Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
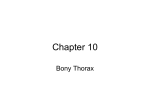
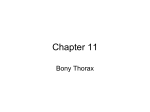
7 Anatomy and Blood Supply of the Sternum Winfried Neuhuber, Stefan Lyer, Christoph Alexiou, and Thomas Buder 2.1 Bony Anatomy – 8 2.2 Relationship to Muscles – 8 2.3 Development – 9 2.4 Arterial Supply – 10 References – 11 R. E. Horch et al. (Eds.), Deep Sternal Wound Infections, DOI 10.1007/978-3-662-49766-1_2, © Springer-Verlag GmbH Deutschland 2017 2 2 8 Chapter 2 · Anatomy and Blood Supply of the Sternum 2.1 Bony Anatomy The sternum is a sword-shaped flat bone about 15–17 cm long in the adult (. Fig. 2.1) (Putz and Müller-Gerbi Benninghoff 2003; Williams and Warwick 1980). Its cranial part, the manubrium, connects to the corpus by a synchondrosis in 90% of adults; in the remaining 10% there is a bony fusion (synostosis). Its caudal part, the xiphoid process, is cartilaginous in youth, but more or less ossified and fused with the corpus in adults. The sternum is slightly convex ventrally emphasized by the individually variable sternal angle (. Fig. 2.1). The clavicle and the cartilage of the first rib articulate on the lateral margin of the manubrium while the cartilages of ribs two through seven insert from the manubrium–corpus connection caudalward on the lateral edge of the corpus, partly by true synovial joints. These articulations correspond to the borders between the primitive segments of the developing sternum, the so-called sternebrae. Sternocostal ligaments arranged criss-cross ventrally and dorsally connect the sternum with the rib cartilages, fusing with both their periosteum and perichondrium, respectively, thus forming a rather firm membrane especially on the ventral side. The cortical bone of the sternum is thickest in the manu brium but relatively thin in the other parts. The spongiosa is lightly constructed with wide inter trabecular spaces containing red bone marrow (. Fig. 2.2) (Whitehouse 1975). 2.2 ..Fig. 2.1 Anterior view of a macerated adult sternum. Costal cartilages were modeled of plastic. The manubrium (M) is connected to the corpus (C) by cartilage at the sternal angle (red arrow). Black arrows point to transverse ridges indicating the fusion lines between the sternebrae. Percentages indicate the relative prevalence of collateral sternal rami from the first to the sixth intercostal spaces. Xiphoid process (X) Relationship to Muscles Ventrally, the sternum provides attachment to the sternal portion of the pectoralis major, dorsally to the transversus thoracis. The xiphoid process provides attachment to the aponeuroses of the oblique and transverse abdominal muscles and the sheath of the rectus abdominis formed by them; the linea alba is attached to its apex. From its dorsal aspect originates the sternal portion of the diaphragm. A sternal muscle is found in about 3% of cases on the ventral side of the sternum (Testut 1884). ..Fig. 2.2 Midsaggital section through the sternum emphasizing the cortical bone and spongiosa. In this case, the manubrium is fused to the corpus by synostosis 9 2.3 · Development 2.3 2 Development The sternum develops from bilateral paramedian cartilaginous sternal plates that interconnect the costal anlagen. Upon their midline fusion in early fetal life, several ossification centers emerge that form the manubrium and four bony plates in the region of the corpus, the sternebrae (. Fig. 2.3). They fuse during adolescence, while the connection between the manubrium and corpus remains cartilaginous in the great majority of adults (. Fig. 2.1). Transverse ridges on the anterior surface of the adult sternum indicate the fusion lines. The second through sixth or seventh ribs insert at these lines, and thus the intersegmental position of the sternebrae is evident. As the arterial supply of the developing sternum is directed to the ossification centers of the sternebrae, an intersegmental pattern of arterial branches to the sternum (rami sternales) is defined (. Fig. 2.3, . Fig. 2.4) (Putz and Müller-Gerbi 2003; Williams and Warwick 1980). a ..Fig. 2.3 Posterior view of an infant sternum with attached ribs. The large ossification center on top will form the manubrium, the four smaller will form the sternebrae of the corpus. Red arrows indicate the intersegmental arteries to ossification centers. ITA internal thoracic artery and vein, MPHA musculophrenic artery. Historic specimen, late eighteenth century. (Courtesy of Anatomy Collection of the Institute of Anatomy, University of Erlangen-Nürnberg) b ..Fig. 2.4 Three-dimensional reconstruction of a postmortem computed tomographic digital subtraction angiography of the internal thoracic artery (ITA) of an 80-year-old female body donor. Iodine contrast agent (Imeron 350, Bracco Altana Pharma, Konstanz, Germany, diluted 1:1 with 0.9% NaCl, 175 mg/ml iodine) was injected manually into the right artery (RITA) filling its various ipsilateral branches but also the left artery (LITA) via a commissural vessel (comm) behind the apex of the sternum. Note that the main trunks of the RITA and LITA, the sternal (rs) and intercostal (ic) branches, as well as the commissural and musculophrenic (MPHA) arteries are better visualized in the oblique left posterior (b) than in the oblique left anterior (a) view that emphasizes perforating branches (perf). Data were created using a C-arm cone beam computed tomographic scanner (Siemens Artis zee floor, Siemens Healthcare, Forchheim, Germany). Three-dimensional reconstruction of arteries and skeletal structures in an 8-cm-thick slice volume was achieved using special software (MultiModality Workplace, Siemens Healthcare, Forchheim, Germany) 10 Chapter 2 · Anatomy and Blood Supply of the Sternum 2 a b c d ..Fig. 2.5 Scheme of noncollateral (a) and three types of collateral (b, c, d) sternal rami. In a, the three main branches of the ITA, i.e., the sternal (st), anterior intercostal (ant intercost), and perforating (perf), are depicted as originating separately from the internal thoracic artery (ITA). If the common trunk in b (sternal/intercostal type) is ligated, the collateral sternal circulation is maintained from the posterior intercostal artery (post intercost) via the anterior intercostal ramus. In the sternal/perforating type, the collateral supply of the sternum (ST) in the case of ligation is established from branches of lateral thoracic and/or acromiothoracic arteries in the pectoral muscle (PM) or overlying skin via the perforating branch of the ITA that shares its origin with the sternal ramus. In d, all three branches share a common origin from the ITA. In this sternal/perforating/intercostal type, sources of collateral circulation may be both lateral thoracic/acromiothoracic and posterior intercostal arteries anastomosing with perforating or anterior intercostal rami, respectively. Dashed line indicates the periosteal plexus 2.4 Arterial Supply Detailed studies of the arteries to the sternum have been repeatedly performed over the past four decades prompted by the notorious complications in sternotomy wound healing, particularly if the internal thoracic artery was harvested for coronary bypass. Both anatomical dissection on large series of donated bodies and radiography techniques were used. The major source of branches to the sternum is the internal thoracic or mammary artery (ITA) (. Fig. 2.3, . Fig. 2.4). It originates from the subclavian artery directly or sometimes from a common trunk with another artery of the thyrocervical trunk; this was observed in about 30% of cases on the left but rarely on the right side (Henriquez-Pino et al. 1997; Paliouras et al. 2015). Before entering the mediastinum, it crosses the phrenic nerve either dorsally or ventrally (Owens et al. 1994; Rigaud et al. 1998). This may explain diaphragmatic dys function upon open heart surgery (Abd et al. 1989; Owens et al. 1994; Wilcox et al. 1990). It descends 1–2 cm from the lateral margin of the sternum adjacent to the