713-792-1220; E-mail: [email protected] Running Title: Predictive Markers for VEGF and EGFR Inhibition in NSCLC Disclosure of Potential Conflicts of Interest J.V. Heymach reports receiving commercial research grants from AstraZeneca, Bayer, and GlaxoSmithKline, and is a consultant/advisory board member for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Exelixis, Genentech, GlaxoSmithKline, Novartis, and Synta Pharmaceuticals. No potential conflicts of interest were disclosed by the other author. Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Summary There are no validated markers for predicting benefit from angiogenesis inhibitors or classifying tumors with distinct angiogenic phenotypes. In NSCLC patients treated with bevacizumab and erlotinib, Franzini and colleagues find that angiogenesis- and hypoxiaassociated gene expression signatures predict tumor response and/or clinical outcome, and may define distinct angiogenic patterns. 2 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. In this issue of Clinical Cancer Research, Franzini and colleagues (1) investigate the association between angiogenesis- and hypoxia-related gene expression signatures and clinical outcome in non-squamous non-small cell lung cancer (NSCLC) patients treated with the Vascular Endothelial Growth Factor (VEGF) inhibitor bevacizumab plus the Epidermal Growth Factor Receptor (EGFR) inhibitor erlotinib. A remarkable advance in the treatment of NSCLC, and other cancers, is the development of biomarker-defined classifications that help define subgroups likely to benefit from particular targeted agents. The major genomically-defined “slices of the pie” for NSCLC are now familiar, such as those marked by EGFR, ALK, or BRAF alterations. Immunotherapy is rapidly moving in a similar direction; emerging data already supports that tumors expressing varying amounts of PD-L1 on tumor or immune cells may derive different degrees of benefit from agents targeting the PD-1/PD-L1 axis, and more refined immune classifications are no doubt on the way (2). Given this progress, it is perhaps surprising that after about two decades of testing angiogenesis inhibitors such as the anti-VEGF monoclonal antibody bevacizumab, we still do not have clinically useful markers for classifying tumors based on their angiogenic phenotype, or for predicting which patients are more likely to benefit from these drugs. This is surely an important unmet need, given that only a minority of patients derive significant benefit from bevacizumab, serious toxicities may occur, and resistance inevitably occurs. Bevacizumab significantly improves clinical outcomes when added to platinumbased chemotherapy in NSCLC (3). The addition of bevacizumab to erlotinib did not prolong survival compared with erlotinib in the overall platinum- refractory NSCLC 3 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. population, but two randomized phase III studies suggest that bevacizumab plus erlotinib may be superior to erlotinib alone among EGFR mutation positive patients (4, 5). Outside of EGFR mutation, there are currently no validated markers for identifying which patients are more likely to benefit from bevacizumab when added to either chemotherapy or erlotinib. Franzini and colleagues (1) performed gene expression profiling on bronchoscopic biopsies from 42 patients with stage IIIB/IV non-squamous NSCLC enrolled in the Swiss Group for Clinical Cancer Research 19/05 phase II trial (6) and treated with bevacizumab and erlotinib. Pretreatment gene expression profiles were correlated with clinical outcomes (tumor shrinkage [TS], time to progression [TTP], and OS) and then subjected to gene set enrichment analysis (GSEA) using a 43-gene core angiogenesis signature and a 51-gene hypoxia signature, previously reported. GSEA revealed that both angiogenic and hypoxic-associated signatures are enriched within genes that associate with TTP under bevacizumab and erlotinib therapy. Further unsupervised hierarchical clustering of the top 10-ranked angiogenesis-associated genes revealed that patients with increased expression of angiogenic genes at baseline (low risk) possess an improved median TTP (7.1 months) versus a 2.1 month median TTP in patients with a decreased signature (high risk). Patients with a diminished hypoxiasignature (low-risk) had a prolonged median TTP (6.9 months) versus a 2.9 month median TTP in patients with elevated levels (high risk). Unlike the angiogenesis signature, increased expression of the hypoxia signature was predictive of TS after 12 weeks of bevacizumab plus erlotinib, suggesting that it may possess greater potential for assessing treatment response. Furthermore, both signatures 4 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. were found to have prognostic value for OS, as the median OS for patients with elevated