Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
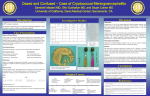
Central Nervous System Cryptococcosis: Parenchymal Calcification and Large Gelatinous Pseudocysts Karen S. Caldemeyer, Vincent P. Mathews, Mary K. Edwards-Brown, and Richard R. Smith Summary: In an 11-year-old immunocompetent girl with protracted cryptococcal infection of the central nervous system, CT showed multiple areas of parenchymal calcification. MR imaging showed large gelatinous pseudocysts around the brain stem. These imaging features and the child’s age are unusual for intracranial cryptococcosis. with back pain, lethargy, a 2.3-kg weight loss, and vomiting. CSF culture showed 65 leukocytes (1% polymorphonuclear, 88% lymphocytes, 11% monocytes), a glucose level of 89 mg/dL, and a protein level of 4100 mg/dL. CSF was negative for cryptococcal antigen, and cytologic findings were normal. Serologic tests for cryptococcosis, histoplasmosis, blastomycetes, coccidioidomycosis, brucella, and syphilis were negative. Urine was negative for histoplasmosis antigen. CT scans showed multiple areas of parenchymal calcification and low attenuation in the posterior fossa. MR images of the brain showed leptomeningeal enhancement; multiple enhancing lesions in the cortex, basal ganglia, and thalami; dilatation of VirchowRobin spaces; and large cysts compressing the brain stem (Fig 1). Spinal MR images showed diffuse leptomeningeal enhancement. The child underwent a suboccipital craniectomy and fenestration of the infratentorial cysts. At surgery, a grayish mucoid material was seen throughout the posterior fossa. CSF obtained at the time of surgery showed an extremely elevated cryptococcal antigen titer of 1:2560. The child was subsequently treated with intravenous amphotericin B. Index term: Brain, infection Cryptococcosis, the most common mycotic infection of the central nervous system (CNS), primarily manifests as meningitis (1–7). Several reports have described extension of the meningeal infection along perivascular spaces giving rise to small cysts, termed gelatinous pseudocysts, in the Virchow-Robin spaces and adjacent brain (1– 8). We present a case of CNS cryptococcosis in which there were large gelantinous pseudocysts compressing the brain stem and multiple areas of intraparenchymal calcification. Case Report Discussion In September 1993, a then 9-year-old girl was treated at another hospital for headache, nausea, vomiting, neck and back pain, and left-sided numbness. The child was afebrile and confused and had nuchal rigidity. There was no papilledema or focal neurologic deficit. Lumbar puncture disclosed three leukocytes, a protein level of 120 mg/dL, and a glucose level of 91 mg/dL. Cerebrospinal fluid (CSF) gram stain and bacterial, fungal, acid fast bacillus, and viral cultures were negative. Computed tomography (CT) and magnetic resonance (MR) imaging showed mild ventricular dilatation. The child was placed on amoxicillin and symptoms improved. Three weeks later, the girl was seen for a left-sided focal seizure and placed on anticonvulsant medication. Two months later, MR imaging showed an increase in ventricular size, and a ventriculoperitoneal shunt was placed. CSF culture was again noncontributory. The child was referred to our institution in July 1995 Cryptococcosis, caused by an encapsulated yeastlike fungus, is the most common CNS mycotic infection (1– 4). Cryptococcus neoformans is a ubiquitous organism found in mammal and bird feces, particularly pigeon droppings (2, 3, 5, 7). CNS cryptococcosis is believed to result from hematogenous dissemination from the lung (1–3, 5, 6). Although the infection may occur in immunocompetent persons, many patients have an underlying chronic illness, such as diabetes mellitus, collagen vascular disease, chronic renal disease, alcoholism, or malignantneoplasms, particularly lymphoreticular disor-ders, or they are on immunosuppressive medication (2– 6). Patients with acquired im- Received November 14, 1995; accepted after revision March 17, 1996. From the Department of Radiology, Indiana University School of Medicine, University Hospital, Room 0279, 550 N University Blvd, Indianapolis, IN 46202. Address reprint requests to Karen S. Caldemeyer, MD. AJNR 18:107–109, Jan 1997 0195-6108/97/1801–0107 © American Society of Neuroradiology 107 108 CALDEMEYER AJNR: 18, January 1997 Fig 1. MR findings in an 11-year-old girl with protracted cryptococcal infection of the CNS. A and B, Precontrast T1-weighted (800/20 [repetition time/echo time]) (A) and T2-weighted (2500/80) (B) images show multiple posterior fossa extraaxial cysts compressing the adjacent brain stem. C and D, Contrast-enhanced T1weighted (800/20) images show diffuse enhancement of the leptomeninges and along the margins of the posterior fossa cysts. At surgery, these cysts were seen to be filled