posterior aspect of the chest wall, partly covered by the transversus thoracic muscle from the third to the sixth costal cartilage. After giving off the musculophrenic artery (. Fig. 2.3, . Fig. 2.4) and passing the level of the diaphragm anterior to the sternocostal triangle (Morgagni’s triangle, often erroneously named after Larrey), the ITA enters the sheath of the rectus abdominis, now termed the superior epigastric artery, and anastomoses with the inferior epigastric artery. Branches to the sternum originate either directly from the medial aspect of the ITA (noncollateral branches) or from short (0.5–8.0 mm) trunks that also give rise to perforating branches to the intercos- 11 References tal and pectoral muscles and overlying skin or to anterior intercostal rami (collateral branches; Berdajs et al. 2006; de Jesus and Acland 1995; Pietrasik et al. 1999) (. Fig. 2.4, . Fig. 2.5). They are very small (range of diameters 0.30–0.92 mm: Gupta et al. 2002; Pietrasik et al. 1999; 0.2–1.6 mm: de Jesus and Acland 1995), run at a distance of less than 5 mm from the sternal edge in almost half of the individuals (de Jesus and Acland 1995), and display considerable interindividual and gender (Itezerote et al. 2012) variability. This is also reflected by the slightly differing descriptions and schematic representations in the various studies. However, two consistent patterns emerged. First, sternal branches are intersegmental, i.e., located in the intercostal spaces and form arcades at the lateral edge of the sternum (Berdajs et al. 2006; Rigaud et al. 1998). This reflects the intersegmental location of ossification centers that are supplied by sternal arteries (Pis’menov and Zapetskii 1977). Second, sternal branches are more frequent in cranial than in caudal segments, in particular in the second and third intercostal space, with some caudal spaces even without any artery (de Jesus and Acland 1995; Gupta et al. 2002; Itezerote et al. 2012). Eighty-six percent of collateral vessels were found in the first to fourth intercostal spaces while only 14% occurred in the fifth and sixth spaces (de Jesus and Acland 1995). Noncollateral sternal branches are more numerous than collateral ones. de Jesus and Acland (1995) reported an average of five noncollateral versus one to three collateral branches, depending on the type, per hemisternum. In the study of Berdajs et al. (2006) of 50 donated bodies, a total of 22 noncollateral branches versus 8 to 17 collateral ones, again depending on type, were described. This highlights the generally precarious arterial supply to the sternum. Based on the origins of the collateral sternal branches, three typical patterns can be defined (. Fig. 2.5): sternal/intercostal (from the anterior intercostal rami of the ITA; collateral supply via an anastomosis between the posterior intercostal arteries and anterior intercostal rami), sternal/perforating (from the perforating rami of the ITA; collateral supply via an anastomosis between the perforating rami and branches of acromiothoracic and/or lateral thoracic arteries: Berdajs et al. 2006; de Jesus and Acland 1995; Palmer and Taylor 1986; Reid and 2 Taylor 1984) and sternal/perforating/intercostal (both sternal and anterior intercostal rami originate from a perforating branch; Berdajs et al. 2006; de Jesus and Acland 1995; Itezerote et al. 2012; Pietrasik et al. 1999). A particular rare type is the persistent posterior intercostal artery that reaches the sternum without anastomosing with the ITA (de Jesus and Acland 1995; Itezerote et al. 2012). In some individuals, a commissural anastomosis between both ITAs can be found (. Fig. 2.4). Arteries reach the anterior and posterior aspects of the sternum, feeding into dense periosteal plexuses, which are better developed on the posterior side (. Fig. 2.4). The plexuses are segmentally organized in infants, corresponding to sternebrae, but are confluent craniocaudally in adults (Pis’menov and Zapetskii 1977). They are apparently