hypoxia signature expression was 9.9 months versus 17.8 months in patients with decreased levels. While hypoxia-inducible factor 1-alpha (HIF-1α) was not identified as predictive for TTP, several of its downstream targets were components of the hypoxia signature. These results agree with previously reported studies demonstrating that hypoxia correlates with a more aggressive phenotype, perhaps by enhancing malignant potential through increased genomic instability and by acting as selective pressure for variants with diminished apoptotic potential (7). Assuming the associations described between the angiogenic and hypoxia response signatures are robust, important issues would need to be addressed before they could be used in selecting therapy. In the absence of a control arm, it is not possible to determine whether the signatures are predictive of benefit for bevacizumab plus erlotinib compared with another therapy, or merely prognostic. Caution should be used in assuming that markers associated with improved clinical outcome in a single arm study will be predictive of greater relative benefit compared with another drug in a randomized study. For example, we previously observed that high circulating IL-6 is a negative prognostic marker in metastatic renal cell cancer, but predicts greater relative benefit for patients receiving pazopanib compared with placebo control (8). Such observations would not be evident in a single arm study. Clinically useful predictive biomarkers typically help inform the choice between different therapies. It remains to be seen whether the angiogenic or hypoxia signatures could be used to predict, for example, which patients benefit from bevacizumab in combination with chemotherapy compared with chemotherapy alone. Interestingly, the 5 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. authors report an association between the hypoxia signature and PFS in the sorafenib, but not erlotinib, arm of the BATTLE study, suggesting the signature may have utility for other drugs targeting the VEGF pathway (9, 10). Given the current NSCLC landscape, it would also be important to assess whether the signatures are predictive of benefit within the standard molecularly defined subgroups. As noted above, bevacizumab appears to add greater benefit in the EGFR mutation positive subgroup (4, 5). It would therefore be important to assess the signatures in the EGFR-mutant and wild-type groups separately. The mechanism underlying the apparently increased sensitivity of EGFR mutant tumors to VEGF blockade is not well understood, but it is noteworthy that constitutive EGFR pathway activation results in upregulation of VEGF and the HIF-1α pathway (11), suggesting there may be overlap between EGFR and VEGF pathway dependence. The authors suggest that the signatures are associated with distinct vascular patterns; for example, vessels from tumors most likely to respond to bevacizumab and erlotinib appear to possess a greater level of integrity and are less permeable compared with vessels supplying less responsive tumors. It is known that expression levels of genes encoding proteins critical to endothelial barrier function and vessel integrity are elevated in tumors of patients with improved response to bevacizumab and erlotinib. The authors conclude that when angiogenesis-associated genes are diminished, tumor angiogenesis is dysregulated, resulting in hyperpermeable vasculature, increased hypoxia and earlier disease progression (Fig. 1). Previous studies illustrate that different angiogenic phenotypes impact tumor response to angiogenesis inhibition. For example, we previously showed (12) that NSCLC xenografts which were less responsive to prolonged 6 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. bevacizumab are supplied by tortuous and pericyte-devoid tumor-associated vessels, whereas a more normalized revascularization characterizes NSCLC xenografts with acquired resistance to long-term treatment. It is now widely accepted that genomic phenotypes of a variety of cancers, such as EGFR mutant NSCLC or BRAF mutant melanoma, impact the response to targeted therapeutic strategies in distinct subgroups of patients. However, the search for biomarkers capable of defining distinct angiogenic phenotypes, and identifying NSCLC patients most likely to derive clinical benefit from anti-angiogenic therapies, has proved challenging. The findings reported by Franzini and colleagues (1), while not ready for immediate clinical application, may be a promising step forward towards addressing our collective hunger for angiogenic slices of the NSCLC pie. Grant Support J.V. Heymach is supported in part by the UT Lung Spore (P50CA070907); an NIH Cancer Center Support Grant (P30CA16672); an NCI R01 award (R01CA168484); the V Foundation for Cancer Research; the LUNGevity Foundation; Uniting Against Lung Cancer; the Lung Cancer Research Foundation; and generous philanthropic contributions to The University of Texas MD Anderson Lung Moon Shot Program, the Dell Fund honoring Lorraine Dell, Rexanna’s Foundation for Fighting Lung Cancer, and the Bruton Endowment for Tumor Biology. Acknowledgments The authors thank Emily B. Roarty, PhD, for providing expert editorial assistance. References 7 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. 