Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
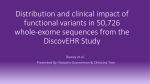
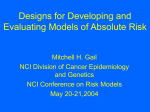
Objectives for today’s class • Questions – What is “precision medicine”? – How is precision medicine used to treat patients? – What do we know about the genetics of race? • Topics for today – Obama’s Precision Medicine Initiative – Precision medicine: Where are we now? – The first “ethnic” drug Definitions • Pharmacogenomics: the study of the role genetics plays in drug response • Precision medicine: customization of medical decisions and courses of treatment based on the individual patient • Personalized medicine: creation of new treatments in response to a particular patient’s need Obama’s Precision Medicine Initiative State of the Union, 2015 “Most medical treatments have been designed for the “average patient”. As a result of this ‘one-size-fits-all-approach,’ treatments can be very successful for some patients but not for others.” The promise: $215 million investment split among the NIH, NCI, FDA, & ONC The objectives: • More and better treatments for cancer • Creation of a voluntary national research cohort • Commitment to protecting privacy • Regulatory modernization • Public-private partnerships https://www.whitehouse.gov/the-press-office/2015/01/30/fact-sheet-president-obama-s-precision-medicine-initiative 2 trios 179 individuals 4 populations 697 individuals 7 populations Estimated numbers of potentially functional variants in genes The 1000 Genomes Project samples a variety of human populations Precision Medicine Initiative - Background Mission: To enable a new era of medicine through research, technology, and polices that empower patients, researchers, and providers to work together toward development of individualized treatments. Information Input: • 4 Workshops between April and July 2015 –Unique Scientific Opportunities for the National Research Cohort – Digital Health Data in a Million-Person Precision Medicine Initiative – Participant Engagement and Health Equity – Mobile and Personal Technologies in Precision Medicine • Requests for Information – Building the cohort – Strategies to address community engagement and health disparities PMI Cohort Program (PMI-CP) WG: Vision and Design for a longitudinal research cohort of ≥1 million volunteers Key Questions: 1) Combine existing cohorts, establish new, or both? 2) How to capture the U.S. population diversity? 3) What data types should be included? 4) What policies needed for maximal benefit to all stakeholders? Slides from www.healthit.gov • FNIH Survey of public perceptions of precision medicine cohort • White House Privacy and Trust Principles Anticipated FY2016 Appropriations Agency NIH $ Million 200 • Cancer • 70 • Cohort • 130 FDA 10 Office of the Natl Coord. for Health IT (ONC) 5 TOTAL 215 Information Flow In Information Flow Out What can we learn from a massive cohort? • Discover new biomarkers predictive of future disease risk • Discover determinants of individual variation in response to therapeutics • Determine quantitative risk estimates in the population by integrating environmental exposures, genetic factors, and gene-environment interactions • Integrate mobile health and sensor technologies • Determine impact of loss-of-function mutations on clinical outcome • Discover new classifications and relationships among diseases • Enable targeted clinical trials of subjects with rich clinical data Desired characteristics of the cohort • One million or more volunteers • Longitudinal cohort with continuing interactions • Re-contactable • Collect – – – – electronic health records biospecimen, survey, and complete a baseline exam Two methods of recruitment • Direct volunteers Anyone can sign up • Healthcare provider organizations Sources of diversity • • • • • Groups that are underrepresented All states of health and disease All areas of the U.S. All life-stages Special policy considerations – enrolling children – decisionally impaired – participants who become incarcerated Initial Core Data Set – Informatics Opportunities Centrally collected and stored in a Coordinating Center Align with other data sets when possible Leverage existing data standards and common data models Data Source Data Provided Self report measures Diet, substance use, self-report of disease and symptoms (e.g., cognitive or mood assessment) Baseline health exam Vitals (e.g., pulse, blood pressure, height, weight), medical history, physical exam Structured clinical data (EHR) ICD and CPT codes, medication history, select laboratory results, vitals, encounter records Biospecimens Blood sample mHealth data Passively-collected data (e.g., location, movement, social connections) from smartphones, wearable sensor data (activity, hours and quality of sleep, time sedentary Genetics as a therapy tool in cancer • Physician-ordered multigene assays can provide recurrence predictions and guide treatment options in node negative or node positive, ERpositive, HER2-negative invasive breast cancer • Oncotype DX (16 cancer-related genes and 5 reference genes) analyzed for gene expression (mRNA) The current state of affairs • In 2013, 114 genes were selected by a panel of experts as “medically actionable genetic conditions possibly undiagnosed in adults”. • In this study of 1,000 people the frequency of likelyhigh-impact variants in these genes was ~3.4% for European descent and ~1.2% for African descent. Am J Hum Genet. 2013 93(4): 631-640 CYP2D6 is responsible for metabolizing ~25% of all drugs Nature Reviews Drug Discovery 2002 1: 37-44 Nature Reviews Drug Discovery 2004 3: 749-761 http://www.pharmacytimes.com/publications/issue/2008/2008-07/2008-07-8624 Ultra-rapid metabolizing mother yields more morphine in breast milk Nature Reviews Drug Discovery 2002 1: 37-44 Nature Reviews Drug Discovery 2004 3: 749-761 Polymorphisms modulate drug disposition Polymorphisms modulate drug targets and actions The treatment of congestive heart failure (HF) • ~5.1 million people in the U.S. • More common in African Americans • About half of people with HF will die within 5 years of diagnosis • Costs the nation ~$32 billion/year http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/ Heart failure prevalence is geographically variable Isosorbide dinitrate / hydralazine colriculsu.freewebsite.biz V-HeFT suggests greater BiDil efficacy in self-identified African-Americans http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4145B2_02_01-NitroMed-Background.htm The A-HeFT Trial • Multicenter, double-blind, placebo-controlled, randomized (H + ISDN=BiDil) vs. placebo • Population = self-reported black (or of African descent) • New York Heart Association Class III-IV HF on standard therapy • Left ventricular ejection fraction (LVEF) ≤ 35% QOL = quality of life Echo = echocardiogram J Card Fail 2002 8 (3): 128-35. BiDil: The first approved “ethnic” drug A-HeFT results: • 43% reduction in mortality in the treatment arm • 39% reduction in first hospitalization from HF in the treatment arm • Improved quality of life BiDil approved by the FDA in June 2005. The genetic underpinnings of BiDil efficacy are still being determined NEJM 2004 351(20): 2049-2057. Drug development can take decades http://www.mdlingo.com/article/fda-approval-process-for-new-drugs