also continuous across the midline as the contralateral ITA fills with contrast medium injected into the ipsilateral ITA (Rigaud et al. 1998; . Fig. 2.4). Evidently, harvesting the ITA for coronary bypass will disrupt sternal circulation to a variable extent (Seyfer et al. 1988), although this hypoperfusion may be temporary in most cases (Carrier et al. 1992). This depends on the number and viability of the altogether rare collateral sternal rami and their access to the periosteal plexus of the sternum. Thus, when the ITA is dissected, any branches should be ligated as close as possible to the main vessel in order to preserve collateral branches. Likewise, sternal cerclages should be placed as close as possible to the sternal edge to preserve the arcades between sternal arteries (de Jesus and Acland 1995; Berdajs et al. 2006). jjAcknowledgments We thank Philip Eichhorn for photographical documentation. References Abd AG, Braun NM, Baskin MI, O’Sullivan MM, Alkaitis DA (1989) Diaphragmatic dysfunction after open heart surgery: treatment with a rocking bed. Ann Intern Med 111:881–886 Putz R, Müller-Gerbi M (2003) Rumpf. In: D Drenckhahn (ed) Anatomie (Vol. 1). Urban & Fischer, Munich, pp 412–481 Berdajs D, Zünd G, Turina MI, Genoni M (2006) Blood supply of the sternum and its importance in internal thoracic artery harvesting. Ann Thorac Surg 81:2155–2159 12 2 Chapter 2 · Anatomy and Blood Supply of the Sternum Carrier M, Grégoire J, Tronc F, Cartier R, Leclerc Y, Pelletier LC (1992) Effect of internal mammary artery dissection on sternal vascularization. Ann Thorac Surg 53:115–119 de Jesus RA, Acland RD (1995) Anatomic study of the collateral blood supply of the sternum. Ann Thorac Surg 59:163–168 Gupta M, Sodhi L, Sahni D (2002) Variations in collateral contributions to the blood supply to the sternum. Surg Radiol Anat 24:265–270 Henriquez-Pino JA, Gomes WJ, Prates JC, Buffolo E (1997) Surgical anatomy of the internal thoracic artery. Ann Thorac Surg 64:1041–1045 Itezerote AM, Gomes WJ, Prates JC (2012) Internal thoracic artery: sternal branches and their importance in thoracic surgery. J Morphol Sci 29:44–48 Owens WA, Gladstone DJ, Heylings DJ (1994) Surgical anatomy of the phrenic nerve and internal mammary artery. Ann Thorac Surg 58:843–844 Paliouras D, Rallis T, Gogakos A, Asteriou C, Chatzinikolaou F, Georgios T, Tsirgogianni K, Tsakiridis K, Mpakas A, Sachpekidis N, Zarogoulidis K, Papaiwannou A, Organtzis J, Karapantzos I, Karapantzou C, Zarogoulidis P, Barbetakis N (2015) Surgical anatomy of the internal thoracic arteries and their branching pattern: a cadaveric study. Ann Transl Med 3:212–215 Palmer JH, Taylor GI (1986) The vascular territories of the anterior chest wall. Br J Plast Surg 39:287–299 Pietrasik K, Bakon L, Zdunek P, Wojda-Gradowska U, Dobosz P, Kolesnik A (1999) Clinical anatomy of internal thoracic artery branches. Clin Anat 12:307–314 Pis’menov IA, Zapetskii EV (1977) Regularities and differences in the structure of the circulatory bed of the sternum. Arkh Anat Gistol Embriol 72:61–67 Reid CD, Taylor GI (1984) The vascular territory of the acromiothoracic axis. Br J Plast Surg 37:194–212 Rigaud J, Armstrong O, Robert R, Rogez JM, Le Borgne J (1998) Anatomic bases of aorto-coronary bypasses: the internal thoracic artery and blood supply of the sternum. Surg Radiol Anat 20:191–201 Seyfer AE, Shriver CD, Miller TR, Graeber GM (1988) Sternal blood flow after median sternotomy and mobilization of the internal mammary arteries. Surgery 104:899–904 Testut L (1884) Les anomalies musculaires chez l’homme. Masson, Paris, pp 74–88 Whitehouse WJ (1975) Scanning electron micrographs of cancellous bone from the human sternum. J Pathol 116:213–224 Wilcox PG, Paré PD, Pardy RL (1990) Recovery after unilateral phrenic injury associated with coronary artery revascularization. Chest 98:661–666 Williams PL, Warwick R (eds). Gray’s anatomy, 36th ed. Churchill Livingstone, London, pp 286–288 http://www.springer.com/978-3-662-49764-7