with grayish mucoid material. muno-deficiency syndrome (AIDS) are particularly susceptible to intracranial cryptococcosis (1, 3). Cryptococcosis may occur at any age, but is rare before puberty (3). Encapsulation occurs in response to the host’s immunologic attack on the organism (1, 3). The capsule consists of viscous acidic polysaccharides, which may produce mucoid deposits in the brain and subarachnoid space (1, 3, 5). CNS cryptococcosis commonly presents with nonspecific manifestations of meningitis and encephalitis, such as headache, mental aberrations, low-grade fever, meningismus, and evidence of increased intracranial pressure (2, 3, 5). The course may be fulminant or chronic and insidious depending on the host’s resistance and the inoculum of infection (1, 3, 6). CSF pressure is often increased, and there may be mild to moderate leukocytosis and decreased glucose and elevated protein levels (2, 3, 5). Infected patients may have elevated cryptococcal antigen titers in the serum or CSF (3, 6). The level of antigen titer corresponds to the severity of disease (5). Organisms may be detected by microscopic examination and culture (3, 6). CNS cryptococcosis primarily manifests as meningitis, most pronounced at the base of the brain (1–3, 6, 7). The infection often provokes little inflammatory reaction, owing to the host’s immunity and to the immunosuppressive effect of the organism’s capsule (1– 4, 7). A grayish, mucinous exudate accumulates over the brain surface (3, 7). Infection of the meninges may AJNR: 18, January 1997 spread to the adjacent brain through the subarachnoid space or along the ependymal surface (2, 3). As the infection spreads along the Virchow-Robin spaces that accompany perforating arteries, the perivascular spaces may become distended with mucoid, gelatinous material that originates from the organism’s capsule (2, 4, 5, 7). Larger collections of organisms and gelatinous capsular material have been termed gelatinous pseudocysts (1, 7). Mass lesions representing cryptococcomas may occur, particularly in the deep gray matter (1, 6). Imaging findings are primarily manifestations of meningitis. Hydrocephalus often develops as a result of meningeal scarring (2, 6). Punctate hyperintensities, representing dilated perivascular spaces or cryptococcomas, are frequently seen in the basal ganglia, thalami, and midbrain on T2-weighted MR images (1, 7). Proliferating masses of organisms and gelatinous material may distend the subarachnoid spaces (2, 8). Granulomas may be seen throughout the brain, along the ependyma, in the choroid plexus, and along the spinal cord and spinal nerve roots (2, 5–7). Contrast enhancement of the meninges and cryptococcomas may or may not occur and frequently is absent in AIDS-related cryptococcosis (1, 6). Calcification of cryptococcomas is rare (2). Our patient showed findings of chronic cryptococcal meningitis. While leptomeningeal and miliary nodular enhancement have been described (7), we have not found reports of the very large gelatinous pseudocysts seen in this patient. These mucinous collections are typi- CRYPTOCOCCOSIS 109 cally small and found along the meninges, in the perivascular spaces, and in the deep gray structures (2, 8). Larger cysts may arise from coalescence of smaller lesions and are seen predominantly in the basal ganglia and thalami (8). These cystic lesions are less common than in the past owing to earlier diagnosis and treatment of CNS cryptococcosis (2). Our patient had a long, untreated course, which most likely contributed to this flagrant manifestation. She also had parenchymal calcification, a rare finding in CNS cryptococcosis. This again most likely occurred as a result of the protracted disease course. References 1. Mathews VP, Alo PL, Glass JD, Kumar AJ, McArthur JC. AIDSrelated CNS cryptococcosis: radiologic-pathologic correlation. AJNR Am J Neuroradiol 1992;13:1477–1486 2. Fetter BF, Klintworth GK, Hendry WS. Mycoses of the Central Nervous System. Baltimore, Md: Williams & Wilkins; 1967:89 –123 3. Hoeprich PD. Infectious Diseases. Hagerstown, Md: Harper & Row; 1977:1232–1141 4. Wehn SM, Heinz ER, Burger PC, Boyko OB. Dilated Virchow-Robin spaces in cryptococcal meningitis associated with AIDS: CT and MR findings. J Comput Assist Tomogr 1989;13:756 –762 5. Everett BA, Kusske JA, Rush JL, Pribram HW. Cryptococcal infection of the central nervous system. Surg Neurol 1978;9:157–163 6. Cornell SH, Jacoby CG. The varied computed tomographic appearance of intracranial cryptococcosis. Radiology 1982;143:703– 707 7. Tien RD, Chu PK, Hesselink JR, Duberg A, Wiley C. Intracranial cryptococcosis in immunocompromised patients: CT and MR findings in 29 cases. AJNR Am J Neuroradiol 1991;12:283–289 8. Garcia CA, Weisberg LA, Lacorte SJ. Cryptococcal intracerebral mass lesions: CT-pathologic considerations. Neurology 1985;35: 731–734