1. Franzini A, Baty F, Macovei, II, Dürr O, Droege C, Betticher D, et al. Gene expression signatures predictive of bevacizumab/erlotinib therapeutic benefit in advanced nonsquamous non–small cell lung cancer patients (SAKK 19/05 trial). Clin Cancer Res 2015 Apr 28. [Epub ahead of print]. 2. Schumacher TN, Kesmir C, van Buuren MM. Biomarkers in cancer immunotherapy. Cancer Cell 2015;27:12-4. 3. Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med 2006;355:2542-50. 4. Herbst RS, Ansari R, Bustin F, Flynn P, Hart L, Otterson GA, et al. Efficacy of bevacizumab plus erlotinib versus erlotinib alone in advanced non-small-cell lung cancer after failure of standard first-line chemotherapy (BeTa): a double-blind, placebocontrolled, phase 3 trial. Lancet 2011;377:1846-54. 5. Seto T, Kato T, Nishio M, Goto K, Atagi S, Hosomi Y, et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous nonsmall-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol 2014;15:1236-44. 6. Zappa F, Droege C, Betticher D, von Moos R, Bubendorf L, Ochsenbein A, et al. Bevacizumab and erlotinib (BE) first-line therapy in advanced non-squamous non-smallcell lung cancer (NSCLC) (stage IIIB/IV) followed by platinum-based chemotherapy (CT) at disease progression: a multicenter phase II trial (SAKK 19/05). Lung Cancer 2012;78:239-44. 8 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. 7. Vaupel P. The role of hypoxia-induced factors in tumor progression. Oncologist 2004;9 Suppl 5:10-7. 8. Tran HT, Liu Y, Zurita AJ, Lin Y, Baker-Neblett KL, Martin AM, et al. Prognostic or predictive plasma cytokines and angiogenic factors for patients treated with pazopanib for metastatic renal-cell cancer: a retrospective analysis of phase 2 and phase 3 trials. Lancet Oncol 2012;13:827-37. 9. Kim ES, Herbst RS, Wistuba II, Lee JJ, Blumenschein GR Jr, Tsao A, et al. The BATTLE trial: personalizing therapy for lung cancer. Cancer Discov 2011;1:44-53. 10. Blumenschein GR Jr, Saintigny P, Liu S, Kim ES, Tsao AS, Herbst RS, et al. Comprehensive biomarker analysis and final efficacy results of sorafenib in the BATTLE trial. Clin Cancer Res 2013;19:6967-75. 11. Xu L, Nilsson M, Hanrahan E, Cascone T, Yang Y, kurie j, et al. Activated EGFR regulates invasiveness of non-small cell lung cancer cells through HIF-1{alpha} mediated Met expression [abstract]. In: Proceedings of the 98th AACR Annual Meeting; 2007 Apr 14-18; Los Angeles, CA. Philadelphia (PA): American Association for Cancer Research; 2007. Abstract nr. 345. 12. Cascone T, Herynk MH, Xu L, Du Z, Kadara H, Nilsson MB, et al. Upregulated stromal EGFR and vascular remodeling in mouse xenograft models of angiogenesis inhibitor-resistant human lung adenocarcinoma. J Clin Invest 2011;121:1313-28. 9 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Figure 1. Angiogenesis- and hypoxia-associated gene expression signatures predict response of NSCLC tumors to combined bevacizumab and erlotinib therapy. Patients with tumors characterized by a robust angiogenesis gene signature and a decreased hypoxia-associated gene signature (upper panel) display increased tumor shrinkage and improved outcome. Gene expression data predict that tumor-associated vascular bed of these tumors is formed through controlled, sustained angiogenesis and that the vasculature is less permeable compared with the vascular network supplying highly hypoxic tumors, which are less responsive to therapy (lower panel). Abbreviations: OS, overall survival; pO2: partial pressure of oxygen; TS, tumor shrinkage; TTP, time to tumor progression; VEGF, vascular endothelial growth factor. 10 Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Figure 1: i TS i TTP pO2 i OS pO2 k TS k TTP Tumor cell k OS Pericyte Endothelial cell Macromolecule VEGF Bevacizumab Erlotinib © 2015 American Association for Cancer Research Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research. Author Manuscript Published OnlineFirst on July 31, 2015; DOI: 10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Can the Lung Cancer Pie Be Divided into Angiogenic Slices? Tina Cascone and John V. Heymach Clin Cancer Res Published OnlineFirst July 31, 2015. Updated version Author Manuscript E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: doi:10.1158/1078-0432.CCR-15-1180 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on June 17, 2017. © 2015 American Association for Cancer Research.