Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
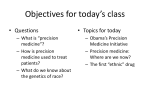
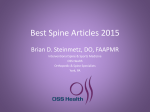
Long-Term Back Pain Relief with Precision Spectra SCS and 32-Contact Anatomically-Based Programming Salim Hayek MD PhD1, Elias Veizi MD1, James North MD2, T. Brent Chafin MD3, Thomas Yearwood MD PhD4, Louis Raso MD5, Robert Frey MD6, Kevin Cairns MD7, Anthony Berg MD8, John Brendel MD9, Nameer Haider MD10, Matthew McCarty MD11, Henry Vucetic MD12, Kasra Amirdelfan MD13, Lilly Chen MD14, Jai Shetake PhD14, Brad Hershey MS14, Nitzan Mekel-Bobrov PhD14 1University Hospitals Case Medical Center, OH; 4Comprehensive 7Florida Pain and Rehabilitation, Spine Specialists, FL; 10Comprehensive 13Integrated 8Spine Pain Clinic, NY; MS; 5Jupiter Team Texas, TX; 11Balcones Pain Management Medical Group, CA; NM-278608-AA_DEC2014 2Carolinas Pain Institute, NC; Pain Clinic, FL; 9Interventional Pain Consultants, TX; 14Boston 3Roanoke-Chowan 6Pacific Pain Hospital, NC; Management, CA; Pain Specialists of Wisconsin, WI; 12The Scientific Corporation, CA Spine and Pain Institute, OH; Disclosures Dr. Salim Hayek has served as a paid consultant for Boston Scientific’s Medical Advisory Board. Background Conventional SCS for low back pain has, historically, been challenging compared to treatment of leg pain. • Modest clinical outcomes for low back pain relief in SCS RCT (PROCESS 2008). • Consistently lower relief of low back pain compared to leg pain in SCS observational studies (Barolat et al. 2001, North et al. 2005). (Kumar et al. 2008) • The nature of the low back innervating fibers is challenging for SCS: 1. More lateral: dorsal roots get recruited first 2. Smaller: higher stimulation threshold 3. Deeper: higher stimulation threshold Background SCS advances have been developed to address these challenges. • Lead configurations − New surgical leads − Greater number of electrodes − New potential lead combinations • Targeting specificity − Constant current − Multiple independent current control − Anatomically-guided neural targeting algorithm • Waveforms and Field Shapes − Anode intensification − High frequency stimulation − Burst stimulation Background Spectra SCS system introduced in 2013 a new SCS paradigm using Anatomically-Guided Neural Targeting Algorithm with 32-contact multiple independent current control (MICC). Key design features: • Algorithmic optimization of contacts and current to target a particular area of the cord. • Accounts for relative positions of contacts and leads relative to each other. • Adjustable resolution for search and coverage around the stimulation target. Background “Technological advancements do not always result in better outcomes” (Kumar et al., 2014) Study objective: characterize the real-world clinical outcomes of the 32-contact MICC Neural Targeting Algorithm to test whether high levels of low back pain relief are being achieved. Materials & Methods: Study Design Study Design Multi-center, consecutive observational study (all patients meeting inclusion criteria at participating sites were included without bias) Study Device Precision Spectra SCS with 32-contact MICC anatomically-guided neural targeting algorithm Sample Size 213 SCS trialed patients Number of Sites 13 US sites Follow-up Duration 2 years planned – currently at 1 year post-implant Key Inclusion Criteria Real-world cohort – only requirement is on label treatment with the Precision Spectra SCS System for low back and leg pain. Study Assessments • • • Baseline information: demographics, diagnosis, pain location Procedural information: lead configuration, programming parameters Clinical outcomes: - SCS trial outcomes success rate - Trial QoLs: sleep improvement, physical function, activities of daily living (ADLs), percent pain relief (PPR). - Pain intensity (0-10 numerical rating scale - NRS) Materials & Methods: Patient Cohort (N=213) 50% 50% 44% 40% 36% 40% 30% 30% 20% 20% 25% 18% 20% 16% 13% 10% 10% 8% 4% 6% 4 5 11% 0% 0% Low Back Only Legs Only Pain Locations Low Back and Legs 1-3 Mild 6 Moderate 7 8 9 10 Severe Baseline Distribution of Pain Intensity (0-10 NRS) • Age (mean ±SD): 57 ±15 • Gender: 63% F, 37% M • The most common location of pain was low back only (44%), followed by low back and legs (36%). • The baseline distribution of pain intensities was skewed towards the severe category, as expected for SCS patients, with a median of 8.0 points. Materials & Methods: