Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
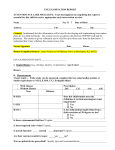
(Insert District Logo/Information Here) Patient’s Name: _____ D.O.B.: Address: City: ____ SASID Number: State: ______ Zip: Attention Eye Care Specialist: Please address each item below. Your thoroughness in completing this report is essential for this patient to receive appropriate services. Ocular History (e.g., previous eye diseases, injuries, or operations) Age of Onset ___________ History _________________________________________________________________ __________________________________________________________________________________________ Visual Acuity If the acuity can be measured, complete this box using Snellen acuities or Snellen equivalents or NLP, LP, HM, CF. Without Glasses With Best Correction Near Distance Near Distance OD OD OD OD Acuity with glare testing, if applicable: OS OS OS OS OD_________ OU OU OU OU OS _________ IMPORTANT: If the acuity cannot be measured, check the appropriate estimation. Functions better than 20/200 corrected, in his/her best eye (Snellen equivalent) Meets the definition of Blindness “MDB” Central vision acuity of 20/200 or less in the better eye with correcting glasses or a peripheral field so contracted that the widest diameter of such field subtends an angular distance no greater than 20 degrees. Functions at the definition of Blindness “FDB” When visual performance is reduced by a brain injury or dysfunction when visual function meets the definition of blindness as determined by an eye care specialist or neurologist. Students in this category manifest unique visual characteristics often found in conditions referred to as neurological, cortical or cerebral vision impairment. Muscle Function Normal Intraocular Pressure Reading Abnormal Describe: OD _______________ OS ______________ Visual Field Test There is no apparent visual field restriction. There is a field restriction. Describe __________________________________________ Yes No The visual field is restricted to 20 degrees or less. Color Vision Normal Abnormal Photophobia Yes No Diagnosis (Primary cause of visual loss) __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Permanent Recurrent Improving Progressive Communicable Can Be Improved Treatment Recommended Glasses Prescription OD ___________________ Patches (Schedule): OS ___________________ OD ______________________________ Medication _______________________ OS ______________________________ Low Vision Evaluation Refer for other medical treatment/exam: Other ____________________________ _________________________________ Scheduling Date of Next Appointment ___________________ Time _____________ Precautions or Suggestions (e.g., lighting conditions, activities to be avoided, etc.) __________________________________________________________________________________________________ ____________________________________________ Print or Type Name of Licensed Ophthalmologist or Optometrist ____________________________________________ Address ___________________________________________ Date of Examination ____________________________________________ City ____________________________________________ Signature of Licensed Ophthalmologist or Optometrist State Zip ____________________________________________ Telephone Number RETURN COMPLETED FORM TO: _______________________________________________ Name _______________________________________________ Address _______________________________________________ Agency _______________________________________________ City State Zip