Procedure Information 1 Lead 3% 8 contacts 1% 50% 42% 4 Leads 12% 40% 30% 30% 3 Leads 14% 2 Leads 71% 32 contacts 50% 16 contacts 37% 20% 10% 10% 24 contacts 12% Number of Contacts Implanted 8% T9 T10 - T12 0% T1 - T5 Number of Leads Implanted 7% 3% T6 T7 T8 Vertebral Position of Implanted Leads (top of lead) • A wide range of lead configurations was used, consistent with intended flexibility. • The predominant mode of implant for this system was two 1x16 percutaneous leads (40% of patients). • 62% of patients were treated with lead configurations using 24-32 contacts. • Lead placement for permanent implant procedures, based on location of the lead tip, was predominantly in the T6-T8 vertebral levels, capturing 88% of cases. Results: SCS trial outcomes Trial-to-perm ratio was 86% in this cohort, with highly significant pain reduction. Patient Reported Trial Outcomes Responders Sleep Improvement (N=56) 18% Medications Reduced (N=56) 31% ADLs Increased (N=36) 28% Physical Function Increased (N=36) 40% • All patients: Highly significant difference of 4.00 points between baseline overall pain (7.17) and overall pain at end of trial (3.17). • Severe patients (baseline NRS = 8-10): Highly significant difference of 5.30 points between baseline pain (8.74) and pain at end of trial (3.44). Results: Overall Pain Outcomes Patients in this cohort showed highly significant overall pain relief maintained out to 12 months post-implant. • All patients: Highly significant difference of 4.21 points between baseline pain (7.17) and pain at 12 months post-implant (2.96). • Severe patients (baseline NRS = 8-10): Highly significant difference of 5.73 points between baseline pain (8.75) and pain at 12 months post-implant (3.02). Results: Low Back Pain Outcomes Patients in this cohort showed highly significant low back pain relief maintained out to 12 months post-implant, equivalent to overall pain relief. • All patients: Highly significant difference of 4.04 points between baseline pain (7.21) and pain at 12 months post-implant (3.17). • Severe patients (baseline NRS = 8-10): Highly significant difference of 5.73 points between baseline pain (8.60) and pain at 12 months post-implant (2.87). Results: Responder Rate Outcomes 71% of patients in this cohort showed ≥50% low back pain NRS reduction at 12 months post-implant, equivalent to the responder rate for overall pain. Responder Rate (≥50% NRS reduction) Responder rates for overall pain and low back pain converge by 6 months post-implant and remain stable out to 12 months post-implant at an equivalently high level. Conclusions • In a cohort of 213 patients treated with the Precision Spectra system, based on an anatomically-guided neural targeting algorithm, and followed out to 12 months post-implant, we found: − High trial-to-perm ratio − Highly significant low back pain reduction, equivalent to reduction in overall pain − High low back pain responder rate, equivalent to responder rate of overall pain • These results suggest that the novel anatomically-guided neural targeting algorithm, with the 32-contact MICC Precision Spectra system, may provide previouslyunattained clinical outcomes for low back pain. • Further study is currently underway in both an RCT and a large-scale registry study. Indications for Use Indications for Use. The Precision Spectra™ Spinal Cord Stimulator System (Precision Spectra System) is indicated as an aid in the management of chronic intractable pain of the trunk and/or limbs, including unilateral or bilateral pain associated with the following: failed back surgery syndrome, intractable low back pain, and leg pain. Contraindications, warnings, precautions, side effects. The Precision Spectra System is contraindicated for patients who: are unable to operate the Precision Spectra System, have failed trial stimulation by failing to receive effective pain relief, are poor surgical risks, or are pregnant. Refer to the Instructions for Use provided with the Precision Spectra System or ControlYourPain.com for potential adverse effects, warnings, and precautions prior to using this product. Caution: Federal (U.S.) law restricts this device to sale by or on the order of a physician. Results from clinical studies are not predictive of results in other studies. Results in other studies may vary. © 2014 Boston Scientific Corporation or its affiliates. All rights reserved. All trademarks are the property of their respective owners.